")
Back to Journals » Patient Preference and Adherence » Volume 16
Emotional Experiences of Skin Markings Among Patients Undergoing Radiotherapy and Related Factors: A Questionnaire-Based Cross-Sectional Study
Authors Asada H , Takahashi Y, Ono Y, Kishi N , Matsuo Y, Mizowaki T , Nakayama T
Received 21 February 2022
Accepted for publication 13 May 2022
Published 26 May 2022 Volume 2022:16 Pages 1359—1369
DOI https://doi.org/10.2147/PPA.S361916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hiromi Asada,1 Yoshimitsu Takahashi,1 Yuka Ono,2 Noriko Kishi,2 Yukinori Matsuo,2 Takashi Mizowaki,2 Takeo Nakayama1
1Department of Health Informatics, Kyoto University School of Public Health, Kyoto, 606-8501, Japan; 2Department of Radiation Oncology and Image-Applied Therapy, Graduate School of Medicine, Kyoto University, Kyoto, Japan
Correspondence: Hiromi Asada, Department of Health Informatics, Kyoto University School of Public Health, Yoshida Konoe-cho, Sakyo-ku, Kyoto, 606-8501, Japan, Tel/Fax +81-75-753-9479, Email [email protected]
Purpose: Patients undergoing radiotherapy often have their skin marked. Previous studies on skin markings examined the durability and physical effects of the markings, but no study has focused on patients’ emotional experiences toward the markings. This study aimed to clarify how patients undergoing radiotherapy feel about skin markings, as well as factors that affect patients’ emotional experiences.
Patients and Methods: We conducted a cross-sectional study using a self-administered questionnaire and medical records. Participants were patients aged ≥ 20 years undergoing cancer radiotherapy at a designated cancer care hospital. The primary outcome was the level of uncomfortable emotions toward skin markings, and the secondary outcome was the level of favorable ratings on skin markings. To examine factors related to uncomfortable emotions, ordinal logistic regression analysis was performed.
Results: Questionnaire forms were distributed to 153 patients, and responses were collected from 132 (86%). Among 108 patients included in the analysis, 56% (59/105, excluding 3 who did not answer this question) responded that they were uncomfortable with skin markings. The proportion of patients who favorably rated skin markings was 63% (59/93, excluding 15 who did not answer this question). No factors were significantly associated with the primary outcome.
Conclusion: Many patients accepted skin markings with resignation, as they understood the necessity of the markings in their treatment. Medical staff should understand the emotional experiences of patients toward skin markings and take sufficient care to ensure that they are provided with explanations, including the impact of skin markings on their daily lives, as well as a sense of security that treatment is being performed in a precise manner.
Keywords: radiotherapy, marking, emotional experiences, questionnaire survey
Introduction
Cancer is a leading cause of death in the world. One of the most effective cancer treatments is radiotherapy,1 a local therapy that imposes little physical burden and can be administered to patients of all ages and conditions for curative and palliative purposes.
In radiotherapy, radiation must be delivered precisely to the same site each time. Thus, in order to ensure reproducibility of the irradiation position, patients often have markings done directly on their skin. Marking methods and products used differ from facility to facility. For example, some facilities use permanent ink tattoos, while others offer non-permanent options such as henna and marker pens.2 Since patients continue to work and lead their daily lives while undergoing treatment,3 markings that are noticeable to others can be a source of concern.4 Moreover, visible skin markings are a constant reminder that they are suffering from cancer.5 Patient emotions in healthcare are influenced not only by what patients express, but also by their experience, stage of illness, and other conditions, as well as their relationship with their healthcare provider. And with regard to emotions of discomfort, it is known that patients often experience these emotions but do not express them.6 It is important to understand the honest emotions of patients in order to provide them with the care they desire.
Previous studies on skin markings compared the durability of products used for markings and reported on their physical effects.7,8 There are reports on behavioral changes in patients that describe negative emotional experiences toward the markings and discomfort experienced during treatment, along with the various emotions associated with tests and examinations during follow-up after completion of cancer treatment.7,9–11 However, none of these studies focused on the psychology of patients with skin markings. While attempts have been made to improve methods for skin markings with recent advances in treatment technologies, only the perspectives of medical providers have been considered, with no attention to patient-oriented evidence. In order to perform treatment in a safe and precise manner, and to provide a greater sense of security and less discomfort to patients by reducing their uncomfortable and complex emotions toward treatment to the extent possible, we need to understand how patients undergoing radiotherapy feel about skin markings, and consider marking methods that take into account patient perspectives.
To this end, the present study aimed to clarify the emotional experiences of patients undergoing radiotherapy toward skin markings, as well as related factors.
Materials and Methods
Study Design
A cross-sectional study with a self-administered questionnaire survey of patients and review of medical records.
Setting and Participants
Participants were patients undergoing radiotherapy at the radiation oncology department of a designated cancer hospital in Kyoto City. Inclusion criteria were 1) cancer patients receiving radiotherapy, 2) age ≥20 years, 3) have skin markings, and 4) cancer diagnosis has been disclosed. Exclusion criteria were 1) patients with difficulty communicating in Japanese, 2) no consent to study participation, and 3) participation was deemed inappropriate by a radiation therapist.
Marking Methods
At the study facility, initial markings are made at the time of radiotherapy planning using a skin marking pen and a brush with a specialized skin ink reddish-purple in color. On the first day of treatment and every weekend thereafter (and whenever markings faded), markings were traced using a permanent marker or skin marking pen with a protective spray.
Survey Items
Items to be extracted from the questionnaire and medical records were prepared based on previous reports and consultation with radiation therapists and nurses (including the author).7,9–13 Then, additions and modifications were made to the survey items based on the opinions of 7 radiation therapists (different from those mentioned above), 2 certified nurses in radiation oncology nursing (not including the author), and 5 patients. In addition, a pilot test was conducted with 3 of the above-mentioned radiation therapists, 2 nurses (different from those mentioned above), and 1 non-medical person to finalize the survey items.
Questionnaire
The questionnaire included the following items: 1) emotional experiences toward skin markings; 2) subjective symptoms and circumstances during the treatment period; and 3) participant attributes. There were 21 questions, and the general response time was about 8 minutes. Other than 2 free-description questions, all questions were multiple choice.
Medical Record Data Sheet
Objective data (eg, age, sex, Performance Status (PS), diagnosis, treatment setting, site of treatment, number of treatment sessions, and purpose of treatment) were obtained from medical records.
Outcomes
The primary outcome was the level of uncomfortable emotional experiences toward skin markings, and the secondary outcome was the level of favorable ratings on skin markings. Responses were provided on a 5-point rating scale (“very uncomfortable/favorable,” “quite uncomfortable/favorable,” “somewhat uncomfortable/favorable,” “not uncomfortable/favorable,” and “I prefer not to answer”). For analysis, binary responses were used, with the first three ratings being classified into “yes,” and the last two into “no.” “I prefer not to answer” was treated as a missing value.
Sample Size
Based on a previous study targeting breast cancer patients and discussions among 3 radiation therapists and a nurse (author),9 the number of patients to be included in this study was set to 100, estimating that a samples size of 93 would be necessary to achieve an expected rate of 60% with a 95% CI within ±10%.
Questionnaire Distribution and Data Collection
Between October 5, 2020 and February 10, 2021, 18 radiation therapists distributed the questionnaire and informed consent form describing the study to patients who met the eligibility criteria, and provided an explanation during the final examination in the treatment period. If patients understood the study and agreed to participate, they checked the box on the consent form and responded to the questionnaire. Patients were asked to place the completed questionnaire in the collection box installed in the hospital, or send it back by postal mail. After confirming that patients returned their questionnaires with a check mark in the box indicating consent, the principal investigator or radiation therapists obtained information from their medical records.
Statistical Analysis
The level of uncomfortable emotional experiences toward skin markings and the level of favorable ratings on skin markings were analyzed using descriptive statistics. For each evaluation item, the proportion and 95% CI were calculated from the cross-tabulation table. For related factors, ordinal logistic regression analysis was performed with the level of uncomfortable emotional experiences as the objective variable, and age (≤64 years/>65 years), sex (male/female), site of treatment (cervicothoracic/abdominal-pelvic), number of treatment sessions (≤16 times/≥17 times), treatment setting (inpatient/outpatient), work status (yes/no), whether they thought prior explanations were consistent with the marking procedure they actually underwent (yes/no), and the purpose of treatment (curative/palliative) as explanatory variables. Treatment sites were classified into 2 categories according to expert opinion (Table 1). As for the number of treatment sessions, 2 categories with a cut-off number of 16 were adopted, given that the working generation in recent years receive hypofractionated radiotherapy; this form of radiotherapy, in which higher dosages are used in fewer fractions (ie, the number of treatment sessions is reduced relative to usual radiation delivery), has been introduced in the treatment of breast cancer and prostate cancer. All analyses were performed using JMP Pro 15.1.0, with missing values excluded from each analysis.
 |
Table 1 Treatment Site Categories |
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. The survey was approved by the Ethics Committee of the Graduate School of Medicine and Faculty of Medicine, Kyoto University and Kyoto University Hospital (R2577-1). The contents of the survey, the time required, data management methods, and that participation was voluntary were thoroughly explained in advance via the informed consent form.
Results
Tabulation of Questionnaire Responses
Questionnaire forms were distributed to 153 patients, and responses were obtained from 132 (86%). Of these, 23 responses without a check mark for consent and 1 which was incomplete were excluded as invalid responses. In the end, responses from 108 patients were subjected to analysis (Figure 1).
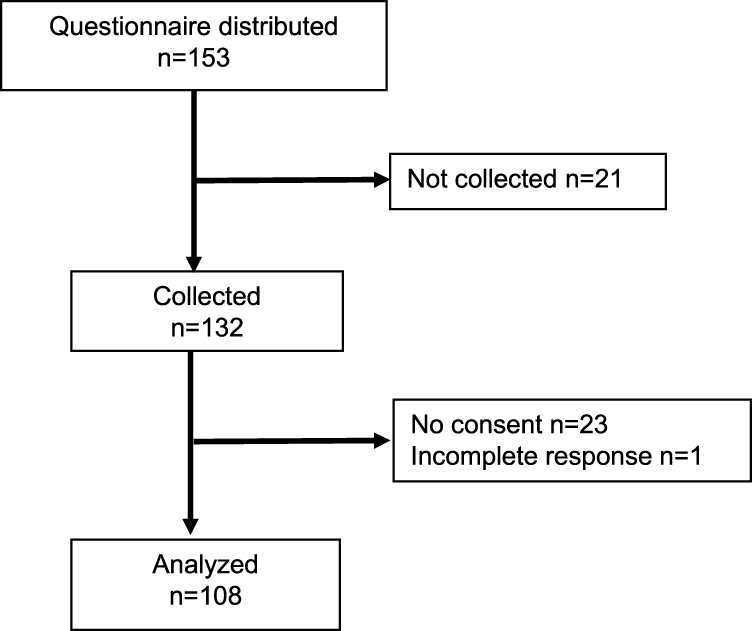 |
Figure 1 Flow chart of participant selection. |
Participant Characteristics
Median age was 66 years, and 59 (55%) participants were female. Among participants who were included in the analysis, 104 (96%) had a PS 0–1, and 85 (79%) were outpatients. The most common site of treatment was breast (27%, n=31), followed by prostate (19%, n=22). During the study period, skin problems due to skin markings were noted in one participant (Table 2).
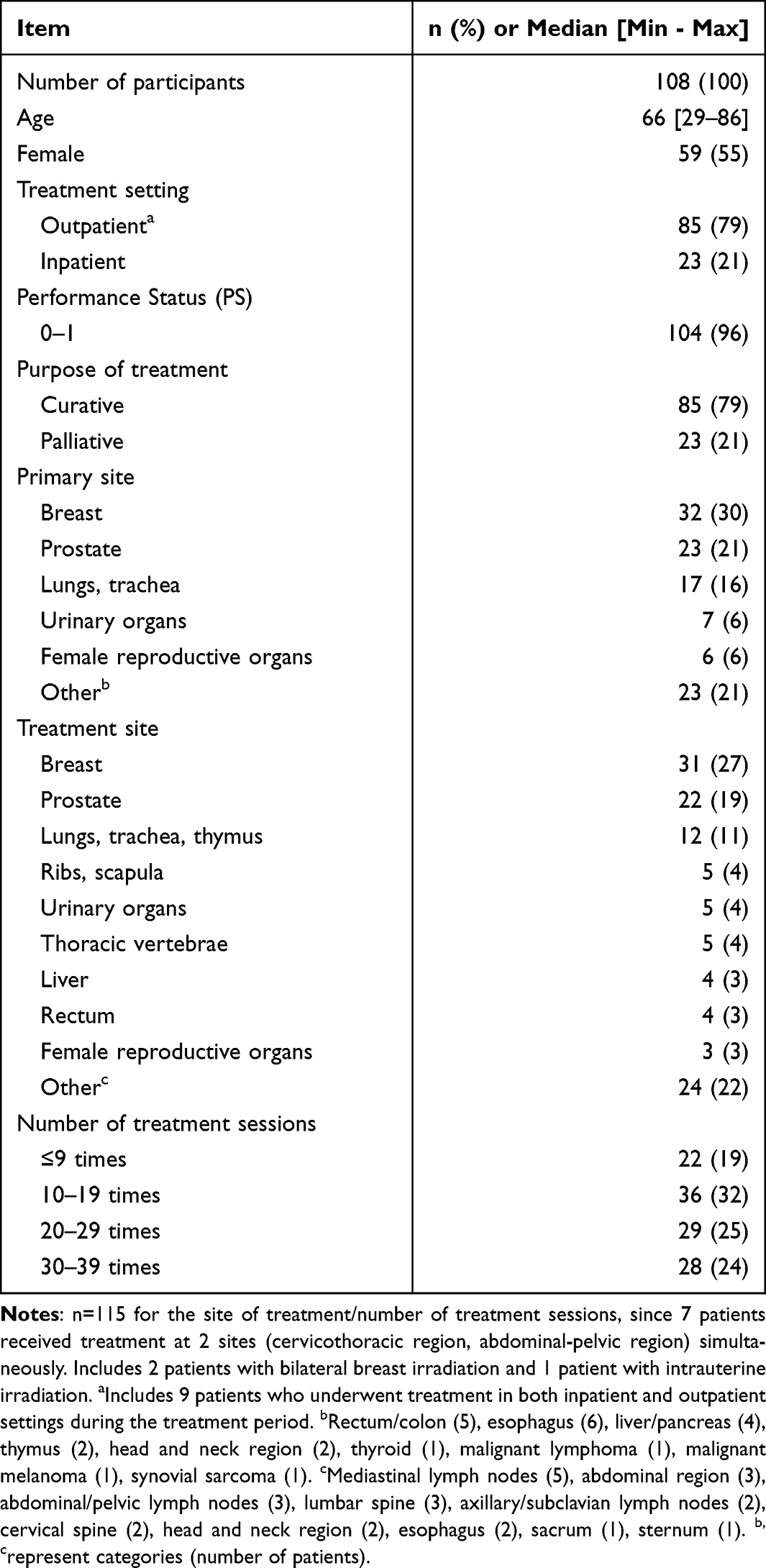 |
Table 2 Participant Characteristics |
Level of Uncomfortable Emotional Experiences
There were 59 (56%, 95% CI: 47–65) participants who responded “yes” to having uncomfortable emotional experiences, with none of the respondents selecting “very uncomfortable.” In total, 40 (68%) of 59 females and 19 (41%) of 46 males had uncomfortable emotional experiences. By age, 26 (46%) of 57 participants aged ≥65 years and 33 (69%) of 48 participants aged ≤64 years had uncomfortable emotional experiences, with the latter showing a higher proportion (Table 3).
 |
Table 3 Distribution of Uncomfortable Emotional Experiences |
Reasons for Uncomfortable Emotional Experiences
Reasons for uncomfortable emotional experiences toward skin markings of the 59 participants are shown in Figure 2. The most common reason was “I have to be careful not to have the markings fade” (85%, n=50), followed by “they make my clothes dirty” (44%, n=26), and “color of the markings”/“the markings are spread across a large area” (22%, n=13). Other reasons included “the pen/brush tip hurts my skin when markings are drawn,” “smell of skin ink,” “protective spray feels unpleasant on the skin,” “ink and spray are cold,” “I don’t like those markings are applied over and over,” “I cannot take a bath as I like,” and “the ink stains the bathtub.”
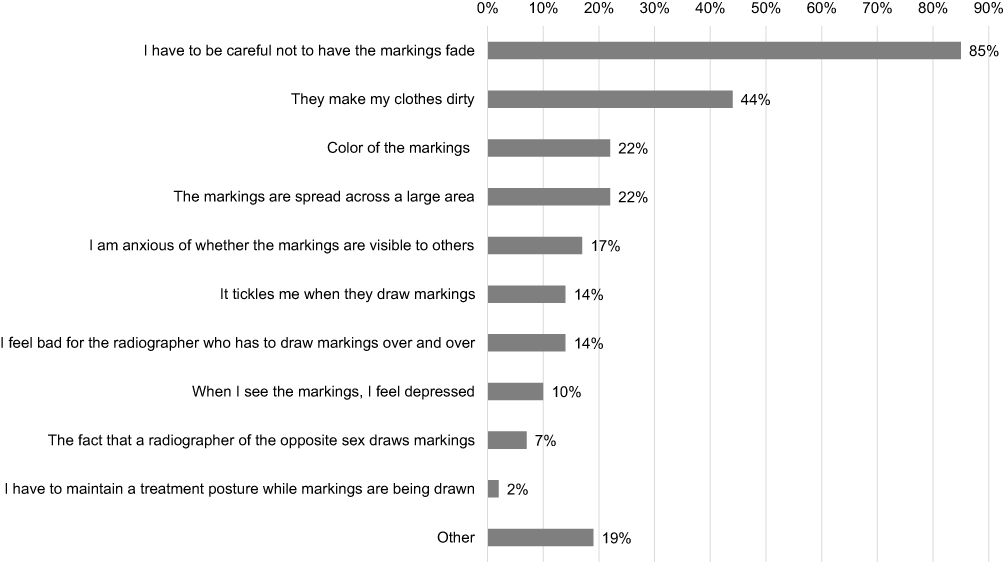 |
Figure 2 Reasons for uncomfortable emotional experiences (n=59). |
Factors That Affect Uncomfortable Emotional Experiences
Univariate and multivariate ordinal logistic regression analyses were performed to identify possible factors affecting patients’ uncomfortable emotional experiences. However, no significant associations were identified for any of the factors examined (Table 4).
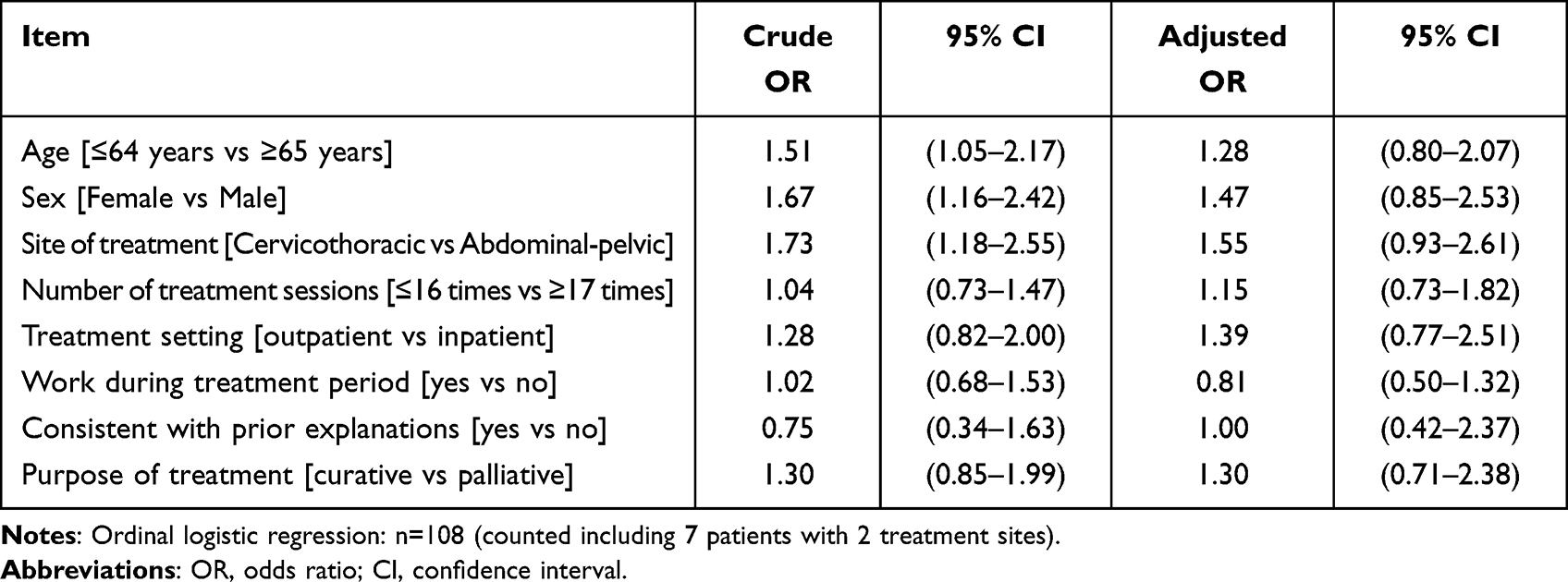 |
Table 4 Associations with Possible Factors Affecting the Level of Uncomfortable Emotional Experiences |
Level of Favorable Emotional Experiences
In total, 59 participants (63%, 95% CI: 53–73) indicated that “it was good to have skin markings.” Although no difference was observed between males and females, the number of participants with favorable ratings was higher among those aged ≥65 years compared to those aged ≤64 years (Table 5).
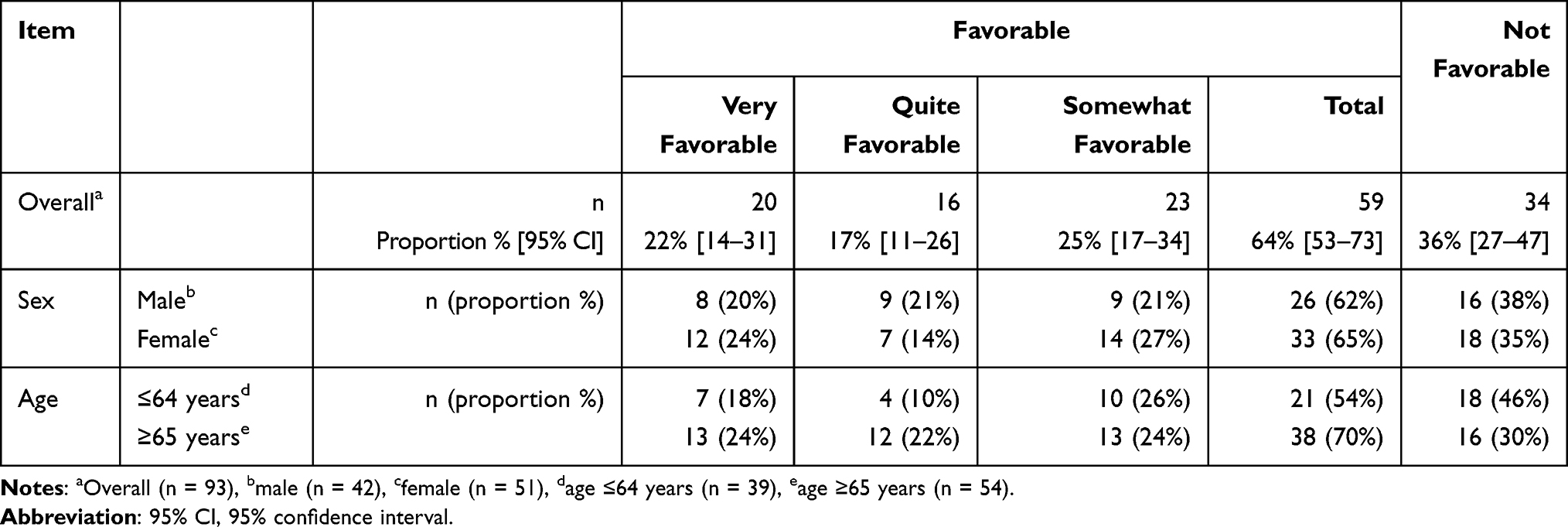 |
Table 5 Level of Favorable Emotional Experiences |
Reasons for Favorable Emotional Experiences
Sixty-six participants provided reasons for why they favorably rated skin markings (including 7 participants who provided reasons without responding to the 5-point rating scale). The most common reason was “they mark the area being treated” (85%, n=56), followed by “markings give me peace of mind” (39%, n=26). Other reasons included “they make me aware of the area being treated so I can avoid irritation,” “they are necessary for safe treatment,” “the time required for positioning by the technician can be shortened,” and “communication with the family.”
Relationship Between Uncomfortable and Favorable Emotional Experiences Ratings
There were 98 participants who responded to both questions regarding the level of uncomfortable emotional experiences and the level of favorable ratings. Among these, the number of participants who had “uncomfortable emotional experiences/favorable ratings” was the highest (n=35, 36%), followed by participants who had “no uncomfortable emotional experiences/favorable ratings” (n=29, 30%).
Subjective Responses Other Than Evaluated Items
With regard to explanations provided by physicians and nurses prior to treatment, 87 of 107 participants who responded to the question indicated that they were “consistent with the marking procedure they actually underwent” (81%), whereas 14 (13%) responded “I do not remember.” Among 106 participants, 98 (92%) exercised caution not to have markings fade during the treatment period. Two (2%) of 108 participants responded, “I don’t like having skin markings, even for treatment purposes,” 61 (56%) responded “skin markings are necessary for treatment, and I don’t mind them,” and 43 (40%) responded “I don’t like having skin markings, but I have no alternative but to accept them for the sake of treatment.” Among 87 participants who accepted skin markings (“I don’t mind skin markings,” “I have no alternative but to accept them for the sake of treatment”) and also responded to the question.
Discussion
This study investigated how patients undergoing radiotherapy feel about skin markings, as well as related factors, through a self-administered questionnaire survey and medical record review. We found that, while 64% of patients favorably rated skin markings for the purpose of treatment, 56% were uncomfortable with them. None of the assessed factors were associated with patients’ uncomfortable emotional experiences.
Radiotherapy is a new experience for first-time patients.10 Therefore, when providing an explanation before starting treatment, medical staff should specifically describe the methods of markings that will be used, why they are necessary, and what precautions to take in daily life, in order to help patients, visualize the treatment they will be undergoing. A previous study of breast cancer patients reported that proper explanations by radiographers before starting treatment promoted understanding in patients and helped reduce their anxiety and psychological distress.14 Many of our patients also reported that explanations provided by doctors and nurses before starting treatment were consistent with the marking procedure they actually underwent, and appropriate explanations by medical staff likely promoted an understanding that markings are indeed necessary. Of the 108 patients, 2 responded that they did not want to have skin markings, whereas 61 (56%) considered them necessary and 43 (40%) accepted them for treatment purposes. However, among the 104 patients who accepted skin markings, 57 (56%) of the 101 who responded to the question about the level of discomfort indicated that they were uncomfortable with skin markings, suggesting that even patients who accepted skin markings felt uncomfortable. As for reasons why patients found skin markings uncomfortable, responses included: “I have to be careful not to have the markings fade,” “they make my clothes dirty,” “color of the markings,” and “the markings are spread across a large area.”
Patients understood skin markings to be necessary and agreed to have them drawn, but the fact that they required attention in daily life and affected clothes or were noticeable likely made them uncomfortable. This is consistent with a report by Akaishi et al on a qualitative study of 13 patients undergoing radiotherapy for the first time.15 Taken together, these findings suggest the need for medical staff to treat patients while recognizing the uncomfortable emotional experiences many patients have about skin markings, despite understanding the need for them. Since methods for skin markings vary from facility to facility, each facility must examine the extent to which their methods of choice – from the range of markings to the characteristics of products used – affect the daily lives of patients from the patient perspective. With recent advances in therapeutic technologies, some facilities have adopted treatment approaches that require no markings,16 or the use of markings which are only visible under a special light.13 While these methods effectively reduce uncomfortable emotional experiences toward skin markings, issues such as costs, education, and development of treatment systems will need to be addressed in order to allow for treatment without skin markings. Thus, it will take some time before many facilities start introducing them.17,18
The proportion of patients who favorably rated skin markings was 64% (59 patients), which was higher than that of those indicating uncomfortable emotional experiences. In radiotherapy, it can be difficult for patients to properly understand the range of irradiation, and they can feel anxious regardless of being treated accurately.10,12 The present study revealed that the range of markings provided a clue to patients as to which parts of the skin they should pay attention to, and gave them peace of mind that treatment is being performed at precise locations. In the future, visual approaches are expected to become available as a means to reduce anxiety, such as the installation of monitors which allow patients to confirm the sites of irradiation, without causing a burden as in the case of skin markings.
Finally, none of the factors assessed in this study influenced the uncomfortable emotional experiences of patients. In considering the impact of markings, it is necessary to understand the patient’s social position, such as his or her role in the household and employment status, as well as his or her cultural background. Compared to non-employed people, employed individuals have more opportunities for personal contact in their social activities, and chances of them experiencing uncomfortable emotional experiences due to others discovering their skin markings are likely higher.19 However, in order to examine the relationship between employment status and uncomfortable emotional experiences toward skin markings, it is necessary to take into account the influence of various factors including internal factors, such as age and medical condition, as well as the type of work and form of employment, place of work, and understanding in the workplace.20–22 We did not obtain this information in the present study, but plan to address these factors in the future. Having skin markings drawn on one’s body may be linked with the awareness of being a cancer patient for those undergoing treatment. This could negatively affect quality of life in some patients, including their self-esteem. Further studies with a larger number of patients with diverse backgrounds will be needed to determine background characteristics which might help identify patients requiring special attention.
In the present study, the questionnaire and explanatory forms were handed to patients by a physician in charge at the radiotherapy department. Thus, even though the physician was not informed of the content of individual responses, patients might have been tempted to provide answers that they thought would please the physician. That is, there is a potential reporting bias due to patients refraining from mentioning the burden of skin markings and/or negative emotional experiences in their responses. In addition, as a specific feature of the study facility, the radiotherapy reception room where the collection box for questionnaires was placed is located in a different building from where the main examination room is. This may have prevented patients from submitting their forms immediately after completing the questionnaire, possibly resulting in a reduced collection rate. In addition, many of the questionnaire items were multiple-choice questions. An additional interview survey might provide a better and more detailed understanding of patients’ emotional experiences toward skin markings.
Conclusion
Among cancer patients receiving radiotherapy, 64% rated skin markings favorably, whereas 56% had uncomfortable emotional experiences about them. Medical staff should understand patients’ emotional experiences toward skin markings and provide explanations, including their impact on daily life, as well as a sense of security that treatment is being performed in a precise manner.
Acknowledgments
We express our sincere gratitude to all participants who cooperated with this study, to the radiation therapists at the studied institutions for their guidance and support, and all involved parties at Kyoto University School of Public Health.
Funding
This study was funded by the operating expenses of the Department of Health Informatics, Kyoto University School of Public Health.
Disclosure
Dr Yukinori Matsuo reports grants from Varian Medical Systems, outside the submitted work. Prof. Dr. Takeo Nakayama reports personal fees from Ohtsuka Pharmaceutical Co., Pfizer Japan Inc., MSD K.K, Chugai Pharmaceutical Co., Takeda Pharmaceutical Co., Janssen Pharmaceutical K.K. Boehringer Ingelheim International GmbH, Eli Lilly Japan K.K., Mitsubishi Tanabe Pharma Co, and Novartis Pharma K.K.; grants from I&H Co., Ltd. And Nakagawa Pharmacy Co., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol. 2015;16(10):1153–1186. doi:10.1016/S1470-2045(15)00222-3
2. Rathod S, Munshi A, Agarwal J. Skin markings methods and guidelines: a reality in image guidance radiotherapy era. South Asian J Cancer. 2012;1(1):27–29. doi:10.4103/2278-330X.96502
3. JASTRO. Japanese radiation oncology database: JROD 2018 working papers. Available from: https://www.jastro.or.jp/medicalpersonnel/data_center/JROD2018.pdf.
4. O’Neill A, McAleer S, McCarty H, et al. Semi-permanent tattoos in breast radiotherapy (STaBRad) study: a randomised-controlled clinical trial comparing the ‘Precision Plus Micropigmentation System’ to permanent skin tattoos in radical breast radiotherapy patients. J Radiother Pract. 2018;17(1):12–19. doi:10.1017/S1460396917000577
5. Townend C, Landeg S, Thorne R, Kirby AM, McNair HA. A review of permanent marking for radiotherapy in the UK. Radiography. 2020;26(1):9–14. doi:10.1016/j.radi.2019.08.003
6. Heyman RE, Baucom KJW, Giresi J, Isaac LJ, Slep AMS. Patient experience and expression of unpleasant emotions during health care encounters. J Patient Exp. 2020;7(6):969–972. doi:10.1177/2374373520978869
7. Wurstbauer K, Sedlmayer F, Kogelnik DH. Skin markings in external radiotherapy by temporary tattooing with henna: improvement of accuracy and increased patient comfort. Int J Radiat Oncol Biol Phys. 2001;50(1):179–181. doi:10.1016/S0360-3016(01)01439-0
8. Marks JG
9. Moser T, Creed M, Walker R, Meier G. Radiotherapy tattoos: women’s skin as a carrier of personal memory-What do we cause by tattooing our patients? Breast J. 2020;26(2):316–318. doi:10.1111/tbj.13591
10. Shaverdian N, Wang X, Hegde JV, et al. The patient’s perspective on breast radiotherapy: initial fears and expectations versus reality. Cancer. 2018;124(8):1673–1681. doi:10.1002/cncr.31159
11. Brandzel S, Rosenberg DE, Johnson D, et al. Women’s experiences and preferences regarding breast imaging after completing breast cancer treatment. Patient Prefer Adherence. 2017;11:199–204. doi:10.2147/PPA.S122244
12. Habibullah G, Gul R, Cassum S, Elahi R. Experiences of the breast cancer patients undergoing radiotherapy at a public hospital Peshawar Pakistan. Asia Pac J Oncol Nurs. 2018;5(2):184–194. doi:10.4103/apjon.apjon_70_17
13. Landeg SJ, Kirby AM, Lee SF, et al. A randomized control trial evaluating fluorescent ink versus dark ink tattoos for breast radiotherapy. Br J Radiol. 2016;89(1068):20160288. doi:10.1259/bjr.20160288
14. Halkett G, O’Connor M, Jefford M, et al. RT Prepare: a radiation therapist-delivered intervention reduces psychological distress in women with breast cancer referred for radiotherapy. Br J Cancer. 2018;118(12):1549–1558. doi:10.1038/s41416-018-0112-z
15. Akaishi M, Fuse Y, Kanda H. Feeling of the patient undergoing radiotherapy for the first time and qualitative study about stress coping behavior. Ann Gunma Health Sci. 2004;25:77–84.
16. Rigley J, Robertson P, Scattergood L. Radiotherapy without tattoos: could this work? Radiography. 2020;26(4):288–293. doi:10.1016/j.radi.2020.02.008
17. Hoisak JDP, Pawlicki T. The role of optical surface imaging systems in radiation therapy. Semin Radiat Oncol. 2018;28(3):185–193. doi:10.1016/j.semradonc.2018.02.003
18. Batista V, Meyer J, Kugele M, Al-Hallaq H. Clinical paradigms and challenges in surface guided radiation therapy: where do we go from here? Radiother Oncol. 2020;153:34–42. doi:10.1016/j.radonc.2020.09.041
19. Nozawa K, Tomita M, Takahashi E, Toma A, Arai Y, Takahashi M. Distress from changes in physical appearance and support through information provision in male cancer patients. Jpn J Clin Oncol. 2017;47(8):720–727. doi:10.1093/jjco/hyx069
20. Sun W, Chen K, Terhaar A, et al. Work-related barriers, facilitators, and strategies of breast cancer survivors working during curative treatment. Work. 2016;55(4):783–795. doi:10.3233/WOR-162449
21. Bae KR, Cho J. Changes after cancer diagnosis and return to work: experience of Korean cancer patients. BMC Cancer. 2021;21(1):86. doi:10.1186/s12885-021-07812-w
22. Main DS, Nowels CT, Cavender TA, Etschmaier M, Steiner JF. A qualitative study of work and work return in cancer survivors. Psychooncology. 2005;14(11):992–1004. doi:10.1002/pon.913
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.