")
Back to Journals » International Journal of Women's Health » Volume 10
Emergency transport for obstetric emergencies: integrating community-level demand creation activities for improved access to maternal, newborn, and child health services in northern Nigeria
Authors Oguntunde O , Yusuf FM, Nyenwa J , Dauda DS , Salihu A, Sinai I
Received 16 July 2018
Accepted for publication 14 September 2018
Published 28 November 2018 Volume 2018:10 Pages 773—782
DOI https://doi.org/10.2147/IJWH.S180415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Olugbenga Oguntunde,1,2 Farouk Musa Yusuf,1,3 Jabulani Nyenwa,1,4 Dauda Sulaiman Dauda,1,2 Abdulsamad Salihu,1,3 Irit Sinai5
1UKAid/Nigeria MNCH2 Programme, Kano, Nigeria; 2Palladium, Abuja, Nigeria; 3Society for Family Health, Abuja, Nigeria; 4Palladium, London, UK; 5Palladium, Washington, DC, USA
Purpose: Ensuring adequate access to skilled birth attendants during and after childbirth is a key strategy to reducing maternal and newborn mortalities. Transportation difficulties in emergency situations continue to be a significant barrier to accessing emergency obstetric care, especially in rural and hard-to-reach areas. Emergency transport schemes (ETS) have been introduced in various settings to increase access to emergency care and reduce the second obstetric delay with varying degrees of success. This qualitative study assessed the perceptions of stakeholders and beneficiaries of ETS in two states in northern Nigeria, comparing two models of ETS: one in which the ETS were introduced as a stand-alone intervention, and another in which ETS were part of a package of interventions for increasing demand and improving utilization of maternal and newborn health services.
Methods: We carried out focus group discussions with ETS drivers, mothers who delivered in the past year and utilized ETS, husbands of women who benefited from the schemes in the past year, health care providers, traditional birth attendants, and religious leaders, supplemented by in-depth interviews with program focal persons.
Results: Demand creation activities – especially working with traditional birth attendants and religious leaders – provided a strong linkage between the ETS and families of women in need of emergency transport services. Community members perceived the ETS model that included demand-generating activities as being more reliable and responsive to women’s needs.
Conclusion: ETS remain a key solution to lack of transport as a barrier to utilizing maternal and newborn health services in emergency situations in many rural and hard-to-reach communities. Programs utilizing ETS to improve access to emergency obstetric care should explore the potential of increasing their utility and reach by integrating the schemes with additional demand-side interventions, especially engagement with traditional birth attendants and religious leaders.
Keywords: emergency transport, maternal health, emergency obstetric care, access, northern Nigeria
Introduction
Health systems in many low- and middle-income countries are characterized by unavailable or nonfunctional emergency medical transport systems. This often means poor access to quality Emergency Obstetric and Newborn Care (EmONC), which is an important determinant of maternal mortality.1 Transport challenges exacerbate the second obstetric delay, ie, delay in getting pregnant women who need EmONC services to the health facility, and may lead to deaths from complications arising from causes of maternal deaths, such as hemorrhage, prolonged obstructed labor, sepsis, and eclampsia.2 An interplay of economic, sociocultural, geographic, and health system factors contributes to the delays and limits women’s access to prompt EmONC services in times of need.3
Barriers to accessing health facilities and trained birth attendants, resulting from transportation difficulties, remain a significant concern.2–4 In many settings where the emergency transport system is managed or provided by the government health system, efforts to transfer women with obstetric complications to health facilities often fail, especially in rural and remote areas, because no vehicles are available, the terrain is difficult, or families cannot afford the associated fees.5–7 This is the case in northern Nigeria, a region characterized by maternal health indictors that are among the poorest in the world. For example, the maternal mortality ratio for Northeast region of Nigeria was recently estimated at 1,549 per 100,000 live births compared with the national figure of 576.8
Emergency transport schemes (ETS) interventions, designed to improve pregnant women’s access to EmONC at health facilities, have been undertaken globally in many underserved communities, usually with positive results.9–12 In northern Nigeria, these schemes often involve collaborations between government departments, development partners, and members of the National Union of Road Transport Workers (NURTW). Pilots began in the mid-1990s.13 Since then, various donor-funded projects scaled up ETS interventions in several states in the region. The Partnership for Reviving Routine Immunization in Northern Nigeria; Maternal Newborn and Child Health Initiative (PRRINN-MNCH) reported nearly 20,000 women transported in their project states.14 The Maternal Newborn and Child Health 2 (MNCH2) Programme, a 5-year DFID-funded technical assistance project running from 2014 to 2019, is scaling up these earlier efforts in six states in northern Nigeria. MNCH2 is adding an additional focus – integrating ETS with various demand creation efforts to increase utilization of maternal and child health services. The current study assessed and compared two approaches to ETS. In the first approach, ETS continue to operate as a stand-alone program as implemented by previous projects. In the second, it is integrated with demand creation activities.
MNCH2 implements the ETS intervention in six northern Nigeria states, to bridge transportation challenges during obstetric emergencies, as part of a package of interventions designed to improve demand for, and increase utilization of maternal and newborn health services. The project’s approach ensures that ETS operate within an integrated demand creation framework at the community level. The full package integrates ETS with demand-generating activities, including establishing women’s and men’s support groups, training traditional birth attendants (TBAs), and sensitizing religious leaders. These elements, which are described in Table 1, are particularly important in the northern-Nigeria environment, because of social and cultural norms that serve as barriers to maternal and child health service utilization in the region.15,16–27
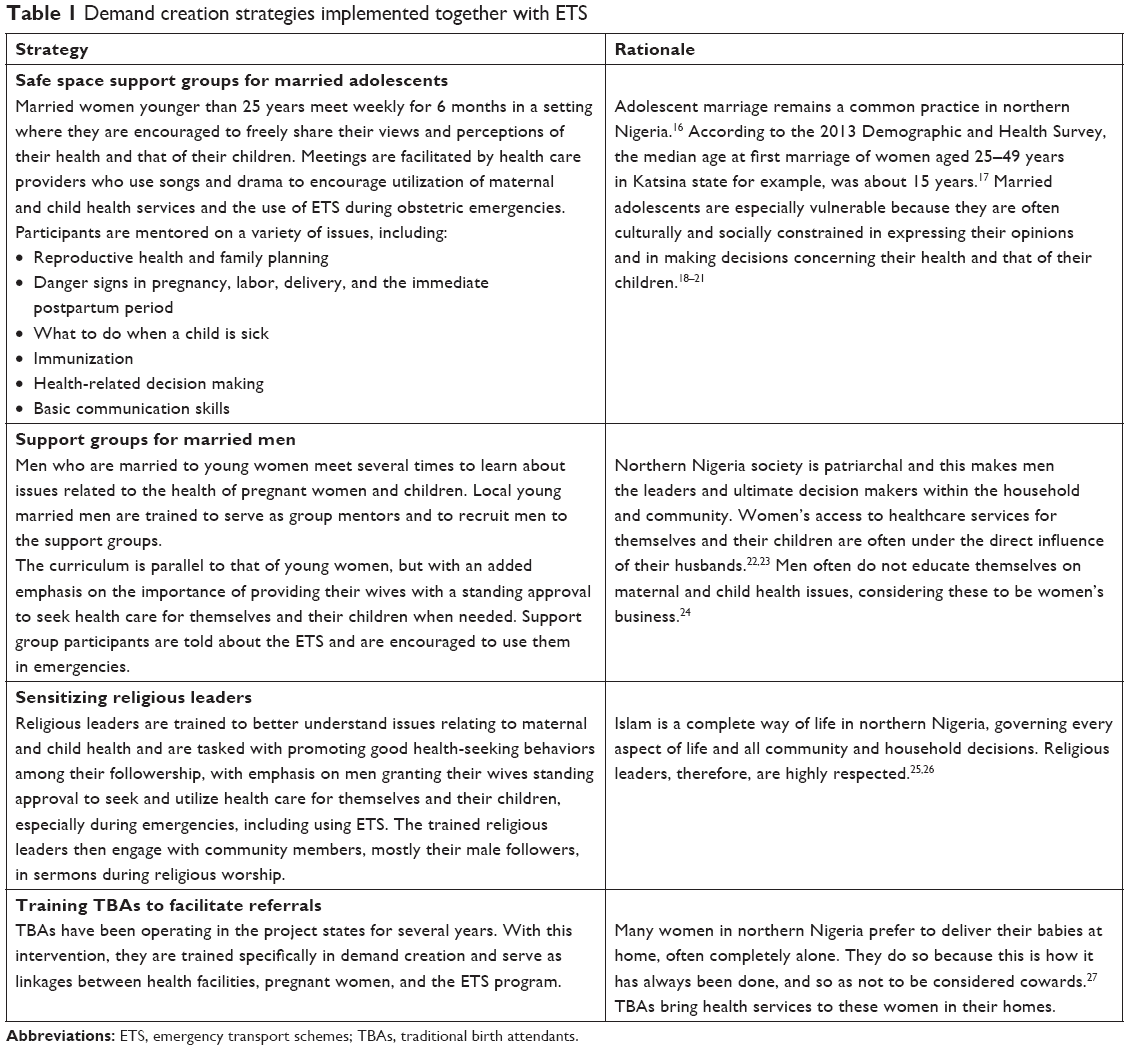 | Table 1 Demand creation strategies implemented together with ETS |
Like its predecessor projects, the MNCH2 program partners with NURTW to identify and recruit volunteer drivers who then participate in a 4-day training workshop on providing emergency transport during obstetric complications in the contexts of their communities. Training sessions utilize a combination of didactic and participatory adult learning approaches that build participants’ capacity on basic skills needed for effective handling and transporting of women with obstetric complications. Participants brainstorm and discuss factors contributing to delays in accessing care for women during obstetric emergencies and how to overcome them. The volunteer drivers are also trained on road safety and regulations and first aid techniques.28
As the program expands geographically, community sensitization and mobilization activities including advocacy meetings with community leaders and community dialog on maternal and child health issues to discuss and highlight problems associated with inadequate access to health facilities also extends to those new program communities. Activities encourage the use of ETS to access EmONC services and promote community ownership of the ETS intervention. These activities further provide opportunities for recruitment of more volunteer drivers from bus stations in each program area. The trained volunteer drivers facilitate the training sessions for these additional drivers.
After the volunteer drivers are judged to be technically competent by post-training tests, including practical driving skills assessment, they begin driving women to health facilities in cases of obstetric emergencies. The only incentive offered ETS drivers, in addition to the training they receive, is priority to load passengers ahead of their colleagues after each successful volunteer emergency trip, instead of joining a queue in bus stations for commercial trips.
The integrated ETS model further involves creating a synergy between the ETS intervention and several demand creation community structures (Table 1) operating in those communities:
- TBAs, religious leaders, members of married men support group, and safe space support groups are provided with contact details of ETS drivers working in their communities;
- Religious leaders talk of the benefits of ETS and other community health resources in their sermons, encouraging utilization and urging their followers to grant their wives standing approvals to access services, especially during emergencies;
- TBAs identify and refer pregnant women in their communities to health facilities for maternal care and contact an ETS driver in case of obstetric complication; and
- Men support group mentors encourage utilization of maternal health services in their communities by advocating for granting standing approvals for women by their husbands to access services at health facilities.
- Representatives of ETS, religious leaders, TBAs, and support groups meet quarterly to review activities and strengthen synergies.
Materials and methods
This qualitative study consisted of focus group discussions and in-depth interviews with various types of stakeholders. We conducted the study in Jigawa and Kaduna, two of the MNCH2 program states. The project began implementing the integrated ETS model in areas where ETS were already operating as a stand-alone activity, as well as in new areas where the project also introduced ETS. This was an extensive effort that needed time to scale up. By the time of field work for this study, some project areas already received the integrated ETS but ETS was still operating as a stand-alone activity in others. This provided the perfect opportunity to compare the two ETS models.
To identify study participants, we created a list of all local government areas (LGAs) where integrated ETS were implemented. We determined that at the time of the study, MNCH2 was implementing integrated ETS interventions in nine out of a total of 23 LGAs in Kaduna state in which ETS were active, and 11 of a total of 27 LGAs with active ETS in Jigawa state. In the remaining LGAs, ETS was operating as a stand-alone activity, without any of the demand-side interventions. Study activities were undertaken in both sets of LGAs.
Focus groups and in-depth interviews with stakeholders
We conducted focus group discussions in both sets of LGAs in each state (those with integrated ETS and those with stand-alone ETS). One focus group was conducted with each of the following types of stakeholders in each set of LGAs in each state, for a total of 24 focus group discussions (Table 2):
- ETS drivers
- Mothers who delivered within the last year and utilized ETS
- Husbands of mothers who delivered within the last year and utilized ETS
- Health care providers from facilities to which ETS refer patients
- TBAs
- Religious leaders
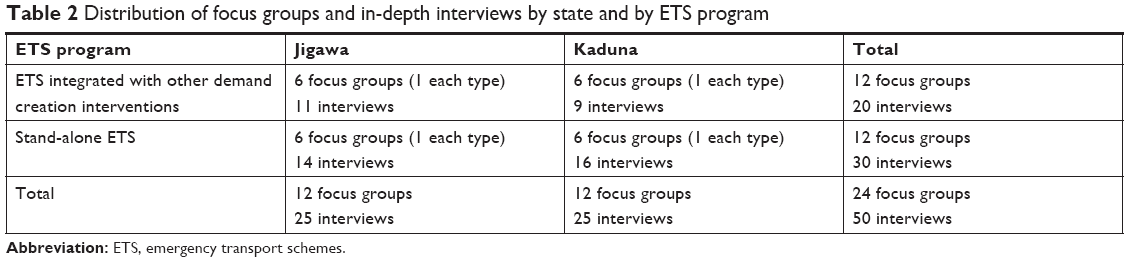 | Table 2 Distribution of focus groups and in-depth interviews by state and by ETS program |
In collaboration with traditional leaders and ETS focal persons, we purposefully selected focus group participants across LGAs within project intervention areas in each state. Focus group discussions revolved around participants’ perceptions of and attitudes toward the current ETS services, if and how schemes can benefit from additional demand-side interventions, the acceptability and utility of expanding ETS to include not only initial transfer from community to facility but also further transport of women who need referral to other health facilities from the initial health facility they are transported to and for children under the age of 5 years to access immunization services (ETS Plus). Between eight and ten participants took part in each focus group. Sessions lasted about 2 hours and were audiorecorded with the consent of participants. Discussions were in participants’ native language of Hausa, in convenient locations where the conversation could not be interrupted, observed, or overheard.
In addition to these focus groups, we conducted in-depth interviews with 50 NURTW LGA Secretaries who served as ETS focal persons, 25 in each state. We asked respondents open-ended questions on their opinions and satisfaction with the current services that ETS provide, how schemes could benefit from additional demand-side interventions, and the feasibility and utility of expanding the intervention. The interviews lasted 60–90 minutes and were audiorecorded with the consent of respondents. As with the focus group discussions, interviews were undertaken in Hausa in convenient locations that offered visual and auditory privacy.
Field work and analysis
Focus group facilitators and note takers, in-depth interview data collectors, and supervisors were individuals with experience in qualitative data collection techniques. They participated in a 3-day training workshop before data collection started. The training focused on study background, objectives, and methodology, as well as review of data collection tools. Additional topics included ethics in research involving human subjects, the rights of participants, and quality assurance issues. The training included practical sessions and role plays highlighting interviewing and facilitation techniques and appropriate community entry approaches. Immediately after the training, the interviewers and facilitators pretested the study instruments in an LGA in Kaduna state that was not sampled for the study because no ETS was implemented there.
Study procedures complied with international and Nigerian guidelines for research with human subjects. The Health Research and Ethics Committees of both participating states approved all study protocols and instruments before fieldwork began. All participants signed a written informed consent form, after all the pertinent information was explained to them and they had the opportunity to ask questions. After data collection was completed, audio recordings from the qualitative interviews and focus groups were transcribed in the local language (Hausa) and subsequently translated to English for analysis.
The qualitative analysis commenced with first page inductive data coding using ATLAS.ti v7. We then analyzed themes and presented codes thematically to develop an emerging story within and across groups, with a focus on comparing stand-alone ETS initiatives with those that were integrated with demand creation activities.
Results
Perspectives of drivers, focal persons, and health providers
Drivers joined the program to save lives.
Because I saw the issue as an opportunity to help, it’s for helping [pregnant women to get to health facility]. [ETS driver, ETS only, Kaduna]
Because of a day I saw a woman beside the road trying to give birth and she died instantly. Ever since then I made up my mind to help. [ETS driver, integrated ETS, Jigawa]
Drivers felt very good about their participation. While some were skeptical about the utility of the program before they joined, they now believed that their volunteer driver status gave them prestige and were excited about saving lives and serving their communities.
Truly, this ETS has helped a lot. Before I joined, I didn’t think it was going to be accepted by the people and that it would be very effective. But when it started, I saw how it has helped. [ETS Driver, ETS only, Kaduna State]
[…] the community makes us feel important. Anytime there is a woman in labor, if you come to pick the woman, not even [only] the people in the house, but the whole area value and respect you. [ETS Driver, integrated ETS, Jigawa]
ETS focal persons similarly agreed that the program is successful in saving lives. They were proud of the drivers for being so dedicated.
It [ETS] has really helped. Back in the days, women weren’t going to the hospital [to deliver their babies], but now the case is different, it has helped in saving the lives of women and babies. [Focal person, integrated ETS, Jigawa]
[…] they [drivers] are putting much effort […] any time they are called upon, they make themselves available, day or night. [Focal person, ETS only, Jigawa]
Health providers also uniformly praised the ETS.
Personally, I believe in the program, […] I pray God gives strength [to] this program to continue. [Health care provider, integrated ETS, Kaduna]
The beneficiary perspective
Beneficiaries of the ETS program – both women who used the program and their husbands – had only good things to say about ETS. They strongly felt that introducing ETS in their respective communities had improved access to emergency care during pregnancy and childbirth.
It [ETS] has really helped women. Immediately we get to know that a woman is in labor and she is bleeding, we immediately call the driver to come take her to the hospital […] yes, it is a success. [Woman, integrated ETS, Kaduna]
[…] in the past women are backed, grabbed and carried while in labor because of scarcity of vehicles […] But with this initiative [ETS], the drivers are very gentle with the women. [Husband of beneficiary, ETS only, Jigawa state]
Women and their husbands heard about the availability of ETS in their communities from a variety of sources. Most heard about the program from friends and relatives. One respondent talked about how the wife of their community’s ETS driver told other women about it. In communities with integrated ETS, some respondents heard about the program from religious leaders during a sermon or a religious celebration or from TBAs who were called to help women with their pregnancies.
TBAs and ETS
TBAs are typically older women, who are very well respected in the community. They are perceived as the first helpline for women and their families when the woman is in labor or experiences pregnancy complications.
When there are issues that pertain to childbirth, they are the first people that are called. [ETS Driver, integrated ETS, Kaduna]
TBAs who were trained by MNCH2 create demand for obstetric services by advocating for facility use for maternal and reproductive health. When a TBA who attends a home delivery advises that the woman needs urgent care at a health facility, the family is more likely to agree because of TBAs’ respected position in the community. ETS beneficiaries and their husbands agreed that in cases of difficult deliveries, TBAs facilitate referral to the hospital by calling an ETS driver and in some cases convincing husbands and family members to accept the free services of ETS to convey the woman with complications to the health facility. Both women and their husbands praised TBAs’ role in the community and their advocacy for ETS in case of emergencies.
If you have these elderly women (TBAs) around, they know if there is a problem, they are the ones that get the driver or tell your husband to call the driver to take you to the hospital. [Woman, integrated ETS, Kaduna]
In the TBA focus groups, participants confirmed that they counsel women on the need for antenatal services and help pregnant women deliver their babies safely. They also encourage husbands and families to utilize the ETS when they observe danger signs of pregnancy or childbirth. The TBAs themselves were very thankful for the existence of the ETS program. They call drivers in cases of emergency and introduce them to the woman and her husband.
If anybody wants to deliver and the situation is beyond me, I would advise them to let us call a driver. [TBA, ETS only, Kaduna]
Sincerely, if I don’t go into partnership with drivers, women will suffer. If we see that the delivery is beyond our control, we quickly call drivers to come and take the woman to the hospital for her to be safe. [TBA, integrated ETS, Kaduna]
While TBAs contribution to increased utilization of ETS program is clear in places where they were trained to do so as part of the integrated demand creation intervention, the picture is mixed in areas where ETS operate as a stand-alone activity. On the contrary, because TBAs had been active in the community prior to the current intervention, some have been advocating for ETS use even if they were not trained as part of this intervention. Therefore, we see praise for TBAs role in ETS utilization also in communities where ETS was implemented as a stand-alone intervention, but more so in areas with the integrated intervention.
[…] when a woman is in labor, they [TBAs] are the first responders. […] and when they arrive, they hurriedly look for a vehicle and the people doing this [ETS]. [Husband of beneficiary, ETS only, Kaduna]
Many drivers in stand-alone ETS areas have never heard of TBAs working with the ETS or were not aware that TBAs can contribute to the ETS program. They could list a few TBAs working in their communities but emphasized that they do not work with them on the ETS scheme.
The TBAs are also not involved; we work directly with the community people. [Focal person, ETS only, Kaduna]
Honestly, I told you I don’t have knowledge about this [TBAs working with ETS] because it’s not my line, what I know is how they [TBAs] bring a woman to the hospital and how they help her. [Focal person, ETS only, Jigawa]
Religious leaders and ETS
Religious leaders support the ETS program because of their desire to help their communities and their respect for the work the ETS drivers are doing.
Religiously, it is encouraged that one should use what he has to help others and that is the reason why those people [ETS drivers] have been doing what they are doing diligently. Those who have cars have been doing their best on this program and when we were informed about it, we came into it and began to contribute our quota, we are happy for it. [Religious leader, integrated ETS, Kaduna]
Our results confirm the importance of religious leaders in northern Nigerian society. Following their training for the demand-side intervention, they now advocate for women to attend health facilities when they have an obstetric emergency.
Religious leaders are playing a vital role……; they enlighten their followers in the mosque, in places of gathering, in the church, they tell the women what to do […] even when the husband is not around and something happens, they advise the women to call for help and not wait. [ETS focal person, integrated ETS, Kaduna]
There is this group […] their mosque is over there, for about four months now, I heard the Imam preaching about child birth. I overheard him mentioning helping pregnant women in giving life, so this is another way they help. [ETS Driver, integrated ETS, Jigawa]
It is because of their influence in the community that religious leaders can contribute to expanding demand for obstetric care. They also increase utilization by advocating for use of ETS in times of need.
[…] they often preach to people […] and in the process, they make them understand the importance of the [ETS] program. [ETS Driver, integrated ETS, Jigawa]
The integrated approach
The full umbrella of demand creation activities included support groups for young married women and for married men, training of TBAs, and working with religious leaders. In all focus groups and interviews, TBAs and religious leaders were touted as being a very positive influence on increasing demand for maternal and child health services and increased utilization of ETS. There was little spontaneous mention of the support groups. Yet, when asked directly about them, most participants agreed that they can be helpful in increasing demand for and utilization of maternal health services, including use of ETS.
Women groups are very important because they mentor the pregnant woman about how to care for the baby. [Focal person, integrated ETS, Jigawa]
When asked which of the demand creation activities is most beneficial in increasing utilization of the ETS, and by extension of EmONC in health facilities, the overwhelming response by ETS drivers and focal persons was the TBAs.
The TBAs usually come to check on women in labor immediately their attention is called. They advise husbands or relatives on what to do when they observe signs of complication. [ETS Driver, integrated ETS, Jigawa]
They are mostly women, they know more than us, they know families that often have such issues [complications] during child birth or issues relating to infant illnesses. As such, they advise families to call us [for transport to health facility]. [ETS Driver, integrated ETS, Kaduna]
The TBAs are the ones that render more help […], when problems arise during child birth and you call them, no matter the time of the day or night, they will come to your house to give you the assistance needed. [Focal person, ETS only, Kaduna]
In Jigawa, participants added that TBAs are very committed to the services they provide. Several respondents attributed this to the fact that TBAs are very happy with being part of the demand-side initiative which has strengthened their capacity to serve their communities better:
The TBAs are really pleased with the program because of the knowledge and skills that they acquired through trainings, thus they give their maximum co-operation to the program and render help whenever it is called for. [Focal person, integrated ETS, Jigawa]
ETS plus
The current ETS were designed only to transport women from their home or community to a health facility in case of emergency. Across all sites and intervention types, drivers and focal persons agreed that there often is an additional need to take women from one health facility to another based on referral. Drivers explained that they usually already do this – they take pregnant women to other facilities to which they are referred, even though this arrangement is not part of the current ETS program. To do so, they wait around after delivering her to the initial health facility until they receive instructions from the health care provider on next steps, before they depart the health facility.
They said she should further be transferred to [Name of facility]. They put her (back) in my car and I took her to [Name of facility] without wasting time. By God’s grace, she delivered safely. [ETS Driver, integrated ETS, Kaduna]
There is a set rule that when you take a pregnant woman on ETS, you wait until you are sure the newborn is fine and the mother is fine. If there is one or two problems and the doctor says you should wait, you wait. If he makes referral, then you must take the woman to the new hospital she has been referred to. This is not a problem. [Focal Person, integrated ETS, Kaduna]
Most ETS drivers similarly supported transporting newborn babies delivered at home and who had complications to the health facility. However, most drivers would not transport older children for immunization or other child health services. In both integration- and stand-alone-ETS, drivers were adamant that they would not transfer children for immunization. They suggested that parents should arrange and pay for transporting their under-five children to the health facility to get immunized:
This is among the things that we are asked to do [transporting children]. If it’s a new baby that has complications, we pick and transport them to the hospital. [ETS Driver, integrated ETS, Kaduna]
[…] we are more concerned about sick babies. For immunization, they [parents] should try and get a vehicle. [Health worker, integrated ETS, Kaduna]
Facilitators and barriers to the ETS intervention
Most focus group participants across stakeholders identified the dedication and selflessness of drivers as a key facilitator to the success of the ETS. Focal persons praised the drivers; health providers were impressed by the commitment with which ETS drivers conduct the ETS work and their willingness to respond to the need of the community without being paid; beneficiaries and their husbands were extremely thankful.
What really impressed me about the drivers is their level of commitment. Whenever they are called to take a patient to the hospital, they respond immediately, be it in the morning or night. [Health care Provider, ETS only, Jigawa State]
The integrated approach employed by the program was identified as a strong lever of support that creates community awareness and strengthens cohesion among community members in the prevention of maternal mortality. However, some challenges were identified to the operations of the ETS. Most drivers and focal persons identified security challenges as a significant barrier, given that they often drive women at night.
I won’t forget [the experience] of one of my drivers that once took a woman in labor to the health facility […] in the night. Thieves attacked them on the way, forced them to stop [;;], laid them flat on the ground and they collected the little money that the woman’s husband had on him. [Focal person, integrated ETS, Kaduna state].
In some communities, drivers also reported not being issued with identification materials that they can use to identify themselves as ETS drivers when on duty as a challenge. Apparently, some health facilities do not readily admit women brought by the ETS drivers because the drivers do not have the means to identify themselves as volunteer drivers for the program.
[…] at times when […] you come with a sick person, they [health workers] may not respond to you on time and this is because you don’t have an ID card. [ETS Driver, Integrated ETS, Jigawa]
Other factors, including inadequate numbers of volunteer drivers and vehicles to increase coverage of the intervention, as well as poor road conditions, and the occasional incidence in which a husband would not let the driver transport his wife, were also mentioned as barriers to optimal utilization of ETS to increase access to EmONC.
Discussion
The need for interventions to remove barriers that delay women’s access to prompt EmONC services has been identified as critical to preventing maternal deaths.4,29,30 In the last two decades, development projects around the world, especially in developing countries, have implemented interventions designed to address these delays, with varied results. In northern Nigeria, the MNCH2 ETS initiative is currently being delivered within an integrated package of demand creation activities to increase demand for and use of maternal and child health services.
Recognizing that perceptions of community members about the utility of interventions is key to ownership and use of the services the intervention offers, this study explored the perceptions of various stakeholders and beneficiaries regarding the performance of the ETS initiative, comparing the integrated approach with the original stand-alone approach to ETS.
Our findings show that the ETS interventions play an important role in improving access to EmONC services at health facilities. These findings confirm positive results from assessments of ETS interventions elsewhere.11–13 The study further revealed the high potential for ETS success, when combined with additional demand-side interventions, as affirmed by the level of awareness, approval, and use of the ETS in communities where demand-side interventions were implemented with the ETS.
The integrated demand-side intervention galvanized support and sensitized communities toward a common goal of maternal mortality prevention in their communities. For care seekers, the integrated ETS was perceived as more effective, and all ETS stakeholders similarly perceived and reported that ETS utilization of maternal and child health services had increased considerably in some communities where ETS operated with additional demand-side interventions. Therefore, an ETS intervention integrated with demand-side activities has the potential to significantly increase EmONC service utilization, especially working with TBAs and religious leaders.
The current ETS were designed to only transport women from their home or community to a health facility. Focus groups with ETS drivers revealed that drivers go beyond that to also transport newborn babies to facilities in cases of emergencies and to transport women to other facilities when referred. However, drivers are not willing to transport children to health facilities for nonemergency medical needs such as immunization. Considering the pivotal role of immunization in child survival, it is pertinent that measures are taken to bridge the access gap in immunization services for young children. This may be achieved through expanding the ETS services to encompass not only emergency services but also transporting under 5 years to the health facility for routine immunization. Reinforcement of child health messages, and perhaps incentivizing drivers to transport children for immunization, may therefore further improve the utility of ETS for child health.
Other works have documented that getting women who need EmONC services to health facilities may not be sufficient to avert maternal deaths, due to obstetric complications, understaffing, insufficient training and equipment, and other supply-side concerns at the facility.31,32 One barrier to facility utilization identified by our study is difficulties in being admitted to the facility when transported by an ETS driver. We therefore recommend that programs implementing ETS ensure that all drivers are provided with a means of identification such as an identity card, vest, or cap. This would facilitate prompt admission and initiation of services, after the woman is successfully transported to the facility. Other possible bottlenecks that may be present at the facility must be identified and addressed.
A limitation of our study is that participants were mainly individuals who may be biased in support of the program and therefore expressed more positive views in favor of ETS success. ETS drivers and focal persons are proud of their work and are more likely to provide positive feedback; women and their husbands who participated in the study had benefited from the program – it may have saved their lives or that of their wives or children – and therefore are more likely also to have positive views. We did not conduct focus groups with women who had not used ETS services for comparison. More research is needed to assess the effect of the intervention at the community level, especially as part of the full umbrella of demand creation activities. Yet, results consistently suggest that the ETS program, especially in combination with demand creation activities, can improve EmONC utilization and save lives.
Conclusion
This study demonstrated that implementing the ETS within an integrated community framework can promote a positive perception of the ETS among community members, increasing utilization and improving access to emergency obstetric services in health facilities. It would be useful for other MNCH implementers and policy makers to consider integrating ETS with demand-side interventions in future scale-up plans. This will facilitate greater involvement and participation of communities and improve ease of implementation of the schemes. Ultimately, scaling up the ETS in northern Nigeria and elsewhere together with other community activities to promote ETS utilization will improve health outcomes.
Acknowledgments
All work related to this study was funded by aid from the UK government through the Department for International Development’s UKAid/Nigeria MNCH2 Programme (PO 6468). The views expressed are the authors’ and do not necessarily reflect the UK government’s official policies.
Disclosure
The authors report no conflicts of interest in this work.
References
Nour NM. An introduction to maternal mortality. Rev Obstet Gynecol. 2008;1(2):77–81. | ||
Holmes W, Kennedy E [webpage on the Internet]. Reaching emergency obstetric care: overcoming the “second delay,” Burnet Institute. Available from: https://www.burnet.edu.au/publications/3465_reaching_emergency_obstetric_care_overcoming_the_second_delay. Accessed May 3, 2018. | ||
Ellis C, Schummers L, Rostoker J-F. Reducing maternal mortality in Uganda: applying the “three delays” framework. Int J Childbirth. 2011;1(4):218–226. | ||
Nyamtema AS, Mwakatundu N, Dominico S, et al. Enhancing maternal and perinatal health in under-served remote areas in sub-saharan Africa: a Tanzanian model. PLoS One. 2016;11(3):e0151419. | ||
Jammeh A, Sundby J, Vangen S. Barriers to emergency obstetric care services in perinatal deaths in rural Gambia: a qualitative in-depth interview study. ISRN Obstet Gynecol. 2011;2011:1–10. | ||
Echoka E, Makokha A, Dubourg D, Kombe Y, Nyandieka L, Byskov J. Barriers to emergency obstetric care services: accounts of survivors of life threatening obstetric complications in Malindi District, Kenya. Pan Afr Med J. 2014;17(Suppl 1):4. | ||
Koşum Z, Yurdakul M. Factors affecting the use of emergency obstetric care among pregnant women with antenatal bleeding. Midwifery. 2013;29(5):440–446. | ||
African Population and Health Research Center [webpage on the Internet]. Maternal Health in Nigeria: Facts and Figures. Available from: http://aphrc.org/post/publications/maternal-health-nigeria-facts-figures. Accessed May 3, 2018. | ||
Sabde Y, de Costa A, Diwan V. A spatial analysis to study access to emergency obstetric transport services under the public private “Janani Express Yojana” program in two districts of Madhya Pradesh, India. Reprod Health. 2014;11:57. | ||
Schmid T, Kanenda O, Ahluwalia I, Kouletio M. Transportation for maternal emergencies in Tanzania: empowering communities through participatory problem solving. Am J Public Health. 2001;91(10):1589–1590. | ||
Hofman JJ, Dzimadzi C, Lungu K, Ratsma EY, Hussein J. Motorcycle ambulances for referral of obstetric emergencies in rural Malawi: do they reduce delay and what do they cost? Int J Gynaecol Obstet. 2008;102(2):191–197. | ||
Ehiri J, Alaofè H, Asaolu I, Chebet J, Esu E, Meremikwu M. Emergency transportation interventions for reducing adverse pregnancy outcomes in low- and middle-income countries: a systematic review protocol. Syst Rev. 2018;7(1):65. | ||
Shehu D, Ikeh AT, Kuna MJ. Mobilizing transport for obstetric emergencies in northwestern Nigeria. The Sokoto PMM Team. Int J Gynaecol Obstet. 1997;59(Suppl 2):S173–S180. | ||
PRINN-MNCH. Emergency Transport Schemes for Prevention of Maternal Mortality; 2013. Available from: www.prrinn-mnch.org/documents/PRRINN-MNCH3EmergencyTSSummary.pdf. Accessed April 27, 2018. | ||
Sinai I, Anyanti J, Khan M, Daroda R, Oguntunde O. Demand for women’s health services in northern Nigeria: a review of the literature. Afr J Reprod Health. 2017;21(2):96–108. | ||
Braimah TS. Child marriage in Northern Nigeria: Section 61 of Part I of the 1999 Constitution and the protection of children against child marriage. Afr Hum Rights Law J. 2014;14(2):474–488. | ||
National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International; 2014. | ||
Kahlid S [database on the Internet]. Socio-Economic and Cultural Roots of Reproductive Healthcare problems in Northwestern Nigeria. Available from: http://www.gamji.com/article6000/news6048.htm. Accessed May 3, 2018. | ||
Lane C, Joof YM, Hassan AA, Pryor S. Promoting healthy timing and spacing of pregnancy with young married women in Northern Nigeria: a short report. Afr J Reprod Health. 2012;16(2):263–269. | ||
Rai RK, Singh PK, Singh L. Utilization of maternal health care services among married adolescent women: insights from the Nigeria Demographic and Health Survey, 2008. Womens Health Issues. 2012;22(4):e407–e414. | ||
Godswill J. Adolescents’ sexual and reproductive health challenges in northern Nigeria: road map to effective interventions. Int Lett Soc Humanistic Sci. 2014;24:1–11. | ||
Shamaki MA, Buang A. Sociocultural practices in maternal health among women in a less developed economy: an overview of Sokoto State, Nigeria. Geografia. Malaysian. J Soc Space. 2014;10(6):1–14. | ||
Kaye DK, Kakaire O, Nakimuli A, Osinde MO, Mbalinda SN, Kakande N. Male involvement during pregnancy and childbirth: men’s perceptions, practices and experiences during the care for women who developed childbirth complications in Mulago Hospital, Uganda. BMC Pregnancy Childbirth. 2014;14:54. | ||
Iliyasu Z, Abubakar IS, Galadanci HS, Aliyu MH. Birth preparedness, complication readiness and fathers’ participation in maternity care in a northern Nigerian community. Afr J Reprod Health. 2010;14(1):21–32. | ||
Mairiga AG, Kyari O, Kullima A, Abdullahi H. Knowledge, perceptions and attitudes of Islamic scholars towards reproductive health programs in Borno State, Nigeria. Afr J Reprod Health. 2007;11(1):98–106. | ||
Abdul NM, Anose M, Ibrahim MT. An analysis of the socio-economic, socio-cultural, religious, environmental, technological, language and educational factors on women’s right in Nigeria: the case of Northern Nigeria; 2012. Available from: www.nawey.net/wp-content/plugins/download-monitor/download.php?id=28. Accessed May 3, 2018. | ||
Doctor HV, Findley SE, Ager A, et al. Using community-based research to shape the design and delivery of maternal health services in Northern Nigeria. Reprod Health Matters. 2012;20(39):104–112. | ||
NURTW. Training manual: Emergency transport schemes. Abuja: Nigeria. Available from: http://www.prrinn-mnch.org/documents/EmergencytransportschememanualforNURTW_2013.pdf. Accessed July 15, 2018. | ||
Erim DO, Kolapo UM, Resch SC. A rapid assessment of the availability and use of obstetric care in Nigerian healthcare facilities. PLoS One. 2012;7(6):e39555. | ||
Wilson A, Hillman S, Rosato M, et al. A systematic review and thematic synthesis of qualitative studies on maternal emergency transport in low- and middle-income countries. Int J Gynaecol Obstet. 2013;122(3):192–201. | ||
Pitchforth E, van Teijlingen E, Graham W, Dixon-Woods M, Chowdhury M. Getting women to hospital is not enough: a qualitative study of access to emergency obstetric care in Bangladesh. Qual Saf Health Care. 2006;15(3):214–219. | ||
Knight HE, Self A, Kennedy SH. Why are women dying when they reach hospital on time? A systematic review of the ‘third delay’. PLoS One. 2013;8(5):e63846. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.