")
Back to Journals » OncoTargets and Therapy » Volume 11
Elevated urinary 8-oxo-7,8-dihydro-2'-deoxyguanosine and serum uric acid are associated with progression and are prognostic factors of colorectal cancer
Authors Mao L , Guo C, Zheng S
Received 25 May 2018
Accepted for publication 8 August 2018
Published 17 September 2018 Volume 2018:11 Pages 5895—5902
DOI https://doi.org/10.2147/OTT.S175112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Takuya Aoki
Lingna Mao,1,2 Cheng Guo,1 Shu Zheng1
1Cancer Institute, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2General Practice Department, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Background and purpose: Oxidative stress is closely related to the pathogenesis of colorectal cancer (CRC). 8-Oxo-7,8-dihydro-2'-deoxyguanosine (8-oxodG) is a typical biomarker of oxidative stress. Serum uric acid (SUA) is one of the most abundant molecules with antioxidant properties in human blood. This study aimed to explore whether 8-oxodG and SUA could be prognostic factors of CRC.
Methods: Urinary 8-oxodG level was analyzed using ultrahigh performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS). SUA concentration was measured using an automatic biochemistry analyzer. Seventy-three newly diagnosed Chinese CRC patients were included. According to the mean level of urinary 8-oxodG or SUA, patients were divided into high and low groups.
Results: The level of 8-oxodG and SUA gradually elevated from stage I to stage IV in CRC patients. High 8-oxodG concentration and SUA levels were associated with worse overall survival (P=0.03). In the stage II and stage III CRC group, no statistically significant relationship was found between the urinary 8-oxodG level and overall survival or between the SUA level and overall survival. Nevertheless, when these two biomarkers were combined, there was a statistically significant association with overall survival (P=0.02).
Conclusion: Elevated urinary 8-oxodG and SUA levels measured at the time of diagnosis were associated with the progression of CRC. Both urinary 8-oxodG and SUA might be valuable as CRC prognostic factors, and the combination of the two biomarkers might help to determine the prognoses of CRC, particularly in stage II and stage III CRC patients.
Keywords: colorectal cancer, urinary 8-oxo-7, 8-dihydro-2'-deoxyguanosine, serum uric acid, oxidative stress, prognostic factor
Introduction
Colorectal cancer (CRC) is the third most common cancer in men and the second in women worldwide.1 The incidence of CRC is still rising in People’s Republic of China.2 Oxidative stress is involved in the pathogenesis of CRC. 8-Oxo-7,8-dihydro-2′-deoxyguanosine (8-oxodG), as a typical biomarker of oxidative stress, also plays a role in carcinogenesis.3,4 In our recently published article,5 we observed elevated levels of urinary 8-oxodG in CRC patients with tumor metastasis, but did not reach a conclusion about the association between urinary 8-oxodG and CRC mortality or CRC prognosis, due to a shortage of follow-up data.
Serum uric acid (SUA) is known as one of the most abundant molecules with antioxidant properties in human blood and acts as a free radical scavenger and a chelator of transitional metal ions.6,7 SUA not only may play a protective role against cancer but also may function as a pro-oxidant and contribute to tumorigenesis by entering normal cells and promoting tumor cell proliferation, migration, and survival, assisted by ROS and inflammatory stress.8 Many epidemiological studies have investigated the cancer protective hypothesis but provided inconsistent findings. Meta-analysis reported by Yan et al9 concluded that a high SUA level increased the risk of total cancer incidence and cancer mortality. All the abovementioned studies put emphasis on the association between SUA and overall cancer incidence/mortality but not on the association between SUA and CRC or on the association between SUA and CRC prognosis.
There are ethnic differences in oxidative stress between the Chinese and the Caucasian. Studies have shown that the Chinese are more susceptible than the Caucasian to free radical damage caused by diet.10 There are different genetic polymorphisms between the Chinese and the Caucasian in DNA repair enzymes related to the pathogenesis and development of CRC.11,12 Since diet and genetic background are two important factors related to the pathogenesis of CRC, they may partly explain the different development and prognosis of CRC in different ethnics. Studies conducted by Dziaman et al13 revealed that 8-oxodG and uric acid can serve as predictors of survival in Caucasian CRC patients, while there is no related information about Chinese patients.
In this study, for the first time, we analyzed the overall survival and levels of urinary 8-oxodG and SUA and explore the association between these two biomarkers and the progression/prognosis of CRC in a Chinese population.
Methods
Study population
This study was approved by the institutional review board of Medical Research, the Second Affiliated Hospital, Zhejiang University School of Medicine (SAHZU). All the experiments were carried out in accordance with the approved guidelines.
Seventy-three CRC patients enrolled in the study were followed up between March 2011 and December 2017. The mean follow-up time was 64 months (range: 12–70). All participants were Han Chinese, and there were no relatives among them. The date of diagnosis, age, gender, body mass index (BMI), histological type of tumor, disease stage (according to TNM classification, using numerals I, II, III, and IV to describe the progression of cancer), and biochemical markers at diagnosis for all patients were reviewed. Patients were divided into four groups according to tumor stage. All individuals participating in the study were recruited through SAHZU. All subjects signed written informed consent prior to participation.
Inclusion criteria: all patients recruited had pathologically diagnosed adenocarcinoma and had not been treated with abdominal operation, chemotherapy, or radiotherapy. Patients with a history of other malignant tumor(s), diabetes mellitus, metabolic syndrome, rheumatologic diseases, hematological malignancies, alcoholism, gout, previous chemotherapy, and/or radiotherapy applications; patients who had acute coronary syndrome or cerebrovascular diseases within the past 6 months; patients on medication for hyperuricemia; and patients without an SUA level were excluded from the study.
Blood samples for laboratory analysis were drawn following an 8- to 12-hour fasting period. SUA and serum creatinine levels were measured at the time of diagnosis. Overnight spot urine samples were collected for measurement of 8-oxodG at the time of diagnosis.
Measurement of urinary 8-oxodG
After urine collection, the samples were frozen immediately and stored at −80°C in the dark until analysis. Urinary 8-oxodG levels were measured using ultrahigh performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) analysis combined with a solid-phase extraction procedure. To provide a correction factor for urine concentration, aliquots of urine supernatant were also assayed for creatinine. The urinary 8-oxodG level was normalized with creatinine concentration and is presented as nmol of 8-oxodG/mmol of creatinine. This method has been described in a previous publication.5
Measurement of SUA and serum creatinine
SUA levels were determined by the urate peroxidase coupling method using an automatic biochemistry analyzer (AU5831; Beckman Coulter, CA, USA). The normal value of SUA for males is 208–428 μmol/L, and for females it is 154–357 μmol/L. Serum creatinine was determined by the sarcosine oxidase methods using the same biochemistry analyzer used to determine the SUA levels. The normal value of serum creatinine is 40–106 μmol/L for males and 44–88 μmol/L for females.
Statistical analyses
All the statistical analyses were performed using SPSS statistics version 18.0 (SPSS Inc., Chicago, IL, USA). Concentrations of SUA, urinary 8-oxodG, and characteristics of the study population in different cancer stages were compared using one-way ANOVA and chi-squared test (for categorical data).
Survival was analyzed by using Kaplan–Meier curves and the log-rank test. In survival analysis, urinary 8-oxodG and SUA concentrations were re-formatted as two-class variables using the mean level as a cutoff point. Thus, survival rate comparison was made between patients in the high value group (with urinary 8-oxodG or SUA concentration ≥ mean value) and patients in the low value group (with urinary 8-oxodG or SUA concentration below the mean value). Cox proportional hazard model was established to estimate the differences in survival among different factors, including SUA, 8-oxodG, age, BMI, serum creatinine, and stage. Statistical tests were two-sided, and P<0.05 was considered to indicate a statistically significant difference.
Results
Characteristics of the study population
Demographic and clinical characteristics of the study population are summarized in Table 1. Subjects were divided into four groups according to pathological TNM (pTNM) classification. There were totally 73 pathologically diagnosed CRC patients (38 colon adenocarcinomas and 35 rectal adenocarcinomas), of whom, 13, 20, 28, and 12 patients were classified into stages I–IV, respectively. No patient received colorectal surgery, chemotherapy, or radiotherapy before participating in this study. The mean age of all patients was 62.5 years (range: 25–87). The average concentration of urinary 8-oxodG and SUA was 1.64±0.77 nmol/mmol creatinine and 309.0±76.6 μmol/L, respectively. By the end of the study period, 19 patients had died due to CRC, metastasis, or other reasons, and the overall survival rate was 74%.
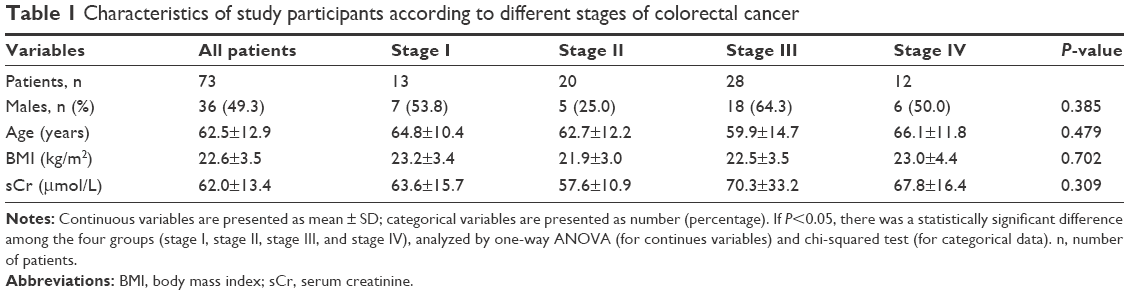 | Table 1 Characteristics of study participants according to different stages of colorectal cancer |
Association of urinary 8-oxodG and SUA with tumor progression
Urinary 8-oxodG (Figure 1A) and SUA levels (Figure 1B) gradually increased from stages I to IV in CRC patients. As shown in Figure 1A, the average concentration of 8-oxodG in stages I, II, III, and IV is 0.91±0.45, 1.57±0.55, 1.69±0.74, and 2.16±0.89 nmol/mmol creatinine, respectively. As shown in Figure 1B, the average concentration of SUA in stages I, II, III, and IV is 272±67.6, 275.5±46.8, 334.5±70.8, and 358.5±88.6 μmol/L, respectively. There were significant differences among four tumor stages in the distribution of urinary 8-oxodG and SUA. Both P-values were 0.0002 (one-way ANOVA), indicating that oxidative stress increased systematically with CRC disease progression.
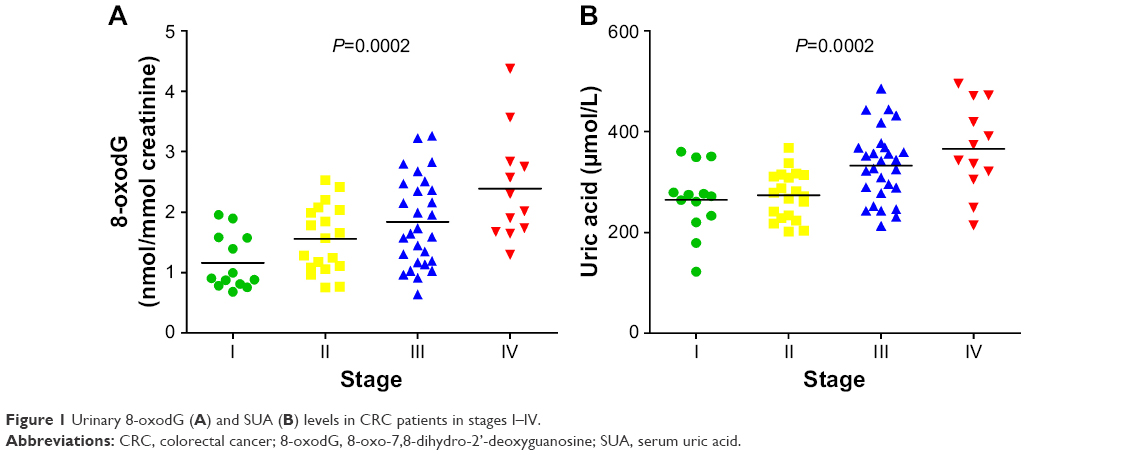 | Figure 1 Urinary 8-oxodG (A) and SUA (B) levels in CRC patients in stages I–IV. |
Survival analysis
The overall survival probability at 60 months (OSP60) is 75%. Patients were divided into two groups according to the mean value: one group of patients with urinary 8-oxodG/SUA levels above or equal to the mean value (high value group) and one group with levels below the mean value (low value group). A survival comparison was made between the high value and low value groups. In the whole study sample, high urinary 8-oxodG (Figure 2A, P=0.03) and SUA levels (Figure 2B, P=0.03) were associated with worse overall survival. Patients with a high urinary 8-oxodG level did not survive as long as patients with a low 8-oxodG level (Figure 2A, OSP60=64% vs OSP60=89%), and patients with a high SUA level did not survive as long as patients with a low SUA level (Figure 2B, OSP60=64% vs OSP60=88%). When combining urinary 8-oxodG and SUA, we found that patients with low urinary 8-oxodG and SUA levels lived longer than those with high urinary 8-oxodG and SUA levels (OSP60=100% vs OSP60=70%, P=0.03; Figure 2C).
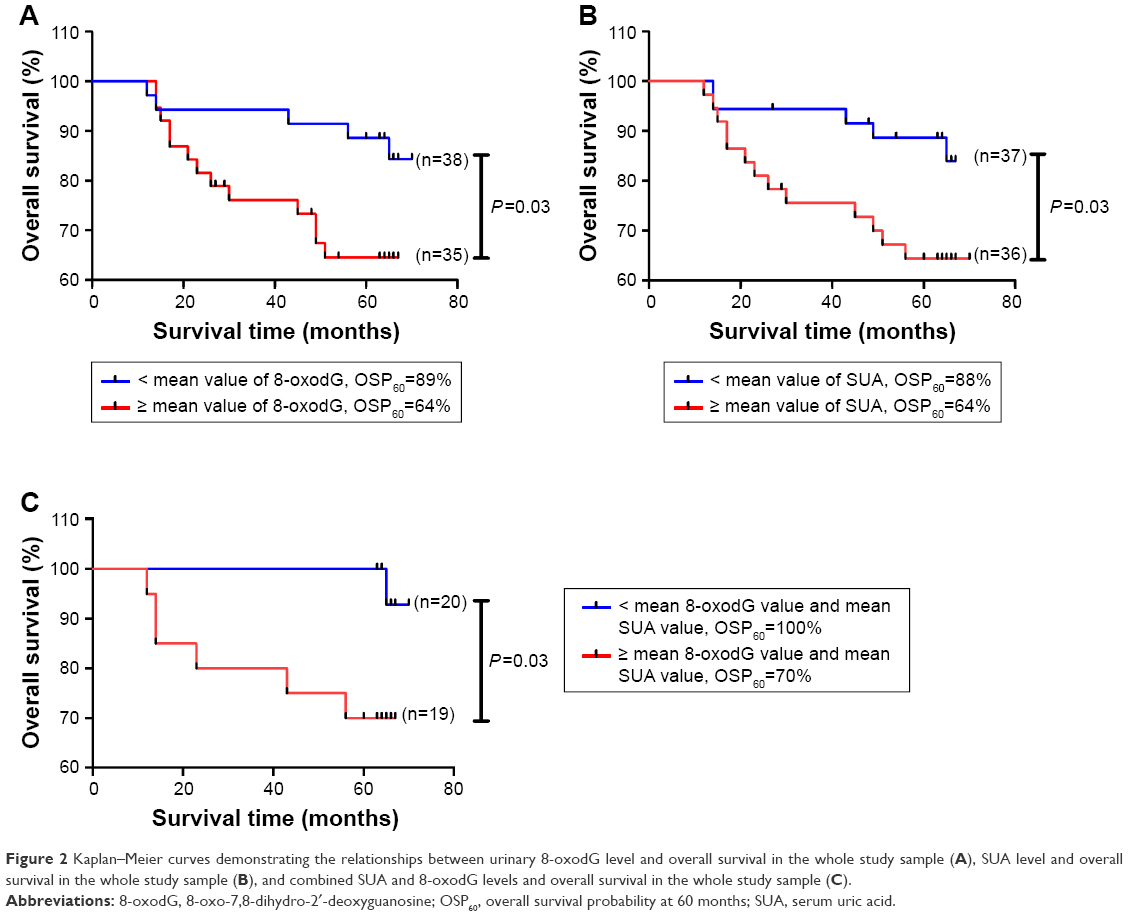 | Figure 2 Kaplan–Meier curves demonstrating the relationships between urinary 8-oxodG level and overall survival in the whole study sample (A), SUA level and overall survival in the whole study sample (B), and combined SUA and 8-oxodG levels and overall survival in the whole study sample (C). |
There were 48 patients in stage II (n=20) and stage III (n=28); no statistically significant relationship was found between urinary 8-oxodG level (Figure 3A, P=0.2) or SUA level (Figure 3B, P=0.45) and overall survival. Patients in stage II seemed to live longer than patients in stage III, but there was no statistically significant difference between these two stages (Figure 3D, P=0.05). When combining 8-oxodG with SUA, there was a statistically significant relationship between the two markers’ content and overall survival (Figure 3C, P=0.02), and more patients lived 60 months in the low value group than in the high value group (OSP60=89% vs OSP60=62%, Figure 3C). Compared with TNM staging (Figure 3D, P=0.05), the combination of urinary 8-oxodG and SUA seemed to be more effective in determining CRC prognosis in stage II and stage III patients (Figure 3C, P=0.02). This implies that combining urinary 8-oxodG and SUA may provide better prognostic value in CRC than the individual biomarkers.
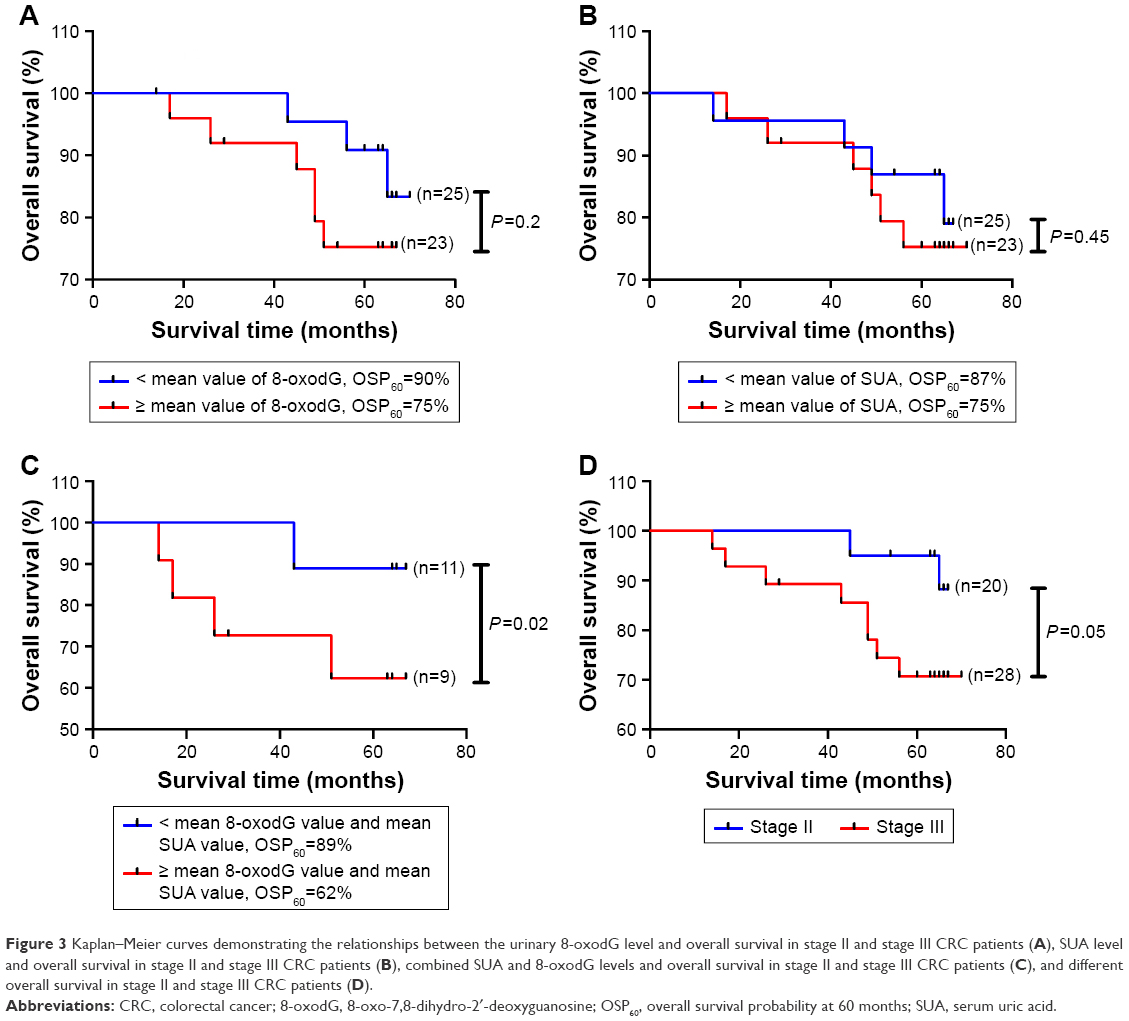 | Figure 3 Kaplan–Meier curves demonstrating the relationships between the urinary 8-oxodG level and overall survival in stage II and stage III CRC patients (A), SUA level and overall survival in stage II and stage III CRC patients (B), combined SUA and 8-oxodG levels and overall survival in stage II and stage III CRC patients (C), and different overall survival in stage II and stage III CRC patients (D). |
In order to evaluate the correlation of the survival of CRC patients with respect to the SUA level, urinary 8-oxodG level, tumor stage, BMI, age, and serum creatinine level, the Cox regression model was established (Table 2). In this model, the values of SUA and 8-oxodG are set as 0 when their levels are lower than the average values, or else they are set as 1. The results showed that stage (P=0.003), SUA (P=0.004), and 8-oxodG (P=0.006) were significantly associated with the survival of CRC. This implied that stage, SUA, and 8-oxodG could be prognostic factors of CRC.
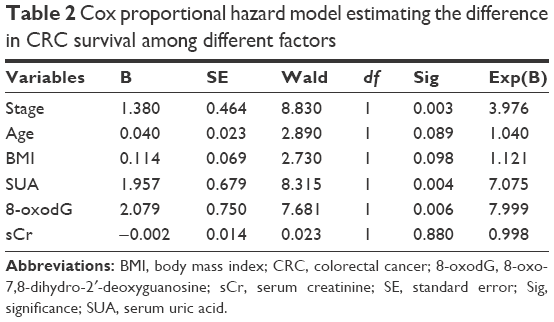 | Table 2 Cox proportional hazard model estimating the difference in CRC survival among different factors |
Discussion
In this study, we examined the urinary 8-oxodG and SUA levels in patients with CRC without treatment and followed the patients for 64 months on average. To exclude the effect of kidney function on the urinary 8-oxodG level, we examined the serum creatinine level of all participants, and there were no statistically significant differences among the patients in the four stages of CRC (Table 1). We found that the level of urinary 8-oxodG and SUA gradually increased from stage I to stage IV (Figure 1) in CRC patients and that there were significant differences among the four cancer stages of patients with respect to 8-oxodG and SUA concentrations (Figure 1, P<0.01). This indicates that the oxidative DNA damage becomes more serious as CRC progresses, and the levels of urinary 8-oxodG and SUA can reflect the severity of CRC. This implied that the increased level of 8-oxodG and SUA may be adverse prognostic factors of CRC. In other studies about the association between the oxidative stress and CRC,14–16 the emphasis was all put on the question whether oxidative stress could be pathogenic/prognostic factors to CRC, but not on the association between oxidative stress and the whole process of CRC development. So, this is a new discovery of this study that urinary 8-oxodG and SUA can reflect the severity of CRC, and in that case they may help to evaluate the therapy effect and estimate the prognosis of CRC.
Although pathological staging is well known as the gold standard for determining CRC prognosis, even patients within the same stage demonstrate quite different clinical outcomes. This is particularly important for CRC patients in stages II and III: the survival rates of CRC patients in stages I and IV are comparatively stable and easier to predict, but in patients with stages II and III CRC, TNM staging less clearly distinguishes groups of patients with different prognoses, with 5-year overall survival between 50% and 90%.17 Hence, in this study, we put more focus on CRC patients in stages II and III. Oxidative stress has been proved to be involved in the pathogenesis and progression of CRC and other cancers.3,18,19 In our previous study,5 oxidative stress (8-oxodG level) was found to be elevated in the early stage of CRC, and in this study we found that it was intensified during disease progression. So, it is possible that biomarkers of oxidative stress together with pathological staging could be helpful in predicting clinical outcomes more precisely.
In the whole study sample, a significant increase in overall survival was found in patients with low urinary 8-oxodG and/or SUA level (Figure 2A–C). In CRC patients in stage II (20) and stage III (28), the overall survival rates were higher in the low 8-oxodG and SUA group than in the high 8-oxodG and SUA group (Figure 3A and B). When combining urinary 8-oxodG and SUA, the overall survival difference between the high value and low value groups was even more significant (Figure 3C, P=0.02). This result is partly consistent with the conclusion drawn by Dziaman et al13 that a combination of low levels of 8-oxodG and high levels of SUA had a more significant predictive power than a single biomarker. Nevertheless, the results that the overall survival rates were higher in the low SUA group in this study is opposite to that of Dziaman et al. In their study, they found that the overall survival was higher in patients with high levels of SUA and low levels of 8-oxodG. Such difference between the two studies may be due to the ethnic variability and the different role that SUA plays in the progression of CRC. It is postulated that the Chinese population are more susceptible than Caucasian to free radical damage caused by diet.10 Due to the different gene polymorphisms modified by race, the Chinese CRC patients have not shown higher DNA repair activity than the Caucasian. So, it is reasonable that the elimination of DNA damage in the Chinese CRC patients is incomplete and hence the oxidative stress biomarkers (such as SUA) increase more than the Caucasian during the disease progression.
Excretion of 8-oxodG in urine represents the average rate of oxidative stress/DNA damage in the whole body. Although it is still not clear if increased oxidative stress/damaged DNA plays a role in carcinogenesis or is merely a result of tumor development, it has been proved by many studies and in this study that the level of urinary 8-oxodG reflected the severity of tumor progression.20–22 In this study, we further proved that urinary 8-oxodG is helpful in predicting the overall survival of CRC patients. Oxidative stress is closely linked with chronic inflammation, and there are several studies demonstrating that inflammation-related factors may be associated with the pathological staging of the tumor or may be tumor stage-independent prognostic factors.23 The pro-oxidative environment may not only confer a growth advantage to tumor cells but it may also influence carcinogenic potential by stimulating specific signaling cascades that regulate cell growth and apoptosis.24 Therefore, it is reasonable that urinary 8-oxodG can serve as a prognostic factor to CRC, but the quantitative relationship between oxidative stress/DNA damage and CRC is still unclear and needs further exploration.
There is evidence that SUA, as an important antioxidant in human, is inversely correlated with oxidative damaged DNA and may also be a predictor of survival in CRC patients.4,25,26 A cohort study of 354,110 participants in Taiwan, conducted by Kuo et al,27 supported the hypothesis that uric acid is cancer protective because it suggested that low SUA levels were associated with a higher risk of all cancer mortality. Conversely, a cohort study of 8,274 participants in People’s Republic of China found that the incidence of cancer increased with SUA levels, but only in females with diabetes.28 A cohort study of 493,281 individuals in Sweden found a positive association between uric acid levels and overall cancer risk, but an inverse association for pulmonary and central nervous system (CNS) cancers in men and breast, lymphatic, and hematological, and CNS malignancies in women.29 This study showed that elevated SUA concentration was associated with the progression of CRC (Figure 1B), and high levels of SUA predicted worse prognosis than low levels. These results seem to conflict with the antioxidant role of SUA, while in fact, there is inconsistency concerning the anti/pro-oxidant role that SUA plays in human cancer progress. In physiological concentration, uric acid is a main antioxidant;30 in the late stages of tumors, it has been shown that increased cell death accompanied elevated levels of uric acid as dying tumor cells release uric acid.31,32 In addition, in very high concentrations (about 420 μmmol/L), uric acid may trigger inflammation.33 Therefore, SUA is associated with the progression and prognosis of CRC. SUA, together with urinary 8-oxodG, is helpful in identifying high-risk CRC patients. But, how it functions as an anti/pro-oxidant during CRC progression in different ethnics needs further exploration.
As far as we know, this study is the first to show the association between these two biomarkers and CRC progression in the Chinese population. We found that elevated levels of urinary 8-oxodG and SUA can reflect the severity of CRC. But, there were limitations in this study. Due to the strict inclusion criteria, there was a limited sample size. Although our mean follow-up time for the enrolled patients was 64 months, we need to validate our results in a longer follow-up time. In addition, the results of this study need to be further verified on the cell and molecular levels by laboratory research work.
Conclusion
Elevated urinary 8-oxodG and SUA levels measured at the time of diagnosis were associated with the severity of CRC. Both urinary 8-oxodG and SUA may serve as CRC prognostic factors and are helpful in identifying more high-risk CRC patients. The combination of these two biomarkers may help determine the prognoses of CRC, particularly in stage II and stage III CRC patients.
Acknowledgment
This study was supported by the Foundation of Education Department of Zhejiang Province (Y201534681 and Y201636729) and Zhejiang Medical and Health Science and Technology Plan Project (2017KY373).
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | ||
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA: A Cancer J Clin. 2016;66(2):115–132. | ||
Tudek B, Speina E. Oxidatively damaged DNA and its repair in colon carcinogenesis. Mutat Res. 2012;736(1–2):82–92. | ||
Xie Y, Yang H, Cunanan C, et al. Deficiencies in mouse Myh and Ogg1 result in tumor predisposition and G to T mutations in codon 12 of the K-ras oncogene in lung tumors. Cancer Res. 2004;64(9):3096–3102. | ||
Guo C, Li X, Wang R, et al. Association between Oxidative DNA Damage and Risk of Colorectal Cancer: Sensitive Determination of Urinary 8-Hydroxy-2′-deoxyguanosine by UPLC-MS/MS Analysis. Sci Rep. 2016;6:32581. | ||
Glantzounis GK, Tsimoyiannis EC, Kappas AM, Galaris DA. Uric acid and oxidative stress. Curr Pharm Des. 2005;11(32):4145–4151. | ||
Kang DH, Ha SK. Uric acid puzzle: dual role as anti-oxidant and pro-oxidant. Electrolyte Blood Press. 2014;12(1):1–6. | ||
Fini MA, Elias A, Johnson RJ, Wright RM. Contribution of uric acid to cancer risk, recurrence, and mortality. Clin Transl Med. 2012;1(1):16. | ||
Yan S, Zhang P, Xu W, et al. Serum Uric Acid Increases Risk of Cancer Incidence and Mortality: A Systematic Review and Meta-Analysis. Mediators Inflamm. 2015;2015:764250–7. | ||
Yim J, Petrofsky J, Berk L, et al. Protective effect of anti-oxidants on endothelial function in young Korean-Asians compared to Caucasians. Med Sci Monit. 2012;18(8):CR467–CR479. | ||
Kohno T, Shinmura K, Tosaka M, et al. Genetic polymorphisms and alternative splicing of the hOGG1 gene, that is involved in the repair of 8-hydroxyguanine in damaged DNA. Oncogene. 1998;16(25):3219–3225. | ||
Perera FP. Environment and cancer: who are susceptible? Science. 1997;278(5340):1068–1073. | ||
Dziaman T, Banaszkiewicz Z, Roszkowski K, et al. 8-Oxo-7,8-dihydroguanine and uric acid as efficient predictors of survival in colon cancer patients. Int J Cancer. 2014;134(2):376–383. | ||
Gackowski D, Banaszkiewicz Z, Rozalski R, Jawien A, Olinski R. Persistent oxidative stress in colorectal carcinoma patients. Int J Cancer. 2002;101(4):395–397. | ||
Obtułowicz T, Swoboda M, Speina E, et al. Oxidative stress and 8-oxoguanine repair are enhanced in colon adenoma and carcinoma patients. Mutagenesis. 2010;25(5):463–471. | ||
Yuan C, Xu XH, Wang XL, Xu L, Chen Z, Li YQ. Relationship between serum uric acid and metastatic and nonmetastatic rectal cancer patients with undergoing no chemotherapy. Medicine. 2016;95(47):e5463. | ||
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Mantovani A, Bussolino F, Dejana E. Cytokine regulation of endothelial cell function. Faseb J. 1992;6(8):2591–2599. | ||
Guo C, Ding P, Xie C, et al. Potential application of the oxidative nucleic acid damage biomarkers in detection of diseases. Oncotarget. 2017;8(43):75767–75777. | ||
Leung EY, Crozier JE, Talwar D, et al. Vitamin antioxidants, lipid peroxidation, tumour stage, the systemic inflammatory response and survival in patients with colorectal cancer. Int J Cancer. 2008;123(10):2460–2464. | ||
Ll W, Chiou CC, Chang PY, et al. Urinary 8-oxodG: a marker of oxidative stress to DNA and a risk factor for cancer, atherosclerosis and diabetics. Clinica Chimica Acta. 2004;339(2):1–9. | ||
Cao C, Lai T, Li M, et al. Smoking-promoted oxidative DNA damage response is highly correlated to lung carcinogenesis. Oncotarget. 2016;7(14):18919–18926. | ||
Leitch EF, Chakrabarti M, Crozier JE, et al. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br J Cancer. 2007;97(9):1266–1270. | ||
Benhar M, Engelberg D, Levitzki A. ROS, stress-activated kinases and stress signaling in cancer. EMBO Rep. 2002;3(5):420–425. | ||
Foksinski M, Gackowski D, Rozalski R, et al. Effects of basal level of antioxidants on oxidative DNA damage in humans. Eur J Nutr. 2007;46(3):174–180. | ||
Yang J, Wang Y, Zhao Q, et al. Association of serum uric acid with increased risk of cancer among hypertensive Chinese. Int J Cancer. 2017;141(1):112–120. | ||
Kuo CF, See LC, Yu KH, Chou IJ, Chiou MJ, Luo SF. Significance of serum uric acid levels on the risk of all-cause and cardiovascular mortality. Rheumatology. 2013;52(1):127–134. | ||
Deng Z, Gu Y, Hou X, et al. Association between uric acid, cancer incidence and mortality in patients with type 2 diabetes: Shanghai diabetes registry study. Diabetes Metab Res Rev. 2016;32(3):325–332. | ||
Yiu A, van Hemelrijck M, Garmo H, et al. Circulating uric acid levels and subsequent development of cancer in 493,281 individuals: findings from the AMORIS Study. Oncotarget. 2017;8(26):42332–42342. | ||
Sevanian A, Davies KJ, Hochstein P. Conservation of vitamin C by uric acid in blood. J Free Radic Biol Med. 1985;1(2):117–124. | ||
Shi Y, Evans JE, Rock KL. Molecular identification of a danger signal that alerts the immune system to dying cells. Nature. 2003;425(6957):516–521. | ||
Hu DE, Moore AM, Thomsen LL, Brindle KM. Uric acid promotes tumor immune rejection. Cancer Res. 2004;64(15):5059–5062. | ||
Shi Y. Caught red-handed: uric acid is an agent of inflammation. J Clin Invest. 2010;120(6):1809–1811. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.