")
Back to Journals » International Journal of General Medicine » Volume 14
Elevated Nesfatin-1 Level in Synovium and Synovial Fluid is Associated with Pro-Inflammatory Cytokines in Patients with Rheumatoid Arthritis
Authors Zhang S, Rong G, Xu Y, Jing J
Received 19 July 2021
Accepted for publication 24 August 2021
Published 7 September 2021 Volume 2021:14 Pages 5269—5278
DOI https://doi.org/10.2147/IJGM.S330099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shuo Zhang,1 Genxiang Rong,2 Yayun Xu,3 Juehua Jing1
1Department of Orthopedics, The Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Orthopedics, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Epidemiology and Biostatistics, School of Public Health, Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Juehua Jing
Department of Orthopedics, The Second Affiliated Hospital of Anhui Medical University, 678 Furong Road, Hefei, Anhui, 230032, People’s Republic of China
Email [email protected]
Background: Adipocytokines have been proven to be involved in the progression of autoimmune diseases, including rheumatoid arthritis (RA). Nesfatin-1, a newly discovered adipokine, has recently been reported to possess potent anti-inflammatory, antiapoptotic, and antioxidative properties. However, its role in RA has not yet been reported. Therefore, this study aimed to determine nesfatin-1 levels in the synovium and synovial fluid (SF) of patients with RA and examine their correlation with clinical manifestations and proinflammatory cytokine levels.
Methods: Synovium and SF samples were collected from patients with RA and non-RA patients during joint surgery. Immunohistochemistry was used to measure nesfatin-1 protein expression in the synovium. Enzyme-linked immunosorbent assay was used to measure nesfatin-1, interleukin-1β (IL-1β), and tumor necrosis factor-α (TNF-α) levels in the synovium and SF. Pearson correlation analysis was used to evaluate the correlations between nesfatin-1 levels, RA clinical features, and proinflammatory cytokines. The diagnostic value of synovium nesfatin-1 for RA was assessed using receiver operating characteristic (ROC) curve analysis.
Results: The results showed that nesfatin-1, IL-1β, and TNF-α levels in the synovium were significantly higher in patients with RA than in controls, with age and body mass index as covariates. Moreover, the results of Pearson correlation analysis showed that nesfatin-1 levels were positively correlated with IL-1β and TNF-α levels in the synovium of patients with RA. Furthermore, there was a positive relationship between synovium nesfatin-1 levels and rheumatoid factor in patients with RA. Additionally, the results of the ROC curve analysis revealed an area under the curve of 0.733 with 77.5% sensitivity and 60.0% specificity for synovium nesfatin-1 in discriminating patients with RA from controls.
Conclusion: These findings suggest that increased nesfatin-1 levels in the synovium may be associated with proinflammatory cytokines and RA severity.
Keywords: rheumatoid arthritis, adipocytokine, nesfatin-1, synovium, synovial fluid, pro-inflammatory cytokines
Introduction
As a chronic, autoimmune inflammatory type of arthritis, rheumatoid arthritis (RA) affects approximately 1% of the adult population worldwide.1 The clinical features of RA mainly include leukocyte infiltration and synovial hyperplasia, which cause chronic joint inflammation as well as subsequent cartilage and bone erosion.2 Although a number of treatment options have been used over the last few decades to improve the signs and symptoms, including inflammation, most patients with RA continue to experience joint damage, disability, and serious illness due to its unknown etiology.3 Therefore, an in-depth understanding of the pathogenesis of RA will be of great significance and may facilitate the identification of new therapeutic targets. Additionally, the current clinical diagnosis of RA relies on patient symptoms and laboratory blood testing, such as rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPAs). However, the RF-positive rate and ACPA-specificity of RA are only 60–70% and 60–75%, respectively, suggesting low diagnostic efficacy.4 Thus, there has been growing interest in the identification of new biomarkers to improve the diagnostic accuracy of RA.
Evidence has accumulated in support of the regulatory roles of adipocytokines in the pathogenesis of RA.5,6 Adiponectin, leptin, and resistin levels are reportedly elevated in both blood and synovial fluid (SF) of patients with RA compared to those in controls.7–9 Nesfatin-1, a novel adipocytokine derived from the precursor protein nucleobindin-2,10 is widely expressed in both central (such as the hippocampus, hypothalamus, amygdala, and prefrontal cortex) and peripheral (such as the esophagus, stomach, small intestine, colon, pancreas, liver, adipocytes, cardiomyocytes, testes, ovaries, uterus, and epididymis) tissues.11,12 Nesfatin-1 has recently been reported to possess potent anti-inflammatory, antiapoptotic, and antioxidative properties.13 Recent evidence has revealed a marked association of serum and SF nesfatin-1 concentrations with osteoarthritis disease severity,14 indicating that nesfatin-1 may contribute to the pathophysiological changes in osteoarthritis. However, synovium and SF levels of nesfatin-1 and their relationship with disease severity in patients with RA have not yet been reported.
The imbalance between proinflammatory and anti-inflammatory cytokine activities is conducive to inducing autoimmunity, chronic inflammation, and joint injury in RA.15 Extensive evidence exists suggesting that synovial inflammation and the resultant proinflammatory mediators are directly implicated in the pathogenesis of RA, promoting synovial proliferation, hyperplasia, and angiogenesis.16 More recently, the potential anti-inflammatory activity of nesfatin-1 has been demonstrated in several studies. Nesfatin-1 has been reported to suppress interleukin-1β (IL-1β)-induced activation of nuclear factor kappa B in chondrocytes.17 Moreover, the peripheral use of nesfatin-1 has demonstrated anti-inflammatory effects in subarachnoid hemorrhage and brain injury cases.18,19 Given that nesfatin-1 exhibits potential anti-inflammatory activity in a variety of inflammatory diseases, the relationship between nesfatin-1 and proinflammatory cytokines in the synovium and SF of RA patients was also investigated.
Considering the dysfunction of chronic synovial inflammation in RA, together with the potential anti-inflammatory activity of nesfatin-1, we hypothesized that nesfatin-1 levels in the synovium and SF undergo changes in patients with RA and that this is potentially associated with the overproduction of proinflammatory cytokines. To test this hypothesis, patients with RA and non-RA patients were selected from patients hospitalized at the First Affiliated Hospital of Anhui Medical University. Synovium and SF samples were collected, and enzyme-linked immunosorbent assay (ELISA) was used to measure nesfatin-1, IL-1β, and tumor necrosis factor-α (TNF-α) levels. Pearson correlation analysis was used to evaluate the correlations between nesfatin-1 levels, RA clinical features, and proinflammatory cytokines. The diagnostic value of synovium nesfatin-1 for RA was assessed using receiver operating characteristic (ROC) curve analysis.
Materials and Methods
Patients and Samples
Synovium and SF samples were obtained from patients with RA (n = 40) who were diagnosed with RA and had undergone joint surgery at the First Affiliated Hospital of Anhui Medical University. All patients with RA fulfilled the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism criteria or the 1987 ACR criteria.20,21 Patients suffering from local cartilage damage or traumatic joint lesions (sport injuries) were regarded as the control group, and synovium samples from the control group (n = 15) were collected during joint surgery. Patients with autoimmune or infectious diseases were excluded from the control group. All patients provided written informed consent prior to participation, in accordance with the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of Anhui Medical University.
Measurements
A demographic questionnaire was used to collect general information from study participants, including age, body mass index (BMI), sex, X-ray classification, time of pain, anti-cyclic peptide containing citrulline (anti-CCP), antistreptolysin O (ASO), rheumatoid factor (RF), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and 28-Joint Disease Activity Score based on ESR (DAS28-ESR). Synovium and SF samples were collected during joint surgery and immediately transferred to liquid nitrogen before storage in a freezer at −80 °C until use. Commercially available ELISA kits were used to measure the concentrations of nesfatin-1, IL-1β, and TNF-α (Jianglai Bio, Shanghai, China), according to the manufacturer’s instructions.
Immunohistochemistry Staining
Due to limitations in the available and small sample volume, 5 synovium samples in each group were harvested, fixed in 4% paraformaldehyde for 48 h, and embedded in paraffin. Serial sections (4 μm) were cut. Immunohistochemistry for nesfatin-1 was performed using the SP-9000 Histostain-Plus kit (ZSGB Bio, China), according to the manufacturer’s instructions. Samples were visualized using a digital pathology slide scanner (3DHISTECH Ltd., The Digital Pathology Company, Budapest, Hungary). Image-ProPlus Software (Media Cybernetics, Silver Spring, MD, USA) was used to calculate the integral optical density of the sections.
Statistical Analysis
Data were analyzed using SPSS (version 17.0; IBM Corp., Armonk, NY, USA). Data are expressed as the mean ± standard error of the mean (SEM), and statistical significance was set at P< 0.05. A one-sample Kolmogorov–Smirnov test revealed a normal distribution of continuous variables. Student’s t-test was used to evaluate differences in age and BMI between the groups. The χ2 test was used to analyze sex differences between groups. Analysis of covariance (ANCOVA) was performed to compare differences in the synovium levels of nesfatin-1, IL-1β, and TNF-α between the two groups, controlling for age and BMI by using these variables as covariates. Correlation analyses were performed using Pearson’s correlation test.
Results
Demographic Values and Routine Laboratory Parameters of the RA and Control Groups
As shown in Table 1, there were no significant differences in sex between the two groups (χ2 = 0.284, P = 0.594). However, age (t = –5.586, P< 0.001) and BMI (t = 3.323, P = 0.002) were significantly higher in patients with RA than in controls.
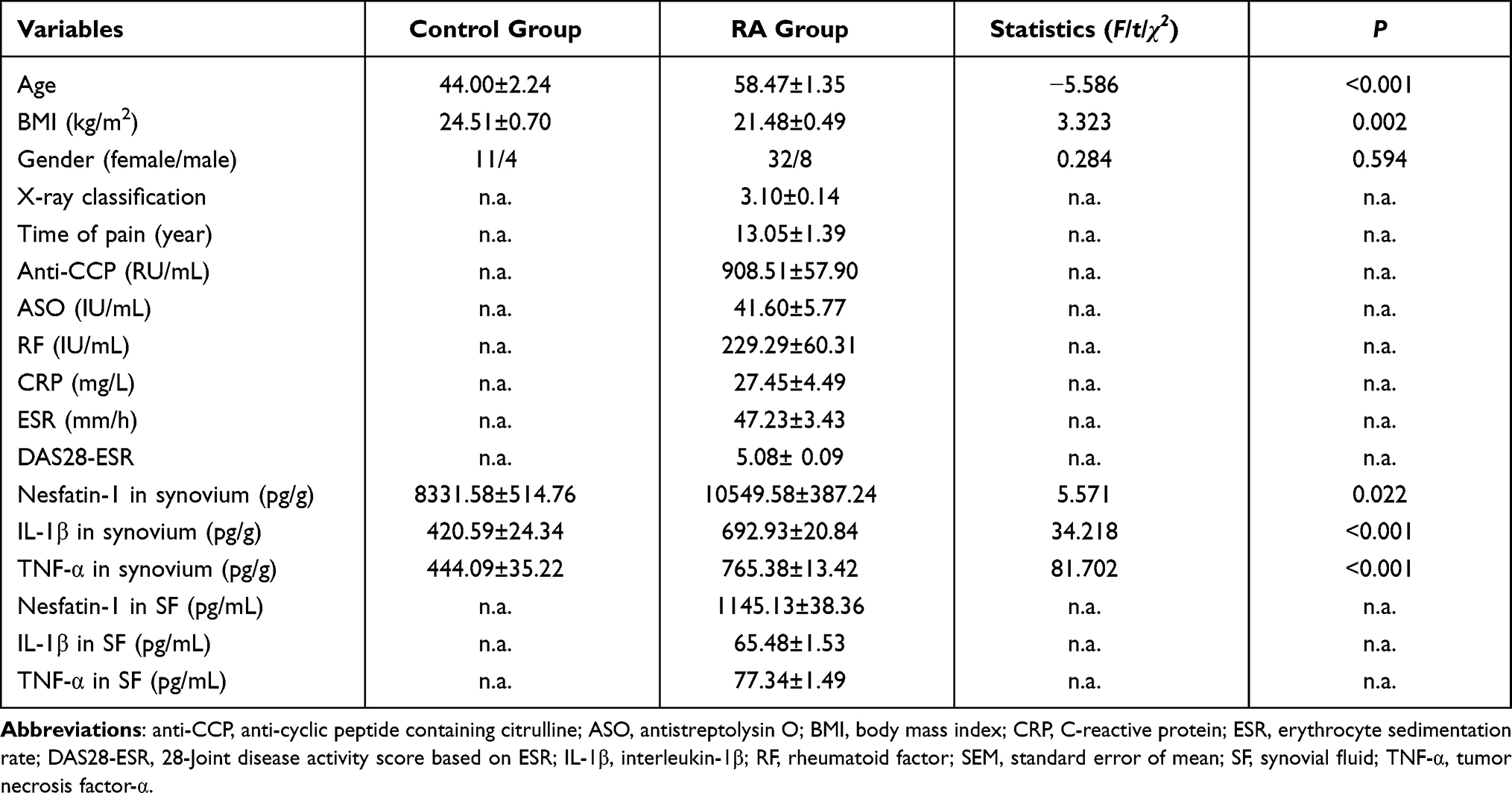 |
Table 1 Comparison of Mean Values (or Ratios) of Demographic Data, Nesfatin-1, IL-1β, and TNF-α Levels in Synovium and SF Between the RA and Control Groups (Mean ± SEM) |
Patients with RA exhibited an average X-ray classification of 3.10 ± 0.14, with a reported time of pain ranging from 1 to 30 years (mean 13.05 ± 1.39 years). The serum CCP, ASO, RF, and CRP levels of patients with RA were 908.51 ± 57.90 RU/mL, 41.60 ± 5.77 IU/mL, 229.29 ± 60.31 IU/mL, and 27.45 ± 4.49 mg/L, respectively. The ESR and DAS28-ESR of patients with RA were 47.23 ± 3.43 mm/h and 5.08± 0.09, respectively (Table 1).
Nesfatin-1, IL-1β, and TNF-α Levels in the Synovium of the RA and Control Groups
As shown in Table 1, ANCOVA results demonstrated that nesfatin-1 levels in the synovium were significantly higher in patients with RA than in controls, with age and BMI as covariates (F = 5.571, P = 0.022). Similarly, immunohistochemistry results also revealed that the level of nesfatin-1 in the synovium was significantly higher in the RA group than that in the control group (t = −6.414, P< 0.001; Figure 1A and B).
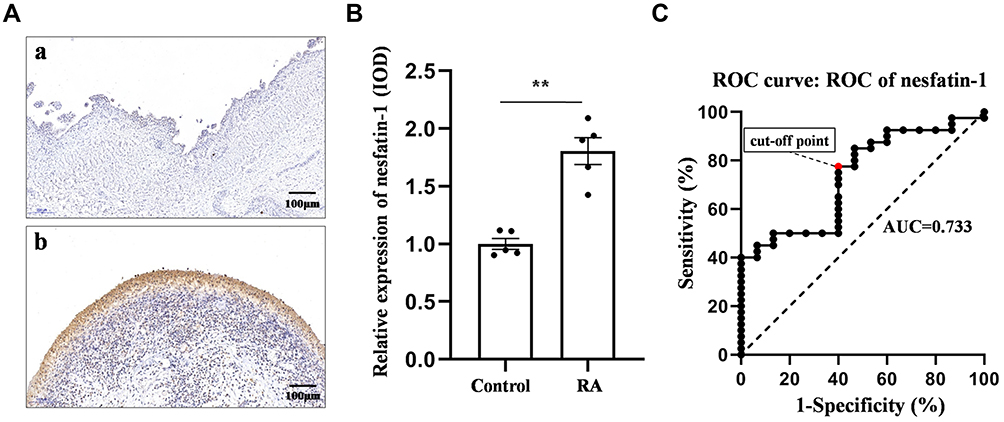 |
Figure 1 Nesfatin-1 levels in the synovium of the RA and control groups. (A) Typical immunohistochemistry images of nesfatin-1 protein expression (n = 5); (B) Quantitative analysis of nesfatin-1 protein expression based on immunohistochemistry results; (C) ROC curve of synovium nesfatin-1 in the identification of patients with RA. The data are presented as the mean ± SEM. **P < 0.01 vs control group. |
The levels of proinflammatory cytokines IL-1β (F = 34.218, P< 0.001) and TNF-α (F = 81.702, P< 0.001) in the synovium were also elevated in patients with RA (Table 1).
Additionally, ROC curve analysis indicated the potential diagnostic value of nesfatin-1 levels in the synovium (Figure 1C), with an AUC for nesfatin-1 levels of 0.733 (95% CI [confidence interval]: 0.592–0.875). At a cut-off point of 8681.44 pg/g for nesfatin-1, the sensitivity and specificity were 77.5% and 60.0%, respectively, for distinguishing patients with RA from controls.
Relationship Between Synovium Nesfatin-1 Levels and Clinical Features in the RA Group
As shown in Figure 2A, synovium nesfatin-1 concentrations were positively correlated with serum RF levels (r = 0.650, P< 0.001) in patients with RA. However, no significant relationship was observed between synovium nesfatin-1 and anti-CCP (r = 0.084, P = 0.622; Figure 2B), ASO (r = 0.299, P = 0.081; Figure 2C), CRP (r = 0.159, P = 0.340; Figure 2D), ESR (r = 0.156, P = 0.344; Figure 2E), and DAS28-ESR (r = 0.163, P = 0.321; Figure 2F) in patients with RA.
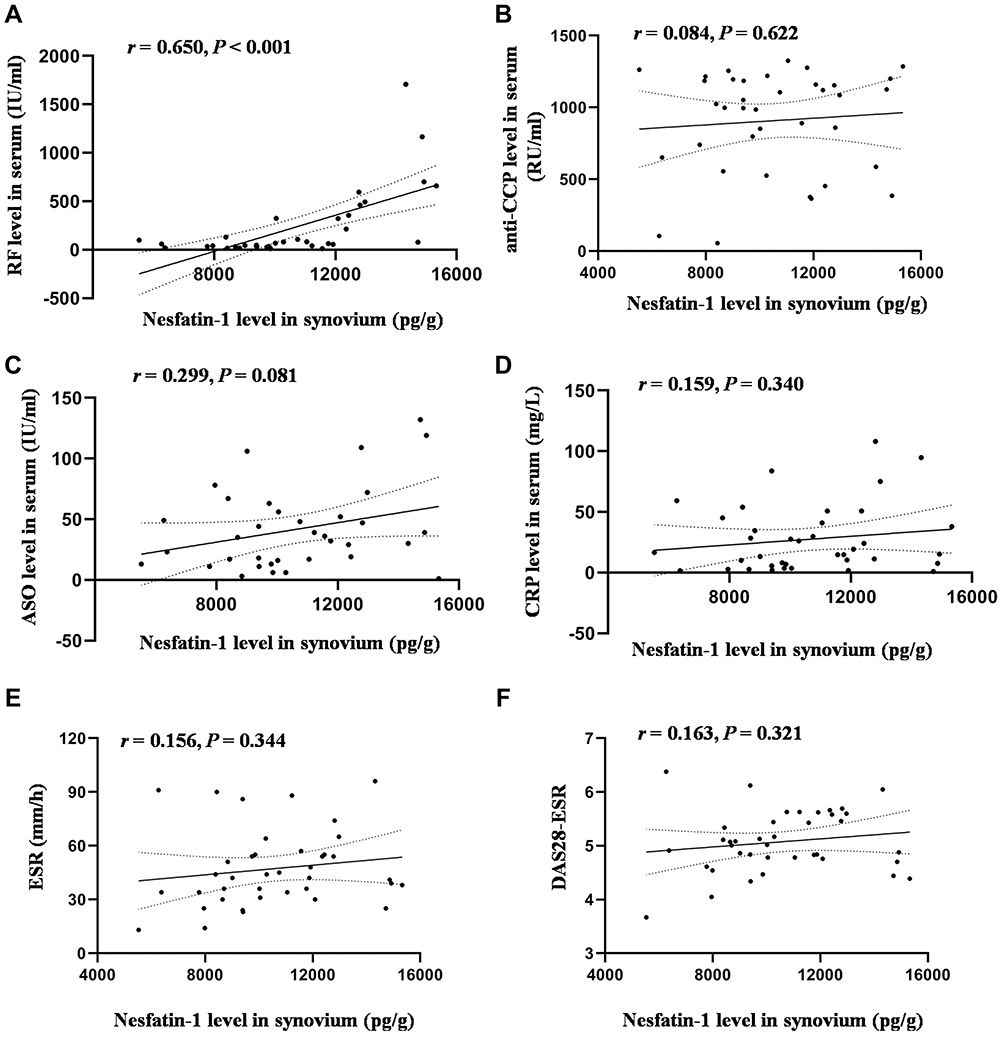 |
Figure 2 Correlation between nesfatin-1 levels in the synovium and clinical features in the RA group. (A) Correlation between synovium nesfatin-1 levels and serum RF levels; (B) Correlation between synovium nesfatin-1 levels and serum anti-CCP levels; (C) Correlation between synovium nesfatin-1 levels and serum ASO levels; (D) Correlation between synovium nesfatin-1 levels and serum CRP levels; (E) Correlation between synovium nesfatin-1 levels and ESR levels; (F) Correlation between synovium nesfatin-1 levels and DAS28-ESR scores. |
Relationship Between Nesfatin-1 Levels in SF and Clinical Features in the RA Group
As shown in Figure 3, no significant relationship was observed between nesfatin-1 in SF and RF (r = 0.294, P = 0.082; Figure 3A), anti-CCP (r = 0.127, P = 0.454; Figure 3B), ASO (r = 0.233, P = 0.177; Figure 3C), CRP (r = 0.051, P = 0.763; Figure 3D), ESR (r = −0.172, P = 0.296; Figure 3E), and DAS28-ESR (r = −0.041, P = 0.803; Figure 3F) in patients with RA.
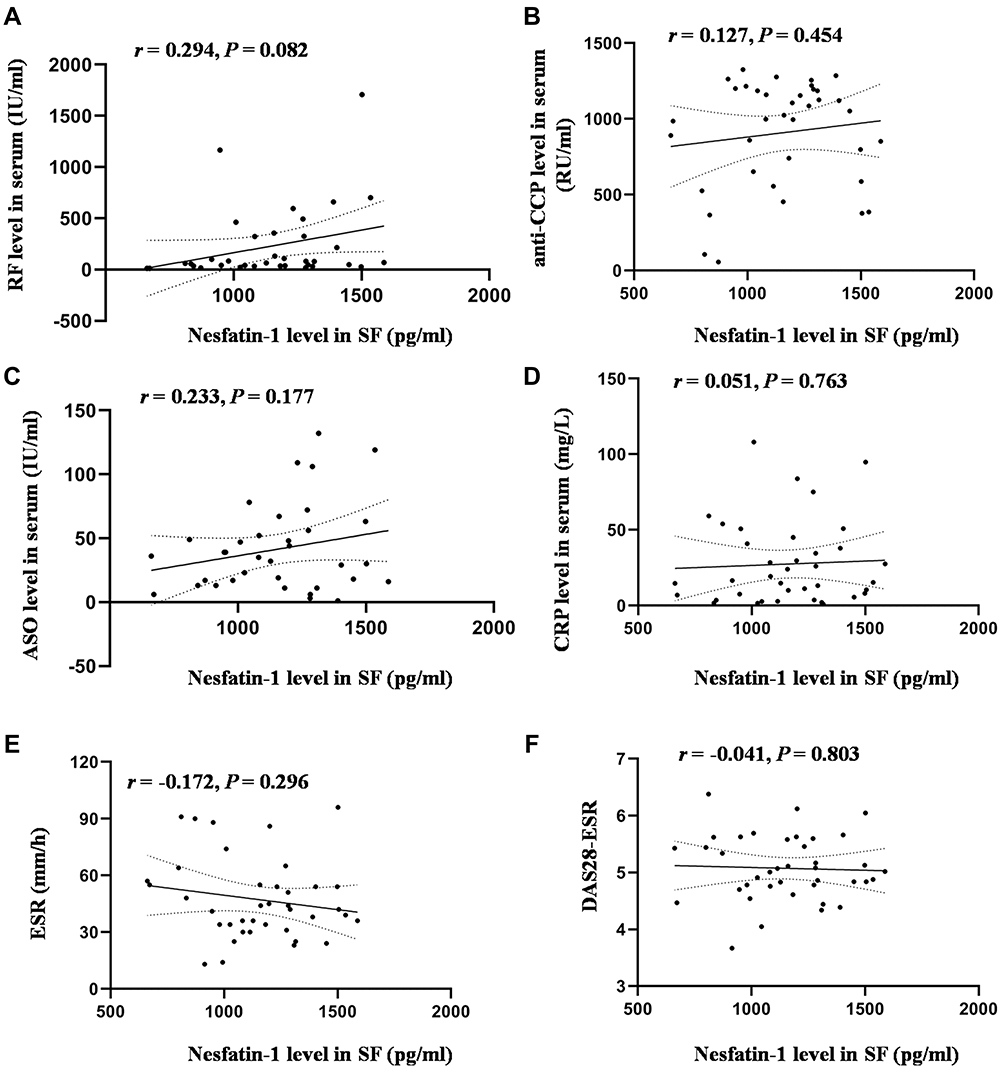 |
Figure 3 Correlation between nesfatin-1 levels in SF and clinical features in the RA group. (A) Correlation between SF nesfatin-1 levels and serum RF levels; (B) Correlation between SF nesfatin-1 levels and serum anti-CCP levels; (C) Correlation between SF nesfatin-1 levels and serum ASO levels; (D) Correlation between SF nesfatin-1 levels and serum CRP levels; (E) Correlation between SF nesfatin-1 levels and ESR levels; (F) Correlation between SF nesfatin-1 levels and DAS28-ESR scores. |
Relationship Between Nesfatin-1 Levels and Proinflammatory Cytokines in the RA Group
As shown in Figure 4A and B, synovium nesfatin-1 levels were positively correlated with IL-1β (r = 0.320, P = 0.044) and TNF-α (r = 0.589, P< 0.001) levels. However, SF nesfatin-1 levels were not correlated with IL-1β (r = 0.030, P = 0.853) and TNF-α levels (r = 0.084, P = 0.608) (Figure 4C and D).
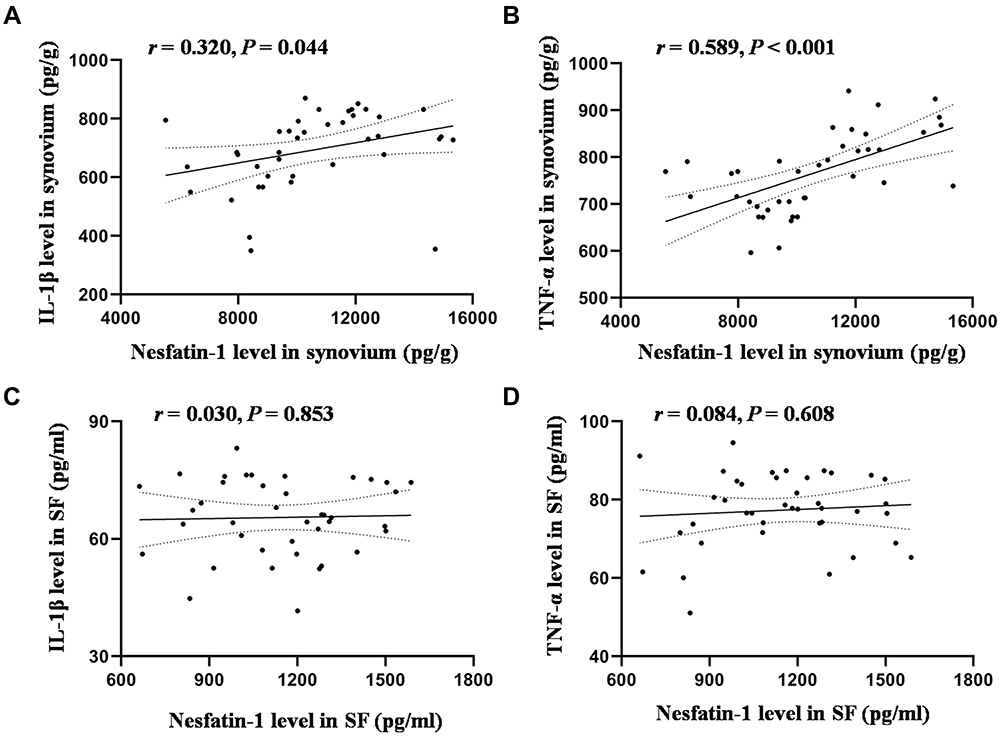 |
Figure 4 Correlation between nesfatin-1 levels and proinflammatory cytokines in the synovium and SF in the RA group. (A) Correlation between nesfatin-1 and IL-1β levels in the synovium; (B) Correlation between nesfatin-1 and TNF-α levels in the synovium; (C) Correlation between nesfatin-1 and IL-1β levels in SF; (D) Correlation between nesfatin-1 and TNF-α levels in SF. |
Discussion
In the present study, we demonstrated that nesfatin-1, IL-1β, and TNF-α levels in the synovium were significantly higher in patients with RA than in the control group, with age and BMI as covariates. Moreover, the results of the Pearson correlation analysis showed that nesfatin-1 levels were positively correlated with IL-1β and TNF-α levels in the synovium. Furthermore, there was a positive relationship between synovium nesfatin-1 levels and serum RF in patients with RA. Additionally, the results of the ROC curve analysis revealed an AUC of 0.733 with 77.5% sensitivity and 60.0% specificity for synovium nesfatin-1 in discriminating patients with RA from controls.
Age is an important risk factor for both disease onset and disease severity in epidemiological studies of RA.22 The mean age at RA onset has been reported to increase significantly from 55.8 years in 2002–2003 to 59.9 years in 2012–2013 in Japan using a nationwide database.23 Similarly, the mean age at RA onset was 59 years in the Rochester Epidemiology Project.24 Moreover, approximately 30% of RA cases occur in patients over 60 years of age.25 Accordingly, the mean age of patients with RA in the present study was 58.47 ± 1.35 years. Although obesity is another risk factor for the development of RA, accumulating evidence has demonstrated that a low BMI is associated with accelerated mortality in patients with RA.26 With the development of RA, skeletal muscle protein levels decrease, and BMI continually decreases, predominantly due to metabolic disorders caused by rheumatoid cachexia, decreased lean body mass, and increased levels of proinflammatory cytokines.27 In the present study, a lower BMI was observed in patients with RA. To eliminate the possible influences of age and BMI on synovium nesfatin-1 and proinflammatory cytokine levels, ANCOVA was performed to compare synovium nesfatin-1 and proinflammatory cytokine levels between the two groups, controlling for age and BMI by using these variables as covariates.
Nesfatin-1, a newly discovered feeding regulator, has been suggested to play an important physiological role in the central nervous system and peripheral tissues.28 There is growing evidence that abnormal changes in nesfatin-1 production are associated with various inflammation-related diseases. Specifically, nesfatin-1 levels were significantly higher in the cerebrospinal fluid of patients with multiple sclerosis, a neuroinflammatory disease.29 Moreover, increased or decreased nesfatin-1 concentrations in the peripheral blood have been observed in acute myocardial infarction, polycystic ovary syndrome, and knee osteoarthritis.14,30,31 These data may allow us to presume the involvement of nesfatin-1 in RA, a chronic autoimmune disease. In this study, nesfatin-1 levels were significantly increased in the synovium of patients with RA. To the best of our knowledge, this study is the first to report abnormal changes in synovium nesfatin-1 levels in patients with RA, providing further clinical data linking nesfatin-1 with RA. Additionally, a positive relationship was observed between synovium nesfatin-1 concentrations and serum RF levels in patients with RA. RF has routinely been used as a factor in patients with RA to evaluate disease activity and severity.32,33 This corroborates the findings of Kvlividze et al, who demonstrated that a higher serum nesfatin-1 level was characteristic of patients with a more severe clinical course of RA.34 Overall, these results suggest that increased nesfatin-1 production may be associated with RA severity.
As the main pathological and pathogenic factor, synovial inflammation plays a crucial role in the occurrence and progression of RA, mediating articular cartilage and bone destruction. Studies to uncover the cause of RA have recently scrutinized the importance of proinflammatory cytokines, such as TNF-α and IL-1β, in the pathogenesis of RA.35,36 TNF-α inhibitors have increasingly been used to treat patients with RA who are non-responsive to conventional anti-arthritic drugs.37 Accordingly, in the present study, synovium proinflammatory cytokines, including IL-1β and TNF-α, were elevated in patients with RA, providing further clinical evidence to support the viewpoint that agents targeting proinflammatory cytokines may be a promising strategy for RA treatment.
Accumulated evidence suggests a link between nesfatin-1 and proinflammatory cytokines. Plasma nesfatin-1 concentrations have been found to be positively correlated with IL-6 and CRP concentrations among patients with major depressive disorder.38 Moreover, a previous clinical study revealed a significant correlation of serum nesfatin-1 and hsCRP levels with synovial nesfatin-1 and IL-18 levels in patients with osteoarthritis.39 Furthermore, nesfatin-1 was significantly correlated with IL-2 and IL-13 levels in patients with primary open-angle glaucoma.40 Additionally, higher serum nesfatin-1 levels have been reported to be positively correlated with higher CRP concentrations in patients with RA.35 Consistent with these results, the results of the present study demonstrated that nesfatin-1 levels were positively correlated with IL-1β and TNF-α levels in the synovium of RA patients, suggesting that the involvement of nesfatin-1 in the pathogenesis of RA may be related to its correlation with the levels of proinflammatory factors.
It has been suggested that adipocytokines may be new biological markers that can be used in the diagnosis of a number of diseases.41,42 In terms of nesfatin-1, nesfatin-1 has been reported to be capable of distinguishing patients from the healthy population in gastric cancer,43 major depression44 and epilepsy.45 Therefore, in the present study, the potential of nesfatin-1 as a biomarker for RA diagnosis was investigated. Based on ROC analysis, the nesfatin-1 cut-off point of 8681.44 pg/g in the synovium was found to exhibit 77.5% sensitivity and 60.0% specificity, indicating that nesfatin-1 in the synovium has a superior diagnostic value for RA.
This study had certain limitations. First, the sample size was relatively small, and all subjects were recruited from a single hospital. Second, due to the cross-sectional study design, the causal association between nesfatin-1 and RA could not be determined. Third, we only measured nesfatin-1 levels in the SF of patients with RA, but not in healthy controls, because the collection of SF samples is invasive, and there are limitations to obtain SF samples from healthy controls.46,47 Finally, the serum anti-CCP levels of the controls and SF anti-CCP levels of the two groups were not measured, which is considered a flaw in the study design.
Nonetheless, several clinical implications have been highlighted. First, our study suggests that synovium nesfatin-1 levels may be related to synovium proinflammatory-cytokine levels and RA severity. Second, the level of nesfatin-1 in the synovium may be used as a diagnostic marker for screening patients with RA. Third, considering the antioxidant, anti-inflammatory, and antiapoptotic properties of nesfatin-113 as well as the findings of the present study, nesfatin-1 is a potential drug for the treatment of RA, a finding that needs to be validated by multicenter and longitudinal studies.
In conclusion, high nesfatin-1 levels in the synovium are associated with the disease severity of RA (as indicated by serum RF levels), which may be related to proinflammatory cytokine levels. The findings suggest that synovium nesfatin-1 is potentially a novel biomarker for the diagnosis of RA. Because distinct lymphoid and myeloid immune cell types in the synovium and their functions contribute to RA pathogenesis, future research is required to clarify the exact relationship between these immune cell types and nesfatin-1 in the synovium.
Funding
This work was supported by the National Natural Science Foundation of China (grant number: 81472088).
Disclosure
The authors declare no conflicts of interest.
References
1. Aletaha D, Smolen J. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
2. Smolen J, Aletaha D, McInnes I. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. doi:10.1016/s0140-6736(16)30173-8
3. Radawski C, Genovese M, Hauber B, et al. Patient perceptions of unmet medical need in rheumatoid arthritis: a cross-sectional survey in the USA. RheumatolTher. 2019;6(3):461–471. doi:10.1007/s40744-019-00168-5
4. Mun S, Lee Y, Park A, et al. Proteomics approach for the discovery of rheumatoid arthritis biomarkers using mass spectrometry. Int J Mol Sci. 2019;20(18):4368. doi:10.3390/ijms20184368
5. Vasileiadis G, Lundell A, Zhang Y, et al. Adipocytokines in untreated newly diagnosed rheumatoid arthritis: association with circulating chemokines and markers of inflammation. Biomolecules. 2021;11(2):325. doi:10.3390/biom11020325
6. Singh A, Gupta M, Mishra S. Study of correlation of level of expression of Wnt signaling pathway inhibitors sclerostin and dickkopf-1 with disease activity and severity in rheumatoid arthritis patients. Drug Discov Ther. 2019;13(1):22–27. doi:10.5582/ddt.2019.01011
7. Otero M, Lago R, Gomez R, et al. Changes in plasma levels of fat-derived hormones adiponectin, leptin, resistin and visfatin in patients with rheumatoid arthritis. Ann Rheum Dis. 2006;65(9):1198–1201. doi:10.1136/ard.2005.046540
8. Seven A, Güzel S, Aslan M, Hamuryudan V. Serum and synovial fluid leptin levels and markers of inflammation in rheumatoid arthritis. Rheumatol Int. 2009;29(7):743–747. doi:10.1007/s00296-008-0764-8
9. Migita K, Maeda Y, Miyashita T, et al. The serum levels of resistin in rheumatoid arthritis patients. Clin Exp Rheumatol. 2006;24:698–701.
10. Oh-I S, Shimizu H, Satoh T, et al. Identification of nesfatin-1 as a satiety molecule in the hypothalamus. Nature. 2006;443(7112):709–712. doi:10.1038/nature05162
11. Wei Y, Li J, Wang H, Wang G. NUCB2/nesfatin-1: expression and functions in the regulation of emotion and stress. Prog Neuropsychopharmacol Biol Psychiatry. 2018;81:221–227. doi:10.1016/j.pnpbp.2017.09.024
12. Angelone T, Rocca C, Pasqua T. Nesfatin-1 in cardiovascular orchestration: from bench to bedside. Pharmacoll Res. 2020;156:104766. doi:10.1016/j.phrs.2020.104766
13. Xu Y, Chen F. Antioxidant, anti-inflammatory and anti-apoptotic activities of nesfatin-1: a review. J Inflamm Res. 2020;13:607–617. doi:10.2147/jir.s273446
14. Zhang Y, Shui X, Lian X, Wang G. Serum and synovial fluid nesfatin-1 concentration is associated with radiographic severity of knee osteoarthritis. Med Sci Monitor. 2015;21:1078–1082. doi:10.12659/msm.892875
15. McInnes I, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol. 2007;7(6):429–442. doi:10.1038/nri2094
16. Feldmann M, Maini S. Role of cytokines in rheumatoid arthritis: an education in pathophysiology and therapeutics. Immunol Rev. 2008;223(1):7–19. doi:10.1111/j.1600-065X.2008.00626.x
17. Jiang L, Xu K, Li J, et al. Nesfatin-1 suppresses interleukin-1β-induced inflammation, apoptosis, and cartilage matrix destruction in chondrocytes and ameliorates osteoarthritis in rats. Aging. 2020;12(2):1760–1777. doi:10.18632/aging.102711
18. Tang C, Fu X, Xu X, Wei X, Pan H. The anti-inflammatory and anti-apoptotic effects of nesfatin-1 in the traumatic rat brain. Peptides. 2012;36(1):39–45. doi:10.1016/j.peptides.2012.04.014
19. Özsavcí D, Erşahin M, Şener A, et al. The novel function of nesfatin-1 as an anti-inflammatory and antiapoptotic peptide in subarachnoid hemorrhage-induced oxidative brain damage in rats. Neurosurgery. 2011;68(6):
20. Arnett F, Edworthy S, Bloch D, et al. The American rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–324. doi:10.1002/art.1780310302
21. Kay J, Upchurch K. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology. 2012;51(suppl_6):vi5–9. doi:10.1093/rheumatology/kes279
22. Goronzy J, Weyand C. Immune aging and autoimmunity. Cell Mol Life Sci. 2012;69(10):1615–1623. doi:10.1007/s00018-012-0970-0
23. Kato E, Sawada T, Tahara K, et al. The age at onset of rheumatoid arthritis is increasing in Japan: a nationwide database study. Int J Rheum Dis. 2017;20(7):839–845. doi:10.1111/1756-185x.12998
24. Kremers H, Myasoedova E, Crowson C, Savova G, Gabriel S, Matteson E. The Rochester epidemiology project: exploiting the capabilities for population-based research in rheumatic diseases. Rheumatology. 2011;50(1):6–15. doi:10.1093/rheumatology/keq199
25. van Schaardenburg D, Breedveld F. Elderly-onset rheumatoid arthritis. Semin Arthritis Rheum. 1994;23(6):367–378. doi:10.1016/0049-0172(94)90087-6
26. Baker J, Billig E, Michaud K, et al. Weight loss, the obesity paradox, and the risk of death in rheumatoid arthritis. Arthritis Rheumatol. 2015;67(7):1711–1717. doi:10.1002/art.39136
27. Tański W, Wójciga J, Jankowska-Polańska B. Association between malnutrition and quality of life in elderly patients with rheumatoid arthritis. Nutrients. 2021;13(4):1259. doi:10.3390/nu13041259
28. Schalla M, Unniappan S, Lambrecht N, Mori M, Taché Y, Stengel A. NUCB2/nesfatin-1 - Inhibitory effects on food intake, body weight and metabolism. Peptides. 2020;128:170308. doi:10.1016/j.peptides.2020.170308
29. Shimizu M, Manome T, Kumami M, et al. Detection of NUCB2/nesfatin-1 in cerebrospinal fluid of multiple sclerosis patients. Aging. 2020;12(23):24134–24140. doi:10.18632/aging.202287
30. Dai H, Li X, He T, et al. Decreased plasma nesfatin-1 levels in patients with acute myocardial infarction. Peptides. 2013;46:167–171. doi:10.1016/j.peptides.2013.06.006
31. Catak Z, Yavuzkir S, Kocdemir E, et al. NUCB2/nesfatin-1 in the blood and follicular fluid in patients with polycystic ovary syndrome and poor ovarian response. J Reprod Infertil. 2019;20:225–230.
32. Aletaha D, Alasti F, Smolen J. Rheumatoid factor, not antibodies against citrullinated proteins, is associated with baseline disease activity in rheumatoid arthritis clinical trials. Arthritis Res Ther. 2015;17(1):229. doi:10.1186/s13075-015-0736-9
33. Sokolove J, Johnson D, Lahey L, et al. Rheumatoid factor as a potentiator of anti-citrullinated protein antibody-mediated inflammation in rheumatoid arthritis. Arthritis Rheumatol. 2014;66(4):813–821. doi:10.1002/art.38307
34. Kvlividze T, Zavodovsky B, Akhverdyan Y, et al. Serum nesfatin-1 as a marker of systemic inflammation in rheumatoid arthritis. Klin Lab Diagn. 2019;64:53–56. doi:10.18821/0869-2084-2019-64-1-53-56
35. Kim G, Lee N, Pi R, et al. IL-6 inhibitors for treatment of rheumatoid arthritis: past, present, and future. Arch Pharm Res. 2015;38(5):575–584. doi:10.1007/s12272-015-0569-8
36. Feldmann M, Brennan F, Foxwell B, Maini R. The role of TNF alpha and IL-1 in rheumatoid arthritis. Curr Dir Autoimmun. 2001;3:188–199. doi:10.1159/000060522
37. Wang D, Li Y, Liu Y, Shi G. The use of biologic therapies in the treatment of rheumatoid arthritis. Curr Pharm Biotechnol. 2014;15(6):542–548. doi:10.2174/138920101506140910150612
38. Xia Q, Liang J, Cao Y, Shan F, Liu Y, Xu Y. Increased plasma nesfatin-1 levels may be associated with corticosterone, IL-6, and CRP levels in patients with major depressive disorder. Clin Chim Acta. 2018;480:107–111. doi:10.1016/j.cca.2018.02.004
39. Jiang L, Bao J, Zhou X, Xiong Y, Wu L. Increased serum levels and chondrocyte expression of nesfatin-1 in patients with osteoarthritis and its relation with BMI, hsCRP, and IL-18. Mediators Inflamm. 2013;2013:631251. doi:10.1155/2013/631251
40. Pahlitzsch M, Fritsche-Guenther R, Pompös I, et al. Correlation of NUCB2/nesfatin-1 with cytokine levels in primary open-angle glaucoma. Clinical Ophthalmol. 2021;15:2505–2517. doi:10.2147/opth.s307379
41. Loosen S, Koch A, Tacke F, Roderburg C, Luedde T. The role of adipokines as circulating biomarkers in critical illness and sepsis. Int J Mol Sci. 2019;20(19):4820. doi:10.3390/ijms20194820
42. Su X, Peng D. Adipokines as novel biomarkers of cardio-metabolic disorders. Clin Chim Acta. 2020;507:31–38. doi:10.1016/j.cca.2020.04.009
43. Wang X, Zheng Y, Fang P, Song X. Nesfatin-1 is a potential diagnostic biomarker for gastric cancer. Oncol Lett. 2020;19:1577–1583. doi:10.3892/ol.2019.11200
44. Xu Y, Ge J, Liang J, et al. Nesfatin-1 and cortisol: potential novel diagnostic biomarkers in moderate and severe depressive disorder. Psychol Res Behav Manag. 2018;11:495–502. doi:10.2147/prbm.s183126
45. Pałasz A, Krzystanek M, Worthington J, et al. Nesfatin-1, a unique regulatory neuropeptide of the brain. Neuropeptides. 2012;46(3):105–112. doi:10.1016/j.npep.2011.12.002
46. Lee B, Song Y, Rhodes C, et al. Protein phosphatase magnesium-dependent 1A induces inflammation in rheumatoid arthritis. Biochem Biophys Res Commun. 2020;522(3):731–735. doi:10.1016/j.bbrc.2019.11.112
47. Pousinis P, Gowler P, Burston J, Ortori C, Chapman V, Barrett D. Lipidomic identification of plasma lipids associated with pain behaviour and pathology in a mouse model of osteoarthritis. Metabolomics. 2020;16(3):32. doi:10.1007/s11306-020-01652-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.