")
Back to Journals » Journal of Pain Research » Volume 15
Elevated Levels of PGE2-Metabolite in Cerebrospinal Fluid and Cox-2 Gene Polymorphisms in Patients with Chronic, Post Cholecystectomy Pain and Visceral Hyperalgesia Compared to Healthy Controls. A Hypothesis-Generating Pilot Study
Authors Blichfeldt-Eckhardt MR , Olsen DA , Andersen RF, Toft P , Bendix L
Received 26 August 2022
Accepted for publication 3 November 2022
Published 14 December 2022 Volume 2022:15 Pages 3921—3929
DOI https://doi.org/10.2147/JPR.S387502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Morten Rune Blichfeldt-Eckhardt,1– 3 Dorte Aalund Olsen,4 Rikke Fredslund Andersen,4 Palle Toft,3,5 Laila Bendix2
1Department of Anesthesiology, Vejle Hospital, Vejle, Denmark; 2Multidiciplinary Pain Center of Southern Denmark, Department of Anesthesiology and Intensive Care, Odense University Hospital, Odense, Denmark; 3Department of Clinical Research, University of Southern Denmark, Odense, Denmark; 4Department of Biochemistry and Immunology, Vejle Hospital, Vejle, Denmark; 5Department of Anesthesiology and Intensive Care, Odense University Hospital, Odense, Denmark
Correspondence: Morten Rune Blichfeldt-Eckhardt, Multidisciplinary Pain Center of Southern Denmark, Department of Anesthesiology and Intensive Care, Odense University Hospital, Heden 9, Indgang 200, Odense, DK-5000, Denmark, Tel +4565414721, Fax +45 6541 3026, Email [email protected]
Purpose: Chronic, abdominal pain remains a problem in a subset of patients after cholecystectomy. The cause is often obscure but central sensitization may be an important component and could theoretically be mediated by spinal PGE2, which is regulated by several cytokines. The aim of the study was to examine cerebrospinal fluid (CSF) of participants with post cholecystectomy syndrome and healthy volunteers for signs of PGE2 and cytokine mediated central sensitization.
Patients and Methods: In phase 1 of the study, 83 subjects were included for DNA analysis, eight of these subjects with post cholecystectomy syndrome. We examined the SNPs rs5275, rs16944 and rs1800795 from the Cox-2, IL-1β and IL-6 genes respectively. In phase 2 of the study, we examined concentrations of PGE2-metabolite (PGEM), IL-1β and IL-6 in CSF and plasma from 6 patients with post cholecystectomy syndrome and visceral hyperalgesia and 11 pain free volunteers.
Results: We found a significant difference in distribution of the rs5275 SNP of the Cox-2 enzyme (CT-genotype=88% in pain group, 45% in pain free group, TT-genotype=0 in pain group, 41% in pain free group, p=0.05) but not in the other SNPs. PGEM, but not IL-6, was significantly elevated in CSF of the pain group (3.6 pg/mL, sd=1.9 vs 2.1 pg/mL, p=0.03), IL-1β was undetectable.
Conclusion: We found elevated PGEM levels in CSF of patients with post cholecystectomy syndrome and visceral hyperalgesia, suggesting a central, possibly inflammatory component to the pain, and overrepresentation of the CT-genotype in the rs5275 SNP in the Cox2 gene, suggesting overexpression of Cox2 as a possible cause for elevated PGEM levels.
Keywords: T8473, visceral pain, post cholecystectomy syndrome, hyperalgesia, central sensitization
Plain Language Summary
Chronic, abdominal pain is a problem in some persons after gallbladder surgery. The cause is often unclear and in these cases, the treatment options is often insufficient.
A possible theory is that nerves in the central nervous system (brain and spinal cord) become hypersensitive to pain, which means that they overreact to input so that non-harmful stimuli provoke pain. This pain hypersensitivity is sometimes facilitated by signaling substances from the immune system.
We completed a study in two phases. In phase 1, we examined 83 persons undergoing gallbladder surgery. Eight of these persons developed chronic abdominal pain afterwards. We found that persons with chronic pain had a different variant of the gene that controls the Cox-2 enzyme, which is an enzyme that reacts to activity in the immune system and elevates the substance, prostaglandin E2 (PGE2), which increase pain sensitivity in the central nervous system.
In phase 2, we examined the cerebrospinal fluid of 17 persons, of which six persons developed chronic pain after gallbladder surgery. We found that persons with chronic pain had higher levels of PGE2-metabolite (which is an indicator of PGE2 levels) in the cerebrospinal fluid and hypersensitivity to pain in the gallbladder area of the abdomen.
This indicates that the cause of chronic, abdominal pain after gallbladder surgery is subtle activity of the immune system, eg inflammation, causing pain hypersensitivity in the central nervous system and by genetic factors. However, this must be tested in a larger population before final conclusions can be made.
Introduction
Persistent or chronic pain in the upper abdomen continues to be a problem in 5–40% of patients after cholecystectomy and is often referred to as post cholecystectomy syndrome (PCS) when combined with various gastrointestinal symptoms.7,17,23,40 While the cause can be identified and treated in many cases (ie biliary stones, gastric ulcers, gastro-esophageal reflux) the cause of the pain remains unexplained in up to one third of the patients.7,15,19 Sphincter of Oddi dysfunction (SOD) is often proposed as a possible cause, but only a subset of patients with unexplained PCS have demonstrable sphincter of Oddi dysmotility. Furthermore, in the patients where dysmotility is demonstrated, endoscopic sphincterotomy has very limited effect on the pain.10–12,38
Visceral hyperalgesia, caused by persistent hyper-excitability of relevant nociceptive neurons in the central nervous system (CNS), in some situations referred to as central hypersensitivity or central sensitization, has been hypothesized as a possible mechanism behind PCS. This theory is supported by findings of hyperalgesia in the referred pain area in patients with PCS and could be caused by persistent, abnormal, sensory visceral input caused by neuronal damage or a local, subclinical, chronic inflammatory condition.9,21
Prostaglandin E2 (PGE2) is a key mediator of both peripheral and central sensitization in inflammatory pain, but a role in visceral and neuropathic pain has also been suggested.6,18,30,39 It is well established that spinal PGE2 elevation can be induced by a peripheral insult, causing upregulation of spinal interleukin-1β (IL-1β), which induces upregulation of spinal cyclooxygenase-2 (Cox-2) expression, which again leads to increased spinal PGE2 levels and peripheral hyperalgesia. Interleukin-6 (IL-6) has been suggested as a mediator of this response.13,26,34
Variations in pain and pain sensitivity are partly explained by genetic variations, which could be important in the control of the IL-1β–Cox2–PGE2 axis.16,31,33 The Cox-2 gene (PTGS2) carries a common single-nucleotide polymorphism (SNP), T8473 (rs5275), which is a key regulator of Cox-2 expression and the T8473C-allele has been associated with COX-2 overexpression, followed by increased PGE2 levels.22,29 The rs16944 SNP is located in the promoter region of the IL-1β gene and is important in the regulation of IL-1β levels.14 Finally, the IL-6 “–174” polymorphism (rs1800795) has been associated with the inflammatory IL-6 response.24
The aim of this study was to investigate the levels of PGE2-metabolite, IL-1β and IL-6 in cerebrospinal fluid (CSF) and plasma in patients with chronic pain and visceral hyperalgesia after cholecystectomy compared to healthy volunteers, and to investigate possible genetic polymorphisms in rs5275, rs16944 and rs1800795 SNPs in the two groups.
We hypothesized that participants with persistent post cholecystectomy pain would have increased levels of PGE2-metabolite and IL-1β in CSF, possibly elevated levels of IL-6 in plasma compared to healthy controls, and that we would find polymorphisms in one or more of the associated SNPs.
Methods
Design and Patients
From a cohort of 100 patients for laparoscopic cholecystectomy, which has been described elsewhere,9 all participants were invited to undergo additional tests.
In the original study, 100 patients were followed for 12 months after cholecystectomy. In this period, they all completed an extensive program for diagnosing and treating post cholecystectomy pain. Based on this, the participants for this study were classified into two groups: chronic, unexplained pain in the upper abdomen 12 months after cholecystectomy or no pain 12 months after cholecystectomy. These included patients with well-defined causes of post cholecystectomy pain (ie common bile duct stone, peptic ulcer etc.) where the cause could be treated and resolved within the first months after cholecystectomy.
There were 2 phases of this study. In phase 1 all participants were invited to contribute with blood samples for genetic tests at the 12-months interview.
In phase 2, participants were invited to also contribute with blood and CSF for investigation of cytokine levels and a test for abdominal pain pressure threshold. Inclusion criteria were participation in phase 1, exclusion criteria were: other chronic pain, acute pain during the previous week, immunological disease or immunosuppressive treatment. In the original study, participants with disease in the central and peripheral nervous system or any paresthesias had also been excluded. Due to a limited number of pain free participants from the original study, the pain free group was expanded with participants who were to receive spinal anesthesia for elective gynecological operations and participants who responded to community advertisements. The same exclusion criteria applied for this group and with the additional criteria of no previous abdominal surgery. The study was conducted according to the Helsinki Declaration and approved by the regional ethics committee (39561) and the Danish data protection agency (4308). Written informed consent was obtained from all participants.
Procedures
Four milliliters of blood was collected from all participants in phase 1 with standard venous puncture. Blood was frozen directly as whole blood and kept at −80 °C. An additional 8 mL of blood was collected from participants in phase 2, which was centrifuged at room temperature and frozen at −80 °C within one hour after sampling.
CSF was collected by lumbar puncture, performed by an experienced anesthesiologist specialist using sterile technique and a 27 G pencil point needle. All CSF samples were placed in ice water immediately after sampling, centrifuged at 4 °C and frozen at –80 °C within one hour.
Pain Pressure Threshold (PPT) was performed at the time of the 12-months interview in the original study. It was done with an Alogmeter II (Somedic AB), with a probe area of 1 cm2 and determined as the mean response of 3 independent measurements, each applied at a slowly increasing ramp of 50 kPa/s. The test area was the gall bladder area and the corresponding contralateral area was the control area.
Genetic Tests
The following SNPs were investigated: rs5275, rs16944 and rs1800795. DNA was extracted from 300 µL whole blood using the Maxwell 16 instrument (Promega, Madison, WI, USA) with a Maxwell 16 Blood DNA Purification Kit (Promega). DNA was eluted in 300 µL elution buffer. The concentration of DNA was determined by NanoDrop spectrophotometry (Thermo Fisher Scientific, Waltham, MA, USA). DNA was shipped to LGC genomics Ltd. (Hoddesdon, UK)1 for genotyping. DNA was quality checked and genotyped using Kompetitive Allele Specific PCR (KASP). Data were received as .csv files and visualized with SNPViewer software from LGC Biosearch Technologies.1
Cytokine Tests
Commercially available enzyme-linked immunosorbent assays from R&D Systems (Minneapolis, MN, USA) were used for quantifying IL1b and IL-6 (IL1b HSLB00C and IL-6 HS600B). Because no direct test of PGE2 was available to the laboratory, PGE2-metabolite levels were measured as an indicator of PGE2-concentration. PGE2-metabolite concentrations have been demonstrated to be closely associated with PGE2 concentrations8,36 and were measured using a commercially available competitive assay from Cayman (PGEM 514531, Cayman Chemical, Ann Arbor, MI, USA). The analyses were performed according to the manufacturer’s protocols. All samples were analysed in duplicates and the average of the two were applied. The intra assay coefficient of variations were between 13% and 17%.
Statistics
Parametric data are presented as means and compared with a t-test. A chi2 test were used for comparing categorical data. Because of small sample size, data from phase 2 of the study were presented as non-parametric data, using medians and compared with a Wilcoxon–Mann–Whitney test. Delta pain perception threshold (ΔPPT) was calculated as the difference in PPT between the pain area/gallbladder area and the control area: PPT control area–PPT test area, and used as an assessment of hyperalgesia in the referred pain area. A P-value <0.05 was considered statistically significant.
Results
Phase 1, Genetic Data
Samples were collected from August 2011 to December 2013. In phase 1 (Figure 1), 83 subjects from the original study participated. Eight of the participants reported chronic, post cholecystectomy pain and 75 participants reported no pain. Demographic data for participants in phase 1 of the project are shown in Table 1.
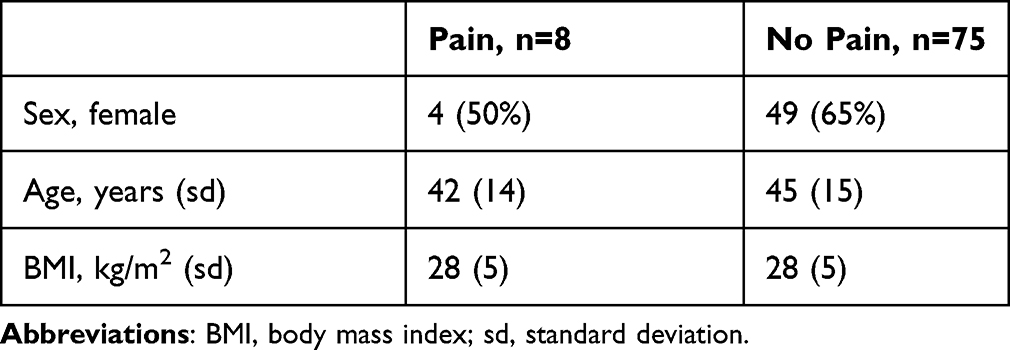 |
Table 1 Demographic Data for Participants in Phase 1 |
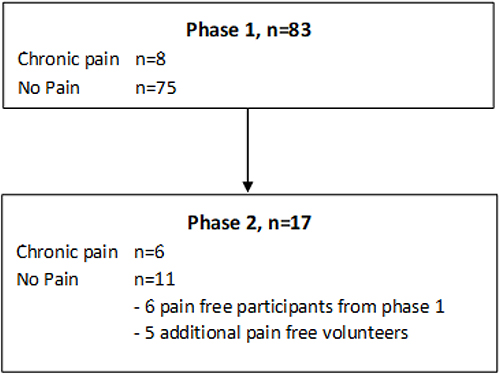 |
Figure 1 Study flow chart. |
Participants with chronic pain had significantly higher ΔPPT (PPT control area–PPT test area) (80 kPa, sd=97) compared to pain free controls (17 kPa, sd=70, p=0.04). PPT in the test area (gallbladder area) versus the control area in the two groups is depicted in Figure 2.
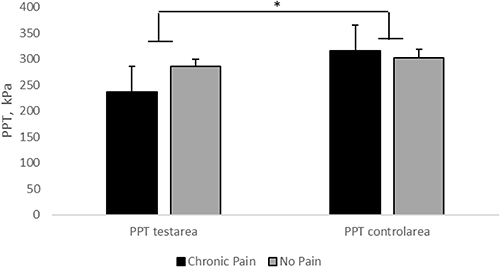 |
Figure 2 Pain pressure threshold (PPT). Pain pressure threshold (PPT) in the test area versus the control area, in participants with and without chronic pain in the upper abdomen. Error bars are SEM. n=83. *Significant difference (p=0.04) in ΔPPT (PPT control area–PPT test area) between pain patients and pain free controls. |
The three investigated SNPs (rs5275, rs1800795, rs16944) were all found not to deviate from Hardy–Weinberg equilibrium (P>0.05). The genotypes for all three SNPs are presented in Table 2. The genotype distribution of the rs5275 SNP (Cox-2 gene) was significantly different in the 2 groups with 7 out of 8 (88%) participants from the pain group displaying the CT-genotype and 0 out of 8 participants displaying the TT-genotype, versus 45% of participants in the pain free group displaying the CT-genotype and 41% displaying the TT-genotype (p=0.05). There were no significant differences in the rs1800795 (IL-6) or the rs16944 (IL-1β) SNPs.
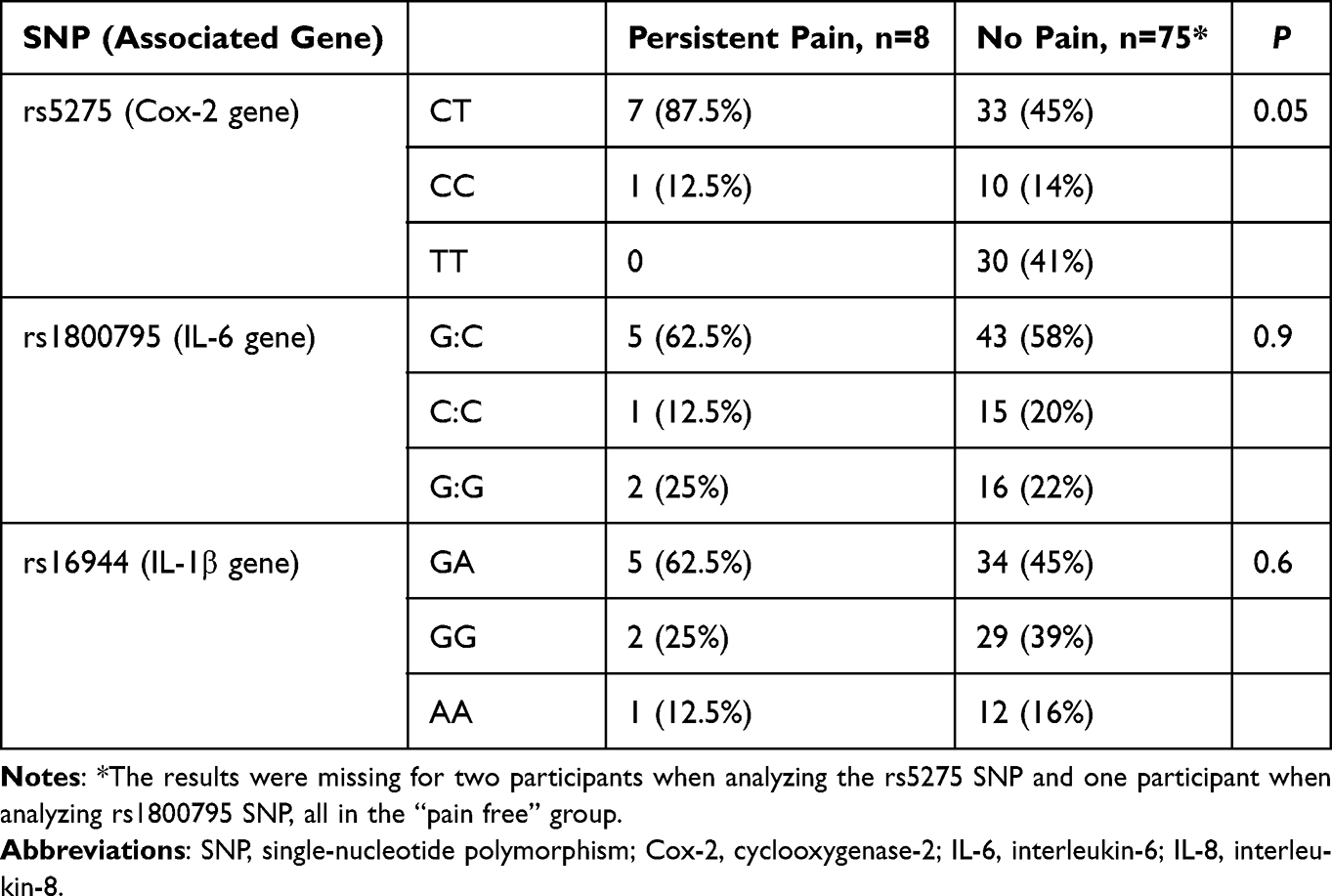 |
Table 2 Distribution of Genotypes of the rs5275, rs1800795 and rs16944 SNPs in Patients with Persistent Pain After Cholecystectomy Compared to Pain Free Controls |
Phase 2, Cytokine Data
Of the 83 patients from phase 1, 12 participants (six participants with post cholecystectomy pain and six pain free controls) and five additional pain free volunteers (two were operated for cystocele in spinal anesthesia and three responded to community advertisements) were included in phase 2 of the study (Figure 1), giving six participants with chronic pain after cholecystectomy and 11 pain free participants. Demographic data for the participants in phase 2 are shown in Table 3.
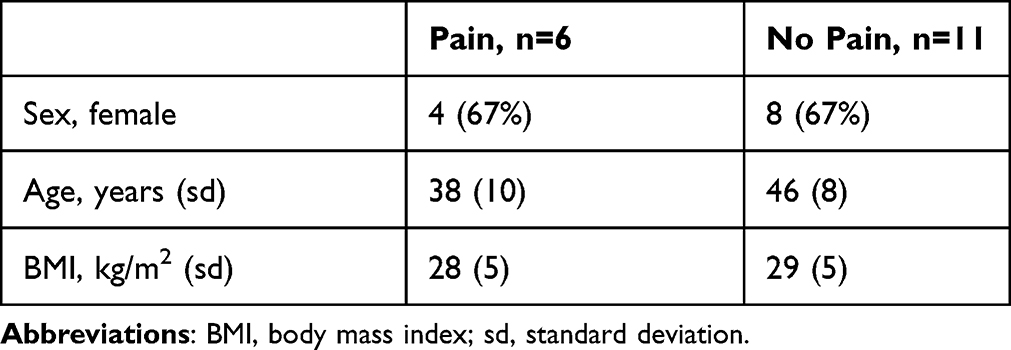 |
Table 3 Demographic Data Phase 2 |
PGE2-metabolite concentrations in CSF (Figure 3A) were significantly higher in the pain group (2.9 pg/mL, interquartile range=2.7–3.3) compared to pain free participants (2.0 pg/mL, interquartile range=1.6–2.4, p=0.01). There were no differences in the median PGE2-metabolite concentrations in plasma between the groups. IL-6 concentrations (Figure 3B) in plasma were higher in the pain group (0.91 pg/mL, interquartile range=0.62–1.38) compared to the pain free group (0.62 pg/mL, interquartile range=0.40–0.87) but this difference was not statistically significant. There were no difference in CSF concentrations. For IL-1β there were too few measurements within detectable concentrations to make meaningful statistical analysis (six out of 17 (35%) CSF-samples and seven out of 17 (41%) of plasma samples).
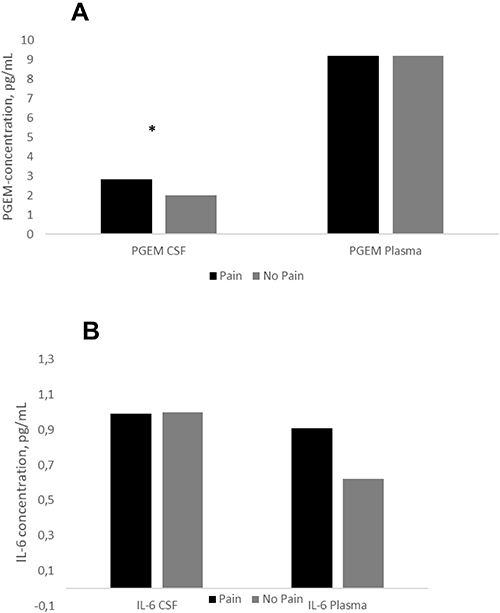 |
Figure 3 Cytokine concentrations in CSF and plasma. (A) PGE-metabolite. (B) IL-6. Black bars are participants with chronic pain in the upper abdomen; grey bars are pain free participants. (A) PGE2-metabolite concentrations in CSF and plasma. *p=0.03. (B) IL-6 concentrations in CSF and plasma. Error bars are SEM. n=17. Abbreviations: CSF, cerebrospinal fluid; PGE2, prostaglandin E2; PGEM, PGE2-metabolite; IL-6, interleukin-6. |
Complications
No participants suffered post procedural complications, including spinal headache, except temporary soreness at the puncture site as expected.
Discussion
In this study, we confirmed the hypothesis that PGE2-metabolite concentrations were elevated in CSF in patients with chronic, unexplained pain more than 12 months after cholecystectomy and visceral hyperalgesia. We also found a corresponding, specific polymorphism in the Cox-2 enzyme in which the rs5275C-allele was overrepresented in the pain group. We did not find any significant difference in IL-6 in plasma or CSF and IL-1B was below detection limit in most of the samples and thus beyond meaningful analysis.
The finding of elevated PGE2-metabolite concentrations in CSF and visceral hyperalgesia in the pain group confirms the theory of a central component in chronic post cholecystectomy pain and suggests an inflammatory origin of the pain. While the authors are not aware of any other studies of PGE2 or PGE2-metabolite concentrations in the CSF from this patient group, elevated spinal PGE2 concentrations have been extensively associated with secondary peripheral hyperalgesia in a number of studies of inflammatory pain models.13,20,35
The hypothesis is further confirmed by the clear overweight of the rs5275C-allele of the Cox-2 gene in participants with chronic, unexplained pain after cholecystectomy. The Cox-2 enzyme is a well-established regulator of spinal PGE2 levels and the C-allele of the rs5275 SNP previously has been associated with over-activity of the Cox-2 enzyme. The rs5275 SNP is located in exon 10 which encodes the Cox-2 3’-untranslated region (3’UTR) and is important in controlling Cox-2 expression through control of Cox-2 mRNA decay. Thus the variant allele rs5275T is associated with Cox-2 mRNA degradation and the rs5275C-allele is associated with Cox-2 mRNA stabilization, Cox-2 mRNA overexpression and increased PGE2 concentrations.29 While the rs5275 (T8773C) SNP in the Cox-2 gene, to our knowledge, has not previously been studied in a population with chronic pain, it has been linked to overexpression of Cox-2 in several other studies.3,25,32 The importance of Cox-2 in regulating spinal PGE2 levels and secondary hyperalgesia is also well known. Samad et al established that peripheral inflammation caused elevated spinal IL-1β levels, possibly mediated via circulating IL-6. Spinal IL-1β in turn induced increased Cox-2 mRNA expression in CNS leading to elevated PGE2 levels in CSF and was associated with peripheral, secondary hyperalgesia. This hyperalgesia could be blocked by IL-1β and Cox-2 inhibitors and the mechanism has been confirmed in several other studies.30,34,41 Unfortunately, it was not possible to evaluate IL-1β concentrations because of missing values, which unfortunately is a well-known problem as IL-1β concentrations are generally low in CSF and blood.4,5,37 The fact that we did not find any difference in the rs16944 SNP of the IL-1β gene suggests that this SNP is not important in regulation of hyperalgesia in chronic, unexplained pain after cholecystectomy but we cannot use the finding to draw any conclusions on the overall role of IL-1β in this condition. IL-6 has been suggested to be a peripheral regulator of spinal IL-1β upregulation in inflammatory pain and was found to be elevated in other pain conditions, but the importance of IL-6 for the Cox-2/PGE2 axis has not been confirmed.2,27,34 We did not find any significant difference in the concentration of the cytokine or the rs1800795 SNP and therefore, we cannot confirm any important role for IL-6 in the described mechanism. It could, however, not be ruled out that the non-significant elevation in plasma IL-6 concentration we found in the pain group would have been significant in a larger sample size.
The main limitation to this pilot study is obviously the small sample size and the fact that only a subset of the participants in phase 1 of the study participated in phase 2 of the study. The additional pain free participants in phase 2 of the study also adds to the heterogeneity of the population in the two phases of the study, but also adds power to the result. Overall, the findings must be interpreted with caution. The coherence between the proposed theory, the biochemical and the clinical findings, however, are remarkable and should be investigated in a larger sample size.
The described mechanism of increased Cox-2 mRNA expression, elevated PGE2 levels and clinical hyperalgesia is primarily confirmed in models of inflammatory pain, and chronic, unexplained pain after cholecystectomy is not usually considered an inflammatory type of pain. The existence of a chronic, perhaps subclinical inflammation in the gallbladder area could however be a theoretical possibility and has previously been suggested.9 Another possibility is that PGE2-induced, central hyperalgesia is also involved in other types of chronic pain. Perioperative damage to visceral nerves causing persistent neuropathic pain could theoretically be a possibility and a role for PGE2 in neuropathic pain has also been suggested, but is not well established.18,28,30,39 We did not measure PGE2 directly, but instead the PGE2-metabolite concentrations. Yet, it is well established that PGE2-metabolite concentrations can be used as a marker of PGE2 concentrations.8,36 A direct measurement of the Cox-2 enzyme would have been relevant, but not a possibility we had at the time of the study.
In conclusion, patients with chronic, unexplained pain and deep visceral hyperalgesia more than 12 months after cholecystectomy have elevated PGE2-metabolite concentrations in CSF and a polymorphism in the rs5275-allele of the Cox-2 gene, which is associated with Cox-2 overexpression. This confirms the theory of a central component in chronic, unexplained pain after cholecystectomy and suggests an inflammatory component.
Abbreviations
PCS, post cholecystectomy syndrome; SOD, sphincter of Oddi dysfunction; CNS, central nervous system; PGE2, prostaglandin E2; IL-1β, interleukin-1β; Cox-2, cyclooxygenase-2; IL-6, interleukin-6; SNP, single-nucleotide polymorphism.
Ethics Approval and Informed Consent
The study was conducted according to the Helsinki Declaration and approved by the regional ethics committee (39561) and the Danish data protection agency (4308). Written informed consent was obtained from all participants.
Acknowledgments
The authors wish to thank late Steen Kølvraa, MD, Professor of Genetics, for guidance, discussions and for pointing out the rs5275-allele as a possible important regulator of Cox2 and PGE2 in pain.
Funding
The following private and independent foundations funded the work: Oberstinde Kirsten Jensa la Cours Legat and Lippmann Fonden.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. LGC Biosearch Technologies. Genotyping services. Available from: https://www.biosearchtech.com/services/genotyping-services.
2. Alexander GM, van Rijn MA, van Hilten JJ, Perreault MJ, Schwartzman RJ. Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Pain. 2005;116:213–219. doi:10.1016/j.pain.2005.04.013
3. Ali IU, Luke BT, Dean M, Greenwald P. Allellic variants in regulatory regions of cyclooxygenase-2: association with advanced colorectal adenoma. Br J Cancer. 2005;93:953–959. doi:10.1038/sj.bjc.6602806
4. Backonja MM, Coe CL, Muller DA, Schell K. Altered cytokine levels in the blood and cerebrospinal fluid of chronic pain patients. J Neuroimmunol. 2008;195:157–163. doi:10.1016/j.jneuroim.2008.01.005
5. Backryd E, Tanum L, Lind AL, Larsson A, Gordh T. Evidence of both systemic inflammation and neuroinflammation in fibromyalgia patients, as assessed by a multiplex protein panel applied to the cerebrospinal fluid and to plasma. J Pain Res. 2017;10:515–525. doi:10.2147/JPR.S128508
6. Bianchi M, Martucci C, Ferrario P, Franchi S, Sacerdote P. Increased tumor necrosis factor-alpha and prostaglandin E2 concentrations in the cerebrospinal fluid of rats with inflammatory hyperalgesia: the effects of analgesic drugs. Anesth Analg. 2007;104:949–954. doi:10.1213/01.ane.0000258060.89380.27
7. Bisgaard T, Rosenberg J, Kehlet H. From acute to chronic pain after laparoscopic cholecystectomy: a prospective follow-up analysis. Scand J Gastroenterol. 2005;40:1358–1364. doi:10.1080/00365520510023675
8. Bjork L, Leifsdottir K, Saha S, Herlenius E. PGE-metabolite levels in CSF correlate to HIE score and outcome after perinatal asphyxia. Acta Paediatr. 2013;102:1041–1047. doi:10.1111/apa.12361
9. Blichfeldt-Eckhardt MR, Ording H, Andersen C, Licht PB, Toft P. Early visceral pain predicts chronic pain after laparoscopic cholecystectomy. Pain. 2014;155:2400–2407. doi:10.1016/j.pain.2014.09.019
10. Costamagna G. Sphincter of Oddi dysfunction: the never-ending story has come to a conclusion. Gastrointest Endosc. 2018;87:211–212. doi:10.1016/j.gie.2017.07.004
11. Cotton PB, Durkalski V, Romagnuolo J, et al. Effect of endoscopic sphincterotomy for suspected sphincter of Oddi dysfunction on pain-related disability following cholecystectomy: the EPISOD randomized clinical trial. JAMA. 2014;311:2101–2109. doi:10.1001/jama.2014.5220
12. Cotton PB, Pauls Q, Keith J, et al. The EPISOD study: long-term outcomes. Gastrointest Endosc. 2018;87:205–210. doi:10.1016/j.gie.2017.04.015
13. Ferreira SH, Lorenzetti BB. Intrathecal administration of prostaglandin E2 causes sensitization of the primary afferent neuron via the spinal release of glutamate. Inflamm Res. 1996;45:499–502. doi:10.1007/BF02311085
14. Iglesias Molli AE, Bergonzi MF, Spalvieri MP, Linari MA, Frechtel GD, Cerrone GE. Relationship between the IL-1beta serum concentration, mRNA levels and rs16944 genotype in the hyperglycemic normalization of T2D patients. Sci Rep. 2020;10:9985. doi:10.1038/s41598-020-66751-x
15. Isherwood J, Oakland K, Khanna A. A systematic review of the aetiology and management of post cholecystectomy syndrome. Surgeon. 2019;17:33–42. doi:10.1016/j.surge.2018.04.001
16. James S. Human pain and genetics: some basics. Br J Pain. 2013;7:171–178. doi:10.1177/2049463713506408
17. Jaunoo SS, Mohandas S, Almond LM. Postcholecystectomy syndrome (PCS). Int J Surg. 2010;8:15–17. doi:10.1016/j.ijsu.2009.10.008
18. Kawabata A. Prostaglandin E2 and pain--an update. Biol Pharm Bull. 2011;34:1170–1173. doi:10.1248/bpb.34.1170
19. Kim H, Han IW, Heo JS, et al. Postcholecystectomy syndrome: symptom clusters after laparoscopic cholecystectomy. Ann Surg Treat Res. 2018;95:135–140. doi:10.4174/astr.2018.95.3.135
20. Kras JV, Dong L, Winkelstein BA. Increased interleukin-1alpha and prostaglandin E2 expression in the spinal cord at 1 day after painful facet joint injury: evidence of early spinal inflammation. Spine. 2014;39:207–212. doi:10.1097/BRS.0000000000000107
21. Kurucsai G, Joo I, Fejes R, et al. Somatosensory hypersensitivity in the referred pain area in patients with chronic biliary pain and a sphincter of Oddi dysfunction: new aspects of an almost forgotten pathogenetic mechanism. Am J Gastroenterol. 2008;103:2717–2725. doi:10.1111/j.1572-0241.2008.02068.x
22. Lai ZZ, Yang HL, Ha SY, et al. Cyclooxygenase-2 in Endometriosis. Int J Biol Sci. 2019;15:2783–2797. doi:10.7150/ijbs.35128
23. Lamberts MP, Lugtenberg M, Rovers MM, et al. Persistent and de novo symptoms after cholecystectomy: a systematic review of cholecystectomy effectiveness. Surg Endosc. 2013;27:709–718. doi:10.1007/s00464-012-2516-9
24. Landi S, Moreno V, Gioia-Patricola L, et al.; Bellvitge Colorectal Cancer Study Group. Association of common polymorphisms in inflammatory genes interleukin (IL)6, IL8, tumor necrosis factor alpha, NFKB1, and peroxisome proliferator-activated receptor gamma with colorectal cancer. Cancer Res. 2003;63:3560–3566.
25. Langsenlehner U, Yazdani-Biuki B, Eder T, et al. The cyclooxygenase-2 (PTGS2) 8473T>C polymorphism is associated with breast cancer risk. Clin Cancer Res. 2006;12:1392–1394. doi:10.1158/1078-0432.CCR-05-2055
26. Lee YS, Kim H, Brahim JS, Rowan J, Lee G, Dionne RA. Acetaminophen selectively suppresses peripheral prostaglandin E2 release and increases COX-2 gene expression in a clinical model of acute inflammation. Pain. 2007;129:279–286. doi:10.1016/j.pain.2006.10.020
27. Lundborg C, Hahn-Zoric M, Biber B, Hansson E. Glial cell line-derived neurotrophic factor is increased in cerebrospinal fluid but decreased in blood during long-term pain. J Neuroimmunol. 2010;220:108–113. doi:10.1016/j.jneuroim.2010.01.007
28. Ma W, Quirion R. Does COX2-dependent PGE2 play a role in neuropathic pain? Neurosci Lett. 2008;437:165–169. doi:10.1016/j.neulet.2008.02.072
29. Moore AE, Young LE, Dixon DA. A common single-nucleotide polymorphism in cyclooxygenase-2 disrupts microRNA-mediated regulation. Oncogene. 2012;31:1592–1598. doi:10.1038/onc.2011.349
30. Neeb L, Hellen P, Boehnke C, et al. IL-1beta stimulates COX-2 dependent PGE(2) synthesis and CGRP release in rat trigeminal ganglia cells. PLoS One. 2011;6:e17360. doi:10.1371/journal.pone.0017360
31. Nielsen CS, Stubhaug A, Price DD, Vassend O, Czajkowski N, Harris JR. Individual differences in pain sensitivity: genetic and environmental contributions. Pain. 2008;136:21–29. doi:10.1016/j.pain.2007.06.008
32. Ozhan G, Yanar TH, Ertekin C, Alpertunga B. The effect of genetic polymorphisms of cyclooxygenase 2 on acute pancreatitis in Turkey. Pancreas. 2010;39:371–376. doi:10.1097/MPA.0b013e3181bae9ca
33. Palada V, Kaunisto MA, Kalso E. Genetics and genomics in postoperative pain and analgesia. Curr Opin Anaesthesiol. 2018;31:569–574. doi:10.1097/ACO.0000000000000633
34. Samad TA, Moore KA, Sapirstein A, et al. Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature. 2001;410:471–475. doi:10.1038/35068566
35. Sarkar S, Hobson AR, Hughes A, et al. The prostaglandin E2 receptor-1 (EP-1) mediates acid-induced visceral pain hypersensitivity in humans. Gastroenterology. 2003;124:18–25. doi:10.1053/gast.2003.50022
36. Siljehav V, Hofstetter AM, Leifsdottir K, Herlenius E. Prostaglandin E2 mediates cardiorespiratory disturbances during infection in neonates. J Pediatr. 2015;167:1207–1213 e1203. doi:10.1016/j.jpeds.2015.08.053
37. Soderlund J, Olsson SK, Samuelsson M, et al. Elevation of cerebrospinal fluid interleukin-1ss in bipolar disorder. J Psychiatry Neurosci. 2011;36:114–118. doi:10.1503/jpn.100080
38. Tarnasky PR. Post-cholecystectomy syndrome and sphincter of Oddi dysfunction: past, present and future. Expert Rev Gastroenterol Hepatol. 2016;10:1359–1372. doi:10.1080/17474124.2016.1251308
39. Wang YW, Zhang X, Chen CL, et al. Protective effects of Garcinol against neuropathic pain - evidence from in vivo and in vitro studies. Neurosci Lett. 2017;647:85–90. doi:10.1016/j.neulet.2017.03.015
40. Zackria R, Lopez RA. Postcholecystectomy Syndrome. Treasure Island (FL): StatPearls; 2021.
41. Zhang P, Bi RY, Gan YH. Glial interleukin-1beta upregulates neuronal sodium channel 1.7 in trigeminal ganglion contributing to temporomandibular joint inflammatory hypernociception in rats. J Neuroinflammation. 2018;15:117. doi:10.1186/s12974-018-1154-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.