")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Elevated HsCRP in Chronic Obstructive Pulmonary Disease: A Prospective Study of Long-Term Outcomes After Percutaneous Coronary Intervention
Authors Zheng Y , Qi Y, Seery S, Yang J, Li C, Wang W, Gao J, Meng X, Shao C, Tang YD
Received 4 July 2022
Accepted for publication 17 September 2022
Published 7 October 2022 Volume 2022:17 Pages 2517—2528
DOI https://doi.org/10.2147/COPD.S380194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Yitian Zheng,1– 3,* Yu Qi,1,* Samuel Seery,4,5 Jie Yang,2,3 Chen Li,2,3 Wenyao Wang,1 Jun Gao,1 Xiangbin Meng,1 Chunli Shao,1 Yi-Da Tang1
1Department of Cardiology and Institute of Vascular Medicine, Peking University Third Hospital, NHC Key Laboratory of Cardiovascular Molecular Biology and Regulatory Peptides, Key Laboratory of Molecular Cardiovascular Science, Ministry of Education, Beijing Key Laboratory of Cardiovascular Receptors Research, Beijing, People’s Republic of China; 2Department of Cardiology, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 4School of Humanities and Social Sciences, Chinese Academy of Medical Science & Peking Union Medical College, Beijing, People’s Republic of China; 5Faculty of Health and Medicine, Division of Health Research, Lancaster University, Lancaster, UK
*These authors contributed equally to this work
Correspondence: Yi-Da Tang, Department of Cardiology and Institute of Vascular Medicine, Peking University Third Hospital, NHC Key Laboratory of Cardiovascular Molecular Biology and Regulatory Peptides, Key Laboratory of Molecular Cardiovascular Science, Ministry of Education; Beijing Key Laboratory of Cardiovascular Receptors Research, Beijing, 100191, People’s Republic of China, Email [email protected]
Objective: Anti-inflammatory therapies are reported to have additional benefits beyond lipid control for patients with cardiovascular disease. However, no study has focused on the relationship between inflammation status and long-term outcomes for chronic obstructive pulmonary disease (COPD) patients, after percutaneous coronary intervention (PCI).
Methods: 277 COPD-PCI patients were divided into two groups according to hsCRP status upon admission. Major adverse cardiac events (MACE) in high hsCRP patients were compared to patients with low hsCRP. Restricted cubic spline (RCS) analysis was performed using MACE hazard ratios (HR) to investigate interrelations with hsCRP, as a continuous variable.
Results: Patients in the high hsCRP group incurred more inflammation activation, in terms of higher white blood cell counts, neutrophil, lymphocytes, and had higher smoking rates, compared to those with lower hsCRPs. A significant increase in MACEs was observed in hsCRP high group, compared to the low hsCRP group (HR: 2.47, 95% CI: 1.22– 5.00; p = 0.012). RCS curves suggest that HRs rise beyond 1.0, after the 0.24 juncture for Lg HsCRP (base 10 logarithm with hsCRP), HR per SD: 1.19 (95% CI: 0.96– 1.48). Further subgroup analysis implies that elevated hsCRP is associated with a higher risk of MACEs across the sub-groups tested.
Conclusion: HsCRP could be a useful indicator for COPD-CAD patient prognosis, after PCI. This is because hsCRP highlights inflammation activation. More multi-center research, designed for COPD-CAD patients should be conducted to more accurately determine the cut-off value for hsCRP.
Keywords: HsCRP, chronic obstructive pulmonary disease, coronary artery disease, percutaneous coronary intervention, outcomes
Introduction
Chronic obstructive pulmonary disease (COPD) and coronary artery diseases (CAD) are both leading causes of death around the world. Aside from the personal and financial consequences for individuals and their families, these conditions exert a great deal of pressure on health systems and upon social economics.1 The prevalence of COPD in those with CAD is more than 10%, although this is likely to be an underestimation because the pulmonary function test (PFT), which is used to identify COPD, is not so commonly used in clinical practice for CAD patients.2–4 Patients who suffer co-morbid COPD-CAD almost always have poorer outcomes, primarily, due to the multiplication of effects on blood vessels and in the lungs. Having COPD-CAD exponentially increases the likelihood of encountering severe dyspnea, inflammation activation, and metabolic dysfunction.5 In order to alleviate the manifestations of these additional co-morbidities we ought to develop more effective interventions although, we must first learn to identify those most at risk.
For those with COPD alone, it is held that the level inflammation can be used to determine outcomes, to some extent.6–8 Healthier lifestyles, stopping smoking and anti-inflammatory medication are generally prescribed and have been reported to improve COPD outcomes.2 Additionally, several large randomized clinical trials (RCTs) such as the CANTOS trial, which focused on anti-inflammation therapies, have reported benefits beyond lipid-control in CAD patients.9 However, having co-morbid COPD-CAD, generally occurs in older, smokers who also have metabolic syndrome (MeT). These all contribute to inflammation activation which, as has been mentioned, worsens outcomes. Percutaneous coronary intervention (PCI) could be seen as one of the most important therapies in coronary revascularization for COPD-CAD patients, due to the limited use of coronary artery bypass graft (CABG) in COPD patients. Even though revascularization therapy can help alleviate symptoms and improve outcomes, patients always encounter re-stenosis. This occurs for a number of reasons, including inflammation activation, platelet activation, and lipid accumulation in vessels wall. Therefore, we should study inflammation in COPD-CAD patients after PCI, which could be effective.
C-reactive protein (CRP) is an acute-phase reactant and non-specific marker for inflammation, which also increases in those who develop COPD or CAD.10 Researchers have reported a close relationship between cardiovascular outcomes and high-sensitivity C-Reactive-Protein (hsCRP), although early expert panels have rejected routine hsCRP testing in primary prevention.11 This is in spite of recent trials suggesting that hsCRP could be established for therapeutic development, and having observed effective alleviation of symptoms and improved outcomes.9,12 However, the cut-off point for high and low hsCRP values appear to vary between studies, ranging from 1 mg/l up to 3.76 mg/l. This is considered by some to misguide clinical practice because 2 mg//l has been established as a “general” cut-off point.10,13–15 To date, there is no research into the relationship between hsCRP and COPD-CAD, after PCI. Therefore, it would seem useful to assess the predictive value of hsCRP for COPD-CAD patients after PCI, and to generate some evidence-based recommendations around anti-inflammatory therapeutics for patients suffering co-morbid COPD-CAD.
Materials and Methods
Study Design
Consecutive CAD patients who received PCI in Peking University Third Hospital, Beijing were prospectively enrolled from 1st January 2014 until the 31st December 2019. Patients were required to complete PFT upon admission or within four weeks of discharge. Lab tests were collected upon admission and before PCI, to establish baseline measures. Patients with co-morbid COPD-CAD were identified and included in this study. Please see Figure 1 for further information.
 |
Figure 1 Flowchart of COPD patients receiving PCI therapy. Reasons for inclusion and exclusion when exploring the relationship between hsCRP and prognosis for COPD patients received PCI therapy are shown. Abbreviations: COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention; HsCRP, high-sensitivity C reactive protein; AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
Participants were deemed eligible if they were: 1) CAD patients who underwent PCI in our center; 2) aged 18 years and older; and 3) those with post-bronchodilator forced expiratory volume in the 1st second (FEV1)/forced vital capacity (FVC) ratio of less than 0.70, according to spirometric analysis.
Participants were excluded if they were: 1) patients with severe hepatic or renal dysfunction, malignancy, acute or chronic inflammatory disease; 2) patients without recorded hsCRP values; 3) patients with acute exacerbation of chronic obstructive pulmonary diseases (AECOPD) in the previous four weeks; and 4) patients with a history of trauma or surgery within the previous six months.
Ethical approval was acquired through Peking University Third Hospital Research Ethics Committee (No. M2021523). The study process was in accordance with the Declaration of Helsinki. Institutional Review Board approved the protocol. All patients were provided with information regarding the study objectives, before being asked to provide informed consent.
Participants
All COPD-CAD participants received PCI with procedural methods reliant upon specific operators. Baseline measures were collected independently by two researchers. Definition of patients’ characteristics were diagnosed according to the International Classification of Diseases (ICD-9).
COPD cases were diagnosed using spirometry, with post-bronchodilator forced expiratory volume in the 1st second (FEV1)/forced vital capacity (FVC) ratios of less than 0.70, in accordance with recommendations.2 Coronary artery disease was diagnosed through coronary angiography.
Participants were divided into two groups according to hsCRP levels. The median number of hsCRP in this sample was 1.70 mg/l. Therefore, patients were divided as follows: the first group included participants with a hsCRP < 1.70 mg/l, while the second group included those with an hsCRP ≥ 1.70 mg/l. Lg HsCRP was also calculated to assess the relationship between hsCRP and outcomes as continuous variables, with a base 10 logarithmic hsCRP.
Treatments
Patients who had not ingested long-term aspirin or P2Y12 inhibitors, received 300 mg of aspirin and an P2Y12 inhibitor at the loading dose, before receiving selective PCI. During PCI, patients received 50–100 U/kg of Heparin according to bleeding risk.
Follow-Up
Participants completed follow-up at 30 days, six months, and each year after PCI for 4 years. The final time of follow-up was conducted in July 2021. The primary endpoint for this study was major adverse cardiac events (MACE) at 4 years. MACEs were defined as cardiac death, target vessel revascularization (TVR), and non-fatal myocardial infarction (MI). Secondary endpoints consisted of components of MACE and all-cause death. Non-fatal myocardial infarction was defined as Type I myocardial infarction, after PCI. Cardiac death was defined as any death, which was not clearly of extracardiac origin, or myocardial infarction, according to guidelines.16 TVR was defined as angina or ischemia referable to the target vessel requiring repeat PCI or CABG.17
Follow-ups were completed by physicians via telephone or during outpatient visits by related clinical staff. Those “lost to follow-up”, were recorded as censored on the follow-up date. Participant characteristics, including demographics and lab tests etc., were included through the network hospital system by an independent investigator. This independent investigator was not informed of the purpose of the study, to avoid potential bias.
Statistical Analysis
This cohort study was conducted to investigate whether hsCRP could indicate the long-term outcomes for COPD-CAD patients underwent PCI. G*Power (v 3.1.7) was used to determine sample size at 95% power and with an effect size of 0.3. The minimum required sample size was calculated to be 220. Continuous variables are shown as means with SD, compared through Mann–Whitney’s U-test and Student’s T-tests. Categorical data are shown as counts with percentages, compared through Chi-square tests.
Missing laboratory values were imputed using multiple-imputation methods. Kaplan–Meier curves and two-sided Log rank tests were used to calculate cumulative event rates. Cox analysis was used to control for potential confounding factors.
Standardized differences between variables in the two groups were calculated to analyze the extent of differences. Bubble charts were also generated to visualize differences using p values. Co-linearity analysis was performed to explore the linearity and interrelations between Lg HsCRP and baseline variables.
Univariate and multivariate analysis were performed to identify possible predictors. Given the relatively small sample size, we decided to enlist variables with p value less than 0.1 under univariate analysis to the multivariate Cox model.
RCS analysis was performed to determine the correlations between the Lg HsCRP and HRs. Mantel-Cox method was used to calculate HRs. A p value less than 0.05 was thought to be statistically significant.
Subgroup analysis was performed to explore consistencies within subgroups in COPD-CAD participants. P for interactions were calculated to find the interactions between hsCRP and variables of subgroups. Here, p values < 0.05 were considered to be statistically significant.
Analyses were accomplished by two researchers (YZ at Fuwai, Hospital, YQ at Peking University Third Hospital) with guidance from an epidemiologist (SS). SPSS (version 26.0), GraphPad Prism (version 8.0), and RStudio (version 4.0) were used to perform all statistical analyses.
Results
Baseline Characteristics
277 consecutive COPD-CAD participants underwent PCI in our center were enrolled between January 2014 and December 2019. The mean follow-up for participants was 1360 days (SD = 591 days). As demonstrated before, participants were divided into two groups ie group A (low hsCRP group, n = 138); group B (high hsCRP group, n = 139), see Table 1 for further details.
 |
Table 1 Baseline Characteristics According to Different HsCRP Groups |
Patients in the high hsCRP group were more likely to smoke than those in the low hsCRP group (Current smoker (%): 55.4% vs 31.2%, p < 0.001, standardized difference % = 24.3%; past smoker: 74.8% vs 57.2%, p = 0.002, standardized difference % = 18.5%), with lower HDL-C (1.0 vs 1.1, p = 0.01, standardized difference % = 15.5%), and higher inflammation-related marker (White blood cell (*10^9/L): 8.7 vs 6.6, p < 0.001, standardized difference% = 35%; Neutrophil (*10^9/L): 6.1 vs 4.3, p < 0.001, standardized difference % = 32.1; Lymphocyte (*10^9/L): 1.8 vs 1.6, p = 0.024, standardized difference % = 13.4). In the high hsCRP group, patients also had slightly lower left ventricular ejection fraction (EF), overall (LVEF (%): 65.8 vs 69.2, p = 0.016, standardized difference % = 18.7). Please see Table 1 and Figure 2 for further details.
 |
Figure 2 Bubble chart of characteristic differences between the high and low HsCRP groups. Comparison of baseline variables was conducted through t test or Annova analysis for p value as described in the methods section. Standardized differences were measured to reflect the extent of differences. The green arrows on the y axis highlight standardized differences over 10% and p values less than 0.05. Abbreviations: HsCRP, high-sensitivity C reactive protein; CCS, chronic coronary syndrome; PCI, percutaneous coronary intervention; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Lp(a), lipoprotein a; HbA1C, hemoglobin A1C; LVEF, left ventricular eject fraction; LAD, left anterior descending; RCA, right coronary artery; LCX, left circumflex; TVD, three vessel disease; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; GOLD, global initiative for chronic obstructive disease; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; DAPT, dual antiplatelet therapy. |
Co-linearity analysis was performed to find correlations between the Lg HsCRP and baseline characteristics. We found that TC and LDL-C highly correlated with Lg HsCRP, of which variance inflation factors (VIFs) were all greater than 10, with a p value less than 0.05. In addition, there were correlations between white blood cell, neutrophil, lymphocyte, FEV1/FVC and the Lg HsCRP, with the VIFs over 10, and a marginal significant p value, respectively. These variables were also incorporated into univariate analysis and for further multivariate analysis to identify the predictive value for COPD-CAD patients after PCI (Supplementary Table 1).
Univariate and Multivariate Analysis
Univariate and multivariate analyses were performed to determine the predictive value of the hsCRP for MACEs in COPD-CAD patients underwent PCI at four years. The hsCRP attempt to be an independent factor predicting MACEs in COPD patients underwent PCI at median follow-up of 4 years (Group B vs Group A: HR:2.26, 95% CI: 1.03–4.97; Adjusted p = 0.043) (Supplementary Table 2).
Primary and Secondary Endpoints
Kaplan–Meiers curves for the Group B highlights an obvious increase in MACEs compared to Group A at four years after PCI (p = 0.012), Figure 3A. Further RCS curve appears to be linear with HR for MACEs significantly increasing as the Lg HsCRP increased over and above 0.24. For Lg HsCRP, the HR per SD was 1.19, with the 95% CI ranging from 0.96 to 1.48 (Figure 3B).
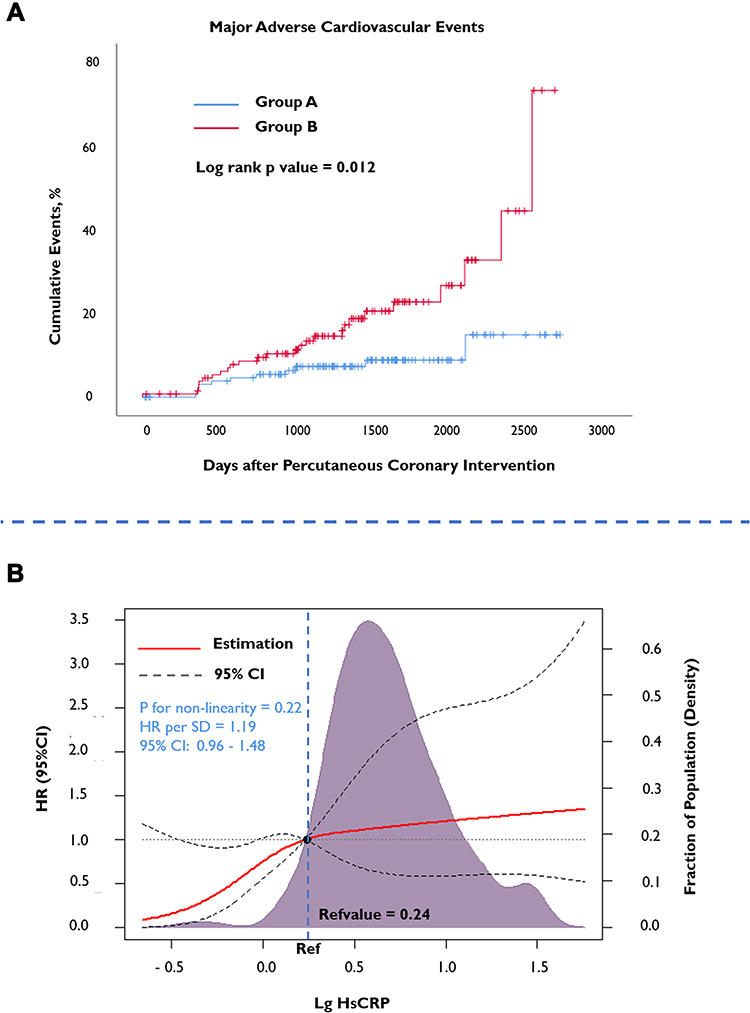 |
Figure 3 Kaplan–Meier curves and restricted cubic Spine curve according to primary endpoints. (A) Kaplan–Meier curves of the high HsCRP group and low HsCRP group for predicting the MACEs after percutaneous coronary intervention. (B) Restricted cubic spline of HsCRP and MACEs. HRs are indicated by red solid lines and 95% CIs by black dotted line. Density plot are presented by purple shadow area. Abbreviations: Ref, reference; HR, hazard ratio; CI, confidence interval; MACE, major adverse cardiovascular events; HsCRP, high-sensitivity C reactive protein. |
Table 2 provides evidence around secondary endpoints for comparisons between groups A and B. TVR significantly initiated the increase of MACEs across different groups (adjusted p = 0.039). HRs for TVR at two years in the Group B was higher than that in Group A (17.99% vs 7.25%; HR: 2.36, 95% CI: 1.04–5.36; adjusted p = 0.039). The incidence rate of MI and composite endpoint of MI and cardiac death also increased in Group B with low incidence rate (Cardiac death/MI: 2.16% vs 0.72%), although this does not appear significant. No other endpoints differed significantly among the groups at four years (Table 2).
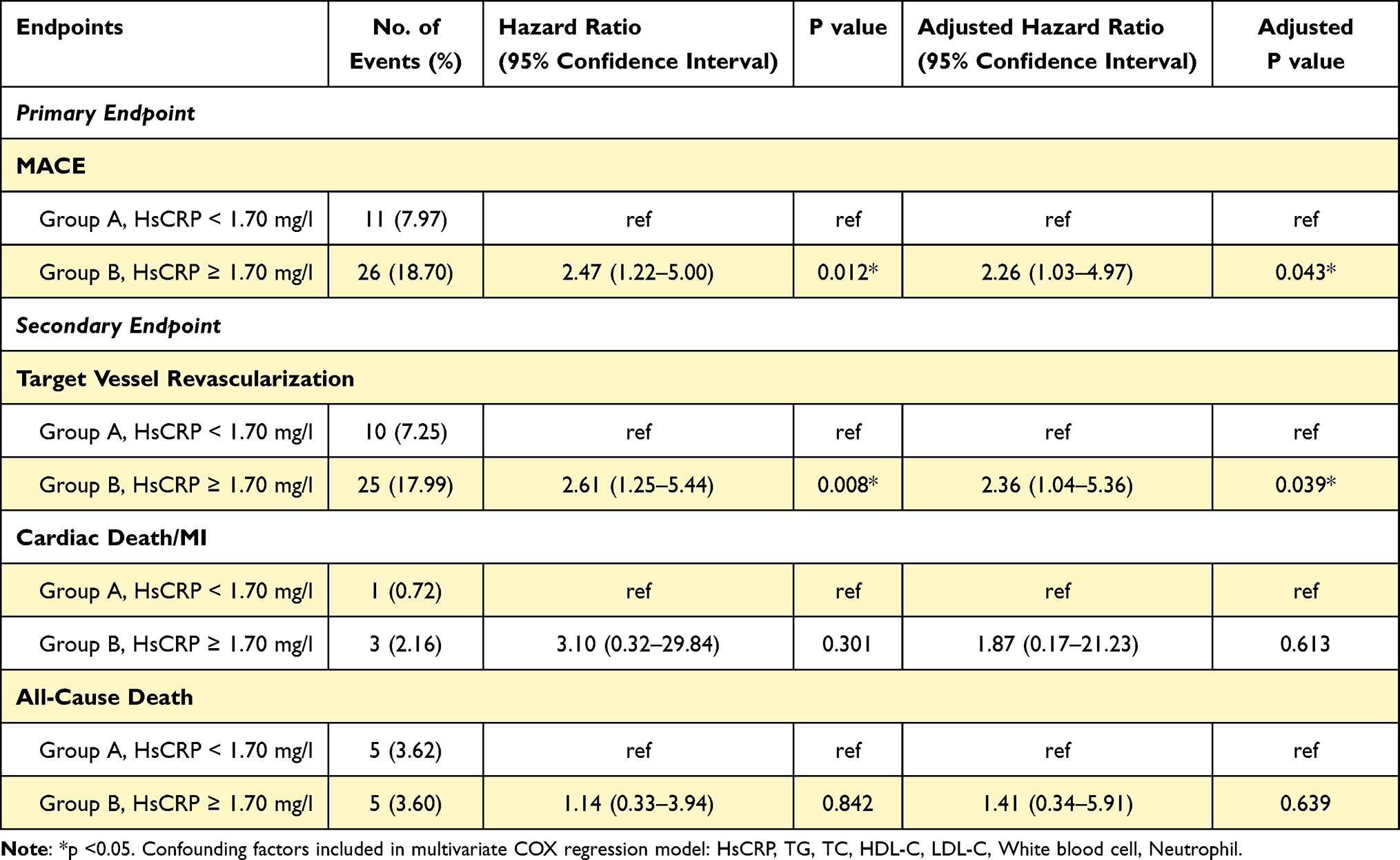 |
Table 2 Long-Term Outcomes According to HsCRP Levels Before and After Multivariate COX Regression Adjustment |
Subgroup Analysis
Subgroup analysis showed that all HRs in different subgroups were over one, including the gender, age, LDL-C groups, smoker, obesity, classification of CAD, hypertension, and the diabetes mellitus group. However, only p values in the patients older than 65 years old, male, not-current smokers, hyperlipidemia subgroup, and in hypertension patients were less than 0.05. No interactions between subgroups and hsCRP were observed (all P for interactions > 0.05), Table 3.
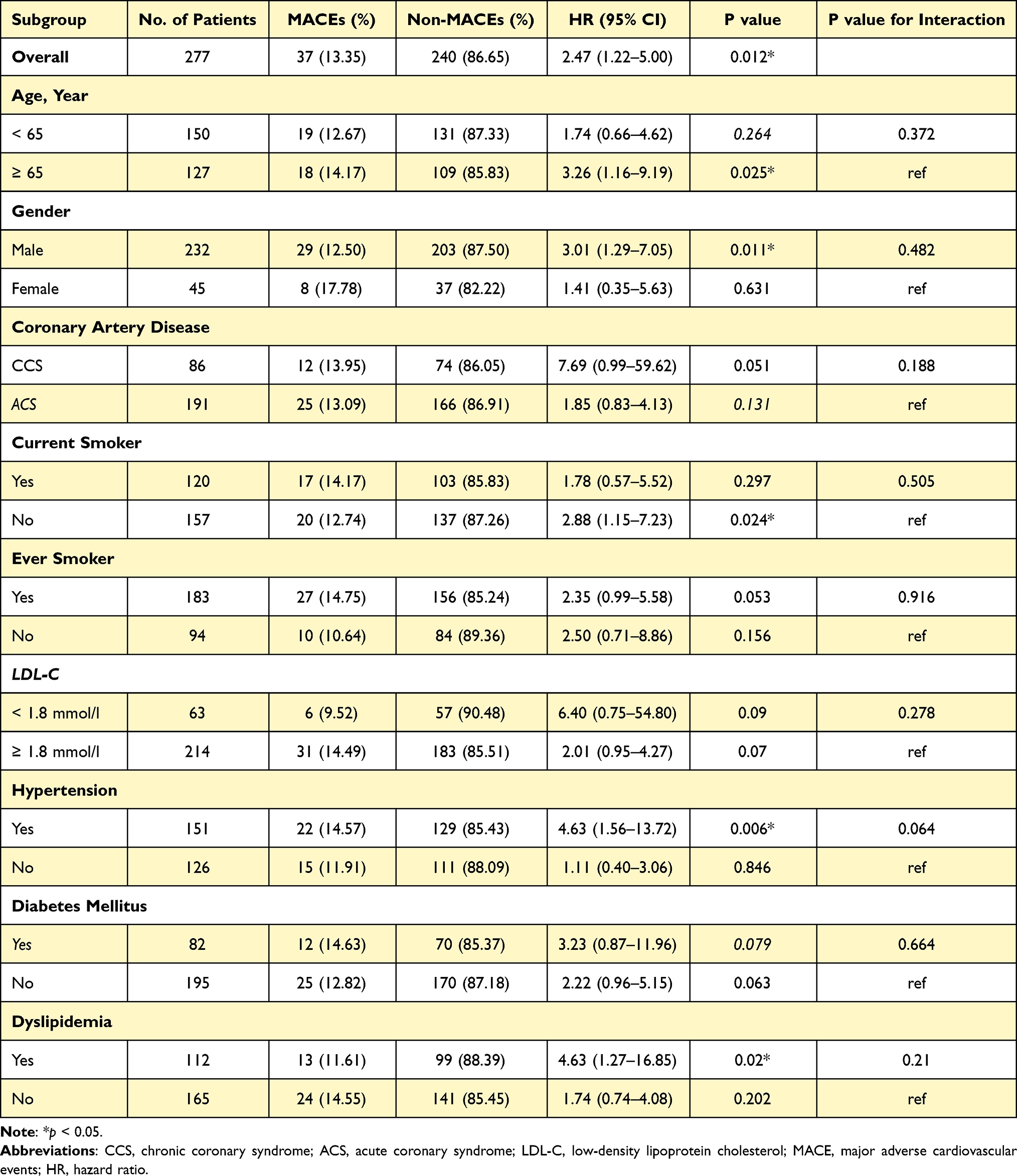 |
Table 3 Summary Table of Subgroup Analysis |
Discussion
This study aimed to assess hsCRP for COPD-CAD patients who received PCI. We found that having a high hsCRP is closely related to a higher incidence rate of MACEs after PCI in COPD-CAD patients and at long-term follow-up. We also found a positive correlation between Lg HsCRP and MACE hazard ratios, with an Lg HsCRP cut-off value of 0.24. This statistically significant correlation appears to occur when the Lg HsCRP increases beyond 0.24. This finding suggests that inflammation impacts on long-term prognosis for COPD-CAD patients after PCI. Therefore, we would suggest that hsCRP has predictive value in terms of outcomes. There is also the possibility to combine hsCRP with an anti-inflammatory therapy for COPD-CAD patients according to the Lg HsCRP cut-off identified here, ie, 0.24.
The function of hsCRP in those with both cardiovascular diseases and COPD has been proven in multiple clinical trials. For example, researchers have found that hsCRP is an effective surrogate measure for lipid metabolisation, inflammation, metabolic dysfunction, and immune system activation.10 According to the findings of this study, lipid profiles including TC, LDL-C, were also closely related to hsCRP levels. This finding is also consistent with previous research, which suggests that hsCRP with LDL-C can be used to accurately predict MACEs.18 This interrelationship does appear to indicate the potential involvement of hsCRP in the formation of atherosclerotic plaque, due to its correlation with lipid metabolisation.
Inflammation-related markers, such as white blood cell count and neutrophil among others, also appear to have a close relationship with hsCRP. However, these do not appear to have statistically significant predictive value in outcomes for COPD-CAD patients. The group considered to have high hsCRP levels also appear to have substantially higher white blood cell counts and/or neutrophil when compared to those with lower hsCRP. Even though within the normal range, this also appears to suggest these biomarkers are involved in an activation mechanism for inflammation in COPD-CAD patients. Multivariate analysis also appears to further suggest the importance of hsCRP, as opposed to lipid profiles, white blood count, and neutrophil in long-term outcome predictions for COPD-CAD patients.
COPD is generally believed to exert a hugely detrimental impact on CAD patients although, no related study has identified a suitable index for predicting outcomes in those with comorbid COPD-CAD. From a physiological perspective, there are a number of difficulties in understanding the pathogenesis involved in COPD and CAD using a specific indices or combination.5 HsCRP has been reported to reflect systemic inflammation and cardiovascular risk to certain extent8 although, these are generalized and may not be transposed to those with comorbid COPD-CAD. We found, compared with white blood cell counts, neutrophil, or other lipid parameters, that hsCRP is the most reliable factor and could be used in conjunction with anti-inflammatory therapies, where necessary. COPD-CAD patients could greatly benefit from anti-inflammatory therapies although identifying those in need has been an issue.
The hsCRP cut-off found in different trials has varied substantially from 1 mg/l up to almost 3 mg/l for predicting CAD patient outcomes. At an early stage, experts have used either 1 mg/l or 3 mg/l as the threshold for determining risk stratification.19 However, studies observed a great deal of heterogeneity across different ethnicities and within different CAD types. Recently, a large RCT which utilized 2 mg/l as the hsCRP cut-off to determine the anti-inflammation effect, found reasonably satisfactory results.20 Therefore, we are beginning to hone in on the most suitable hsCRP cut-point for predicting outcomes. Here, we used restricted cubic spine analysis to explore correlations between hsCRP and HR as a continuous variable. Considering hsCRP variations, which can be as high as 100 mg/l, or as low as 0.01 mg/l, we chose to use the Lg HsCRP to find the most suitable cut-off point for hsCRP. We found that that when the Lg HsCRP rose to 0.24, the hazard ratio began to increase beyond one, with the 95% CI including 1. Possible reasons for this may be the limited sample size in this study. We hypothesize that a larger sample would generate a more accurate Lg HsCRP cut-off. However, there were a number of issues with this study which will be discussed, not least of all the small sample size of 277 participants. That said, all patients in this study were diagnosed with co-morbid COPD-CAD using gold standards and all participants completed approximately a four year average follow-up period. Therefore, we can tentatively accept these findings as a reasonable representation of what could be expected in Chinese COPD-CAD patients.
Great variability in hsCRP level exists across ethnicities, with the highest levels observed in African Americans, followed by Hispanics, South Asians, white and East Asians.10 A report from National Health and Nutrition Examination Survey (NHANES) in America, suggests that hsCRP ranges from 0.1 to 296 mg/l.13 However, in this study, we found that hsCRP ranged from 0.01 to 110.23 mg/l. This appears to suggest that cut-off should be different for specific ethnicities when determining inflammation level. Lg HsCRP might be more appropriate as it may be less sensitive to variation.
Subgroup analysis was also conducted to understand other factors involved in outcomes. We found that even though Ps for interactions did not highlight significant interactions, this may have been because of the relative size of each subgroup. For those with a high level of hsCRP, and being 65 years of age and older, with hypertension, or dyslipidemia, and being a non-smoker may substantially increase the risk. However, given the small subgroup sample sizes we would recommend further research to validate this early assertion.
Strengths and Limitations
This study of hsCRP as a predictor of outcomes for COPD-CAD patients who received PCI therapy, provides physicians an option for assessing high-risk patients before starting anti-inflammatory therapeutics. While this study was the first to highlight a correlation between hsCRP and long-term outcomes of COPD-CAD patients, we were only able to involve a relatively small sample. The underlying controversy around which hsCRP cut-off point is more appropriate is ongoing; however, the method used here was quite novel and we managed to identify a clear cut-off point for COPD-CAD patients. It is important to recognize that this threshold could be different between ethnicities and may fluctuate according to sample sizes. We only enrolled patients from one center in this study and therefore we would recommend a larger, multicenter study in China as this may provide further insights.
Conclusion
HsCRP could be seen as the useful prognosis indicator for those COPD-CAD patients after PCI, due to the ability to highlight inflammation activation. The cut-off point between high or low hsCRP could be exist when Lg HsCRP equals 0.24. However, more multi-center research, designed for COPD-CAD patients should be conducted to more accurately determine the cut-off value for hsCRP.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Key R&D Program of China (2020YFC2004700), National Natural Science Foundation of China (81825003, 91957123, 81800327, 81900272), Beijing Nova Program (Z201100006820002) from Beijing Municipal Science & Technology Commission, and the Research Unit of Medical Science Research Management/Basic and Clinical Research of Metabolic Cardiovascular Diseases (2021RU003) from Chinese Academy of Medical Sciences.
Disclosure
Authors declare no conflicts of interest.
References
1. Roversi S, Fabbri LM, Sin DD, Hawkins NM, Agusti A. Chronic obstructive pulmonary disease and cardiac diseases. an urgent need for integrated care. Am J Respir Crit Care Med. 2016;194(11):1319–1336. doi:10.1164/rccm.201604-0690SO
2. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
3. Almagro P, Lapuente A, Pareja J, et al. Underdiagnosis and prognosis of chronic obstructive pulmonary disease after percutaneous coronary intervention: a prospective study. Int J Chron Obstruct Pulmon Dis. 2015;10:1353–1361. doi:10.2147/COPD.S84482
4. Campo G, Guastaroba P, Marzocchi A, et al. Impact of COPD on long-term outcome after ST-segment elevation myocardial infarction receiving primary percutaneous coronary intervention. Chest. 2013;144(3):750–757. doi:10.1378/chest.12-2313
5. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):149. doi:10.1183/16000617.0057-2018
6. Williams MC, Murchison JT, Edwards LD, et al.Coronary artery calcification is increased in patients with COPD and associated with increased morbidity and mortality. Thorax. 2014;69(8):718–723.
7. Fabbri L, Rabe KJL. From COPD to chronic systemic inflammatory syndrome? Lancet. 2007;370(9589):797–799. doi:10.1016/S0140-6736(07)61383-X
8. Zhang XL, Chi YH, Wang le F, Wang HS, Lin XM. Systemic inflammation in patients with chronic obstructive pulmonary disease undergoing percutaneous coronary intervention. Respirology. 2014;19(5):723–729. doi:10.1111/resp.12295
9. Weber C, von Hundelshausen P. cantos trial validates the inflammatory pathogenesis of atherosclerosis: setting the stage for a new chapter in therapeutic targeting. Circ Res. 2017;121(10):1119–1121. doi:10.1161/CIRCRESAHA.117.311984
10. Yousuf O, Mohanty BD, Martin SS, et al. High-sensitivity C-reactive protein and cardiovascular disease: a resolute belief or an elusive link? J Am Coll Cardiol. 2013;62(5):397–408. doi:10.1016/j.jacc.2013.05.016
11. US Preventive Services Task Force. Using nontraditional risk factors in coronary heart disease risk assessment: u.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(7):474–482.
12. Blaha M, Budoff M, De Filippis A, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: implications for the Jupiter population from Mesa, a population-based cohort study. Lancet. 2011;378(9792):684–692. doi:10.1016/S0140-6736(11)60784-8
13. Ridker P, Cannon C, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005;352(1):20–28. doi:10.1056/NEJMoa042378
14. Ridker P, Danielson E, Fonseca F, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359(21):2195–2207. doi:10.1056/NEJMoa0807646
15. Detrano R, Guerci A, Carr J, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–1345. doi:10.1056/NEJMoa072100
16. Tehrani DM, Seto AH. Third universal definition of myocardial infarction: update, caveats, differential diagnoses. Cleve Clin J Med. 2013;80(12):777–786. doi:10.3949/ccjm.80a.12158
17. Brener SJ, Ertelt K, Mehran R, et al. Predictors and impact of target vessel revascularization after stent implantation for acute ST-segment elevation myocardial infarction: lessons from HORIZONS-AMI. Am Heart J. 2015;169(2):242–248. doi:10.1016/j.ahj.2014.11.005
18. Ridker P, Rifai N, Rose L, Buring J, Cook N. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002;347(20):1557–1565. doi:10.1056/NEJMoa021993
19. Buckley D, Fu R, Freeman M, Rogers K, Helfand M. C-reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann Intern Med. 2009;151(7):483–495. doi:10.7326/0003-4819-151-7-200910060-00009
20. Everett B, MacFadyen J, Thuren T, Libby P, Glynn R, Ridker P. Inhibition of interleukin-1β and reduction in atherothrombotic cardiovascular events in the CANTOS trial. J Am Coll Cardiol. 2020;76(14):1660–1670. doi:10.1016/j.jacc.2020.08.011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.