")
Back to Journals » International Journal of General Medicine » Volume 14
Eight Trigrams Boxing Combined with Wenyang Huoxue Recipe Improves Cardiopulmonary Motor Function and the Quality of Life of Patients with Coronary Heart Disease
Authors Hu XZ, Zhou M, Weng JH
Received 15 June 2021
Accepted for publication 14 September 2021
Published 2 November 2021 Volume 2021:14 Pages 7557—7566
DOI https://doi.org/10.2147/IJGM.S318269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiao-Zhen Hu, Miao Zhou, Jia-Hao Weng
Department of Internal Medicine-Cardiovascular, Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Jia-Hao Weng
Department of Internal Medicine-Cardiovascular, Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, No. 274 of Zhijiang Middle Street, Jingan District, Shanghai, 200071, People’s Republic of China
Tel +86 21 56639828
Fax +86 21 56639828
Email [email protected]
Objective: To investigate the therapeutic effects of Eight Trigrams Boxing combined with a Wenyang Huoxue recipe on the cardiopulmonary motor function and quality of life in patients with coronary heart disease after an interventional operation (percutaneous coronary intervention [PCI]); further, to provide new clinical evidence and ideas for integrated traditional Chinese and Western medicine in cardiac rehabilitation.
Methods: Sixty patients were selected and successfully underwent PCI in designated hospitals after four weeks, from June 2018 to September 2020. The patients were randomly divided into a treatment group and control group, and both groups were given standard pharmaceuticals after PCI and the Wenyang Huoxue recipe. The treatment group was additionally treated with the Eight Trigrams Boxing Method. The control group was provided with aerobic rehabilitation exercise. The maximum oxygen uptake (VO2max), metabolic equivalent (MET), the results of a 6-min walking test, the Seattle Angina Questionnaire (SAQ) score, SF-36 score, and other indicators were evaluated before and after treatment. The therapeutic effect was evaluated by comparison between the groups and within the groups.
Results: The VO2max, MET, 6-min walking distance, SAQ score, and SF-36 score in both groups improved after treatment compared with before treatment. There was no difference between the two groups before treatment. However, after treatment, the VO2max, MET, 6 min walking distance, SAQ score, and SF-36 score in the treatment group were higher compared with the control group.
Conclusion: A traditional Chinese medicine cardiac rehabilitation program of Eight Trigrams Boxing combined with a Wenyang Huoxue recipe can improve the cardiopulmonary function and quality of life of patients. The therapeutic effect was clear and is worthy of further investigation.
Keywords: eight trigrams boxing, Wenyang Huoxue recipe, cardiac rehabilitation, cardio-pulmonary function, quality of life
Corrigendum for this paper has been published
Introduction
A significant number of individuals suffer from cardiovascular disease in China, and the prevalence of the disease and mortality rates are increasing. There are over 910,000 interventional treatment cases of coronary heart disease in mainland China.1 Percutaneous coronary intervention (PCI) and other solutions can reconstruct blood supply and restore the blood supply of ischemic myocardium rapidly and are widely used in clinical practice as the most effective method at present.2,3 However, after PCI, myocardial ischemia-reperfusion injury,4 saphenous vein bypass graft restenosis, the progression of inherent coronary artery lesions, heart dysfunction, decreased exercise tolerance, psychological disorders, and other problems could be raised. Thus, avoiding these problems, reducing the incidence of acute events, and promoting better recovery following PCI are important issues that must be urgently addressed.5,6
Cardiac rehabilitation, which is derived from rehabilitation medicine, has become an important element in the treatment of cardiovascular disease.7 A meta-analysis revealed that cardiac rehabilitation reduced the number of high-risk factors in patients with cardiovascular disease, improved their quality of life, and reduced the rate of readmission and mortality.8 Overseas studies have shown that cardiac rehabilitation can reduce the all-cause mortality rate after myocardial infarction by 8–37% and the cardiovascular mortality rate by 7%–38%, which is an important factor in determining treatment and the patient’s quality of life.9–12 A randomized controlled study in China confirmed the feasibility of cardiac rehabilitation through aerobic exercise in patients with coronary heart disease.13 Hence, increasing attention has been paid to cardiac rehabilitation after coronary heart disease intervention.
Traditional Chinese medicine (TCM) emphasizes the importance of health maintenance and rehabilitation in cardiac rehabilitation.14,15 Yang deficiency blood stasis syndrome is the basic pathogenesis of patients following PCI. Our center created a Wenyang Huoxue recipe to treat patients with Yang deficiency blood stasis syndrome after coronary artery PCI and conducted a systematic study on cardiac rehabilitation of integrated traditional Chinese and Western medicine. It has been showed that Yang deficiency blood stasis syndrome is the most common syndrome in PCI patients with coronary heart disease in China.16 We selected Eight Trigrams Boxing with a Wenyang Huoxue recipe as a TCM cardiac rehabilitation program as a means of achieving satisfactory results in a short period for this type of syndrome. When patients practice Eight Trigrams Boxing with deep slow breathing, the diaphragm sinks and increases, and the chest volume increases. Massaging the middle burner (the portion of the body housing the stomach and spleen) can strengthen blood circulation. Taking slow and deep breaths increases the rise amplitude of the diaphragm, improves abdominal and pelvic blood circulation, speeds up blood return, enhances the diaphragm activity range, increases tidal volume, and improves lung function, which is in line with the central and peripheral effects of exercise therapy for coronary heart disease. We hope to investigate the effect of eight Trigrams Boxing with a Wenyang Huoxue recipe on the PCI patients with coronary heart disease, and provide study ideas and theoretical basis for the treatment of PCI patients with coronary heart disease.
Method
Diagnosis Standard
Western medicine diagnostic criteria: The International Society of Cardiology and Association’s Nomenclature and Diagnostic Criteria for Ischemic Heart Disease and the criteria for compliance with PCI indications formulated by the WHO.
Patients who conformed to the TCM syndrome diagnostic criteria per related dialectical criteria in the Cardiovascular Branch of China Association of Traditional Chinese Medicine’s 2019 Guide for the Diagnosis and Treatment of Stable Angina Pectoris with Coronary Heart Disease.17
Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Patients met the diagnostic criteria of Western medicine and successfully underwent PCI for the first time at four weeks after surgery; (2) Aged between 40–75 years; (3) Met the diagnostic criteria in the low- and medium-risk stratification of cardiac rehabilitation for CHD; (4) Patients with blood stasis syndrome, Yang Qi deficiency syndrome on TCM syndrome differentiation; (5) NYHA cardiac function grade level I–II; (6) Patients could comply with the treatment and all follow-ups.
Exclusion Criteria:(1) PCI performed within one month for acute myocardial infarction; (2) Patients with high-risk stratification of cardiac rehabilitation for coronary heart disease; (3) Patients who had undergone re-PCI due to restenosis; (4) Patients complicated with severe arrhythmia, heart failure, and cardiogenic shock; (5) Patients complicated with other severe systematic diseases, such as chronic cor pulmonale, malignancy, liver, and kidney insufficiency or mental diseases; (6) Patients unable to move or cooperate with the treatment.
Criteria for Loss of Follow-Up and Exclusion
(1) Patients who failed to receive treatment according to the protocol were considered lost to follow-up. (2) Patients who withdrew spontaneously or did not complete the whole course of treatment thus influencing therapeutic effect were excluded.
Randomization and Blinding
The patients were randomly divided into two groups (control group and treatment group) in ration 1:1 with the SPSS 24.0 software. The random allocation sequences were concealed in the opaque envelopes preserved by an administrator not involved in the trial. Blind method was conducted to all clinical investigators and patients.
Patients
The patients included in the present study were selected from 68 patients who successfully underwent PCI for four weeks in the Department of Cardiology of the Shanghai Hospital of Traditional Chinese Medicine and Shanghai Tenth People’s Hospital from June 2018 to September 2020. All the patients participated in this trial provided the informed consent. The sample size was calculated by a type I error of 0.05 and the power of 90%, and 59 patients were needed.
Treatment
The patients were divided into a treatment group (30 cases) and a control group (30 cases). Both groups were given standard pharmaceuticals after PCI and a Wenyang Huoxue recipe. The treatment group was treated with the Eight Trigrams Boxing method. The control group was given aerobic rehabilitation exercise. The patients were observed for 12 weeks, and the specific treatment was as follows:
(1) Conventional Western medicine was utilized in both groups: The Western medicine routine treatment and health education were conducted with reference to the Guide for Percutaneous Coronary Intervention in China (2016). In addition, according to the syndrome differentiation of TCM, it was classified as a Yang deficiency blood stasis syndrome and treated with a Wenyang Huoxue recipe containing Radix aconiti carmichaeli, angelica sinensis, raw pollen typhae, red peony root, white peony root, aurantii, and platycodon grandiflorum, one bag for each treatment, t.i.d., P.O., with continued administration for 12 weeks.
(2) Stage II exercise rehabilitation treatment was conducted for both groups. The specific implementation measures in rehabilitation and exercise therapy were as follows: before the two groups were enrolled in the study, they had to first pass a cardiopulmonary exercise test. The study then assessed the patients’ motor ability and customized the rehabilitation prescription for the training. The details are as follows:
Patients in both groups were given 5–10 minutes of preparation and relaxation exercises before and after each treatment, including static muscle stretching and dynamic muscle activity.
Aerobic exercise: ① Treatment group: Eight Trigrams Boxing was the main intervention. The method was as follows: both hands held a triple burner. Each hand alternated in quick succession in the manner of drawing a bow. Lifting was conducted with one hand to regulate the spleen and stomach while looking backward to relieve exhaustion or lesions in the five internal organs. The head was wagged to remove internal heat, two hands touched the feet to exercise the kidneys and waist, boxing was performed to increase strength. Seven steps on tiptoe were made to relieve illness. The Eight Trigram Boxing Intervention is formulated according to the principle of FITT (frequency, intensity/time and type). Refer to the Eight Trigram Boxing key points issued by the fitness Qigong management center of the State General Administration of sports as the standard, once a day, twice a time; Practice 3 days a week, synthesize 40–80% of the maximum heart rate reserve or oxygen uptake reserve, and Borg rating of perceived exertion scale 12–16 points as an auxiliary index for objective measurement of heart rate. Individualized exercise guidance shall be given, starting from low intensity and gradually. The exercise time was 20–30 min each session. ② Control group: Exercise time: 20–60 min each time; Exercise type: adopt warm-up aerobic exercise resistance exercise combined with flexibility balance training recovery sequential exercise program. The start time of warm-up and recovery exercise should be 5–10 minutes. Each aerobic exercise should be 15–20 minutes/group for twice. The initial aerobic exercise of each group should start from 15 minutes. After 5 times of exercise rehabilitation training, the aerobic exercise of each group should be increased to 20 minutes. Initial flexibility training and balance training for 5 minutes respectively. A total of 12 weeks. Two groups of aerobic exercise used walking and treadmill.
Relaxation exercises: flexibility and muscle relaxation was practiced for 5–10 minutes. The frequency was three times per week.
(3) Treatment cycle: Continuous treatment for 12 weeks was regarded as a treatment cycle, and the indexes were observed and detected before and 12 weeks after treatment.
Outcome Measures
(1) Main observation indicators:
Motor cardiac function evaluation: A cardiopulmonary exercise test (CPET) was conducted for the evaluation. The VO2max in both groups was evaluated before and after treatment.
(2) Secondary observation indicators:
① MET evaluation: a CPET was conducted for the evaluation before and after treatment. ② Six-minute walking test. Based on the 6-min walking test guide (ATS, 2002), the 6-min walking distance of patients in both groups was measured, and patients’ fatigue during walking was evaluated according to the Borg fatigue assessment scale. Testing was stopped immediately if a patient developed chest pain, intolerant dyspnea, lower limb spasms, staggering while walking, profuse sweating, or a pale complexion. The patients were evaluated before and after treatment.
(3) Follow-up visit for clinical symptoms and improvement in quality of life
Clinical symptoms and quality of life were evaluated with the Seattle Angina Questionnaire (SAQ) and the SF-36 Health Survey (SF-36) before and after administration. The SAQ aims to evaluate health conditions related to angina, including 19 questions and five health conditions associated with coronary heart disease: Frequency of angina, limitation of motion, quality of life, the stability of angina pectoris, and satisfaction with treatment. SF-36 scoring covers eight areas of general health, including vitality, physical functioning, bodily pain, general health perceptions, physical role functioning, emotional role functioning, social role functioning, and mental health. A Chinese version of the SF-36 scale was used to measure the two groups of patients, and the scores of the SF-36 scale were counted. The higher the total score, the better the quality of life. Scores for the 8 areas were calculated and summed, and the initial score was converted to a standard score of 0–100. The subjects were consulted before filling out the form to answer any questions. Study personnel gave explanations or filled in the form for patients with a low educational level who could not understand the meaning of the questions after obtaining their consent.
(4) Safety indicators
Routine blood tests, coagulation function, liver and kidney function, blood glucose, blood lipids, and myocardial enzymes were conducted to evaluate the safety of the medicines. They were evaluated before treatment and six months after treatment.
Efficacy Evaluation Criteria
(1) Evaluation for physical fitness and aerobic capacity
Cardiac function, aerobic exercise capacity, and cardiac reserve capacity were evaluated based on the VO2max, which is the gold standard for cardiorespiratory fitness.
Motor cardiac function – level A: VO2max >20 (mL/min/Kg)
Motor cardiac function – level B: VO2max 16–20 (mL/min/Kg)
Motor cardiac function – level C: VO2max 10–16 (mL/min/Kg)
Motor cardiac function – level D: VO2max <10 (mL/min/Kg)
(2) The intensity and prognosis of cardiac rehabilitation exercise were evaluated based on MET.
Classification criteria for cardiac function quantified by MET (NYHA)
Cardiac function Level I: MET≥7 (Unrestricted daily activities)
Cardiac function Level II: MET≥5 and <7 (Physical activity is slightly restricted)
Cardiac function Level III: MET≥2 and <5 (Physical activity is obviously limited)
Cardiac function Level IV: MET<2 (At rest, there are also symptoms of cardiac insufficiency or angina pectoris. Any physical activity will increase discomfort)
(3) Evaluation criteria for the 6-min walking test.
The evaluation was conducted based on the combination of a 6-min walking test (6MWT) and the Borg Rating of Perceived Exertion scale combined with the patients’ cardiac function. It should be noted that 6MWT which is easy to administer and well tolerated could reflect the real situation.18 It has been reported that the intensity of the tests in CR are related.19 Patients were asked to walk as quickly as possible to measure the distance of a 6-min walk: <150 m, severe cardiac insufficiency; 150–425 m, moderate cardiac insufficiency; 426–550 m, mild cardiac insufficiency.20
Statistical Methods
Excel software was used to create a database, and SPSS20.0 software was used for the statistical analysis. Mean ± standard deviation was used to present the measurement data. Data conformed to normal distribution and homogeneity of variance. A paired sample t test was used within the group, and an independent sample t test was used between the groups before and after treatment. Measurement data were expressed as (%). In the two-sided test, P < 0.05 was statistically significant.
Results
Baseline Characteristics
Three patients were excluded from the study due to distrust of TCM, poor compliance, and halfway termination; five were excluded due to being lost to follow-up; following this, 60 patients were enrolled in the study. Demographic and clinical characteristics are presented in Table 1. There were 26 male patients and 14 female patients in the treatment group and 28 male patients and 12 female patients in the control group. The average age of the treatment group was 60.85 ± 11.31 years, and the average age of the control group was 62.42 ± 8.47 years. The differences in age, gender, underlying diseases, and smoking and drinking behavior between the two groups were not statistically significant.
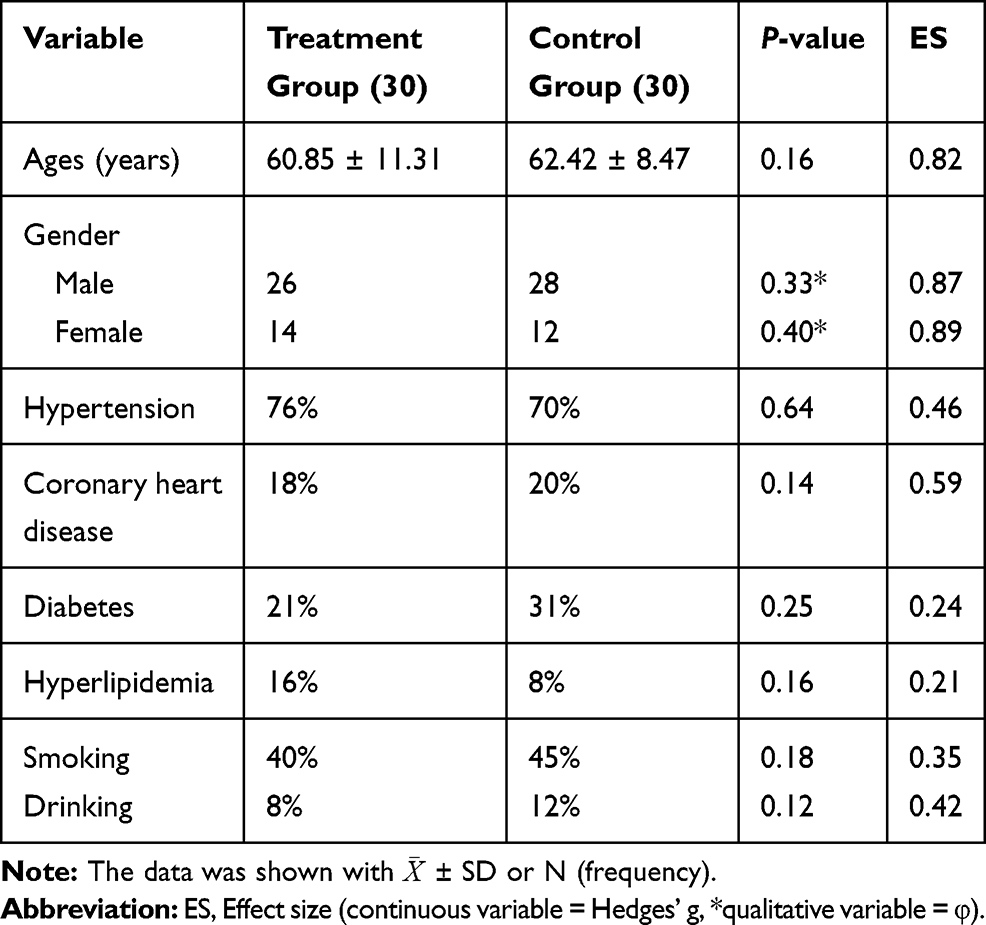 |
Table 1 Baseline of Enrolled Patients |
Comparison of Cardiopulmonary Function of the Patients in the Two Groups Before and After Treatment
The VO2max and METS of the patients in two groups after treatment were statistically increased. In addition, before the treatment, the VO2max and METS of the patients in two groups were no significant different. However, after the treatment, the VO2max and METS of the treatment group were significantly higher compared with that of the control group, which indicated that the cardiopulmonary ability of the treatment group was achieving better improved than that of the control group (Table 2).
 |
Table 2 Comparison of Cardiopulmonary Function of the Patients in That Two Groups Before and After Treatment |
Comparison of the 6-Min Walking Test of the Patients in Two Group Before and After Treatment
The results was shown in Table 2. The 6-min walking distance of the patients in two groups after treatment was significantly improved when compared with that of the patients in two groups before treatment. After treatment, the 6-min walking distance of patients in the treatment group was significantly longer than that of the patients in the control group.
Comparison of SAQ Scores of the Patients in Two Groups After Treatment
The results was shown in Table 3. In the treatment group, angina stability, angina attack frequency, body limitation, satisfaction with treatment, cognition of disease, and five other aspects were significantly improved following treatment compared with that of the patients in control group.
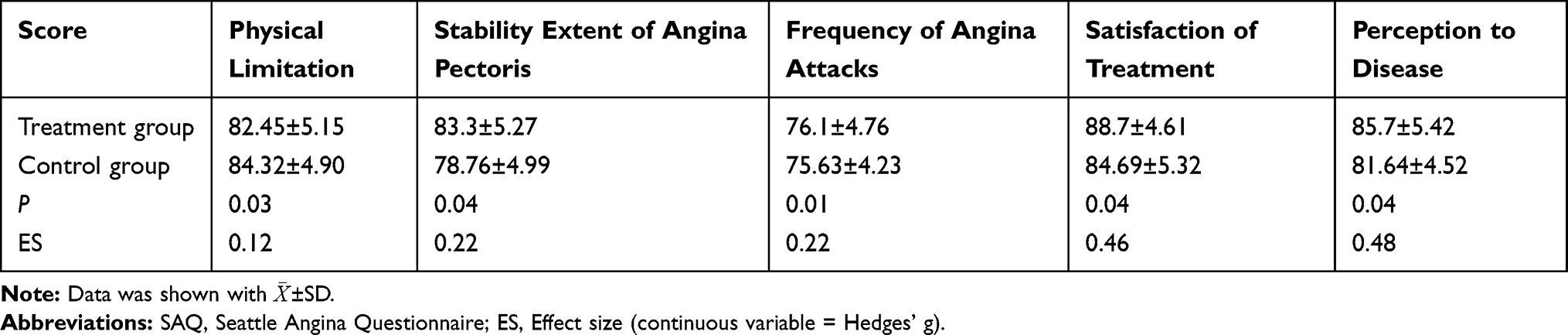 |
Table 3 Comparison of SAQ Scores of Patients Between the Two Groups After Treatment |
Comparison of SF-36 Score of the Patients in Two Group Before and After Treatment
The results was shown in Table 4. After treatment, patients in the treatment group had higher SF-36 scores when compared with that of patients in the treatment group before treatment (P<0.05). Scores for physiological function, physical pain, and stamina of patients in the control group after treatment were higher compared with that of the patients before treatment (P<0.05). After treatment, scores for physical pain, mental health, social function, emotional function, and general health in the treatment group were significantly higher compared with that of the patients in control group.
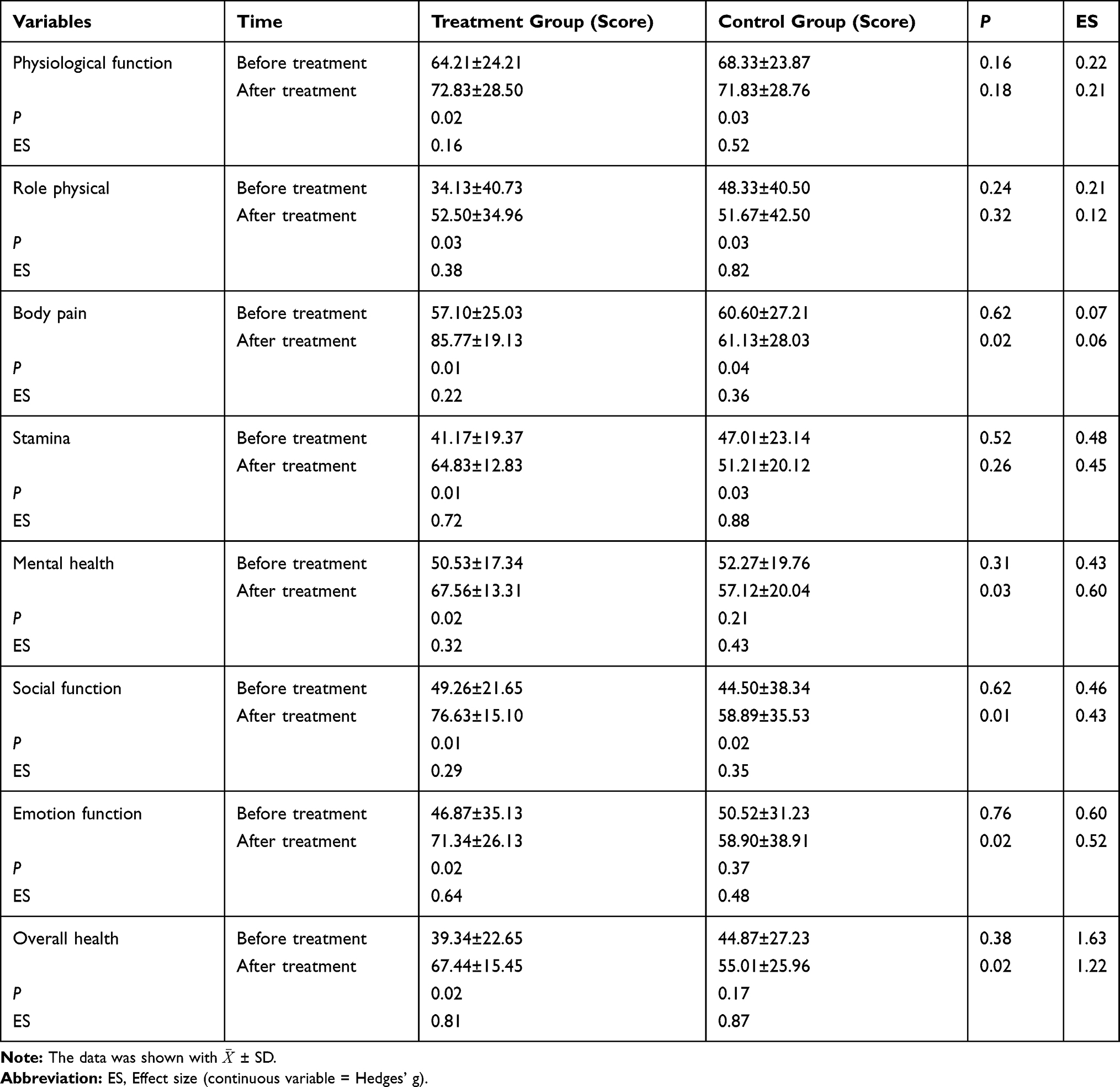 |
Table 4 Comparison of SF-36 Score of Patients in Two Groups Before and After Treatment |
Discussion
Although PCI for coronary heart disease opens the narrow coronary artery, greatly improving acute myocardial ischemia and infarction and saving lives, it cannot completely address the major risk factors for coronary heart disease and cannot prevent the progression of atherosclerosis.21 In the post-operation stage, local vascular injury, inflammatory reactions, and other factors promote the occurrence of vascular restenosis.22 As a result, patients show different degrees of tension, irritability, and even anxiety and depression after PCI, which affects the quality of life and prognosis of these patients.23 Hence, after PCI through cardiac rehabilitation, improving the cardiac function and quality of life of patients with coronary heart disease has become a crucial aspect of the combination of the prevention and treatment of cardiovascular disease. The efficacy and the importance of this treatment have been widely recognized clinically.24
Cardiac rehabilitation has also been scientifically evaluated, and five main interventions (drugs, exercise, smoking cessation, life, psychological), as well as mental health education and other treatments, have been shown to effectively reduce the risk of recurrent myocardial infarction and sudden death in patients after PCI.25–28 Cardiac rehabilitation can help patients improve their quality of life and return to their everyday social activities.29,30 Studies have shown that cardiac rehabilitation therapy can effectively promote the recovery of cardiac function and increase coronary blood flow and cardiac function storage in patients after PCI.31 Research has suggested that cardiac rehabilitation following PCI could delay the development of atherosclerosis, reduce occurrence of the restenosis rate and usage of conventional Western medicine, as well as the economic burden of the disease, meanwhile improve patients’ psychological health and quality of life.32
The cardiac rehabilitation after PCI by TCM belongs to the traditional medical rehabilitation system, which requires rich theoretical and clinical experience in cardiac rehabilitation.33 With the introduction of TCM, integrated TCM, and Western medicine for cardiac rehabilitation, the importance of cardiac rehabilitation in TCM is increasingly widely recognized as a mean of improving the efficacy of the intervention and patients’ quality of life. In this context, the present study explores the improvement in patients’ quality of life after PCI using a traditional Chinese recipe combined with routine cardiac rehabilitation.
Coronary atherosclerotic heart disease falls within the categories of “chest stuffiness and pains,” “angina,” and “precordial pain with cold limbs” in TCM and is frequently seen in the elderly. The progress of the disease is complicated from onset to the development of symptoms to recovery following treatment.25,26 In the early stage of the disease, the pathogenesis is mostly blood stasis, which blocks the meridians and collaterals, leading to thoracic artery paralysis and impedance, and the manifestations are mainly chest pain and chest tightness.25–27 Following stent implantation, patients’ manifestations are poor heart qi, deficiency of Qi and blood, deficient blood supply, and impotence.34 The syndrome develops into qi deficiency and blood stasis.35 The clinical results showed that chest tightness, chest pain, and other manifestations of qi stagnation and blood stasis were often accompanied by fatigue, shortness of breath, and other signs of qi deficiency.36 In the late stage of rehabilitation, deficiency is the main symptom.28–30 There is also a lack of Yang Qi and a sensation of chills and weakness, as well as a Yang deficiency blood stasis syndrome in the cold environment.37 TCM cardiac rehabilitation emphasizes disease prevention and the prevention and treatment of transmission.38 Improving various physiological indexes and symptoms and the recovery of patients’ mental state and social function are the main focuses of TCM. TCM offers many unique, effective, and easily conducted treatment methods, such as traditional Chinese medicine, acupuncture, and acupoints. A series of treatments can improve patients’ conditions and help them recover sooner.
Yang could increase the vitality in the clinical practice of cardiovascular disease.36,39,40 In addition, the basic pathogenesis after PCI is heart-yang deficiency and failure, which is largely related with blood stasis.37 Wenyang Huoxue recipe, in which a small amount of aconite is designed to warm the Yang. Angelica sinensis, pollen typhae, and red paeonia lactiflora can promote blood circulation and remove blood stasis, while fluctuation of Fructus Aurantii and Platycodon grandiflorum can adjust qi movement. The movement of qi leads to the movement of blood. This formula reflects the academic approach to treating qi and blood at the same time by warming the Yang and activating the blood while balancing the Yin and Yang of the Qi and blood. The full prescription has only seven medicinal, with small dose, though the clinical efficacy is good, and the cost performance is reasonably high.
In the present study, after 12 weeks of intervention, the VO2max, MET, 6-min walking distance, SAQ score, and SF36 score in the treatment group and control group after treatment improved when compared with that of patients before treatment. At the same time, the VO2max, MET, 6-min walking distance, SAQ score, and SF-36 score in the treatment group after treatment were higher when compared with that of the patients in control group, which indicated that the Eight Trigrams Boxing combined with a Wenyang Huoxue recipe as a cardiac rehabilitation program of TCM significantly improved the cardiopulmonary function and quality of life of patients after coronary stenting. Previous studies also demonstrated that exercise training in patients with coronary heart disease could increase VO2MAX, the ability to maintain physical activity and the quality of life.41–44
This study also has some limitations. Firstly, the current study belongs to exploratory study with small sample size. Besides, in this study diet control is not carried out, and many objective factors will influence the condition of patients and affect the experimental results. Therefore, based on this study, a large sample size, multicenter RCT would be carried out for the further study to verify the effectiveness and safety of Eight Trigrams Boxing combined with Wenyang Huoxue Recipe on cardiopulmonary motor function and the quality of life of patients with coronary heart disease. Overall, in light of these findings, the suggestion is to integrate the advantages of TCM, acupuncture, massage, and traditional techniques into the diagnosis and treatment system of modern Chinese and Western medicine for cardiac rehabilitation to flexibly combine theory and technology. This would enable a scientific cardiac rehabilitation program of integrated traditional Chinese and Western medicine to gradually be comprehensively developed and subsequently promoted. In terms of specific implementation, it is necessary to draw on the advanced technical approaches to rehabilitation in Western medicine and adopt scientific rehabilitation diagnosis and treatment schemes and processes to provide a scientific basis for cardiac rehabilitation. It is also important to make full use of the characteristics of TCM, inherit and innovate the essence of TCM rehabilitation, and highlight the advantages of “preventing disease before disease onset and preventing disease from exacerbating,” thereby acknowledging the importance of TCM in cardiac rehabilitation.
Conclusion
The VO2max, MET, 6-min walking distance, SAQ score, and SF-36 score of the patients in treatment group after treatment are higher than that of the patients in control group after treatment. The results indicated that Eight Trigrams Boxing combined with Wenyang Huoxue Recipe could improve cardiopulmonary motor function and the quality of life of patients with coronary heart disease. The trend of conducting cardiac rehabilitation through an integrated approach of traditional Chinese and Western medicine is likely to continue in the future.
Funding
This study was supported by Shanghai Municipal Health Commission Research Project (2021–2023) and Clinical study of Wenyang Huoxue Decoction combined with Stage II cardiac rehabilitation on the improvement of cardiac function and quality of life after coronary heart disease intervention (Project No. 202050259).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hu S, Gao R, Liu L, et al. [Summary of Chinese Cardiovascular Disease Report 2018]. Chin J Circ. 2019;34(3):209–220. in Chinese with English abstract.
2. Sawant AC, Bhardwaj A, Banerjee K, et al. Fractional flow reserve guided percutaneous coronary intervention results in reduced ischemic myocardium and improved outcomes. Catheter Cardiovasc Interv. 2018;92(4):692–700. PMID: 29405553. doi:10.1002/ccd.27525
3. Doenst T, Bonow RO, Bhatt DL, Falk V, Gaudino M. Improving terminology to describe coronary artery procedures: JACC review topic of the week. J Am Coll Cardiol. 2021;78(2):180–188. PMID: 34238439. doi:10.1016/j.jacc.2021.05.010
4. Cassese S, Byrne RA, Tada T, et al. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart. 2014;100(2):153–159. doi:10.1136/heartjnl-2013-304933
5. Olsen SJ, Schirmer H, Bønaa KH, Hanssen TA. Cardiac rehabilitation after percutaneous coronary intervention: results from a nationwide survey. Eur J Cardiovasc Nurs. 2018;17(3):273–279. doi:10.1177/1474515117737766
6. Beatty AL, Bradley SM, Maynard C, McCabe JM. Referral to cardiac rehabilitation after percutaneous coronary intervention, coronary artery bypass surgery, and valve surgery: data from the clinical outcomes assessment program. Circ Cardiovasc Qual Outcomes. 2017;10(6):e003364. PMID: 28619725. doi:10.1161/CIRCOUTCOMES.116.003364
7. Price KJ, Gordon BA, Bird SR, Benson AC. A review of guidelines for cardiac rehabilitation exercise programmes: is there an international consensus? Eur J Prev Cardiol. 2016;23(16):1715–1733. doi:10.1177/2047487316657669
8. Haykowsky M, Scott J, Esch B, et al. A meta-analysis of the efects of exercise training on left ventricular remodeling fol- lowing myocardial infarction: startearly and go longer for greatest exercise benefits on remodeling. Trials. 2011;12:92. doi:10.1186/1745-6215-12-92
9. Peixoto TC, Begot I, Bolzan DW, et al. Early exercise-based rehabilitation improves health-related quality of life and functional capacity after acute myocardial infarction: a randomized controlled trial. Can J Cardiol. 2015;31:308–313. doi:10.1016/j.cjca.2014.11.014
10. Qinghua L. The Impact of Cardiac Rehabilitation Exercise on Cardiopulmonary Capacity and Life Quality of the Patients with Myocardial Infarction. Atlantis Press; 2014.
11. Zhang QY, Hu Q, Li Y, et al. Efficacy of CPET combined with systematic education of cardiac rehabilitation after PCI: a real-world evaluation in ACS patients. Adv Ther. 2021;38:4836–4846. PMID: 34351565. doi:10.1007/s12325-021-01871-y
12. Tamulevičiūtė-Prascienė E, Beigienė A, Thompson MJ, Balnė K, Kubilius R, Bjarnason-Wehrens B. The impact of additional resistance and balance training in exercise-based cardiac rehabilitation in older patients after valve surgery or intervention: randomized control trial. BMC Geriatr. 2021;21(1):23. PMID: 33413144; PMCID: PMC7792183. doi:10.1186/s12877-020-01964-3
13. Cao RY, Zheng H, Mi Q, et al. Aerobic exercise-based cardiac rehabilitation in Chinese patients with coronary heart disease: study protocol for a pilot randomized controlled trial. Trials. 2018;19(1):363. doi:10.1186/s13063-018-2771-8
14. Zhang S, Liang C, Yang Y, Zhao Z, Li J, Meng X. Effects of Yangxinshi tablet on exercise tolerance in patients with coronary heart disease: a protocol of randomized, double-blind, placebo-controlled, and multi-center trial. Medicine. 2020;99(31):e21485. PMID: 32756176; PMCID: PMC7402915. doi:10.1097/MD.0000000000021485
15. Jiang Y, He Q, Zhang T, Xiang W, Long Z, Wu S. Exploring the mechanism of Shengmai Yin for coronary heart disease based on systematic pharmacology and chemoinformatics. Biosci Rep. 2020;40(6):BSR20200286. PMID: 32436944; PMCID: PMC7286881. doi:10.1042/BSR20200286
16. Chu FY, Wang J, Yao KW, Li ZZ. Effect of Xuefu Zhuyu Capsule on the symptoms and signs and health-related quality of life in the unstable angina patients with blood-stasis syndrome after percutaneous coronary intervention: a Randomized controlled trial. Chin J Integr Med. 2010;16(5):399–405. PMID: 20535581. Chinese. doi:10.1007/s11655-010-9999-9
17. Cardiovascular Disease Prevention and Rehabilitation Committee of Integrated Traditional Chinese and Western Medicine of China Association for the Promotion of Traditional Chinese Medicine. Expert suggestions of external treatment of traditional chinese medicine in cardiac rehabilitation. J Integr Traditional West Med Cardio-Cerebrovasc Dis. 2017;15(1):53–58.
18. CACM Cardiovascular branch. Guidelines for the diagnosis and treatment of stable angina pectoris in coronary heart disease. J Traditional Chin Med. 2019;60(21):1880–1890.
19. Saba MA, Goharpey S, Attarbashi Moghadam B, Salehi R, Nejatian M. Correlation between the 6-min walk test and exercise tolerance test in cardiac rehabilitation after coronary artery bypass grafting: a cross-sectional study. Cardiol Ther. 2021;10(1):201–209. PMID: 33586086; PMCID: PMC8126529. doi:10.1007/s40119-021-00210-0
20. Yueying F. Guiding effect of 6-minute walking test on rehabilitation training of patients with chronic heart failure [J]. World Latest Med Info Dig. 2017;80:178–179.
21. Fiorina C, Vizzardi E, Lorusso R, et al. The 6-min walking test early after cardiac surgery. Reference values and the effects of rehabilitation programme. Eur J Cardiothorac Surg. 2007;32(5):724–729. doi:10.1016/j.ejcts.2007.08.013
22. Shipman JN, Agasthi P. Orbital atherectomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan. PMID: 33085291.
23. Malik TF, Tivakaran VS. Percutaneous transluminal coronary angioplasty. In: StatPearls [Internet]. Treasure Island (FL):: StatPearls Publishing; Jan 2020.
24. Salari A, Rouhi Balasi L, Ashouri A, Moaddab F, Zaersabet F, Nourisaeed A. Medication adherence and its related factors in patients undergoing coronary artery angioplasty. J Caring Sci. 2018;7(4):213–218. doi:10.15171/jcs.2018.032
25. Sandercock GRH, Cardoso F, Almodhy M, Pepera G. Cardiorespiratory fitness changes in patient receiving comprehensive outpatient cardiac rehabilitation in the United Kingdom: a multicentre study. Heart. 2012;99(11):785–790. doi:10.1136/heartjnl-2012-303055
26. Pepera GK, Bromley PD, Sandercock GRH. A pilot study to investigate the safety of exercise training and exercise testing in cardiac rehabilitation patients. Br J Cardiol. 2013;20:78. doi:10.5837/bjc.2013.012
27. Pepera G, Sandercock G. Does turning affect shuttle walking test performance in cardiovascular disease patients? A narrative review. Critical Rev Phy Rehabil Med. 2021;33(1):17–29. doi:10.1615/CritRevPhysRehabilMed.2021037594
28. Pepera GK, Sandercock GR, Sloan R, Cleland JGF, Ingle L, Clark AL. Influence of step length 6-minute walk test performance in patients with chronic heart failure. Physiotherapy. 2012;98(4):330–334. doi:10.1016/j.physio.2011.08.005
29. Pepera G, Cardoso F, Taylor MJ, Peristeropoulos A, Sandercock GR. Predictors of the shuttle walking test performance in patients with cardiovascular disease. Physiotherapy. 2013;99(4):317–322. doi:10.1016/j.physio.2013.01.003
30. Pepera G, Ingle L, Sandercock GR. Predictors of the 6-minute walk test in patients with chronic heart failure. Br J Cardiac Nurs. 2015;10(9):454–459. doi:10.12968/bjca.2015.10.9.454
31. Amsterdam EA, Wenger NK, Brindis RG, et al.; ACC/AHA Task Force Members. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(25):e344–426.
32. Zhang Y, Cao H, Jiang P, Tang H. Cardiac rehabilitation in acute myocardial infarction patients after percutaneous coronary intervention: a community-based study. Medicine. 2018;97(8):e9785. doi:10.1097/MD.0000000000009785
33. Anderson L, Thompson DR, Oldridge N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2016;1:CD001800.
34. Li FH, Guo SW, Zhan TW, et al. Integrating network pharmacology and experimental evidence to decipher the cardioprotective mechanism of Yiqihuoxue decoction in rats after myocardial infarction. J Ethnopharmacol. 2021;279:114062. PMID: 33771641. doi:10.1016/j.jep.2021.114062
35. Yu L, Lu X, Li X, et al. A study protocol for a randomized, double-blind, placebo-controlled clinical study on the effect of Qishen Yiqi dripping pills on exercise endurance and quality of life in patients with coronary heart disease after percutaneous coronary intervention. Evid Based Complement Alternat Med. 2021;2021:7439852. PMID: 34475964; PMCID: PMC8407996. doi:10.1155/2021/7439852
36. Zhao C, Wang W, Yan K, Sun H, Han J, Hu Y. The therapeutic effect and mechanism of Qishen Yiqi dripping pills on cardiovascular and cerebrovascular diseases and diabetic complications. Curr Mol Pharmacol. 2021;14. PMID: 34382512. doi:10.2174/1874467214666210811153610
37. Hou J, Wang J, Lin C, et al. Circulating MicroRNA profiles differ between Qi-Stagnation and Qi-Deficiency in coronary heart disease patients with blood stasis syndrome. Evid Based Complement Alternat Med. 2014;2014:926962. PMID: 25548593; PMCID: PMC4273468. doi:10.1155/2014/926962
38. Sha JY, Liu H, Xie YM, Zhuang Y. [Clinical application characteristics of Ciwujia Injection in treatment of 5 904 cases with cardiovascular disease in real world]. Zhongguo Zhong Yao Za Zhi. 2020;45(15):3525–3532. PMID: 32893540. Chinese. doi:10.19540/j.cnki.cjcmm.20200616.501
39. Nie D, Jiang G, Liu W, et al. The connotation and advantages of traditional Chinese medicine cardiac rehabilitation. Med J PLA. 2017;29(2):36–39.
40. Health Qigong Management Center of General Administration of Sport of China. Fitness Qigong Baduan Jin. Beijing: People’s Sports Press; 2013:195.
41. Wisløff U, Støylen A, Loennechen JP, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients. Circulation. 2007;115:3086–3094. doi:10.1161/CIRCULATIONAHA.106.675041
42. Edwards DG, Schofield RS, Lennon SL, Pierce GL, Nichols WW, Braith RW. Effect of exercise training on endothelial function in men with coronary artery disease. Am J Cardiol. 2003;93(5):617–620. doi:10.1016/j.amjcard.2003.11.032
43. Heran BS, Chen JM, Ebrahim S, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochran Database Syst Rev. 2011;6:7.
44. Anderson L, Oldridge N, Thompson DR, et al. Exercise based cardiac rehabilitation for coronary heart disease. J Am Col Cardiol. 2016;67(1):1–12. doi:10.1016/j.jacc.2015.10.044
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.