")
Back to Journals » OncoTargets and Therapy » Volume 11
EGFR, KRAS, BRAF, PTEN, and PIK3CA mutation in plasma of small cell lung cancer patients
Authors Lu HY , Qin J , Han N, Lei L, Xie F, Li C
Received 12 December 2017
Accepted for publication 19 March 2018
Published 20 April 2018 Volume 2018:11 Pages 2217—2226
DOI https://doi.org/10.2147/OTT.S159612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samir Farghaly
Hong-Yang Lu,1–3 Jing Qin,2,3 Na Han,2,3 Lei Lei,2 Fajun Xie,2,3 Chenghui Li3
1Department of Oncology, Wenzhou Medical University, Wenzhou, People's Republic of China; 2Zhejiang Key Laboratory of Diagnosis and Treatment Technology on Thoracic Oncology (Lung and Esophagus), Zhejiang Cancer Hospital, Hangzhou, People's Republic of China; 3Department of Thoracic Medical Oncology, Zhejiang Cancer Hospital, Hangzhou, P.R. China
Background: Small cell lung cancer (SCLC) is an aggressive and deadly neuroendocrine tumor derived from bronchial epithelial cells. Although it results in a 95% mortality rate, the development of targeted therapies for SCLCs has lagged behind. The aim of this study is to better research mutation characteristics of SCLC and identify potential biomarkers for target therapy.
Methods: We utilized high- resolution melting analysis to identify the mutations in epidermal growth factor receptor (EGFR), Kirsten rat sarcoma viral oncogene (KRAS), v-raf murine sarcoma viral oncogene homolog B1 (BRAF), phosphatase and tensin homolog (PTEN), and phosphatidylinositol-3-kinase catalytic (PIK3CA) from the blood. A cohort of 99 SCLC patients including 44 limited-stage disease patients and 55 extensive-stage disease patients were prospectively collected.
Results: EGFR 18 (G719X) mutation was found in 5 patients, EGFR 19 (del) mutation in 2, EGFR 20 (T790M) in 3, EGFR 21 (L858R) in 2, KRAS 2 (G13D) in 5, BRAF 15 (V600E) in 1, PIK3CA 9 (E542K) in 1, and no mutations in PTEN 5 (R130G), PTEN 6 (R173C), PTEN 8 (T319fs*1), and PIK3CA 20 (H1047R) were identified. Among these patients, two harbored EGFR double mutation, one patient with EGFR double mutation and KRAS 2 (G13D) mutation.
Conclusion: The mutation form of EGFR may differ from lung adenocarcinoma, and mutations of KRAS, BRAF, and PIK3CA were rare in SCLC. These results aided us in comprehensively analyzing genetic features and laid the foundation for exploring the possibility of target therapy.
Keywords: epidermal growth factor receptor, small cell lung cancer, plasma, high-resolution melting
Introduction
Small cell lung cancer (SCLC), which accounts for 15% of all the lung cancers, is an extremely aggressive disease with particularly poor survival rates.1 Most often, the SCLC patients are categorized into the limited-stage disease (LD) or extensive-stage disease (ED) according to the Veterans Administration Lung Study Group (VALSG) staging system. Furthermore, rapid doubling time and early onset dissemination are the main characteristics of SCLC. SCLC is also characterized by initial chemosensitivity, and the first-line treatment of choice is the platinum-based regimen, usually cisplatin and etoposide.2,3 However, despite initial high response rates to chemotherapy, SCLC inevitably relapses. The follow-up treatment for relapsed SCLC is still a challenge. Currently, target therapies and immunotherapeutic agents are under clinical investigation.4,5 However, most of them have limited efficacy, and till now, there is no efficient drug approved for SCLC.6 Thus, discovering novel predictive biomarkers to differentiate subtypes of SCLC for personalized treatments is the urgent need.
Epidermal growth factor receptor (EGFR) is a transmembrane protein that is a receptor for members of the EGF family of extracellular protein ligands. When endogenous ligands, such as EGF, bind to EGFR, receptor homodimerization or heterodimerization occurs at the cell surface and eventually leads to internalization of the dimerized receptor.7 After receptor dimerization, the autophosphorylation of the intracytoplasmic EGFR tyrosine kinase domain will happen to stimulate the intracellular signal transduction cascade through several downstream pathways.8 The mutations in EGFR exons 18, 19, and 21 in NSCLC are correlated to the response of tumors to tyrosine kinase inhibitors (TKIs). More concretely, short in-frame deletions in exon 19 and a specific point mutation in exon 21 at codon 858 are the most common EGFR mutations in NSCLC patients and correlated with the sensitive response of small-molecule EGFR-TKI.3,4 Whereas the T790M gatekeeper point mutation at exon 20, accounting for ~50% of all cases, is reported to be the most frequently observed resistance mechanism.9 Kirsten rat sarcoma viral oncogene (KRAS) is a GTP-binding protein, involved in G-protein-coupled receptor signaling. The mutation status of the KRAS gene predicts the therapeutic efficacy of EGFR-TKIs in NSCLC. The patients with the wild-type KRAS gene may benefit from the TKI therapy.10 v-raf murine sarcoma viral oncogene homolog B1 (BRAF) kinase links the RAS GTPase to the downstream signaling pathway of KRAS to phosphorylate the MEK protein directly. The mutations in the BRAF gene increase the kinase activity and, in turn, the constitutive stimulation of MAPK2 and MAPK3. The rate of mutation in the BRAF gene in NSCLC is relatively low. BRAF mutations could predict the effect of MEK inhibitors on NSCLC cells.11 Phosphatase and tensin homolog (PTEN) regulates several physiological processes by inhibiting the phosphoinositide 3-kinase-v-akt murine thymoma viral oncogene homolog-mammalian target of rapamycin pathway (PI3K/AKT/mTOR pathway) through its lipid phosphatase activity. Shibata et al showed that the mutation in phosphatidylinositol-3-kinase catalytic α (PIK3CA) in SCLC cells renders them more sensitive to tricribine than the cells with the wild-type gene. Moreover, the SCLC cells harboring a cisplatin-resistant subclone of PIK3CA mutant were sensitive to tricribine similar to those without the resistance.12,13 Another study reported one adenocarcinoma patient with an L858R mutation in EGFR who displayed a robust response to erlotinib (first line of drug). The largest nodule progressed after 1 year. The core biopsy of this lesion revealed a histological transformation to SCLC that carried the L858R mutation in EGFR and acquired a PIK3CA mutation that disappeared after 6 months. Subsequently, the patient with the histological transformation to adenocarcinoma responded to a repeat course of erlotinib as the second-line course treatment.14 Le et al revealed a lack of response to EGFR TKIs in EGFR-mutated de novo SCLC and large cell neuroendocrine carcinomas.15 Therefore, elucidating the mutations in EGFR, KRAS, BRAF, PTEN, and PIK3CA in SCLC is imperative.
Two prospective studies from Taiwan and Japan reported 2.6% and 4% EGFR mutations, respectively.16,17 Surgery can be used in SCLC patients with T1-2N0M0, which is <5% of all the SCLC patients. Thus, obtaining tumors for the detection of EGFR mutation in SCLC patients is rather challenging.18 High-resolution melting (HRM) is a precise method, with 92% sensitivity and 100% specificity, for detecting the EGFR mutation using formalin-fixed tissues. This approach is also useful in predicting the clinical outcomes of NSCLC patients treated with gefitinib.19 Thus, the simplicity, promptness, high sensitivity, and low rate of false-positive mutation in the HRM analysis renders it to be an optimal approach for detecting the EGFR mutations in circulating DNA of lung cancer patients.20,21 In order to distinguish the mutation status of EGFR, KRAS, BRAF, PTEN, and PIK3CA in SCLC patients, we used the HRM technology to assess the genes in the plasma samples.
Materials and methods
Patients
From August 2012 to December 2015, 99 SCLC patients (10 females and 89 males) were prospectively assimilated in this study from the Zhejiang Cancer Hospital, People’s Republic of China. The pathological diagnosis comprising of 98 conventional SCLC and 1 combined SCLC was based on the standard criteria defined by World Health Organization Classification. The mean age of patients was 60 years (range, 24–79 years). The stages as per the VALSG were as follows: LD in 44 patients and ED in 55 patients. These encompassed 14 patients who were nonsmokers, 1 patient was light, 3 were moderate, and 81 were heavy smokers. The mean pack-years was 46 (range, 0–150). The characteristics of 99 SCLC patients are summarized in Table 1. The study was approved by the Medical Ethical Committee of Zhejiang Cancer Hospital, and the patients signed the informed consent.
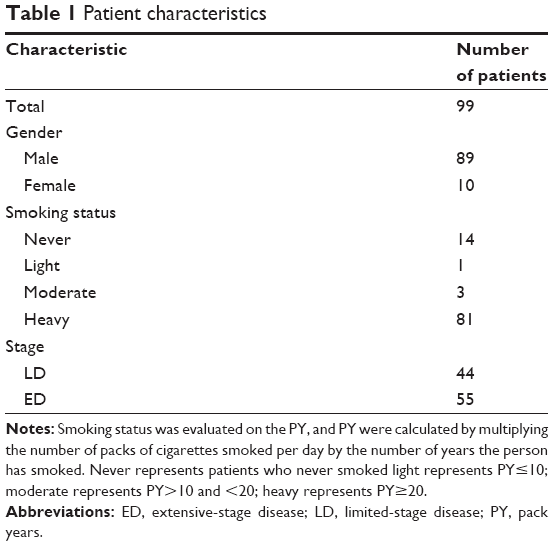 | Table 1 Patient characteristics |
Detection of gene mutation using HRM
A total of 99 blood samples were included in this study for assessing EGFR, KRAS, BRAF, PTEN, PIK3CA mutations. Five milliliters of vascular blood samples was withdrawn in EDTA-anticoagulation tubes. The plasma was isolated from blood samples by centrifugation at 4,000 rpm for 10 min. Then, DNA was extracted from the plasma samples using the High Pure PCR Template Preparation Kit (Roche, Mannheim, Germany) according to the manufacturer’s protocol. Human genomic DNA obtained from Suzhou MicroDiag Biomedical Co., Ltd (Suzhou, People’s Republic of China) was utilized as the control sample.
Eleven primer pairs were designed (Suzhou MicroDiag) to span codons 18 (G719X), 19 (del), 20 (T790M), and 21 (L858R) of the EGFR gene, codon 2 (G13D) of the KRAS gene, codon 15 (V600E) of the BRAF gene, codons 5 (p.R130G), 6 (p.R173C), and 8 (p.T319fs*1) of the PTEN gene, and codons 9 (p.E542K) and 20 (p.H1047R) of the PIK3CA gene (Table 2).
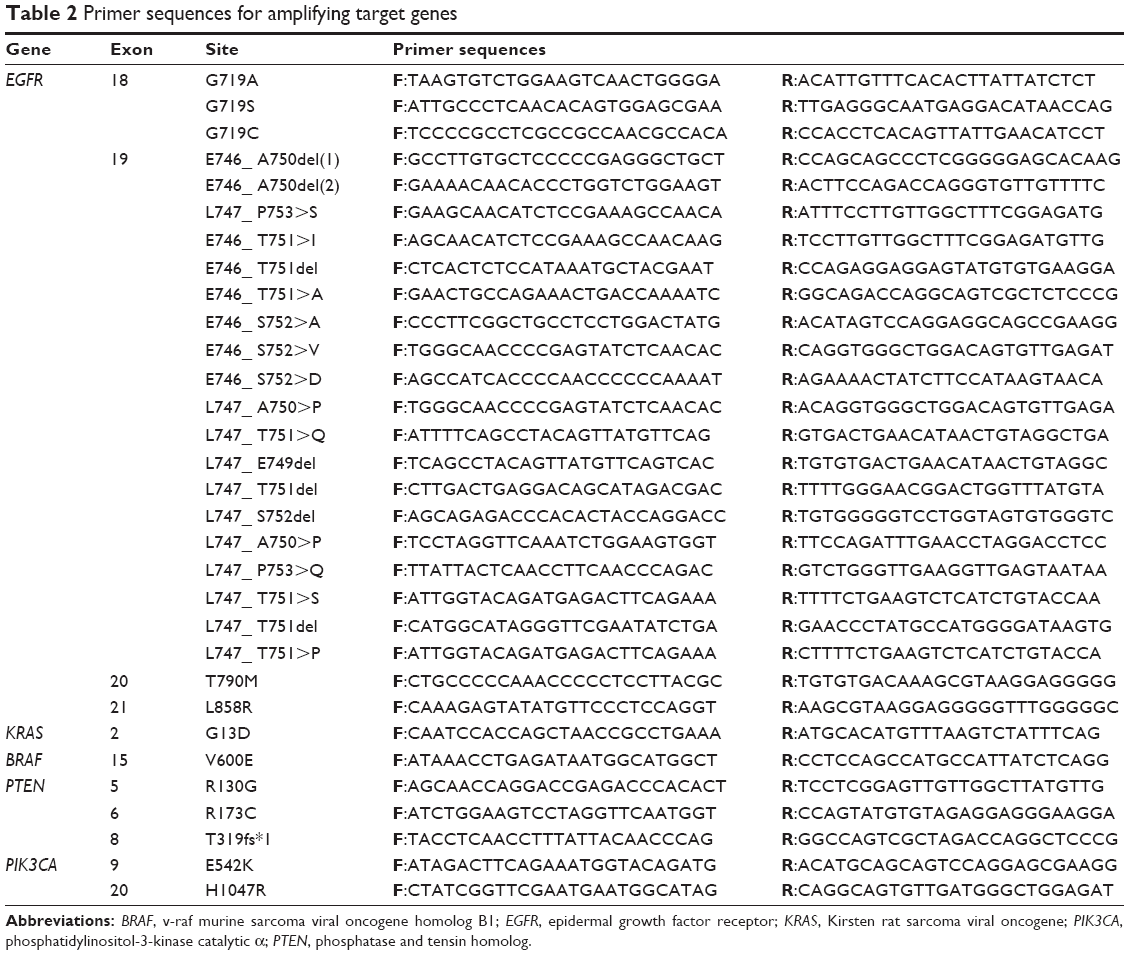 | Table 2 Primer sequences for amplifying target genes |
EVA-Green (Biotium, Fremont, CA, USA) was used as the intercalating dye. The reaction mixture consisted of 5 ng plasma DNA, 10× PCR buffer, 2.5 mM MgCl2, 0.5 μM of each primer, 200 μM dNTP, 1U of FastStart Taq polymerase (Roche), and PCR grade water in a volume of 20 μL.
PCR cycling and HRM analysis were performed on the LightCycler® 480 Real-Time PCR System (Roche Diagnostics). The amplification was carried out according to the following conditions: 1 cycle of 95°C for 5 min; 50 cycles of 95°C for 10 s, 60°C for 15 s, 72°C for 25 s. Before the HRM step, the products were heated to 95°C for 1 min and cooled to 40°C for 1 min. HRM was carried out from 65°C to 95°C, rising at 0.02°C/s with 25 acquisitions per degree.
Results
By HRM, blood samples from 99 SCLC patients were sequenced to detect the genetic mutation of target genes (EGFR, KRAS, BRAF, PIK3CA, and PTEN). Consequently, target-site mutation was detected in 15 patients. Among them, these mutations of 12 patients were mutually exclusive, and the remaining 3 patients carried multiple mutations. As shown in Table 3, the number of patients who carried EGFR/KRAS/BRAF/PIK3CA/PTEN mutation was 9/5/1/1/0, respectively. In detail, EGFR 18 (G719X) mutation in 5 (5.05%) patients, EGFR 19 (del) mutation in 2 (2.02%) patients, EGFR 20 (T790M) mutation in 3 (3.03%) patients, EGFR 21 (L858R) mutation in 2 (2.02%) patients, KRAS 2 (G13D) mutation in 5 (5.05%) patients, BRAF 15 (V600E) mutation in 1 (1.01%) patient (Figure 1), PIK3CA 9 (E542K) mutation in 1 (1.01%) patient (Figure 2), and no mutations of PTEN 5 (R130G), PTEN 6 (R173C), PTEN 8 (T319fs*1), and PIK3CA 20 (H1047R) were found. Three patients with multiple mutations, one patient harboring EGFR 18 (G719X) and EGFR 19 (del) mutations (Figure 3), one patient harboring EGFR 20 (T790M) and EGFR 21 (L858R) (Figure 4), and another patient harboring EGFR 18 (G719X), EGFR 20 (T790M), and KRAS 2 (G13D) mutations (Figure 5) were identified. The nine patients (one female and eight males) harboring EGFR mutations expressed a mean age of 59 years (range, 48–71 years). The stages were as follows: LD in four patients and ED in five patients. One patient was a nonsmoker, and eight were heavy smokers.
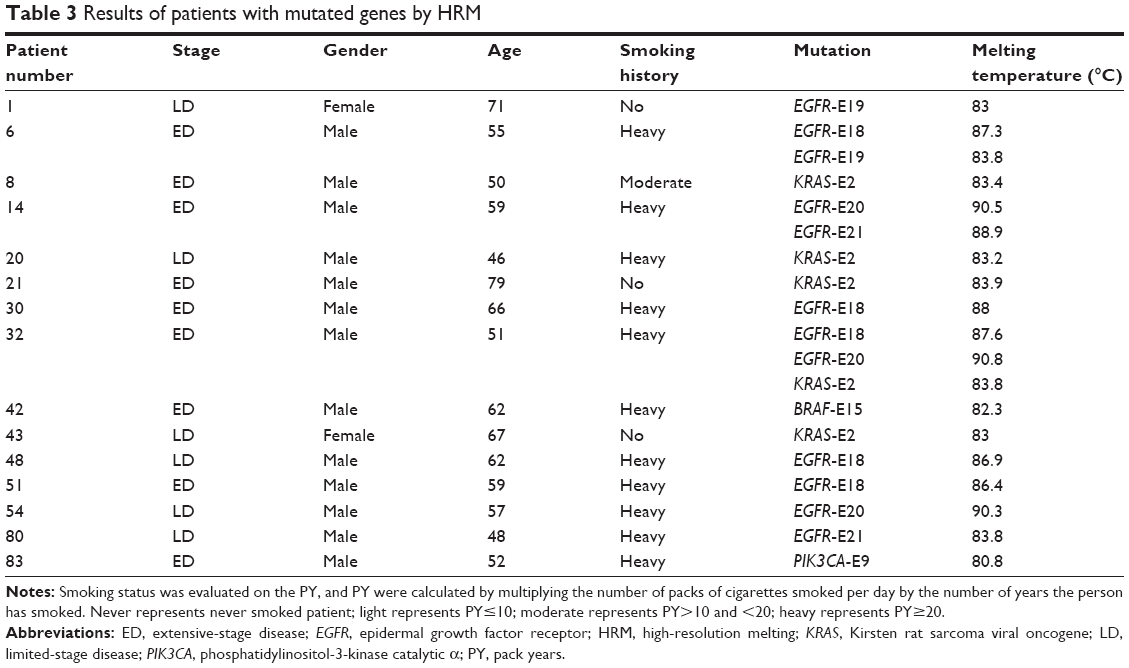 | Table 3 Results of patients with mutated genes by HRM |
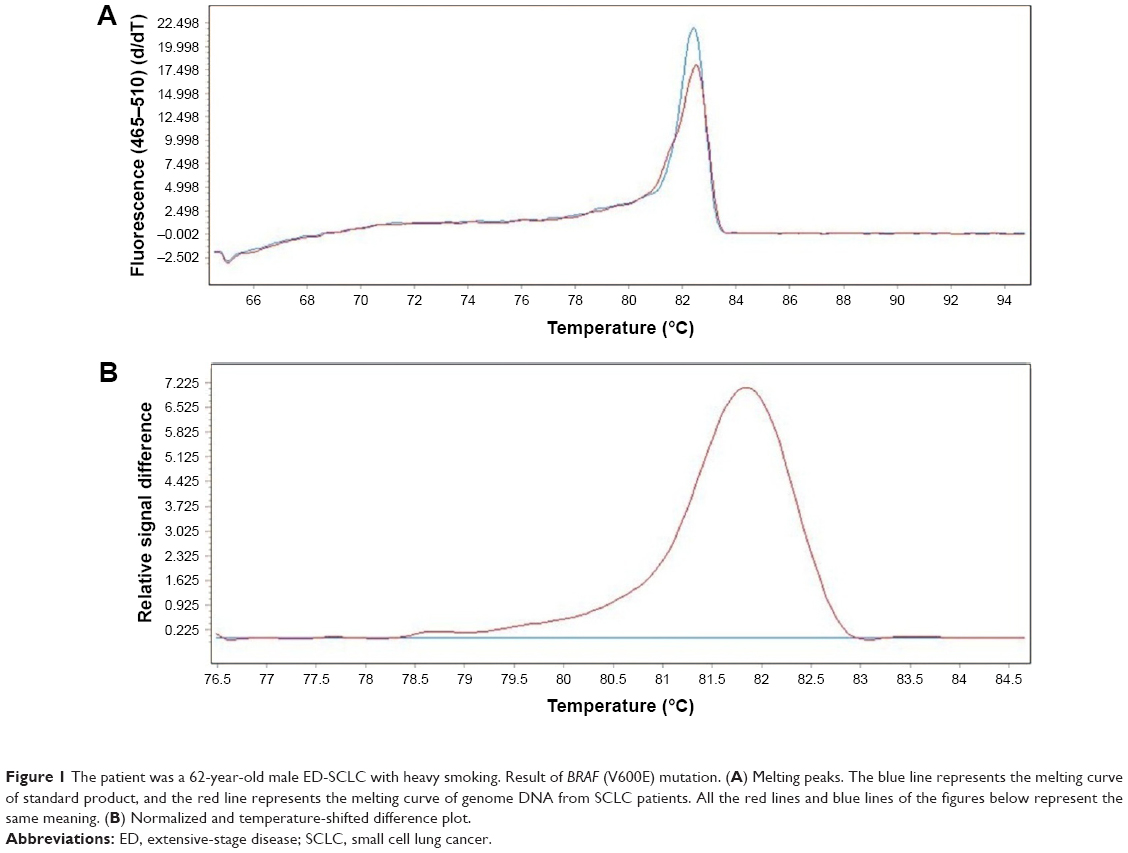 | Figure 1 The patient was a 62-year-old male ED-SCLC with heavy smoking. Result of BRAF (V600E) mutation. (A) Melting peaks. The blue line represents the melting curve of standard product, and the red line represents the melting curve of genome DNA from SCLC patients. All the red lines and blue lines of the figures below represent the same meaning. (B) Normalized and temperature-shifted difference plot. |
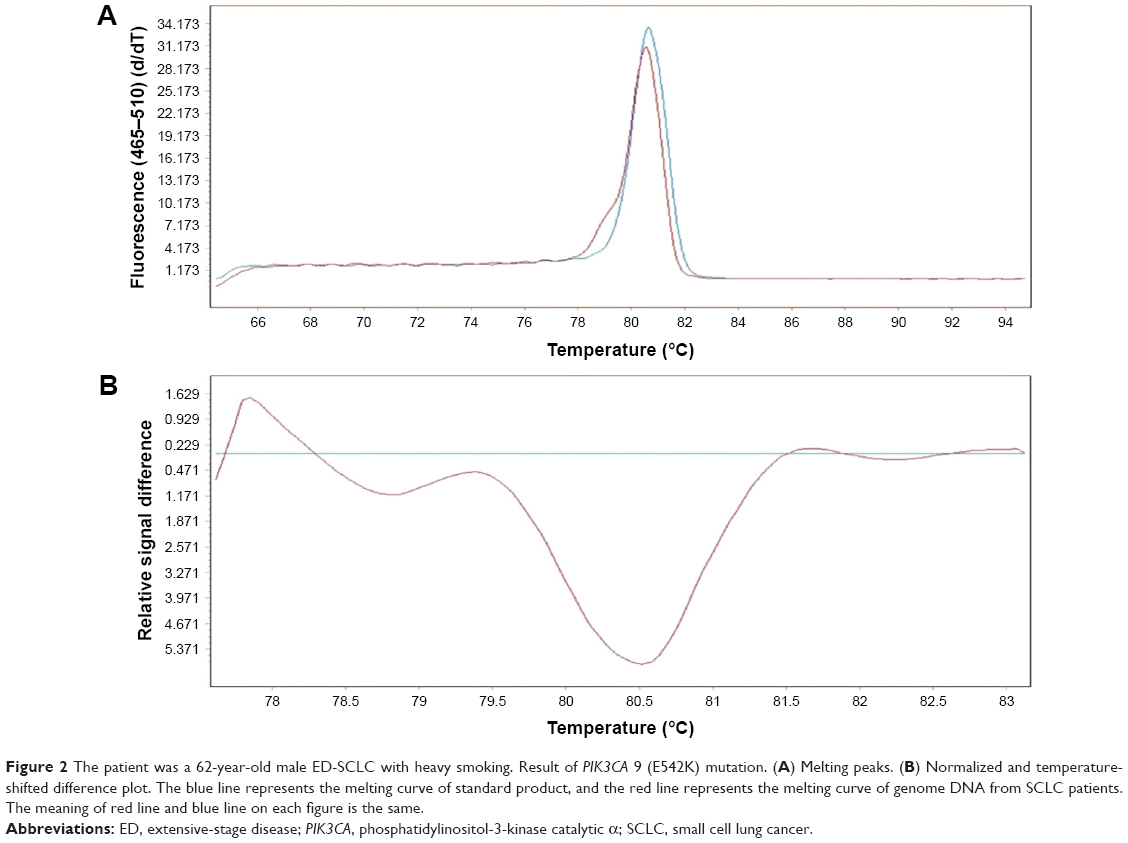 | Figure 2 The patient was a 62-year-old male ED-SCLC with heavy smoking. Result of PIK3CA 9 (E542K) mutation. (A) Melting peaks. (B) Normalized and temperature-shifted difference plot. The blue line represents the melting curve of standard product, and the red line represents the melting curve of genome DNA from SCLC patients. The meaning of red line and blue line on each figure is the same. |
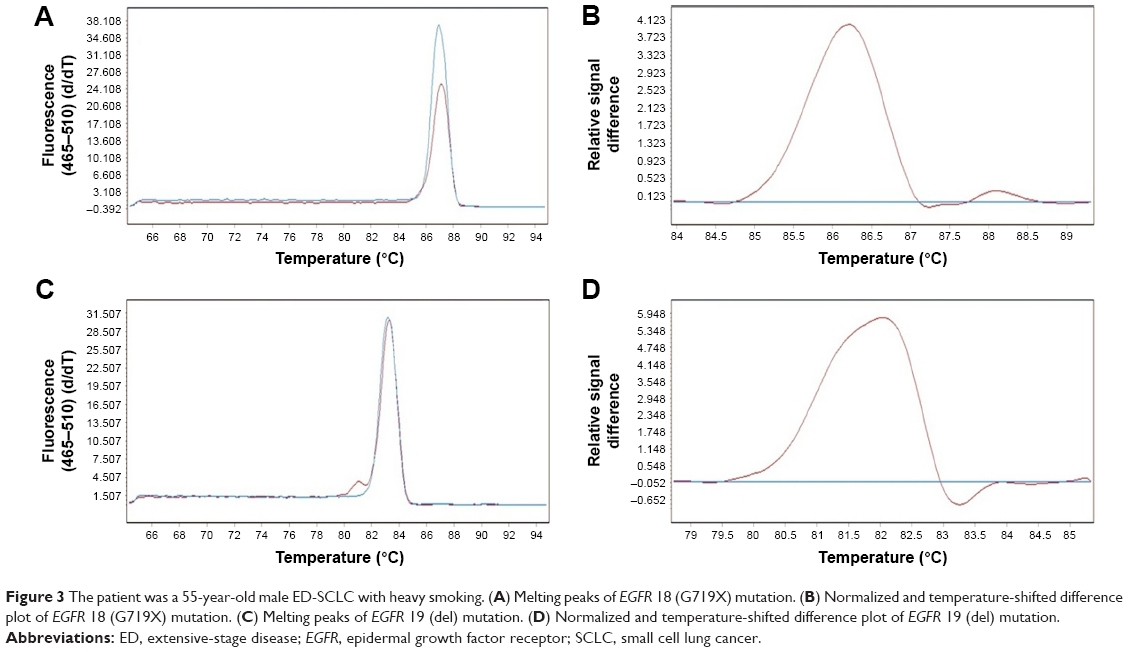 | Figure 3 The patient was a 55-year-old male ED-SCLC with heavy smoking. (A) Melting peaks of EGFR 18 (G719X) mutation. (B) Normalized and temperature-shifted difference plot of EGFR 18 (G719X) mutation. (C) Melting peaks of EGFR 19 (del) mutation. (D) Normalized and temperature-shifted difference plot of EGFR 19 (del) mutation. |
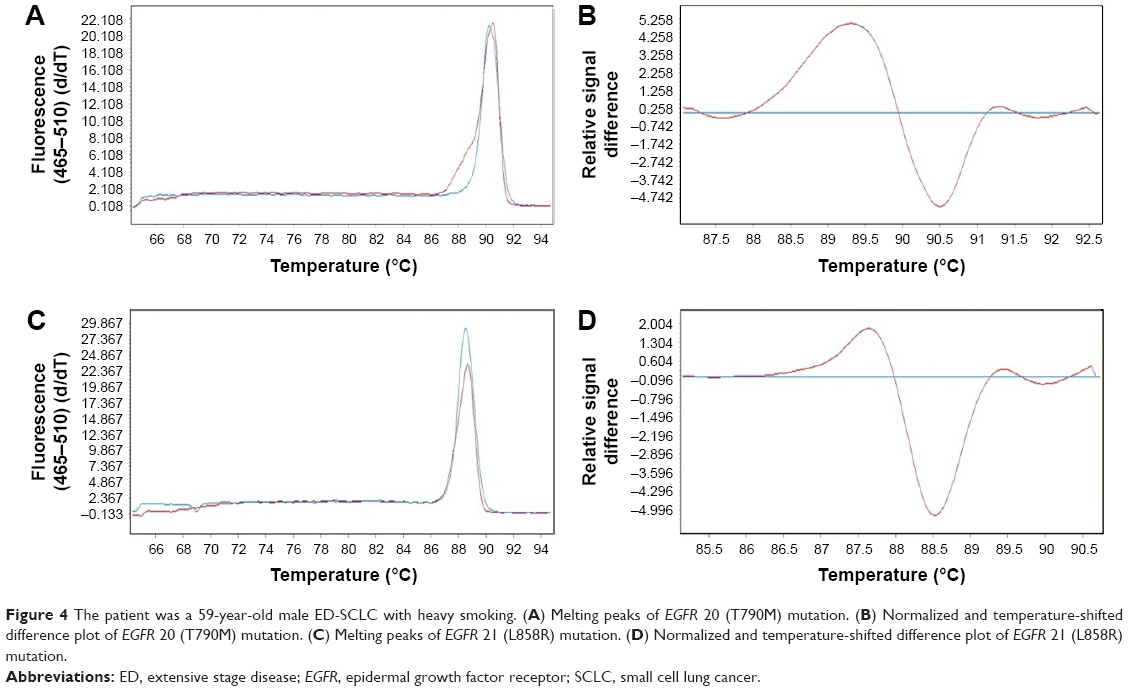 | Figure 4 The patient was a 59-year-old male ED-SCLC with heavy smoking. (A) Melting peaks of EGFR 20 (T790M) mutation. (B) Normalized and temperature-shifted difference plot of EGFR 20 (T790M) mutation. (C) Melting peaks of EGFR 21 (L858R) mutation. (D) Normalized and temperature-shifted difference plot of EGFR 21 (L858R) mutation. |
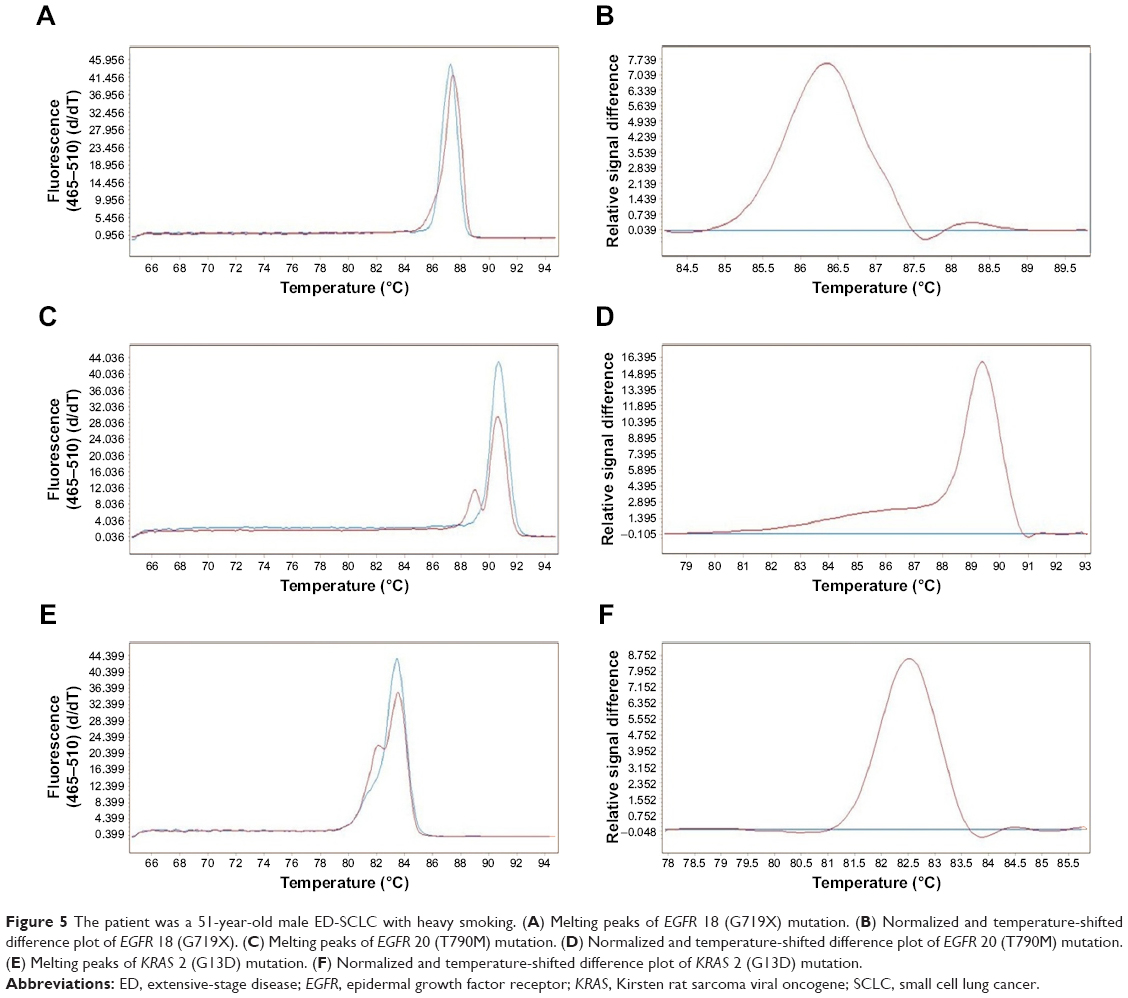 | Figure 5 The patient was a 51-year-old male ED-SCLC with heavy smoking. (A) Melting peaks of EGFR 18 (G719X) mutation. (B) Normalized and temperature-shifted difference plot of EGFR 18 (G719X). (C) Melting peaks of EGFR 20 (T790M) mutation. (D) Normalized and temperature-shifted difference plot of EGFR 20 (T790M) mutation. (E) Melting peaks of KRAS 2 (G13D) mutation. (F) Normalized and temperature-shifted difference plot of KRAS 2 (G13D) mutation. |
Discussion
In the present study, the percentage of EGFR mutations in SCLC plasma is higher than from the tumor tissue in previous reports.16–18,22 The EGFR mutation from tumor tissue can only reflect the mutation status of the tissue that is evaluated; heterogeneity occurs widely in different parts of the tissue in the same patient.23 The EGFR mutation in plasma may originate from all the tumor tissues of the whole body. The patients with EGFR-mutated SCLC tended to be females, nonsmokers, and in SCLC including “conventional SCLC and combined SCLC”. Combined SCLC is SCLC containing discrete areas of non-mall cell morphologic components.25–27 A study revealed 28% of the SCLC patients who underwent surgical resection exhibited combined SCLC,28 while other reports demonstrated that combined SCLC accounted for 1%–3.2% of all the SCLC cases who received no surgery.29,30 Surgery can be considered only in T1-2N0M0 SCLC patients; however, these cases have been reported to account for <5% of all the SCLC patients.18 None of our SCLC patients underwent surgery. The diagnosis of combined SCLC using biopsy or needle puncture is extremely arduous. Twenty to thirty percent of our SCLC patients may have combined SCLC, and we could not diagnose combined SCLC through small specimens obtained from biopsy or needle puncture. Heterogeneity can also explain the double mutation of EGFR in plasma of the same patient. SCLC developing in association with adenocarcinoma, either synchronously or metachronously, seemed to correlate with the EGFR mutation, irrespective of TKI usage.31 The EGFR mutation may easily occur in SCLC combined adenocarcinoma than in SCLC combined with other NSCLC complements.25 Because of the specific involvement of EGFR mutations in adenocarcinoma, it is suggested that the SCLCs may have developed from preexisting adenocarcinomas.17 As we all know, EGFR activating mutations, including exon 19 deletions or an exon 21 Leu858Arg mutation, present favorable outcome after treating with EGFR TKI.32,33 In SCLC, several studies have also performed a similar research. A 72-year-old woman with EGFR exon 19 mutation (del E746-A750) utilized gefitinib as the treatment method.34 After 3 weeks, CT was performed, which revealed marked regression of both the primary lung tumor and the metastatic liver tumor. The histological examination of this patient was confirmed as SCLC. Another clinical report also revealed a pronounced positive effect of gefitinib in a patient with metastatic SCLC.35 Second-generation inhibitors, including afatinib, dacomitinib, and neratinib, have been verified markedly with high efficacy in NSCLC patients with the G719X mutation.36,37 Based on our research, EGFR 18 (G719X) is the most common EGFR mutation of SCLC in the current report, which is different from lung adenocarcinoma with the main mutations EGFR 19 (del) and EGFR 21 (L858R).38,39 Thus, we speculated that G719X might be a promising mutation for treatment. Bordi et al reported that all the SCLC cases harbored wild-type BRAF, KRAS, platelet-derived growth factor receptor alpha, and c-KIT (data available for 82 patients) genes.24 Other studies reveal ~2%–5% KRAS mutations in patients with SCLC.40,41 Our study also confirmed that fewer mutations of KRAS and BRAF in SCLC patients might be correlated with the resistance to TKI in NSCLC in the background of these mutations.10,42–45 In our study, EGFR and KRAS mutations are detected in one SCLC patient. Le et al demonstrated the lack of response to EGFR TKIs in one EGFR-mutated de novo SCLC patient, which might be attributed to the KRAS or BRAF mutation; however, the underlying mechanism is yet to be elucidated.15 Selumetinib is a tight-binding, noncompetitive inhibitor of MEK 1 and 2 that acts downstream of KRAS and is administered orally. Recently, a randomized, Phase II trial involving selumetinib plus docetaxel improved the progression-free survival when compared with docetaxel alone in patients who were treated previously for advanced NSCLC harboring the KRAS mutant.46 Furthermore, the role of BRAF mutation in NSCLC and the optimal treatment are yet to be elucidated. The regression of intracranial disease by Robinson et al indicated that vemurafenib traversed the blood–brain barrier and efficaciously treated the brain metastasis in lung cancer patients with a V600E mutation in BRAF gene.47 Thus, selumetinib and vemurafenib in SCLC with KRAS or BRAF mutation can be explored prospectively.
The PI3K/AKT/mTOR pathway plays a unique role with respect to genomic alterations in SCLC.48 The inactivated PTEN advances the SCLC in a genetic mouse model, thereby suggesting that a subset of patients with SCLC can be treated by targeting the PTEN pathway.49 Li et al indicated that adenovirus-mediated PTEN together with cisplatin could be an efficient novel therapeutic modality for the treatment of patients with SCLC.50 Tricribine is a small molecule inhibitor of AKT signaling. It is localized downstream of PIK3CA and inhibited the growth and colony formation of “PIK3CA-addicted” cells significantly. Moreover, the SCLC cells harboring the mutated PIK3CA are more sensitive to tricribine than the wild-type cells. On the other hand, the cisplatin-resistant subclones of PIK3CA-mutant SCLC cells exhibited sensitivity to tricribine similar to those with PIK3CA. The anti-AKT molecular therapy was found to be efficient for a subgroup of SCLC with PIK3CA mutation.51 PF-4989216 is a potential cancer therapeutic candidate for the treatment of SCLC patients with PIK3CA mutation and without PTEN loss.52 Reverse transcription-polymerase chain reaction and direct sequencing technology were employed for the detection of PIK3CA mutation in 14 cases of patients with SCLC, assimilated retrospectively, who underwent surgical treatment at the Zhejiang Cancer Hospital from 2002 to 2010. The analysis did not reveal any mutations in exons 9 and 20 of the PIK3CA gene in the tumor tissue of patients with SCLC.53 In the current study, one patient presented the PIK3CA mutation. The percentage of PIK3CA mutations is similar to PTEN: ~5%.27,40,48 Sasaki et al and Schmid et al43,54 established the synergistic effects of the combination therapy of Erlotinib and RAD001 with respect to cell viability, proliferation, and autophagy.
Conclusion
Our study revealed the mutation of the targeted genes from SCLC. The mutations in KRAS, BRAF, and PIK3CA are rare in patients with SCLC, and the mutation in EGFR might differ from that in lung adenocarcinoma. The experimental results laid the foundation for better understanding of the mutation characteristics of SCLC and the following research on the application of targeted drugs.
Acknowledgments
This study was funded by Natural Science Foundation of Zhejiang Province of China (LY15H290001), Zhejiang province public welfare and technology application project of China (2016C33118), Zhejiang province medical science project of China (No 2015ZHA006), Zhejiang province traditional medical science project of China (No 2015ZA037), and the 1022 Talent Training Program of Zhejiang Cancer Hospital.
The abstract of this paper was presented at the 2014 ASCO Conference named “EGFR, KRAS, BRAF, PTEN, and PIK3CA mutation in plasma of small cell lung cancer patients” (e18552) as an e-poster with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539–4544. | ||
Sundstrom S, Bremnes RM, Kaasa S, et al; Norwegian Lung Cancer Study Group. Cisplatin and etoposide regimen is superior to cyclophosphamide, epirubicin and vincristine regimen in small-cell lung cancer: results from a randomized phase III trial with 5 years’ follow-up. J Clin Oncol. 2002;20:4665–4672. | ||
Pujol JL, Daurès JP, Rivière A, et al. Etoposide plus cisplatin with or without the combination of 4′-epidoxorubicin plus cyclophosphamide in treatment of extensive small-cell lung cancer: a French Federation of Cancer Institute multicenter phase III randomized study. J Natl Cancer Inst. 2001;93:300–308. | ||
Tiseo M, Boni L, Ambrosio F, et al. Italian, multicenter, Phase III, randomized study of cisplatin plus etoposide with or without Bevacizumab as first-line treatment in extensive-disease small-cell lung cancer: the GOIRC-AIFA FARM6PMFJM Trial. J Clin Oncol. 2017;35(12):1281–1287. | ||
Koinis F, Kotsakis A, Georgoulias V. Small cell lung cancer (SCLC): no treatment advances in recent years. Transl Lung Cancer Res. 2016;5:39–50. | ||
Lu HY, Wang XJ, Mao WM. Targeted therapies in small cell lung cancer (Review). OncolLett. 2013;5(1):3–11. | ||
Herbst RS. Review of epidermal growth factor receptor biology. Int J Radiat Oncol Biol Phys. 2004;59(2 Suppl):S21–S26. | ||
Hirsch FR, Scagliotti GV, Langer CJ, et al. Epidermal growth factor family of receptors in preneoplasia and lung cancer: perspectives for targeted therapies. Lung Cancer. 2003;41(Suppl 1):S29–S42. | ||
Kobayashi S, Boggon TJ, Dayaram T, Varella-Garcia M, Franklin WA. EGFR mutation and resistance of non-small-cell lung cancer to gefitinib. N Engl J Med. 2005;352:786–792. | ||
Eberhard DA, Johnson BE, Amler LC, et al. Mutations in the epidermal growth factor receptor and in KRAS are predictive and prognostic indicators in patients with non-small-cell lung cancer treated with chemotherapy alone and in combination with erlotinib. J Clin Oncol. 2005;23(25):5900–5909. | ||
Pratilas CA, Hanrahan AJ, Halilovic E, et al. Genetic predictors of MEK dependence in non-small cell lung cancer. Cancer Res. 2008;68(22):9375–9383. | ||
Song MS, Salmena L, Pandolfi PP. The functions and regulation of the PTEN tumour suppressor. Nat Rev Mol Cell. 2012;13(5):283–296. | ||
Shibata T, Kokubu A, Tsuta K, Hirohashi S. Oncogenic mutation of PIK3CA in small cell lung carcinoma: a potential therapeutic target pathway for chemotherapy-resistant lung cancer. Cancer Lett. 2009;283(2):203–211. | ||
Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med. 2011;3(75):75ra26. | ||
Le X, Desai NV, Majid A, et al. De novo pulmonary small cell carcinomas and large cell neuroendocrine carcinomas harboring EGFR mutations: lack of response to EGFR inhibitors. Lung Cancer. 2015;88(1):70–73. | ||
Shiao TH, Chang YL, Yu CJ, et al. Epidermal growth factor receptor mutations in small cell lung cancer: a brief report. J Thorac Oncol. 2011;6(1):195–198. | ||
Tatematsu A, Shimizu J, Murakami Y, et al. Epidermal growth factor receptor mutations in small cell lung cancer. Clin Cancer Res. 2008;14(19):6092–6096. | ||
Rostad H, Naalsund A, Jacobsen R, et al. Small cell lung cancer in Norway. Should more patients have offered surgical therapy? Eur J Cardiothorac Surg. 2004;26(4):782–786. | ||
Takano T, Ohe Y, Tsuta K, et al. Epidermal growth factor receptor mutation detection using high-resolution melting analysis predicts outcomes in patients with advanced non small cell lung cancer treated with gefitinib. Clin Cancer Res. 2007;13(18 Pt 1):5385–5390. | ||
Zhao J, Peng QX, Yang BH, Lu DR. [High-resolution melting analysis for the detection of EGFR mutations in circulating DNA of lung cancer patients]. Zhonghua Yi Xue Za Zhi. 2011;91(10):674–678. Chinese. | ||
Jing CW, Wang Z, Cao HX, Ma R, Wu JZ. High resolution melting analysis for epidermal growth factor receptor mutations in formalin-fixed paraffin-embedded tissue and plasma free DNA from non-small cell lung cancer patients. Asian Pac J Cancer Prev. 2014;14(11):6619–6623. | ||
Lu HY, Sun WY, Chen B, et al. Epidermal growth factor receptor mutations in small cell lung cancer patients who received surgical resection in China. Neoplasma. 2012;59(1):100–104. | ||
Zhang J, Fujimoto J, Zhang J, et al. Intratumor heterogeneity in localized lung adenocarcinomas delineated by multiregion sequencing. Science. 2014;346(6206):256–259. | ||
Bordi P, Tiseo M, Barbieri F, et al. Gene mutations in small-cell lung cancer (SCLC): results of a panel of 6 genes in a cohort of Italian patients. Lung Cancer. 2014;86(3):324–328. | ||
Lu HY, Mao WM, Cheng QY, et al. Mutation status of epidermal growth factor receptor and clinical features of patients with combined small cell lung cancer who received surgical treatment. Oncol Lett. 2012;3(6):1288–1292. | ||
Fukui T, Tsuta K, Furuta K, et al. Epidermal growth factor receptor mutation status and clinicopathological features of combined small cell carcinoma with adenocarcinoma of the lung. Cancer Sci. 2007;98(11):1714–1719. | ||
Sun JM, Choi YL, Ji JH, et al. Small-cell lung cancer detection in never-smokers: clinical characteristics and multigene mutation profiling using targeted next-generation sequencing. Ann Oncol. 2015;26(1):161–166. | ||
Nicholson SA, Beasley MB, Brambilla E, et al. Small cell lung carcinoma (SCLC): a clinicopathologic study of 100 cases with surgical specimens. Am J Surg Pathol. 2002;26(9):1184–1197. | ||
Mangum MD, Greco FA, Hainsworth JD, Hande KR, Johnson DH. Combined small-cell and non-small-cell lung cancer. J Clin Oncol. 1989;7(5):607–612. | ||
Fraire AE, Johnson EH, Yesner R, Zhang XB, Spjut HJ, Greenberg SD. Prognostic significance of histopathologic subtype and stage in small cell lung cancer. Hum Pathol. 1992;23(5):520–528. | ||
Norkowski E, Ghigna MR, Lacroix L, et al. Small-cell carcinoma in the setting of pulmonary adenocarcinoma: new insights in the era of molecular pathology. J Thorac Oncol. 2013;8(10):1265–1271. | ||
Mok TS, Wu Y-L, Thongprasert S, et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. | ||
Wu YL, Zhou C, Hu CP, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15:213–222. | ||
Okamoto I, Araki J, Suto R, et al. EGFR mutation in gefitinib-responsive small-cell lung cancer. Ann Oncol. 2006;17(6):1028–1029. | ||
Araki J, Okamoto I, Suto R, et al. Efficacy of the tyrosine kinase inhibitor gefitinib in a patient with metastatic small cell lung cancer. Lung Cancer. 2005;48(1):141–144. | ||
Sequist LV, Besse B, Lynch TJ, et al. Neratinib, an irreversible pan-ErbB receptor tyrosine kinase inhibitor: results of a phase II trial in patients with advanced non-small-cell lung cancer. J Clin Oncol. 2010;28:3076–3083. | ||
Yang JC, Sequist LV, Geater SL, et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: a combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015;16:830–838. | ||
Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735–742. | ||
Mitsudomi T, Morita S, Yatabe Y, et al; West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–128. | ||
Ross JS, Wang K, Elkadi OR, et al. Next-generation sequencing reveals frequent consistent genomic alterations in small cell undifferentiated lung cancer. J ClinPathol. 2014;67(9):772–776. | ||
Wakuda K, Kenmotsu H, Serizawa M, et al. Molecular profiling of small cell lung cancer in a Japanese cohort. Lung Cancer. 2014;84(2):139–144. | ||
Kobayashi M, Sonobe M, Takahashi T, et al. Clinical significance of BRAF gene mutations in patients with non-small cell lung cancer. Anticancer Res. 2011;31(12):4619–4623. | ||
Sasaki H, Kawano O, Endo K, et al. Uncommon V599E BRAF mutations in Japanese patients with lung cancer. J Surg Res. 2006;133(2):203–206. | ||
Marchetti A, Felicioni L, Malatesta S, et al. Clinical features and outcome of patients with non-small-cell lung cancer harboring BRAF mutations. J Clin Oncol. 2011;29(26):3574–3579. | ||
Paik PK, Arcila ME, Fara M, et al. Clinical characteristics of patients with lung adenocarcinomas harboring BRAF mutations. J Clin Oncol. 2011;29(15):2046–2051. | ||
Paolo M, Assunta S, Antonio R, et al. Selumetinib in advanced non small cell lung cancer (NSCLC) harbouring KRAS mutation: endless clinical challenge to KRAS-mutant NSCLC. Rev Recent Clin Trials. 2013;8(2):93–100. | ||
Robinson SD, O’Shaughnessy JA, Cowey CL, Konduri K. BRAF V600E-mutated lung adenocarcinoma with metastases to the brain responding to treatment with vemurafenib. Lung Cancer. 2014;85(2):326–330. | ||
Umemura S, Mimaki S, Makinoshima H, et al. Therapeutic priority of the PI3K/AKT/mTOR pathway in small cell lung cancers as revealed by a comprehensive genomic analysis. J Thorac Oncol. 2014;9(9):1324–1331. | ||
Cui M, Augert A, Rongione M, et al. PTEN is a potent suppressor of small cell lung cancer. Mol Cancer Res. 2014;12(5):654–659. | ||
Li D, Zhang, Y, Xie Y, Xiang J, Zhu Y, Yang J. Enhanced tumor suppression by adenoviral PTEN gene therapy combined with cisplatin chemotherapy in small-cell lung cancer. Cancer Gene Ther. 2013;20(4):251–259. | ||
Shibata T, Kokubu A, Tsuta K, Hirohashi S. Oncogenic mutation of PIK3CA in small cell lung carcinoma: a potential therapeutic target pathway for chemotherapy-resistant lung cancer. Cancer Lett. 2009;283(2):203–211. | ||
Walls M, Baxi SM, Mehta PP, et al. Targeting small cell lung cancer harboring PIK3CA mutation with a selective oral PI3K inhibitor PF-4989216. Clin Cancer Res. 2014;20(3):631–643. | ||
Han N, Cheng QY, Chen B, et al. PIK3CA mutations in resected small cell lung cancer. Adv Clin Exp Med. 2016;25(3):397–402. | ||
Schmid K, Bago-Horvath Z, Berger W, et al. Dual inhibition of EGFR and mTOR pathways in small cell lung cancer. Br J Cancer. 2010;103(5):622–628. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.