")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Efficacy of Vitamin C Supplementation on Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
Authors Lei T, Lu T, Yu H, Su X, Zhang C, Zhu L, Yang K, Liu J
Received 7 April 2022
Accepted for publication 17 August 2022
Published 10 September 2022 Volume 2022:17 Pages 2201—2216
DOI https://doi.org/10.2147/COPD.S368645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Ting Lei,1,2,* Tingting Lu,3,4,* Haichuan Yu,1,2,* Xiaojie Su,1,2 Chuchu Zhang,1,2 Lei Zhu,1,2 Kehu Yang,4,5 Jian Liu1,2
1Department of Clinical Medicine, The First Clinical Medical College of Lanzhou University, Lanzhou, 730000, People’s Republic of China; 2Department of Critical Care Medicine, the First Hospital of Lanzhou University, Lanzhou, 730000, People’s Republic of China; 3Institute of Clinical Research and Evidence Based Medicine, Gansu Provincial Hospital, Lanzhou, 730000, People’s Republic of China; 4Evidence-Based Medicine Center, School of Basic Medical Sciences, Lanzhou University, Lanzhou, 730000, People’s Republic of China; 5Key Laboratory of Evidence-Based Medicine and Knowledge Translation of Gansu Province, Lanzhou, 730000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Liu, No. 1, Donggang West Road, Chengguan District, Lanzhou, Gansu Province, Tel +86 136 0935 4197, Email [email protected]; Kehu Yang, Evidence-Based Medicine Center, Lanzhou University, 199 West Donggang R.D, Lanzhou, 730000, People’s Republic of China, Email [email protected]
Background: In recent years, the pleiotropic roles of antioxidants have drawn extensive attention in various diseases. Vitamin C is a well-known antioxidant, and it has been used to treat patients with chronic obstructive pulmonary disease (COPD). This systematic review and meta-analysis aim to demonstrate the impact of vitamin C supplementation in patients with COPD.
Methods: We searched PubMed, Embase, Cochrane Library, Web of Science, Chinese National Knowledge Infrastructure (CNKI), SinoMed, Wanfang, and China Science and Technology Journal Database (cqvip.com) for eligible randomized controlled trials (RCTs) from their respective inception to May 18th, 2021, by using the searching terms of COPD, vitamin C, and RCTs. A meta-analysis was performed to evaluate the effects of vitamin C on lung function, antioxidant levels, and nutritional conditions in COPD patients by using Review Manager (Version 5.4).
Results: Ten RCTs including 487 participants were eligible for our study. Meta-analysis results showed that vitamin C supplementation (≥ 400 mg/day) can significantly improve the forced expiratory volume in one second as a percentage (FEV1%) in COPD (SMD:1.08, 95% CI:0.03, 2.12, P=0.04). Moreover, vitamin C supplementation significantly improved the ratio of forced expiratory volume in 1 second and forced vital capacity (FEV1/FVC) (WMD:0.66, 95% CI: 0.26, 1.06, P=0.001), vitamin C level in serum (SMD:0.63, 95% CI: 0.02, 1.24, P=0.04) and glutathione (GSH) level in serum (SMD:2.47, 95% CI: 1.06, 3.89, P=0.0006). While no statistically significant difference was observed in body mass index (BMI), fat-free mass index (FFMI), vitamin E level and superoxide dismutase (SOD) level in serum.
Conclusion: Vitamin C supplementation could increase the levels of antioxidation in serum (vitamin C and GSH) and improve lung function (FEV1% and FEV1/FVC), especially in patients treated with vitamin C supplementation greater than 400 mg/day. However, further prospective studies are needed to explore the role of vitamin C in improving nutritional status.
Keywords: vitamin C, COPD, RCTs, lung function, meta-analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is now the third leading cause of death worldwide.1 The increasing social and economic burdens associated with it make its comprehensive control a major public health goal.2,3 COPD is characterized by airflow limitation and persistent respiratory symptoms. These symptoms are the consequences of airway and/or alveolar abnormalities, which are usually caused by smoking gases or significant exposure to noxious particles.1 Oxidative stress is defined as the disturbance of the oxidant/antioxidant balance, and it has been suggested to play a critical role in the pathogenesis of COPD.4–6 Antioxidants are the first line of defense against oxidants by preventing the lung from the delirious consequences resulting from various oxidants and/or reactive oxygen.7 Antibiotics, systemic corticosteroids and short-acting bronchodilators are the three commonly used treatments to manage exacerbations of COPD, but no evidence supports the notion that these medications work against oxidative stress. Meanwhile, most COPD patients respond poorly to cortices due to the steroid refractoriness in their body.8
Vitamin C is a widely consumed natural supplement and is well known for its antioxidant properties.9 It exerts its antioxidant function by keeping both transient oxidants, such as O2•− and nitric oxide, and long-lived oxidants, such as semiquinone radicals, in their corresponding reduced state.7,10,11 Our objective is to evaluate the clinical therapeutic effect of vitamin C supplementation in patients with COPD.
The study conducted by Kanani et al identified a positive correlation between vitamin C intake and adult lung function.12–14 However, a negative correlation between supplemented vitamin C and the antioxidation level of vitamin C and SOD in serum was reported by Liu et al13 while the study of Gouzi et al demonstrated a positively correlated between the two parameters.15 Furthermore, although lots of studies have shown that COPD can cause malnutrition,16,17 no significant change in body mass (BMI) or fat-free mass index (FFMI) after vitamin C supplementation has been found. Therefore, the relationship between vitamin C supplementation and antioxidative stress in COPD patients is conclusive. Thus, we conducted this systematic review and meta-analyses to separately evaluate the efficacy of vitamin C supplementation in improving lung function, antioxidation level in serum and nutrition level in patients with COPD.
Methods
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. The protocol for this study has been pre-registered to the PROSPERO database (registration number: CRD42021259220).
Search Strategy
Two investigators independently searched PubMed, EMBASE, Cochrane Library, Web of Science, Chinese National Knowledge Infrastructure (CNKI), SinoMed, Wanfang, and China Science and Technology Journal Database for publications related to vitamin C and COPD from their corresponding inception until May 18th, 2021 without language restrictions. The search terms were “vitamin C”, or “ascorbic acid”, and “COPD”. Qualified articles must be studies in human. Moreover, we manually checked the reference lists of the retrieved articles and reviews for potentially eligible studies. Detailed search strategies are reported in Appendix 1.
Inclusion Criteria and Exclusion Criteria
Two investigators (LT and YHC) determined the eligibility of potential studies, and any disagreement was resolved by discussion with a third investigator.18–20 The inclusion criteria were:(1) patients in the eligible studies were diagnosed with COPD and were 18 years old or older; (2) the studies compared vitamin C supplementation with a placebo;(3) randomized controlled trials (RCTs) that provided outcomes of lung function, nutrition or serum antioxidant data. Exclusion criteria were: (1) patients in the studies had other accompanying diseases such as diabetes, kidney disease, lung cancer and other complications in addition to COPD. (2) the studies were conducted in cell assays or animal experiments; (3) reviews, case reports, conference abstracts, letters, or editorials; (4) duplicated publications or publications with incomplete data.
Data Extraction and Quality Assessment
Two authors (LT and YHC) independently extracted the following information: from each eligible study: first author, publication year, country of origin, study design, participant characteristics, vitamin C intake and trial duration. According to the Global GOLD guidelines,1 the primary outcome was lung function, and the lung function index included were FEV1%(forced expiratory volume in one second as a percentage) and FEV1/FVC (the ratio of forced expiratory volume in 1 second and forced vital capacity). The secondary outcomes analyzed in the present study included the concentrations of serum vitamin C, vitamin E, GSH (Glutathione), and SOD (Superoxide dismutase), the body mass index (BMI), and Fat-Free Mass Index (FFMI).
Two investigators assessed the risk of bias using the Cochrane risk of bias tool for randomized controlled trials,21 which included random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other potential risk of bias. Each domain was graded as low, unclear or high in terms of risk of bias. GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) was used to assess the certainty of evidence in the meta-analysis.
Statistical Analysis
For continuous variables, the random effect model was used to calculate the standardized mean difference (SMD), weighted mean difference (WMD) and 95% CI confidence interval (CI). Statistical heterogeneity was assessed by using the I2 test and Cochran Q test, and values of over 50% indicated substantial heterogeneity. Direct comparisons were performed using the Review Manager (version 5.4). P<0.05 for the overall effect was considered statistically significant. Subgroup analysis of the FEV1% was performed based on the dosage (<400 mg/d or ≥400 mg/d= of vitamin C supplementation). Subgroup analysis of GSH concentration was performed based on the different duration of vitamin C supplementation (< 3 months, 3–6 months, >6 months). Sensitivity analysis was performed by excluding low-quality studies to explore potential sources of heterogeneity. As for each assessed outcome there were less than ten articles; we could not assess publication bias by funnel plots.
Results
Study Screening and Characterization
Literature search following the search strategy yielded 1269 studies, including 190 duplicated. Title and abstract reviewing led to the exclusion of 1056 studies and a total of 23 articles for full-text review. Finally, ten articles were eligible for the present study.6,13–15,22–27 The PRISMA flow diagram is shown in Figure 1.
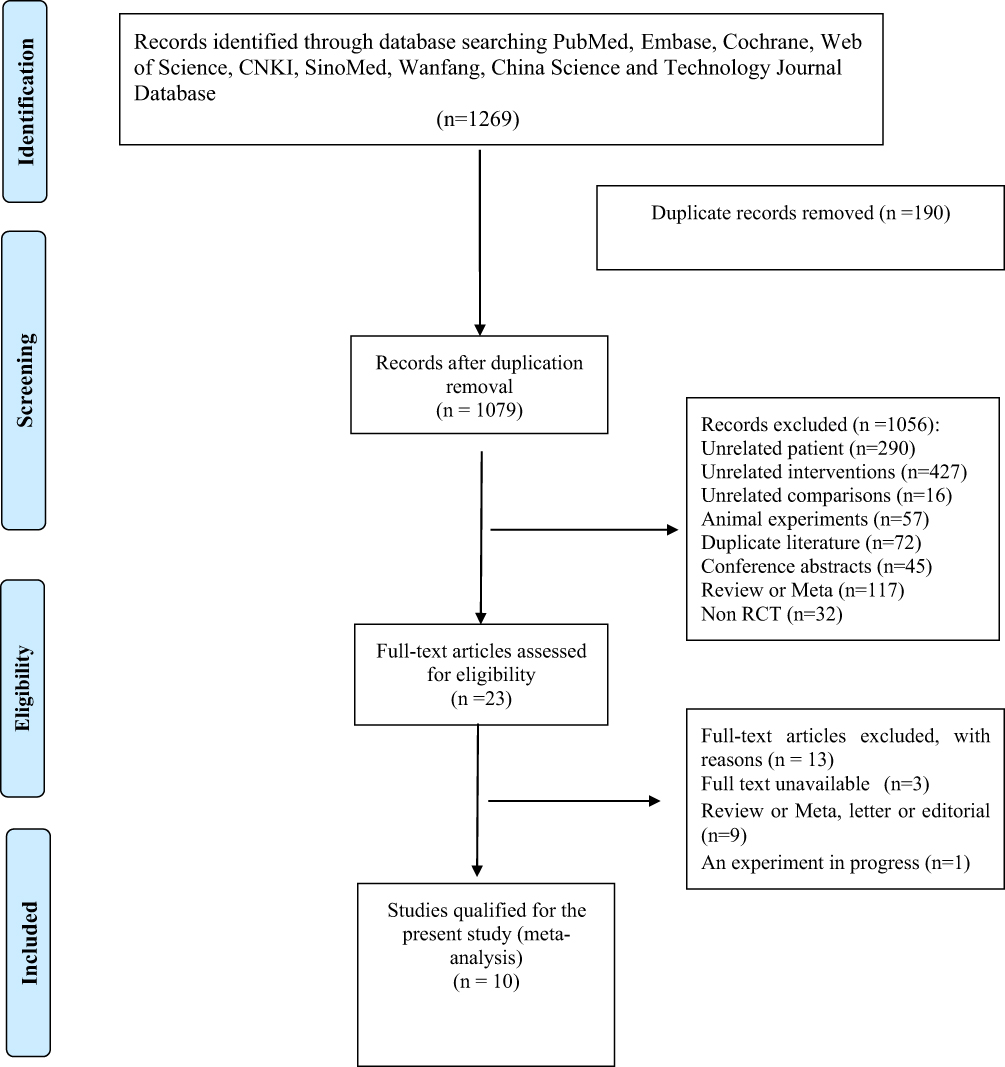 |
Figure 1 PRISMA 2009 Flow Diagram. Notes: PRISMA figure adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. 72. |
All studies were RCTs and described an adequate random sequence generation process. Seven studies6,13,14,22,24–26 described the methods used for allocation concealment. A total number of 487 patients were included in the present meta-analysis, including 248 patients who received vitamin C treatment and 239 patients who were given a placebo. Four studies13,14,23,26 reports included the male of patients, and another four studies6,15,22,24 included male-female ratio. But two studies25,27 did not report the gender of patients. In two studies, patients were treated with a daily supplemented vitamin C of less than 400 mg/day,6,15 while in the other studies, patients took vitamin C at 400 mg/day or more.13,14,22–27 Seven studies reported the lung function as the primary outcome,6,13,14,22,24–26 eight studies reported the levels of serum antioxidation,6,13–15,22–24,27 and three studies reported the nutrition leves15,23,27 as the secondary outcomes. The characteristics of the included RCTs are shown in Table 1.
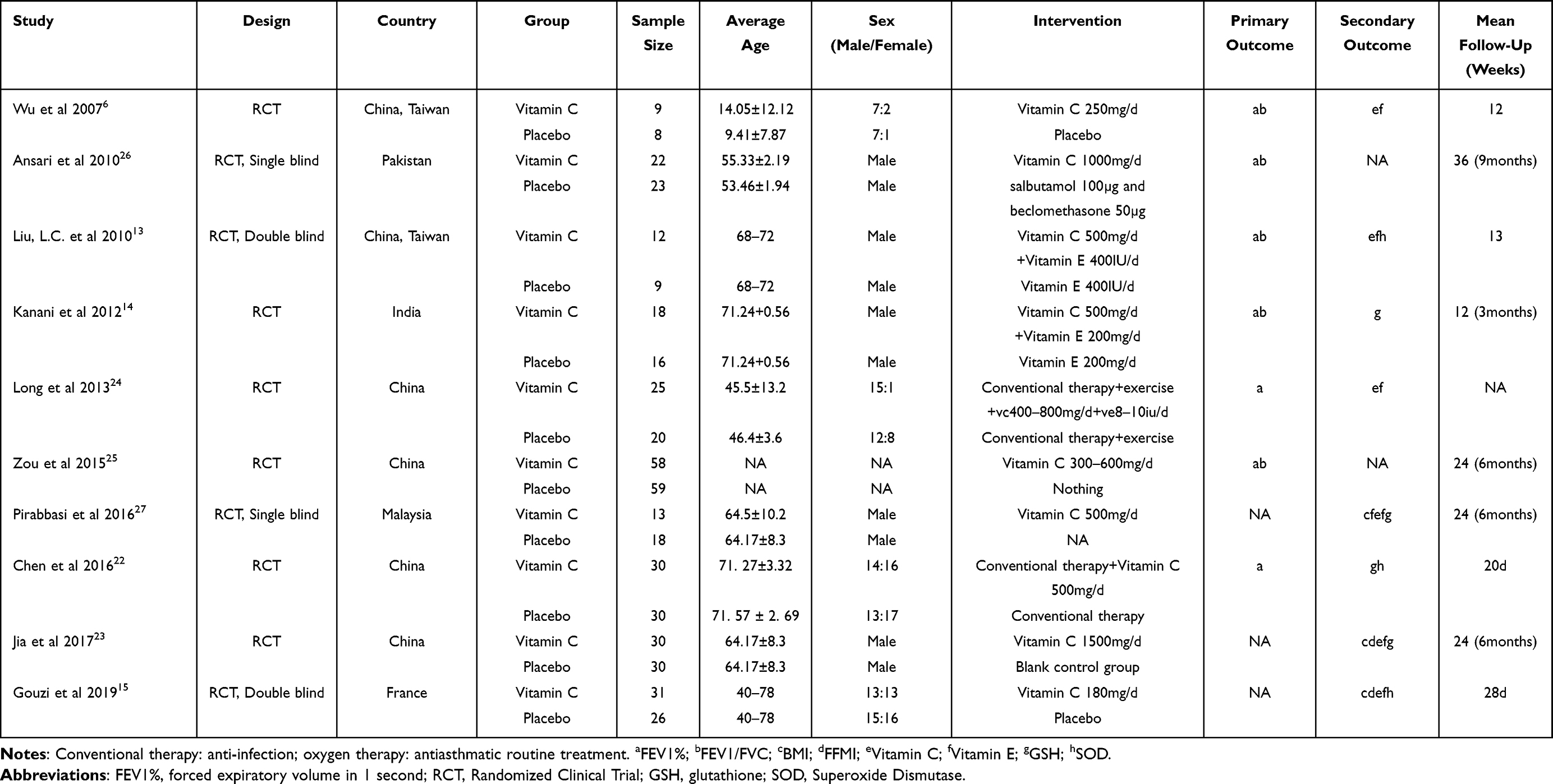 |
Table 1 Characteristics of Included Studies |
Risk of Bias Assessments
Except for the study conducted by Zou et al,25 the risk of bias in allocation concealment for the other studies was low. For the domain of blinding, the risk of bias was low in four studies (40%),13,15,26,27 and it was unclear in the rest of the studies. The risk of bias for all included RCTs (100%) was low regarding the incomplete outcome data and other bias. With respect to the selective reporting outcomes, the risk of bias was unclear for five studies (50%),13,22–25 and it was low for the rest of the studies. The quality assessments based on the risk of bias are shown in Figure 2, and the quality of evidence for the included studies, which were based on the GRADE was presented in Table 2.
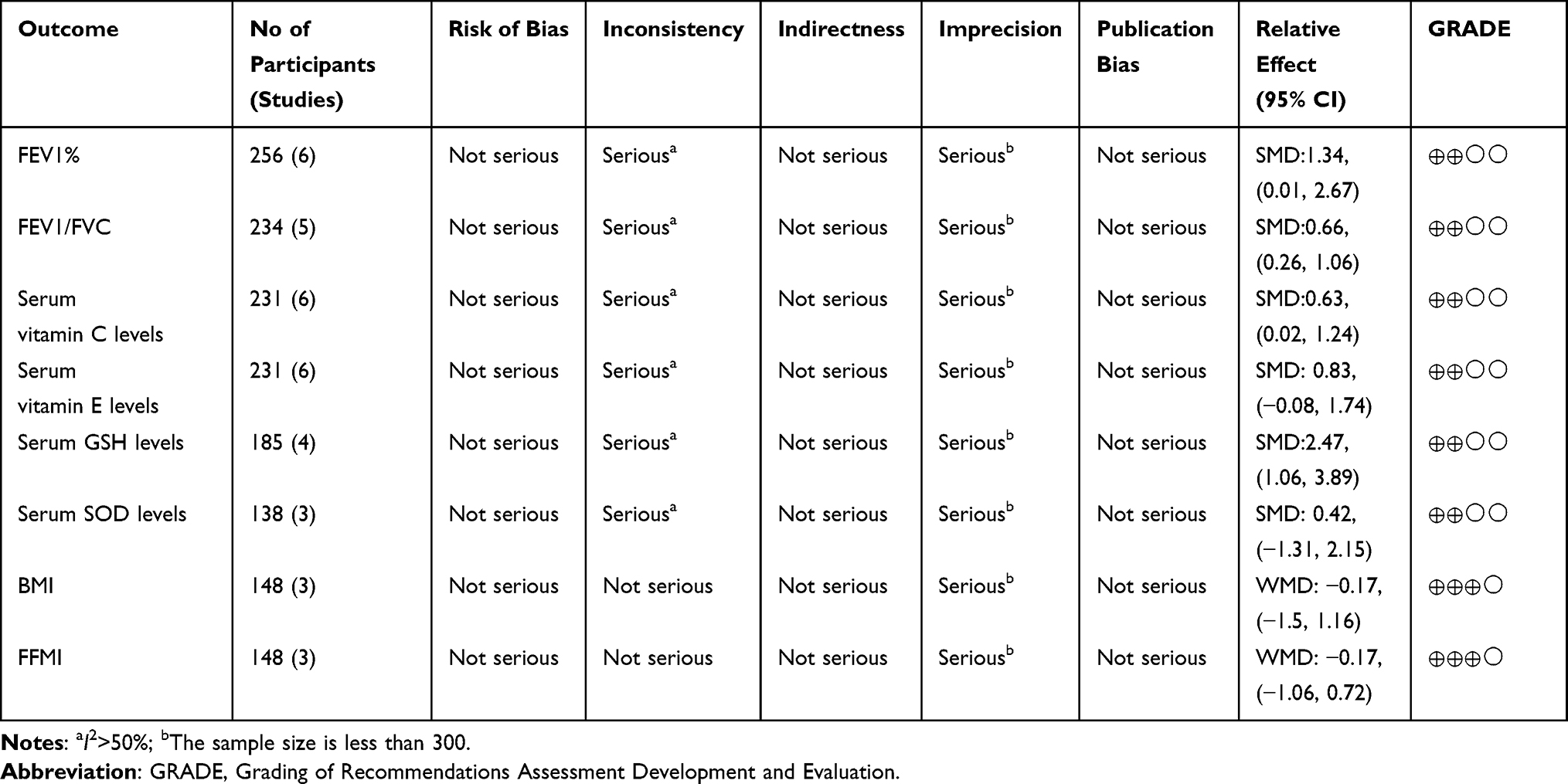 |
Table 2 GRADE Evaluation Results |
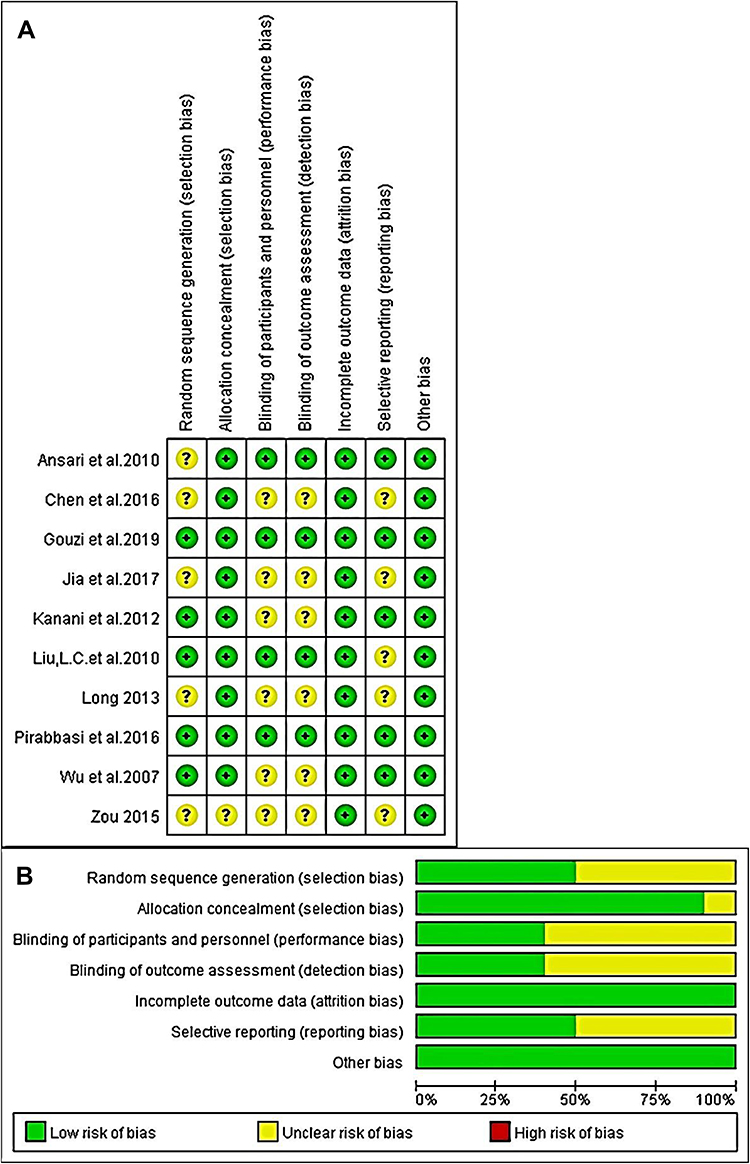 |
Figure 2 (A) Summary of risk of bias for each included study. (B) bar graph of the risk of bias showing the percentage of risk level for each characterized risk. Each color represents a different level of bias: red for high risk, green for low risk, and yellow for unclear risk of bias. |
Meta-Analysis
Lung Function Levels in COPD Patients
It has been pointed out in The Global Gold guide (2021) that the goals of COPD assessment are to determine the level of airflow limitation.1 Spirometry is required to make the diagnosis. FEV1%, which means the forced expiratory volume in the first second expressed as a percentage of the forced vital capacity (FVC), and the ratio of FEV1% and FVC (FEV1/FVC) can be used to diagnose the presence of persistent airflow limitation.1,6 These two diagnostic factors were affected by the supplementation of vitamin C in COPD patients. Among the ten eligible studies,6,13–15,22–27 seven of them reported lung function as an outcome by measuring the FEV1% or FEV1/FVC.6,13,14,22,24–26
Fev1%
FEV1% was used to evaluate lung function. The study conducted by Ansari et al,26 was excluded for lung function analysis since the original raw data could not be obtained. Since the dosage of vitamin C varies dramatically, we divided the pooled data into two subgroups by the amount of supplemented vitamin C: the subgroup with a daily vitamin C supplementation of less than 400 mg (Vitamin C<400 mg) and the subgroup with a daily vitamin C supplementation greater than 400 mg (Vitamin C ≥400 mg). The results showed that no statistical difference was found between the vitamin C group and the placebo group in the vitamin C<400 mg subgroup (SMD: −0.05, 95% CI: −1.00, 0.91, P=0.92). While in the vitamin C≥ 400 mg subgroup, an improved FEV1% was found in the vitamin C treatment group compared to that of the placebo group. The difference was statistically significant (SMD: 1.08, 95% CI: 0.03, 2.12, P=0.04). The result is shown in Figure 3.
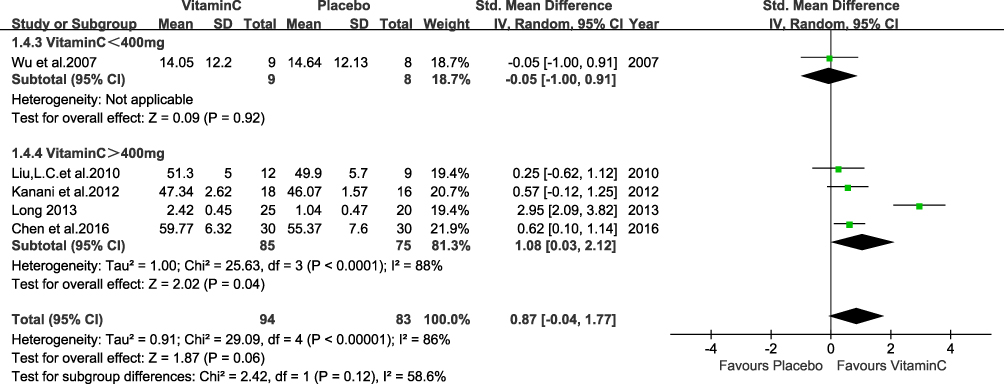 |
Figure 3 FEV1% in lung function. |
The sensitivity analysis result showed that the study conducted by Long et al24 significantly influenced the pooled results (Figure 4). If this study was excluded from our analysis, the I2 dropped from 86% to 0%. However, we did not exclude this study from our analysis. The reason was as follows: although respiratory rehabilitation training was used to treat COPD in Long et al study as the placebo treatment, which was different from the placebo treatments used in other analyzed studies,24 respiratory rehabilitation training alone would not have a significant impact on the lung function in COPD patients in clinical practice.15 Therefore, we concluded that the breathing exercise might not be a main source of heterogeneity.
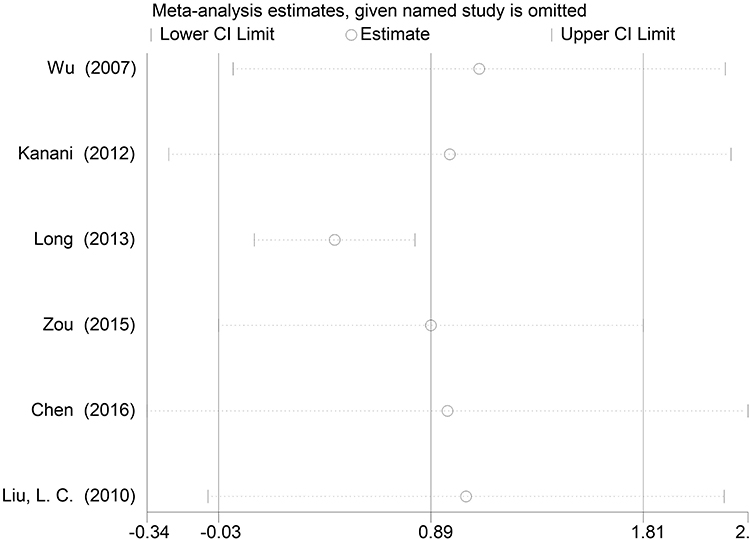 |
Figure 4 Sensitivity Analysis FEV1%. |
Fev1/Fvc
FEV1/FVC ratio was measured in five studies (n=234 patients)6,13,14,25,26 (SMD:0.66, 95% CI: 0.26,1.06, P=0.001; Figure 5), with a significant heterogeneity among these studies (I2=98%, P<0.00001). Sensitivity analyses showed that no individual study significantly influenced the results from the pooled data.
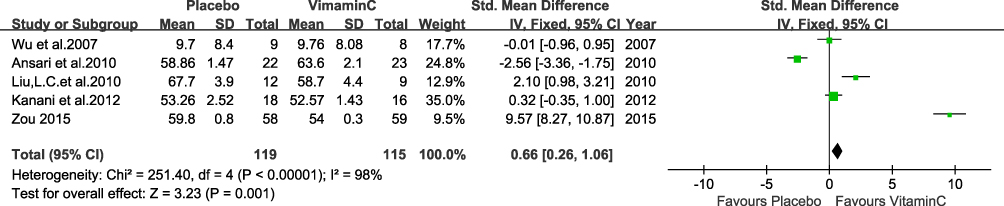 |
Figure 5 FEV1/FVC in lung function. |
Antioxidation Levels in Serum in COPD Patients
Different antioxidants were measured in different studies. Six studies including 231 patients, measured the levels of vitamin C and vitamin E in serum,6,13,15,23,24,27 and four studies, including 185 patients14,22,23,27 measured the level of GSH. Vitamin C, E and GSH are all non-enzymatic antioxidants in the lung. Three studies including 138 patients, measured the level of SOD, which belongs to the family of enzymatic antioxidants in lung.13,15,22
Vitamin C Level in Serum
Six studies reported the levels of vitamin C and vitamin E in serum in 120 COPD patients in the vitamin C group and in 111 patients in the placebo group.6,13,15,23,24,27
The result from the pooled data from the six studies showed that serum vitamin C level was higher in the vitamin C group than that of the placebo group (SMD:0.63, 95% CI: 0.02, 1.24, P=0.04; Figure 6), with significant heterogeneity among these studies (I2=78%, P=0.0004).
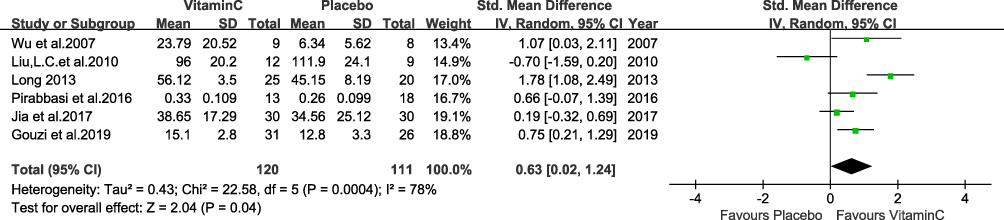 |
Figure 6 Vitamin C level in serum. |
Serum Vitamin E Level
A random effect model was used to analyze the data on serum vitamin E levels, and the result demonstrated that the serum vitamin E level was higher in the vitamin C supplementation group than that in the placebo group (SMD:0.83, 95% CI: −0.08, 1.74, P=0.07; Figure 7), with significant heterogeneity among these studies (I2=90%, P<0.00001). Sensitivity analyses showed that no individual study significantly influenced the results from the pooled data.
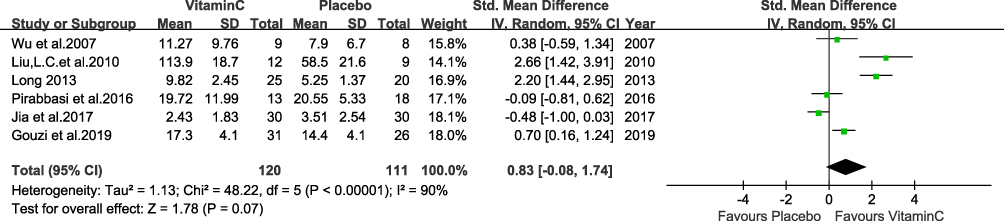 |
Figure 7 Serum vitamin E level. |
GSH Level in Serum in COPD Patients
Four RCTs, including 185 patients14,22,23,27 measured serum GSH levels, which were the major non-enzymatic antioxidants in the lung. The result from pooled data showed that serum GSH levels in vitamin C supplementation groups were higher than that of the placebo group (SMD:2.47, 95% CI: 1.06, 3.89, P=0.0006), with significant heterogeneity among these studies (I2=95%, P<0.00001). The result is shown in Figure 8.
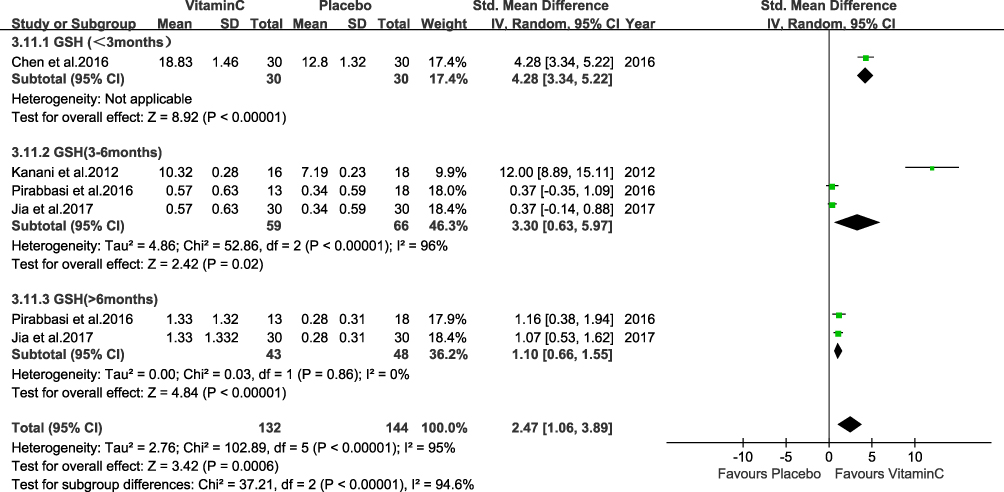 |
Figure 8 GSH level in serum in COPD patients. |
Included patients were divided into three subgroups based on the length of vitamin C supplementation: less than 3 month, 3 to 6 months, and over six months. And a subgroup analysis was conducted. As shown in Figure 8, in each subgroup, supplementation of vitamin C showed a trend to increase the GSH level in serum compared to supplementation with placebo. The difference was statistically significant.
Sensitivity analysis results showed that the study conducted by Kanani et al14 significantly influenced the results from the pooled data. In fact, in Kanani`s study, both vitamin C and vitamin E were used to treat patients as antioxidation agents, which was different from other involved studies, where only vitamin C was used against oxidation. There were studies showing that vitamin E isoform γ-tocotrienol reduced cigarette smoke-induced airway inflammation and oxidative stress so vitamin E might possess the therapeutic potential to treat COPD.28 However, no direct evidence supports the concept that vitamin E could increase the GSH level in serum. Thus, we decide that vitamin E combined with vitamin C in the treatment group may not be the source of heterogeneity in the present study and still keep Kanani`s study included.
Enzymatic Antioxidants of Lungs
Three RCTs, including 138 patients13,15,22 measured the level of serum SOD, which was the major enzymatic antioxidant in the lung. Overall, the result from the pooled data did not show a significant difference in terms of SOD level between the vitamin C group and placebo group (SMD: 0.42, 95% CI: −1.31, 2.15, 3 studies, P=0.64). The result is shown in Figure 9. Sensitivity analyses showed that no individual study significantly influenced the result from the pooled data.
 |
Figure 9 Enzymatic antioxidants of lungs. |
Nutrition Levels
Three studies including 148 patients15,23,27 reported changes in nutrition levels. The fixed effects model was used for the analysis of BMI (WMD: −0.17, 95% CI: −1.5, 1.16, P=0.81) and FFMI (WMD: −0.17, 95% CI: −1.06, 0.72, P=0.70). The results showed no significant improvement in BMI and FFMI by vitamin C treatment compared to placebo treatment. The results are shown in Figure 10.
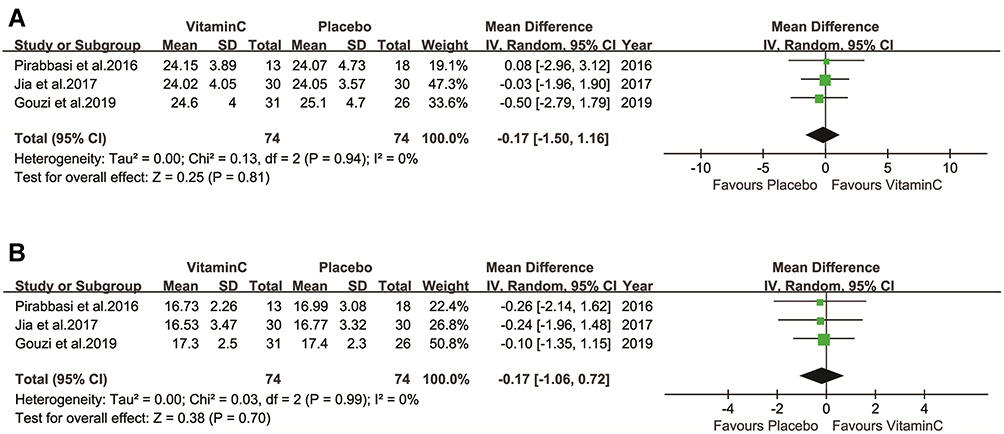 |
Figure 10 Nutrition levels (A, B). |
Discussion
Globally, more than 3 million people die from COPD every year, yet little progress in slowing the disease progression or reducing the mortality has been made.17 Oxidative stress, a result of the oxidant/antioxidant imbalance, has been suggested to play a critical role in the pathogenesis of COPD.4–6 An excess of oxidants may lead to the overexpression of pro-inflammatory genes, inactivation of antiproteases, and oxidative tissue injuries that lead to COPD.29 Various factors, including smoking and air pollution, have been proved to be able to increase systemic oxidative stress in patients with COPD.30 Overexposure to oxidants and /or decrease of antioxidants contribute to the development of COPD. One good example is smoking. In the over 4000 identified constituents of cigarette smoke, a large number of oxidants, especially different free radicals were found, which might be responsible for the extra oxidative stress in COPD patients who smoke.30,31 Antioxidant supplementation may improve the symptoms of COPD.6 Vitamin C is a well-known antioxidant supplementation. It has been shown that vitamin C supplementation were beneficial in COPD treatments by decreasing the damages caused by over oxidative stress.9 Thus, we conducted the present meta-analysis to summarize the effects of vitamin C administration in COPD patients, including pulmonary function, levels of serum antioxidant nutritional levels, to validate the function of vitamin C in treatment of COPD.
The results of the present meta-analysis showed that in COPD patients, vitamin C supplementation was significantly and positively correlated with the improvement of lung function, and higher levels of vitamin C and GSH in serum, but not other tested outcomes. Sensitivity analyses that excluded low-quality studies did not change these results. Through the subgroup analysis, we concluded that dose wisely, supplementation of more than 400 mg/day of vitamin C significantly improved lung function, while no significant change was found in patients supplemented with vitamin C less than 400 mg/day. We also conducted subgroup analysis based on the time of vitamin C supplementation, and the result showed vitamin C supplementation significantly increased the level of GSH in serum in all and each analyzed subgroup. No significant difference among the subgroups was found in terms of improvement of GSH levels in serum. All the evidence support that vitamin C intake provides a clinically meaningful benefit in COPD treatment.
Lung Function Increase
The mechanism of vitamin C supplementation to improve lung function remains unclear.7–9 Liu. et al have shown that vitamin C supplementation will enhance lung function and improves symptoms in COPD patients. Wu et al reported that the levels of dietary antioxidants, such as vitamin C, were positively correlated with lung function, but whether it was also beneficial in COPD treatment was unclear,6 which was contrary to the results from several other studies.13,14,22,24,25 Ansari et al showed that salbutamol and beclomethasone treatments in COPD patients showed noteworthy reductions in FEV1/FVC ratio, while a slight but non-significant drop was observed in FEV1/FVC ratio when vitamin C was added to standard therapy.26 Our meta-analysis results indicate that supplementing vitamin C might improve lung function in COPD patients, which was consistent with other studies.32–35 Such improvement might have many reasons. But the most important one might be its antioxidant property. Oxidative overload in COPD is quite common, mostly caused by hypoxia, and infection and plays a vital role in the impairment and remodeling of lung tissue. Vitamin C, as an antioxidant, has been widely used in many diseases sharing the same pathophysiologic characteristics as sepsis, ARDS, etc.36,37 It has been well proven that vitamin C can effectively attenuate oxidative stress, for which it may slow down the remodeling of lung structure and furtherly the deterioration of lung function.38 For instance, increased oxidative stress can lead to dysregulated antiproteases in lung tissue, which is the core of the pathogenesis of emphysema in COPD.39 Moreover, molecularly, oxidative stress has been found to contribute to pulmonary fibrosis. A bunch of studies show that imbalance between Reactive oxygen/nitrogen species (ROS/RNS), a sign of oxidative stress, leads to overexpression of some pro-fibrotic molecules, for example, TGF-β.40 Albeit there are several potential hypotheses that can explain the improving effect of vitamin C on lung function, there is still a lack of direct study focusing on their relationships. More attention is needed on this topic.
Antioxidants in Serum
The underlying mechanisms by which the lung defends against possible oxidative challenges itself depend on two different types of antioxidants: non-enzymatic antioxidants, including glutathione, vitamin C and E, beta-carotene uric acid and enzymatic antioxidants such as superoxide dismutase, catalase and peroxidases.7 Even for those people who smoke cigarettes, the DNA break induced by H2O2− in the smoke was negatively correlated with the vitamin C level in serum, and the correlation was statistically significant.6 Compared to those of nonsmokers, the levels of major plasma antioxidants (vitamin C, vitamin E and GSH) in smokers are decreased.14,41 Superoxide dismutases (SODs) are a family of metalloenzymes that convert O2– to H2O2. Catalase and glutathione peroxidase neutralize H2O2 into water and oxygen.28,29,42 Peh et al showed that inhibition of the activities of these three key antioxidant enzymes would increase oxidative stress, which contributed to the incidence of emphysema.28 Vitamin C is a widely used antioxidant. In addition to its role as an enzyme cofactor, vitamin C is a critical, chain-breaking antioxidant in the aqueous phase.43 Vitamin C can be rapidly depleted by electron spin resonance in the presence of increased free radical production in body fluids,44 which is a part of the antioxidation process mediated by vitamin C. After being supplemented with vitamin C, the DNA break induced by H2O2 was significantly decreased,6 providing an appropriate environment to regenerate GSH radicals.45
The primary function of vitamin E is working as a chain-breaking antioxidant.46 Vitamin C can facilitate the conversion of oxidized vitamin E into non-oxidized vitamin E to increase the serum concentration of non-oxidized vitamin.47,48 Moreover, vitamin C demonstrated a synergistic effect with vitamin E in antioxidant activity.28 Hanson. et al pointed out that increasing serum vitamin E was protective against COPD mortality.46,49
In the present study, a panel of antioxidants demonstrated a tendency of increased concentration in serum after being supplemented with vitamin C, but only the increase of serum vitamin C and GSH was statistically significant. Among all the studies, Liu et al showed a result about serum vitamin C and SOD that was opposite to the conclusions from other included studies.13 However, in Liu et al study, the baseline vitamin C level in the vitamin C supplementation group was significantly lower than that of the control group. In addition, there were only 21 patients involved in their study, making it impossible to ignore the baseline difference in vitamin C between the two groups. Vitamin C could enhance the reuse of vitamin E, which could increase the activity of individual SOD molecules. Therefore, to keep the total SOD activity at a certain level, the total amount of SOD decreased.
In summary, vitamin C supplementation could improve the antioxidant capacity in serum, enhance the antioxidant ability in COPD patients and reduce the mortality rate of COPD.
Nutritional Condition
Malnutrition is a problem that is often overlooked during the treatment of COPD.50 About 20–50% of COPD patients suffer weight loss and protein and calorie malnutrition,27,50 which contribute to the dysfunction of respiratory muscles, the severity of the disease, the progression of disability, and eventually the mortality of the disease.17,51 Mete et al found that pulmonary function was significantly lower in those COPD patients with low BMI and malnutrition.50 Similarly, the amount of fat-free body mass was also found significantly lower in COPD patients falling in a low BMI category and in patients who were at malnutrition risk or with malnutrition.50 Decreased FFMI could lead to biologically negative consequences in COPD.52,53 These indicated that total body mass and FFM are important prognostic factors in COPD. An imbalance of antioxidants may lead to systemic inflammation, which has been shown to damage bones and muscles, reduce ventilatory capacity, and reduce lung function.54,55
Meanwhile, oxidative stress is an important contributing factor in the pathogenesis of COPD and eventually results in poor respiratory function.27 The limited gas exchange will lead to a sedentary lifestyle, which in turn results in the loss of appetite and nutrient deficiency through consumption of a low-antioxidant diet as feedback. The resulted malnutritional status would promote the disease progression and increase the oxidative stress in patients, which would further deteriorate the existing malnourishment in patients and increase the disease severity.54,56 Multiple studies showed that oxidative stress was indeed a deleterious factor leading to the dysfunction and atrophy of muscles in COPD patients.15,57 Antioxidants play a key role in improving muscle endurance58 and atrophy in COPD.59 Although Gouzi et al pointed out that vitamin C failed to improve quadriceps endurance as a pulmonary rehabilitation supplementation, the improved quadriceps muscle strength, total protein in serum, and type I fiber proportion in vitamin C-treated patients demonstrated a trend toward improved muscle endurance.15 A Cochrane systematic review found that low BMI and fat-free mass index (FFMI) conditions in the COPD population were related to a poor prognosis.60 These findings are consistent with our results that vitamin C supplementation in COPD patients may improve their nutritional status.
Advantages and Limitations
Our research has some advantages. It is the first systematic review and meta-analysis to evaluate the impact of vitamin C supplementation in COPD patients. Second, we conducted a subgroup analysis based on vitamin C intake dosage and found that vitamin C greater than 400 mg improved the symptoms in COPD patients. We also found that intake of vitamin C may contribute to the nutritional improvement in COPD by enhancing quadriceps muscle strength and total serum protein,15 which remains to be confirmed. Based on these results, COPD patients may benefit from vitamin C, especially when given at a dose greater than 400 mg/day.
However, this meta-analysis and systematic review still have some limitations. Rabe et al classified COPD into two types: pink-puffer phenotype of COPD (are primarily affected by emphysema) and blue bloater phenotype of COPD (predominantly have chronic bronchitis) according to various clinical manifests.17 In the present study, we did not analyze the data based on the type of COPD, which may contribute to the irrelevancy of vitamin C to the certain investigated outcomes in this study. Moreover, the relatively small number of included studies and the ethnicity of the patient population included in the study may introduce bias to the result of our meta-analysis.61,62
Conclusion
In conclusion, we found that supplementing vitamin C to patients with COPD demonstrated vital clinical significance. It can promote lung function and serum antioxidant levels by decreasing oxidative damage to the lung. Meanwhile, we also found that vitamin C supplementation could increase the antioxidant level in serum, but not the nutritional level in COPD patients. These result needs to be further confirmed by large and well-designed prospective RCTs.
Acknowledgments
We thank professor Kehu Yang from the Evidence-Based Medicine Center of Lanzhou University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Science and technology project of Chengguan District (2017SHFZ0038). Program of Lanzhou Science and Technology Development Plan (grant number 2018-3-57); Science and Technology Projects of Gansu Province (grant number 18JR3RA344).
Disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. And all authors declare that they have no conflict of interest.
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
References
1. Prevention GSF. Global initiative for chronic obstructive lung disease; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
4. MacNee W. Pulmonary and systemic oxidant/antioxidant imbalance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(1):50–60. doi:10.1513/pats.200411-056SF
5. Morrison D, Rahman I, Lannan S, MacNee W. Epithelial permeability, inflammation, and oxidant stress in the air spaces of smokers. Am J Respir Crit Care Med. 1999;159(2):473–479. doi:10.1164/ajrccm.159.2.9804080
6. Wu TC, Huang YC, Hsu SY, Wang YC, Yen SL. Vitamin E and vitamin C supplementation in patients with chronic obstructive pulmonary disease. Int J Vitam Nutr Res. 2007;77(4):272–279. doi:10.1024/0300-9831.77.4.272
7. Rahman I, Biswas SK, Kode A. Oxidant and antioxidant balance in the airways and airway diseases. Eur J Pharmacol. 2006;533(1–3):222–239. doi:10.1016/j.ejphar.2005.12.087
8. Barnes PJ, Ito K, Adcock IM. Corticosteroid resistance in chronic obstructive pulmonary disease: inactivation of histone deacetylase. Lancet. 2004;363(9410):731–733. doi:10.1016/S0140-6736(04)15650-X
9. Romieu I, Trenga C. Diet and obstructive lung diseases. Epidemiol Rev. 2001;23(2):268–287. doi:10.1093/oxfordjournals.epirev.a000806
10. Church DF, Pryor WA. Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect. 1985;64:111–126. doi:10.1289/ehp.8564111
11. Nakayama T, Church DF, Pryor WA. Quantitative analysis of the hydrogen peroxide formed in aqueous cigarette tar extracts. Free Radic Biol Med. 1989;7(1):9–15. doi:10.1016/0891-5849(89)90094-4
12. Shaheen SO, Jameson KA, Syddall HE, et al. The relationship of dietary patterns with adult lung function and COPD. Eur Respir J. 2010;36(2):277–284. doi:10.1183/09031936.00114709
13. Liu LC, Huang CY, Huang JJ, Lee HC, Huang SY. The effect of vitamin C & E supplement on the antioxidative status in patients with chronic obstructive pulmonary disease: a double-blind placebo-control pilot study. Nutr Sci J. 2010;35(2):
14. Kanani NJ, Patel SA, Hotchandani SC, Bhatt JD. A study of efficacy of antioxidant therapy in the management of chronic obstructive pulmonary disease. Res J Pharm Biol Chem Sci. 2012;3(4):1071–1078.
15. Gouzi F, Maury J, Héraud N, et al. Additional effects of nutritional antioxidant supplementation on peripheral muscle during pulmonary rehabilitation in COPD patients: a randomized controlled trial. Oxid Med Cell Longev. 2019;2019:5496346. doi:10.1155/2019/5496346
16. McNicholas WT. COPD-OSA overlap syndrome: evolving evidence regarding epidemiology, clinical consequences, and management. Chest. 2017;152(6):1318–1326. doi:10.1016/j.chest.2017.04.160
17. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
18. Fu Y, Zha S, Lü N, et al. Carrier frequencies of hearing loss variants in newborns of China: a meta-analysis. J Evid Based Med. 2019;12(1):40–50. doi:10.1111/jebm.12305
19. Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: a systematic review and meta-analysis. J Evid Based Med. 2020;13(2):93–101. doi:10.1111/jebm.12381
20. Pan B, Ge L, Xun YQ, et al. Exercise training modalities in patients with type 2 diabetes mellitus: a systematic review and network meta-analysis. Int J Behav Nutr Phys Act. 2018;15(1):72. doi:10.1186/s12966-018-0703-3
21. Higgins JPT, Green S Cochrane handbook for systematic reviews of interventions version 5.0.1; 2008.
22. Chen M, Zhixian J, Hong B, Junyi D. Research of vitamin C in the treatment of patients with AECOPD. J Clin Pulm Med. 2016;2016(3):456–459.
23. Jia T, Jian H. Effect of antioxidants supplementation on nutritional and antioxidant status of chronic obstructive pulmonary disease patients. J Clin Pulm Med. 2017;22(11):2009–2013.
24. Long Z. Chronic obstructive pulmonary disease patients breathing muscle recovery and vitamin D, E relationship. Natl Med Front China. 20132013;(21):25–26.
25. Zou Y, Fengping L. Influence of antioxidant vitamins combined with moderate protein diet on lung function and quality of life of COPD patients in stable phase. Chin Nurs Res. 2015;29(10B):1.
26. Ansari MA, Ansari S, Memon Z. Does antioxidant ascorbic acid supplementation delay lung function deterioration in stable patients with chronic obstructive? Pulmonary disease. Rawal Med J. 2010;35(2):133–136.
27. Pirabbasi E, Shahar S, Manaf ZA, Rajab NF, Manap RA. Efficacy of ascorbic acid (vitamin C) and/N-Acetylcysteine (NAC) supplementation on nutritional and antioxidant status of male Chronic Obstructive Pulmonary Disease (COPD) Patients. J Nutr Sci Vitaminol. 2016;62(1):
28. Peh HY, Tan WSD, Chan TK, Pow CW, Foster PS, Wong WSF. Vitamin E isoform γ-tocotrienol protects against emphysema in cigarette smoke-induced COPD. Free Radic Biol Med. 2017;110:332–344. doi:10.1016/j.freeradbiomed.2017.06.023
29. Drost EM, Skwarski KM, Sauleda J, et al. Oxidative stress and airway inflammation in severe exacerbations of COPD. Thorax. 2005;60(4):293–300. doi:10.1136/thx.2004.027946
30. Saad A, Mostafa A, Ibrahim K. Role of natural juice in improving the ventilatory functions of smokers with chronic obstructive pulmonary disease. J Nutr Environ Med. 2007;16(1):
31. Marangon K, Herbeth B, Lecomte E, et al. Diet, antioxidant status, and smoking habits in French men. Am J Clin Nutr. 1998;67(2):231–239. doi:10.1093/ajcn/67.2.231
32. Schwartz J, Weiss ST. Relationship between dietary vitamin C intake and pulmonary function in the first National Health and Nutrition Examination Survey (NHANES I). Am J Clin Nutr. 1994;59(1):110–114. doi:10.1093/ajcn/59.1.110
33. Britton JR, Pavord ID, Richards KA, et al. Dietary antioxidant vitamin intake and lung function in the general population. Am J Respir Crit Care Med. 1995;151(5):1383–1387. doi:10.1164/ajrccm.151.5.7735589
34. Hu G, Zhang X, Chen J, Peto R, Campbell TC, Cassano PA. Dietary vitamin C intake and lung function in rural China. Am J Epidemiol. 1998;148(6):594–599. doi:10.1093/oxfordjournals.aje.a009685
35. Chen R, Tunstall-Pedoe H, Bolton-Smith C, Hannah MK, Morrison C. Association of dietary antioxidants and waist circumference with pulmonary function and airway obstruction. Am J Epidemiol. 2001;153(2):157–163. doi:10.1093/aje/153.2.157
36. Martimbianco ALC, Pacheco RL, Bagattini ÂM, De Fátima Carreira Moreira Padovez R, Azevedo LCP, Riera R. Vitamin C-based regimens for sepsis and septic shock: systematic review and meta-analysis of randomized clinical trials. J Crit Care. 2022;71:154099. doi:10.1016/j.jcrc.2022.154099
37. Boretti A, Banik BK. Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition. 2020;12:100190. doi:10.1016/j.phanu.2020.100190
38. Barnes PJ. Oxidative stress in chronic obstructive pulmonary disease. Antioxidants. 2022;11(5):965. doi:10.3390/antiox11050965
39. Mizumura K, Maruoka S, Shimizu T, Gon Y. Autophagy, selective autophagy, and necroptosis in COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:3165–3172. doi:10.2147/COPD.S175830
40. Estornut C, Milara J, Bayarri MA, Belhadj N, Cortijo J. Targeting oxidative stress as a therapeutic approach for idiopathic pulmonary fibrosis. Front Pharmacol. 2021;12:794997. doi:10.3389/fphar.2021.794997
41. Calikoğlu M, Unlü A, Tamer L, Ercan B, Buğdayci R, Atik U. The levels of serum vitamin C, malonyldialdehyde and erythrocyte reduced glutathione in chronic obstructive pulmonary disease and in healthy smokers. Clin Chem Lab Med. 2002;40(10):1028–1031. doi:10.1515/CCLM.2002.179
42. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
43. Jialal I, Vega GL, Grundy SM. Physiologic levels of ascorbate inhibit the oxidative modification of low density lipoprotein. Atherosclerosis. 1990;82(3):185–191. doi:10.1016/0021-9150(90)90039-L
44. Pietri S, Séguin JR, D’Arbigny PD, Culcasi M. Ascorbyl free radical: a noninvasive marker of oxidative stress in human open-heart surgery. Free Radic Biol Med. 1994;16(4):523–528. doi:10.1016/0891-5849(94)90131-7
45. De Flora S, Bennicelli C, Camoirano A, et al. In vivo effects of N-acetylcysteine on glutathione metabolism and on the biotransformation of carcinogenic and/or mutagenic compounds. Carcinogenesis. 1985;6(12):1735–1745. doi:10.1093/carcin/6.12.1735
46. Hanson C, Lyden E, Furtado J, et al. Serum tocopherol levels and vitamin E intake are associated with lung function in the normative aging study. Clin Nutr. 2016;35(1):169–174. doi:10.1016/j.clnu.2015.01.020
47. Ives SJ, Harris RA, Witman MA, et al. Vascular dysfunction and chronic obstructive pulmonary disease: the role of redox balance. Hypertension. 2014;63(3):459–467. doi:10.1161/HYPERTENSIONAHA.113.02255
48. Rossman MJ, Groot HJ, Reese V, Zhao J, Amann M, Richardson RS. Oxidative stress and COPD: the effect of oral antioxidants on skeletal muscle fatigue. Med Sci Sports Exerc. 2013;45(7):1235–1243. doi:10.1249/MSS.0b013e3182846d7e
49. Walda IC, Tabak C, Smit HA, et al. Diet and 20-year chronic obstructive pulmonary disease mortality in middle-aged men from three European countries. Eur J Clin Nutr. 2002;56(7):638–643. doi:10.1038/sj.ejcn.1601370
50. Mete B, Pehlivan E, Gülbaş G, Günen H. Prevalence of malnutrition in COPD and its relationship with the parameters related to disease severity. Int J Chron Obstruct Pulmon Dis. 2018;13:3307–3312. doi:10.2147/COPD.S179609
51. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–109. doi:10.2147/COPD.S54473
52. Heitmann BL, Erikson H, Ellsinger BM, Mikkelsen KL, Larsson B. Mortality associated with body fat, fat-free mass and body mass index among 60-year-old Swedish men-a 22-year follow-up. The study of men born in 1913. Int J Obes Relat Metab Disord. 2000;24(1):33–37. doi:10.1038/sj.ijo.0801082
53. Bigaard J, Frederiksen K, Tjønneland A, et al. Body fat and fat-free mass and all-cause mortality. Obes Res. 2004;12(7):1042–1049. doi:10.1038/oby.2004.131
54. Agustí AG, Noguera A, Sauleda J, Sala E, Pons J, Busquets X. Systematic effects of chronic obstructive pulmonary disease. Eur Respir J. 2003;21(2):347–360. doi:10.1183/09031936.03.00405703
55. Agustí AG, Sauleda J, Miralles C, et al. Skeletal muscle apoptosis and weight loss in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166(4):485–489. doi:10.1164/rccm.2108013
56. Agusti AG. COPD, a multicomponent disease: implications for management. Respir Med. 2005;99(6):670–682. doi:10.1016/j.rmed.2004.11.006
57. Maltais F, Decramer M, Casaburi R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(9):e15–62. doi:10.1164/rccm.201402-0373ST
58. Koechlin C, Couillard A, Simar D, et al. Does oxidative stress alter quadriceps endurance in chronic obstructive pulmonary disease? Am J Respir Crit Care Med. 2004;169(9):1022–1027. doi:10.1164/rccm.200310-1465OC
59. Pomiès P, Blaquière M, Maury J, Mercier J, Gouzi F, Hayot M. Involvement of the FoxO1/MuRF1/Atrogin-1 signaling pathway in the oxidative stress-induced atrophy of cultured chronic obstructive pulmonary disease myotubes. PLoS One. 2016;11(8):e0160092. doi:10.1371/journal.pone.0160092
60. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:Cd000998. doi:10.1002/14651858.CD000998.pub3
61. Yao L, Sun R, Chen YL, et al. The quality of evidence in Chinese meta-analyses needs to be improved. J Clin Epidemiol. 2016;74:73–79. doi:10.1016/j.jclinepi.2016.01.003
62. Yan P, Yao L, Li H, et al. The methodological quality of robotic surgical meta-analyses needed to be improved: a cross-sectional study. J Clin Epidemiol. 2019;109:20–29. doi:10.1016/j.jclinepi.2018.12.013
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.