")
Back to Journals » Open Access Journal of Contraception » Volume 14
Efficacy of Tubal Surgery for Permanent Contraception: Considerations for the Clinician
Received 31 December 2022
Accepted for publication 26 February 2023
Published 17 March 2023 Volume 2023:14 Pages 53—59
DOI https://doi.org/10.2147/OAJC.S385255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Julia Tasset, Jeffrey T Jensen
Department of Obstetrics and Gynecology, Oregon Health & Sciences University, Portland, OR, USA
Correspondence: Julia Tasset, Department of Obstetrics and Gynecology, Oregon Health & Sciences University, 3181 SW Sam Jackson Park Road, Mailstop L466, Portland, OR, 97239, USA, Tel +1 503 494 9556, Fax +1 503 494 2391, Email [email protected]
Abstract: Permanent contraception meets the needs of many people certain in their decision to never become pregnant in the future. Female permanent contraception procedures became more common than male procedures during the 1970s and 1980s, when laparoscopic surgery became widely available. To better understand the efficacy of these new procedures, the US Centers for Disease Control and Prevention conducted a prospective cohort study, known as the Collaborative Review of Sterilization (CREST). For decades, results of this study have defined perioperative counseling around failure risks of such surgeries. However, laparoscopic technology and techniques have changed significantly in recent decades and evidence has emerged supporting noncontraceptive benefits of tubal excision. Therefore, we present here a review of updated information regarding permanent contraception failure in the modern context and implications for clinical practice and future research directions.
Keywords: permanent contraception, gynecology, birth control
Introduction
Despite the wide availability of reversible, highly effective, and less invasive options for birth control, permanent tubal contraception (PC) remains a popular option for limiting family size. Indeed, the US Centers for Disease Control and Prevention’s (CDC) National Survey of Family Growth from 2017 to 2019 indicates approximately one-third of women aged 40–49 years have undergone PC.1 The efficacy of these surgeries, defined as prevention of spontaneous conception, is a major rationale many patients cite as their impetus to undergo these procedures. The main body of evidence supporting the efficacy of surgery for PC comes from the CDC’s seminal study, the Collaborative Review of Sterilization (CREST). Since the 1970–80s when this work was conducted, considerable shifts in the landscape of minimally invasive gynecologic surgery have occurred suggesting that the CREST data may be less applicable to modern practice. We, therefore, have undertaken a review to describe the available contemporary evidence regarding PC efficacy, to identify gaps in the field relevant for future work and facilitate better patient perioperative counseling. We limit our review to tubal interruption from an abdominal approach (either by surgical removal or device placement) rather than hysteroscopic tubal occlusion, given that there are no currently available modalities for this approved by the US Food and Drug Administration (FDA). In addition, we acknowledge that many of the methods described in this paper could be utilized from a vaginal approach via posterior colpotomy, but this practice is not widely utilized in this country and, therefore, not explored here.2
Throughout this paper, we use the preferred nomenclature of permanent contraception, using sterilization only in historic reference to prior publications that use that term. The antiquated terminology “sterilization” is highly pejorative and associated with a history of deplorable campaigns of eugenics carried out in many countries, including the United States. While there is no question that involuntary family planning of any type is an unacceptable violation of human rights, so are policies that restrict a woman’s right to choose the most effective and acceptable methods of family planning to prevent unwanted pregnancy. Use of the term sterilization to describe modern approaches to PC also lacks biologic accuracy. Although these procedures block natural pregnancy, many pathways to fertility exist for people with ovaries (eg in vitro fertilization, surrogacy).
Collaborative Review of Sterilization (CREST) Study
In order to better understand success rates of a variety of modalities for PC, the CDC conducted the CREST study: a multicenter, prospective cohort study comparing laparoscopic unipolar coagulation, laparoscopic bipolar coagulation, laparoscopic silicone rubber band application, laparoscopic spring clip application, or partial salpingectomy (including modified Pomeroy-type ligation, other types of partial salpingectomy, and total salpingectomy) performed by laparotomy.3 This multicenter study prospectively enrolled over 10,000 women between 1978 to 1986 with planned follow-up of five years. Study staff at the collaborating centers approached women and obtained study consent to participate prior to surgery. They collected baseline demographic data and then recorded surgical and postsurgical outcomes. Study staff contacted participants by phone approximately one month after the procedure for a brief follow-up interview, and then annually. Given the long duration of enrollment, some centers continued following participants for up to 14 years. At each follow-up, participants were asked “Since your tubal sterilization, have you had a positive pregnancy test or been told by a physician that you were pregnant?” Positive responses triggered chart reviews of all available data. The investigators classified pregnancies as: (1) true procedure failure; (2) luteal phase pregnancy (pregnancy conceived before procedure but identified after); (3) pregnancy resulting from infertility treatment (tubal anastomosis or in vitro fertilization). The main results, published in 1996 reported efficacy rates for several common laparoscopic techniques and postpartum minilaparotomy.
It is important to consider the context of the study. The introduction of laparoscopy as a method of PC in the 1970s shifted the landscape of permanent contraception from procedures primarily performed on men (vasectomy) to women. By 1988, PC had become the leading method of family planning used by women, a distinction that remains today.1 The CREST study was designed and conducted during this transformative time.
In the 1970s and 1980s, laparoscopic gynecologic surgery looked dramatically different from today. Although residency training programs had begun to teach the skills, many practicing clinicians picked up the techniques without formal training. Given the rapid adoption of the technique, it made sense for the CDC to study safety and efficacy of the approach. From a technology standpoint, it was not until 1986 (the last year of study enrollment) that a computer chip television camera was available to be attached to a laparoscope for video guidance, allowing those other than the primary surgeon to visualize the surgical field and assist in the procedure. Several of the commonly used approaches studied in CREST are no longer in use, and other techniques such as the titanium clip, were not introduced until 1996. Similarly, total salpingectomy was not routinely performed for the purpose of PC at the time of the CREST study. Despite these limitations, CREST represents a landmark study with important findings that remain relevant to modern practice and research. As we review more recent studies, keep the main conclusions of the CREST study in mind;
Although tubal sterilization is highly effective, the risk of sterilization failure is higher than generally reported. The risk persists for years after the procedure and varies by method of tubal occlusion and age.3
Open Approaches
Partial Salpingectomy via Laparotomy or Minilaparotomy
Historically, PC was performed with an open approach, either after a birth or as an interval procedure greater than 42 days after a delivery. There are a variety of methods for performing partial tubal excision, the most common of which include the Pomeroy, modified Pomeroy, and the Parkland methods. Each of these involve removal of a 2–3 cm portion of the mid-isthmic portion of the fallopian tube via suture ligation after identifying and dissecting an avascular window in the mesosalpinx.4 Typically, in this method, the fimbriae are avoided given concerns about increased risk of recanalization and surgical failure with fimbriectomy and interruption in the ampullae, regions with complex redundant luminal folds.5
Despite declining rates of immediate postpartum PC (now 6–7% of live births, down from 8–9% in the late 1990s) performing these procedures during a hospitalization for childbirth remains a critical access opportunity for many people seeking PC.6 This trend likely follows the increasing availability of long-acting, reversible contraceptives as well as wider availability of minimally invasive interval PC. Such minimally invasive techniques offer a shorter recovery time and lower risk of complications over open surgery for those who desire a PC procedure independent from a pregnancy. Indeed, in 2021, greater than 85% of benign adnexal surgery is performed minimally invasively, a trend which is likely mirrored in PC-specific procedures.7
Of the modern methods for PC, postpartum open partial salpingectomy is least likely to have changed significantly in terms of efficacy from the late 1970s and early 1980s, as these techniques have not evolved over time. In the CREST study, pregnancy after postpartum partial salpingectomy occurred on average after 0.6 per 1000 procedures over one year and 7.5 per 1000 procedures over 10 years.3 More recently, the Cochrane Collaboration performed a meta-analysis in 2016 that identified two randomized controlled trials which examined postpartum partial salpingectomy and were powered to assess the rate of procedure failure (Table 1).8–10 This analysis showed limited, moderate quality evidence with similar failure rates to CREST data.8
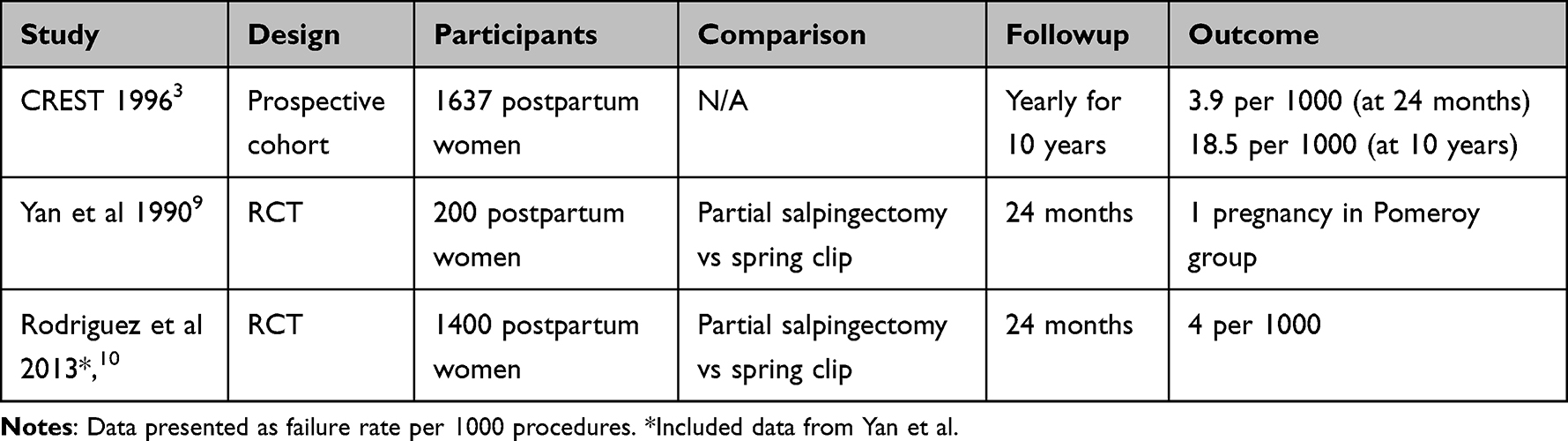 |
Table 1 Postpartum Partial Salpingectomy Failure Rates |
Laparoscopic Approaches
As mentioned above, the introduction of laparoscopy resulted in the development of a variety of approaches for tubal interruption using occlusive devices or energy sources. Below, we briefly summarize the major techniques in use with published data on efficacy (Table 2). Some additional approaches have been described, but lack efficacy data, including laparoscopic segmental tubal resection, and are therefore not presented here.
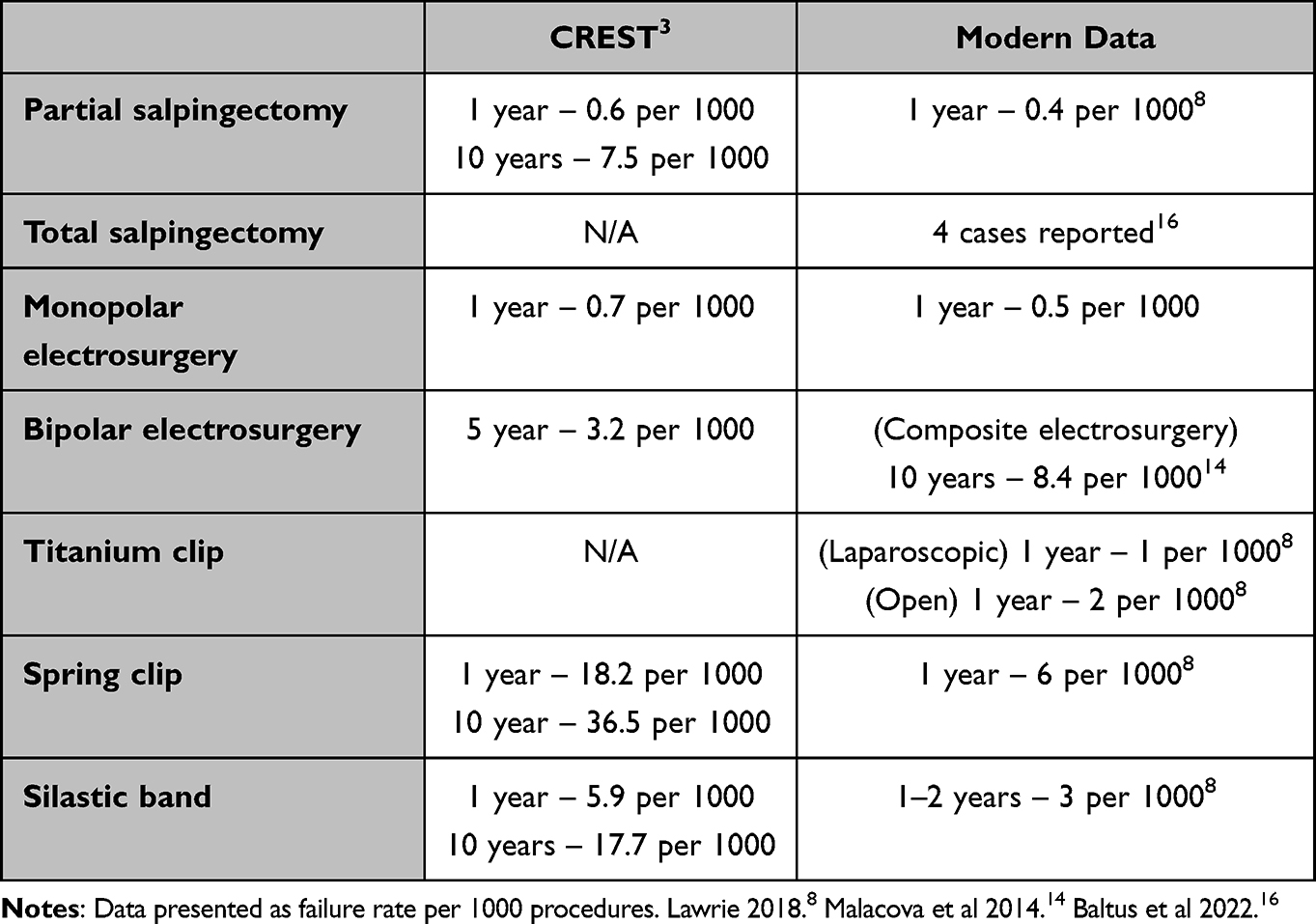 |
Table 2 CREST and Modern Efficacy Data by Surgical Type |
Monopolar Electrocautery
Monopolar electrocautery involves thermal destruction of tissue by transferring a high frequency electric current through a single electrode. Clinicians early in the evolution of laparoscopic surgery had limited tools at their disposal, one of which was monopolar energy. This approach typically involved coagulation of the isthmic portion of the tube, although the exact location and width was not well defined in the literature. Monopolar coagulation demonstrated good efficacy in the CREST study, with a one year cumulative failure rate of 0.7 per 1000 procedures (7.5 per 1000 over 10 years). However, this has fallen out of common use, likely related to safety concerns: out of the four deaths attributed to tubal occlusion surgery during the CREST study, three resulted from bowel injuries after use of monopolar devices.3 The routine use of noninsulated metal ports and lack of video camera assistance during the study period likely contributed to these outcomes.
The Cochrane 2016 meta-analysis identified multiple trials assessing “electrocoagulation” which were powered to analyze efficacy. These data largely pertain to minilaparotomy or laparoscopy with monopolar energy. Analysis of two trials revealed a failure rate of 0.5 per 1000 procedures over one year of follow-up.8
Bipolar Electrocautery
Conventional bipolar electrocautery was introduced in the United States in the 1970s.11 In contrast to unipolar, where current enters the operative field through an electrode and exits through a ground plate, the physics of bipolar improves safety as current passes from one electrode to another through the tissue grasped by the instrument. As the tissue desiccates completely, current ceases to flow. This prevents inadvertent tissue damage due to arcing seen with monopolar, However, many early bipolar devices did not include an ammeter to monitor current flow. This required a surgeon’s judgment to assess for complete tissue coagulation. Incomplete coagulation may result in failure of tubal occlusion. Next generation advanced bipolar generators devices included visual or auditory signals of the impedance meters.12 This feature decreases the chances of incomplete coagulation of a patent vessel (or, in the case of PC, a patent fallopian tube lumen). When applied to PC procedures, bipolar devices were typically used to completely coagulate a cross section of the fallopian tube in three locations along the isthmus, although this technique was not initially well standardized.
With regard to bipolar coagulation, a CREST subset analysis provides evidence that improved laparoscopic techniques positively influenced outcomes: in the two time periods of the study (1978–1982 and 1985–1987, respectively) the proportion of surgeons using highly effective surgical technique (≥3 tubal coagulation sites) increased and five-year cumulative risk of pregnancy decreased from 27.1 to 3.2 per 1000 procedures.13
A retrospective Australian cohort attempted to examine the risk of surgical failure after PC, including laparoscopic electrodestruction (monopolar vs bipolar energy not specified). They included 44,829 women who underwent surgery from 1990 to 2010 in Western Australia. They found a high rate of surgical failure (specifically ectopic pregnancy), with a cumulative 10-year probability of ectopic pregnancy of 8.4 per 1000 procedures.14 This risk was highest in the first five years after surgery.14 Of the 19 women who had electrodestruction of the tubes during an open procedure, none had a pregnancy recorded over 15 years of follow-up.14 This stark difference may be related to small sample size of the open surgery group, and features of laparoscopic technique in this region and the time period.
Spring (“Hulka”) Clip
The spring “Hulka” clip was the first device for tubal occlusion brought to the market in 1972.15 It offered a safety advantage over electrocautery in an era when laparoscopic cameras were not widely available and visualization was limited. However, the spring clip mechanism requires initiation of the trigger to close the jaws around the tissue, direct visual inspection of proper alignment, and then completion of full depression of the trigger to lock the device.4 This cumbersome process likely led to failures in some cases.
The spring clip was studied in the CREST experiment and was found to have the poorest efficacy, with a one year failure rate of 18.2 per 1000 procedures and a 10-year failure rate of 36.5.3 The inferior performance of this device was reinforced in the 2016 Cochrane meta-analysis, with cumulative failure rate of six per 1000 laparoscopic procedures after one year of follow-up.8 These results led clinicians to move toward other devices, such as the titanium clip and silastic band. The titanium clip is no longer marketed.
Titanium (“Filshie”) Clip
The titanium “Filshie” clip is a contraceptive tubal occlusive device designed for laparoscopic application.4 It consists of a clip with a single-action jaw which is applied via a customized metal applicator. The locking mechanism consists of a longer, lower jaw which catches the shorter, upper jaw as the device is closed around the isthmus of the fallopian tube, creating an occlusive seal. After the withdrawal of the titanium clip from the US market, the spring clip became one of the most widely used mechanical method.
The titanium clip was approved by the FDA in 1996 and therefore was not included in the efficacy data reported in the CREST study. In the 2016 meta-analysis, two randomized controlled trials assessed efficacy of laparoscopic application of titanium clips for PC.8 Ultimately, this was consistent with a one-year failure rate of one per 1000 procedures. With regard to open surgery, the same analysis found three randomized controlled trials of postpartum application of titanium clips, which cumulatively had a failure rate at one year of two per 1000 procedures.8
Silastic (“Falope”) Band
The Silastic “Falope” band involves use of a proprietary metal applicator with thin tongs to pull several millimeters of fallopian tube into the barrel of the device.4 An occlusive band is then deployed over the loop of tissue.
The silastic band was included in CREST analysis, which showed a one year cumulative failure rate of 5.9 per 1000 procedures (17.7 per 1000 over 10 years).3 The Cochrane meta-analysis synthesized of six randomized controlled trials (published in 1985 through 2004) with a cumulative failure rate of three in 1000 procedures over one-to-two years.8
Laparoscopic or Open Total Salpingectomy
The efficacy of total bilateral salpingectomy was not studied in the CREST trial. In recent years, interval laparoscopic or open postpartum salpingectomy has been popularized due to the epidemiologic evidence that suggests tubal removal significantly decreases the risk of ovarian cancer.16 Interestingly, the maximum benefit for cancer prevention appears to be in removal of the tubal fimbriae, which, based on fimbriectomy and partial salpingectomy results, appears to have the least impact on success of PC procedures.5 Surveys indicate that up to 50% of surgeons now routinely perform bilateral salpingectomy for interval PC.16
In addition to primary cancer prevention, many postulate that total salpingectomy confers superior protection against postoperative pregnancy than other surgical techniques, although this has not been well studied. As of this writing, no prospective data are available, but a randomized clinical trial is underway to evaluate pregnancy risk after total salpingectomy.18 A large retrospective cohort of over 44,000 patients conducted in Australia from 1990 to 2010 showed no pregnancies after 15 years of follow-up of approximately 600 patients who underwent interval or postpartum salpingectomy.14 A systematic review of the literature in 2022 yielded four case reports of patients who experienced spontaneous conception after bilateral salpingectomy.17 It is interesting to note that all of these occurred after surgery for other pelvic pathology (pelvic inflammatory disease, hydrosalpinx, or ectopic pregnancy), and not for PC. The technical challenges of these cases may have contributed to procedural failure. There have been no reported cases of procedural failure after bilateral salpingectomy for PC, although fistulous connection between proximal tubal ostia and ovarian fossa could theoretically allow this to occur.
Discussion
Surgical PC is highly effective, however, failure rates differ based on the technique used. While most failures occur during the first year of use, failures have been reported years later. This is likely due in part to the fecundity of people who present at younger ages for PC. Both CREST data and the retrospective Australian cohort data indicate higher failure rates with patient ages less than 28 years. This implies that the 10-year risk of failure for a 25 year old and a 40 year old patient would not be the same even if identical methods were utilized. It is important to consider the reduced risk of pregnancy in study populations, and contextualize that while counseling patients.
In addition to surgical modality and age-related changes in fecundity, several other factors likely impact surgical success. Patients with a history of inflammatory pathology in the pelvis (such as prior pelvic inflammatory disease, abdominopelvic surgery, gastrointestinal infections such as appendicitis, or ectopic pregnancy) likely have a higher risk of failed surgery owing on part to either enhanced difficulty of surgical technique leading to surgical error (such as banding or removing part of the round ligament) or possibly recanalization or fistulization of proximal ostia. It has been postulated that an early presentation of pregnancy (less than one year) after PC most likely indicates a failure of surgical technique.19 When counseling a patient about surgical treatment options after PC failure, pending the clinical scenario, it may be reasonable to consider imaging to evaluate location of tubal-peritoneal communication and the relationship of tubes to other adnexal structures, in the case of a surgically complex patient.
Conclusions and Future Directions
PC remains an important contraceptive option for people who have completed their families. Since the publication of CREST, modern studies provide additional nuance to that seminal trial’s results and continue to imply high efficacy for contemporary approaches to the procedure. Improved technology such as the titanium clip, which has been brought to market and shows superior efficacy to the spring clip, but similar efficacy to the laparoscopic silastic band. However, it should be noted that other trial data indicate postpartum application of the titanium clip is inferior to partial salpingectomy.10 Complete bilateral salpingectomy, both in open and minimally invasive surgery, seems to be the most effective, but large scale prospective data and long-term followup have not yet been obtained to better describe risk of failure. Ultimately, surgical decision making around modality should be made in conjunction with each patient’s pregnancy risk tolerance and preferences. As there is no FDA approved mechanism for transcervical PC, this remains a research priority, particularly to meet the needs of patients for whom abdominal surgery is significantly risky, complex, or not preferred. Moving forward, as new techniques are introduced, postmarketing studies following patients over multiple years should be conducted, given that surgical failure can take years to present. Ultimately, PC remains a popular contraceptive option in the modern context and today’s clinician has a variety of reliable options to accomplish this.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Daniels K, Abma JC. Current contraceptive status among women aged 15–49: United States, 2017–2019. NCHS Data Brief. 2020;388:1–8.
2. Picard M, Duforestel T. Stérilisation tubaire par voie vaginale : à propos d’une série de 158 patientes de 2005 à 2021 [Vaginal tubal sterilization: about a series of 158 patients from 2005 to 2021]. Gynecol Obstet Fertil Senol. 2022;50(6):470–474. French. doi:10.1016/j.gofs.2022.01.006
3. Peterson HB, Xia Z, Hughes JM, Wilcox LS, Tylor LR, Trussell J. The risk of pregnancy after tubal sterilization: findings from the U.S. Collaborative Review of Sterilization. Am J Obstet Gynecol. 1996;174(4):1161–1168. doi:10.1016/s0002-9378(96)70658-0
4. Hoffman S, Schaffer H, Bradshaw C. Williams Gynecology. McGraw-Hill Education LLC; 2012.
5. Metz KGP. Failures Following Fimbriectomy. Fertil Steril. 1977;28(1):66–71. doi:10.1016/S0015-0282(16)42319-8
6. Fang NZ, Westhoff CL. Update on incidence of inpatient tubal ligation and long-acting reversible contraception in the United States. Am J Obstet Gynecol. 2022;227(3):477.e1–477.e7. doi:10.1016/j.ajog.2022.05.021
7. Dioun S, Huang Y, Melamed A, et al. Trends in the use of minimally invasive adnexal surgery in the United States. Obstet Gynecol. 2021;138(5):738–746. doi:10.1097/AOG.0000000000004577
8. Lawrie TA, Kulier R, Nardin JM. Techniques for the interruption of tubal patency for female sterilisation. Cochrane Database Syst Rev. 2016;2016(8):CD003034. doi:10.1002/14651858.CD003034.pub4
9. Yan JS, Hsu J, Yin CS. Comparative study of Filshie clip and Pomeroy method for postpartum sterilization. Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 1990;33(3):263–267. doi:10.1016/0020-7292(90)90012-a
10. Rodriguez MI, Seuc A, Sokal DC. Comparative efficacy of postpartum sterilisation with the titanium clip versus partial salpingectomy: a randomised controlled trial. BJOG Int J Obstet Gynaecol. 2013;120(1):108–112. doi:10.1111/j.1471-0528.2012.03482.x
11. Lau WY, Leow CK, Li AK. History of endoscopic and laparoscopic surgery. World J Surg. 1997;21(4):444–453. doi:10.1007/pl00012268
12. Brill AI. Bipolar electrosurgery: convention and innovation. Clin Obstet Gynecol. 2008;51(1):153–158. doi:10.1097/GRF.0b013e318161e7ee
13. Peterson HB, Xia Z, Wilcox LS, Tylor LR, Trussell J. Pregnancy after tubal sterilization with bipolar electrocoagulation. U.S. Collaborative review of sterilization working group. Obstet Gynecol. 1999;94(2):163–167. doi:10.1016/s0029-7844(99)00316-6
14. Malacova E, Kemp A, Hart R, Jama-Alol K, Preen DB. Long-term risk of ectopic pregnancy varies by method of tubal sterilization: a whole-population study. Fertil Steril. 2014;101(3):728–734. doi:10.1016/j.fertnstert.2013.11.127
15. Hulka JF, Fishburne JI, Mercer JP, Omran KF. Laparoscopic sterilization with a spring clip: a report of the first fifty cases. Am J Obstet Gynecol. 1973;116(5):715–718. doi:10.1016/S0002-9378(15)33141-0
16. Alexander AL, Strohl AE, Rieder S, Holl J, Barber EL; American College of Obstetricians and Gynecologists. Opportunistic salpingectomy as a strategy for epithelial ovarian cancer prevention. Obstet Gynecol. 2019;133(4):6. doi:10.1097/AOG.0000000000002990
17. Baltus T, Brown J, Molakatalla S, Kapurubandara S. Spontaneous pregnancy after total bilateral salpingectomy: a systematic review of literature. J Minim Invasive Gynecol. 2022;29(2):213–218. doi:10.1016/j.jmig.2021.09.713
18. SALpingectomy for STERilization (SALSTER). Tabular view - clinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/record/NCT03860805.
19. Varma R, Gupta JK. Predicting negligence in female sterilization failure using time interval to sterilization failure: analysis of 131 cases. Hum Reprod. 2007;22(9):2437–2443. doi:10.1093/humrep/dem188
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.