")
Back to Journals » Journal of Pain Research » Volume 14
Efficacy of Specified Manual Therapies in Combination with a Supervised Exercise Protocol for Managing Pain Intensity and Functional Disability in Patients with Knee Osteoarthritis
Authors Reza MK, Shaphe MA , Qasheesh M, Shah MN, Alghadir AH, Iqbal A
Received 5 October 2020
Accepted for publication 24 December 2020
Published 26 January 2021 Volume 2021:14 Pages 127—138
DOI https://doi.org/10.2147/JPR.S285297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Mohammad Kashif Reza,1 Mohammad Abu Shaphe,1 Mohammed Qasheesh,1 Mudasir Nazar Shah,1 Ahmad H Alghadir,2 Amir Iqbal2
1Physical Therapy Department, Jazan University, Jazan, Saudi Arabia; 2Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Amir Iqbal
Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh 11433, Saudi Arabia
Tel +966 1 4696010
Fax +966 1 4693589
Email [email protected]
Purpose: The current study aimed to determine the efficacy of specified manual therapies in combination with a supervised exercise protocol for managing pain intensity and functional disability in patients with knee osteoarthritis.
Methods: The study was based on a two-arm parallel-group randomized controlled trial design, including a total of 32 participants with knee osteoarthritis randomly divided into groups A and B. Group A received a supervised exercise protocol; however, group B received specified manual therapies in combination with a supervised exercise protocol. Pain and functional disability were measured with the numeric pain rating scale (NPRS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), respectively. Data were collected at baseline (pre-intervention), 2 weeks, and 4 weeks post-intervention. To evaluate the efficacy of specific manual therapies with supervised exercise compared to supervised exercise alone, an unpaired t-test and repeated measures ANOVA were used to analyze the data, keeping the level of significance at p< 0.05.
Results: A significant (p< 0.05) mean difference (∆MD) was found within group A and group B for both outcomes when we compared their baseline scores with 2-week (group A, NPRS: ∆MD=− 1.56 and WOMAC: ∆MD=14.94; group B, NPRS: ∆MD=2.06 and WOMAC: ∆MD=22.19) and 4-week post-intervention scores (group A, NPRS: ∆MD=0.62 and WOMAC: ∆MD=6.75; group B, NPRS: ∆MD=0.75 and WOMAC: ∆MD=11.12). In addition, significant mean differences (p< 0.05) reported for both outcomes when we compared their scores between groups A and B at 2 weeks (∆MD: NPRS=0.69; WOMAC=10.87) and 4 weeks post-intervention (∆MD: NPRS=0.31; WOMAC=8.00). Furthermore, a post hoc Scheffe analysis for the outcomes NPRS and WOMAC revealed the superiority of group B over group A.
Conclusion: The specified manual therapies, in combination with a supervised exercise protocol, were found to be more effective than a supervised exercise protocol alone for improving pain and functional disability in patients with knee osteoarthritis.
Keywords: specified manual therapy, strengthening exercise, stretching exercise, knee OA
Introduction
Osteoarthritis (OA) is a degenerative, complex, and common form of arthritis responsible for chronic disability among older adults worldwide and is associated with a high cost to the individual and society. The anticipated number of cases of OA will increase to 59.4 million (18.2% of the population) by 2020 in the United States alone.1 The prevalence of OA increases with age, especially in women over the age of 50.2,3 Osteoarthritis is a disorder involving movable joints characterized by cell stress and extracellular matrix degradation, initiated by micro- and macro-injury that activates maladaptive repair responses, including pro-inflammatory pathways of innate immunity. The disease manifests first as a molecular derangement (abnormal joint tissue metabolism) followed by anatomic, and/or physiologic derangements (characterized by cartilage degradation, bone remodeling, osteophyte formation, joint inflammation and loss of normal joint function), that can culminate in illness, as defined by Osteoarthritis Research Society International (OARSI).4 The disease most commonly affects the more movable joints, including the hand, hips, knees, and spine; however, it is not specific to large weight-bearing joints.2,5 The disease onset is gradual and usually begins after the age of 40.2,4 The specific causes of osteoarthritis are unknown, but are believed to be a result of both mechanical and molecular events in the affected joints. Other physiological changes, such as a reduction in quadriceps muscle strength and range of motion (ROM) in the sagittal plane, as well as the shortening of soft tissues around the joints, collectively yield the distinctive clinical features of OA, such as articular pain (worsening during weight-bearing activities), resting/morning joint stiffness, progressive decline in physical activities and increasing deformities/disabilities.6–8 The Kellgren–Lawrence grading system and the Ahlbäck classification for radiographic OA, including grade 2 (presence of osteophytes) and grade 3 (narrowing of joint space), have been widely used to diagnose knee OA for decades.9,10
Due to the idiopathic nature of the aetiology, symptomatic treatment has been offered to manage the symptoms rather than completely cure the disease. In recent years, an evidence-based approach has been applied to manage the OA, including the patient’s education, pharmacological and non-pharmacological management, and surgical interventions.11–13 Patient education includes a complete knowledge of OA, such as causes, symptoms, management, complications and the prognosis of the disease.11 Pharmacological management includes the use of non-steroidal anti-inflammatory drugs (NSAIDs), analgesics, and intra-articular injections.12 Non-pharmacological management is used as an adjunct to pharmacological management and includes weight loss programs, exercise, manual physiotherapy and occupational therapy interventions, such as the use of transcutaneous electrical nerve stimulation and interferential therapy for pain relief, optimal activities with the use of orthotic devices, exercises, patellar taping and manual techniques for restoring joint mobility, improving physical function and reducing physical disabilities.13–19 Moreover, patients’ participation in self-pain management, functional improvement, the prevention of disability and the progression of the disease is also required.18,20,21
The American college of radiology (ACR) considers exercise therapy as the backbone of OA treatment and recommended its adoption in the management of knee OA based on its effectiveness in reducing pain and physical impairments, and improving the functional status and physical fitness of people with knee OA.22–25 Previous studies reported that the high-velocity thrust technique and NSAIDs were equally effective in reducing knee pain.23 However, spinal manual therapy and home exercise with advice were found to be more effective than medications in reducing neck pain in the short term and long term.20,26 Therefore, structured exercise therapy and manual techniques could be considered as an adjunct or alternative to pharmaceutical management of OA.14,22,27–29
Recently, a systemic review study reported that manual orthopedic therapy provides a short-term reduction in pain intensity, as well as improvements in functional status and performance when compared with exercise therapy alone.19 In an experimental study, researchers reported that manual therapy (myofascial release technique) significantly reduced knee pain and improved functional outcomes (self-reported knee function) at the end of 2 weeks post-intervention in patients with knee OA.20 Moreover, a study reported that manual therapy applied by an experienced physiotherapist yielded greater functional improvements and slowed or avoided the need for surgical intervention compared to suboptimal ultrasonic therapy in patients with knee OA.30 A meta-analysis of randomized controlled trials reported that the add-on effects of manual mobilization along with exercise therapy were found to be moderately more effective in reducing pain intensity than strength training or exercise therapy alone.31 Likewise, in another study, researchers reported that the addition of manual therapy (in the form of booster sessions for over a year) to exercise therapy was found to be more effective than 12 consecutive exercise therapy sessions alone.29 Furthermore, in a previous study, manual therapy along with a supervised exercise protocol led to a significant reduction in joint stiffness, knee pain and improvements in the functional status of patients with knee OA in the short term and long term (1-year follow-up) compared to the placebo therapy (sub-therapeutic doses of ultrasound).32
To date, many studies have proven the effectiveness of manual therapy (including either mobilization or manipulation techniques) alone or/and in combination with other physical therapy exercises (including either stretching or strengthening protocols) in reducing pain and improving the functional status and physical performance of patients with knee OA. None of these studies examined the comparative add-on effects of a specified manual technique (with both mobilization and manipulation techniques) along with a supervised exercise program (with both stretching and strengthening exercises) in managing pain and functional outcomes in patients with knee OA. Therefore, this study aimed to evaluate the efficacy of specified manual therapies in combination with a supervised exercise protocol and a supervised exercise protocol alone for managing the pain intensity and functional disability of patients with knee osteoarthritis.
Patients and Methods
Participants
A total of forty-seven consecutive patients with discomfort due to knee pain, previously diagnosed as knee osteoarthritis (OA) by a consultant orthopedic surgeon based on ACR clinical classification criteria for knee OA, were screened for inclusion in this study from the physiotherapy outpatient department (OPD) of our university hospital.25 Thirty-two out of 56 patients who met the inclusion criteria were recruited and randomly allocated to group A or B. The inclusion criteria were as follows: male and female patients aged between 47 and 60 years;3 mild to moderate pain in one/both knees for three months; a pain intensity score between 2 and 6 on the numeric pain rating scale (NPRS);3 morning stiffness <30 minutes; self-reported crepitus during knee motion; exhibited a grade between 1 and 3 on the Kellgren–Lawrence radiographic grading scale for knee OA.10 However, patients were excluded from the study when the following criteria applied: a diagnosed case of post-traumatic knee stiffness (within 14 days of trauma); a history of bone infection and malignancy (osteomyelitis and tumor); neurological disorders (sciatica); and currently not taking/or will not take any pharmacological intervention such as anti-inflammatory medication, analgesics and calcium supplements during the study period; history of joint replacement/meniscal surgery/mechanical knee pain/infection of the knee joint; suffering from severe cardiopulmonary disease (chronic obstructive pulmonary disease); and non-cooperation in the study.
Study Design
This study was based on a two-arm parallel-group randomized controlled trial design. We used the online web address http://www.randomization.com to allocate the 32 patients into two groups. This study used the convenience method to collect the sample.
Ethical Consideration
The ethical approval for this study was obtained from the ethics sub-committee, King Saud University (file ID: RRC-2019-20), and the trial was registered on ClinicalTrials.gov Protocol Registration System (ClinicalTrials.gov ID: NCT04589858). The committee confirmed that the study preserved the human rights of the participants and followed the code of conduct of appropriate research ethics. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the study participants prior to study commencement.
Sample Size
Local software (GPower V3.1.9.4) was used for the calculation of sample size to ensure the enough power. The power analysis and test family applied were selected a priori: computer required sample size (given α=0.05, power=0.80, and effect size=0.82) and t-tests (matched pairs), respectively, using the data from a pilot study done on four participants. The effect size was obtained by calculating the mean and standard deviation differences (1.00±1.22) between the pre and post interventions scores of the outcome (NPRS). After obtaining an effect size (dz) of 0.82, a sample of 14 participants in each group was required (total sample=28) to ensure an actual power of 80%.
Outcome Measures
Outcomes were pain intensity and functional disability assessed by the numeric pain rating scale (NPRS), and the Western Ontario and McMaster Universities Arthritis Index (WOMAC), respectively. NPRS is an eleven-point scale, beginning at 0 and ending at 10. The NPRS is often used in clinical settings to assess pain intensity. The reliability of the NPRS is 0.92.33 WOMAC subscales (pain, stiffness, and physical function) were internally consistent with Cronbach’s alpha coefficients of 0.91, 0.81, and 0.84, respectively. Test–retest reliability was satisfactory, with ICCs of 0.86, 0.68, and 0.89, respectively.34 The universal goniometer used was a full goniometer (360̊) with one-axis joints with two-arms (one movable and one fixed arm). The intra-tester reliability was 0.997 in flexion and 0.98 in extension. The inter-tester reliability was 0.98 in flexion and 0.92 in extension.35 An assistant physiotherapist (assessor) who was blinded to the patient group allocation and specified the intervention protocol, and took the baseline, post-intervention, and follow-up measurements of all variables for all the participants in the presence of a specialist physiotherapist as to avoid any errors related to the tester and intratester reliability.
Procedures
This study was carried out using a two-arm parallel-group randomized controlled trial design and was comparative in nature. The sample used in this study was a sample of convenience: all the knee OA patients were referred to the physiotherapy outpatient department (O.P.D) of our university hospital for recruitment into this study after being diagnosed as having knee OA by an orthopedic surgeon. After identification of unilateral/bilateral knee OA on radiographs, along with meeting the inclusion criteria for the study, 32 participants were recruited to the study in total and were randomly divided into two groups. All the participants were blinded to their group allocation and recognized by a unique identification number written on their registration card. Each participant was asked to sign an informed consent form regarding their enrolment in the study. The study protocol is explained in a CONSORT flow diagram in Figure 1. All the participants were informed not to take any analgesics or other supplementary drugs until completion of the study. If any participants did take any of the aforementioned drugs, then they were told to inform us before the start of the intervention session.
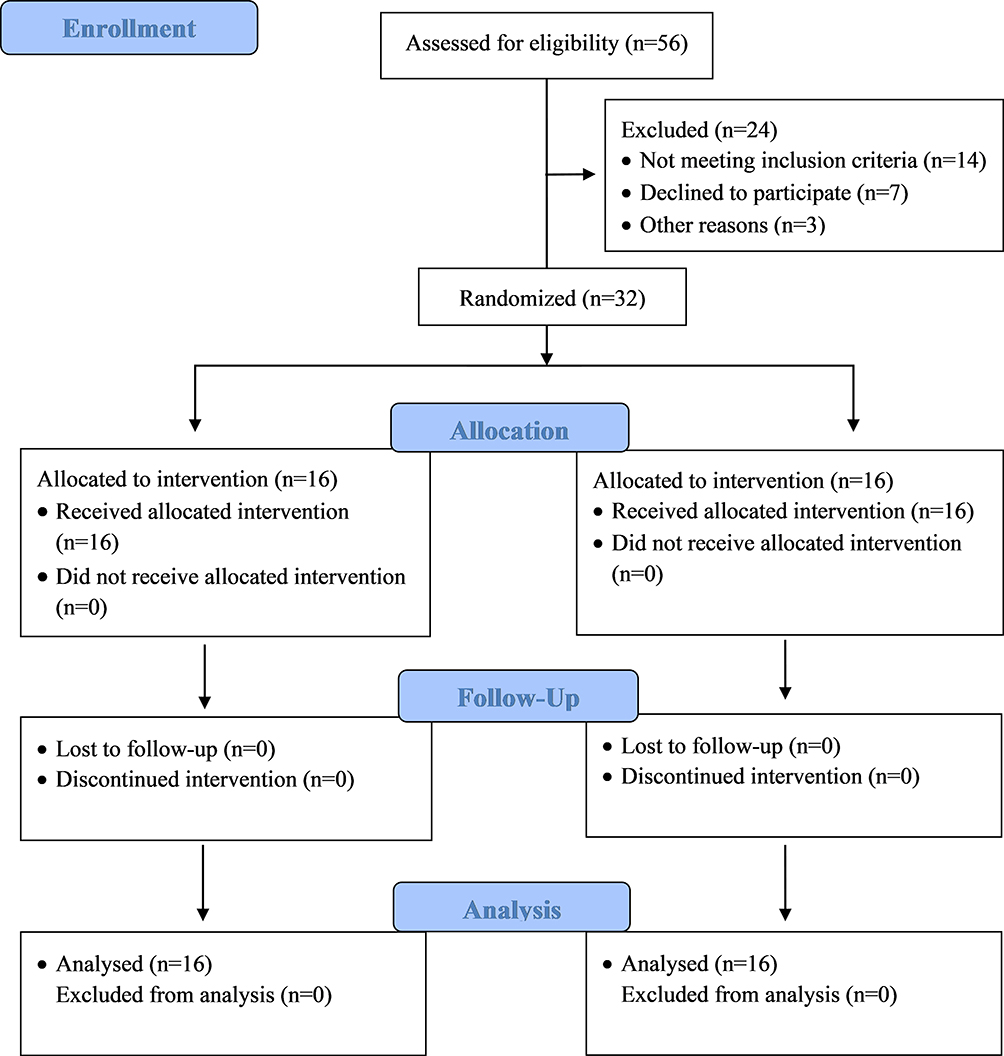 |
Figure 1 A CONSORT (2010) flow diagram of study procedure (enrollment, allocation, follow-up and analysis). |
The interventions given to groups A and B are shown in Table 1. One specialist physiotherapist delivered complete verbal commands, hands-on instructions, strengthening, and stretching exercises and the second specialist physiotherapist delivered the manual therapies only in order to ensure the maximum effects of the given interventions. In addition, a supporting handout containing detailed instructions and enough photographs of the exercises and therapies was delivered to all the participants by the same assistant physiotherapist (assessor) who assessed the outcome measures to make them more aware about their given interventions.
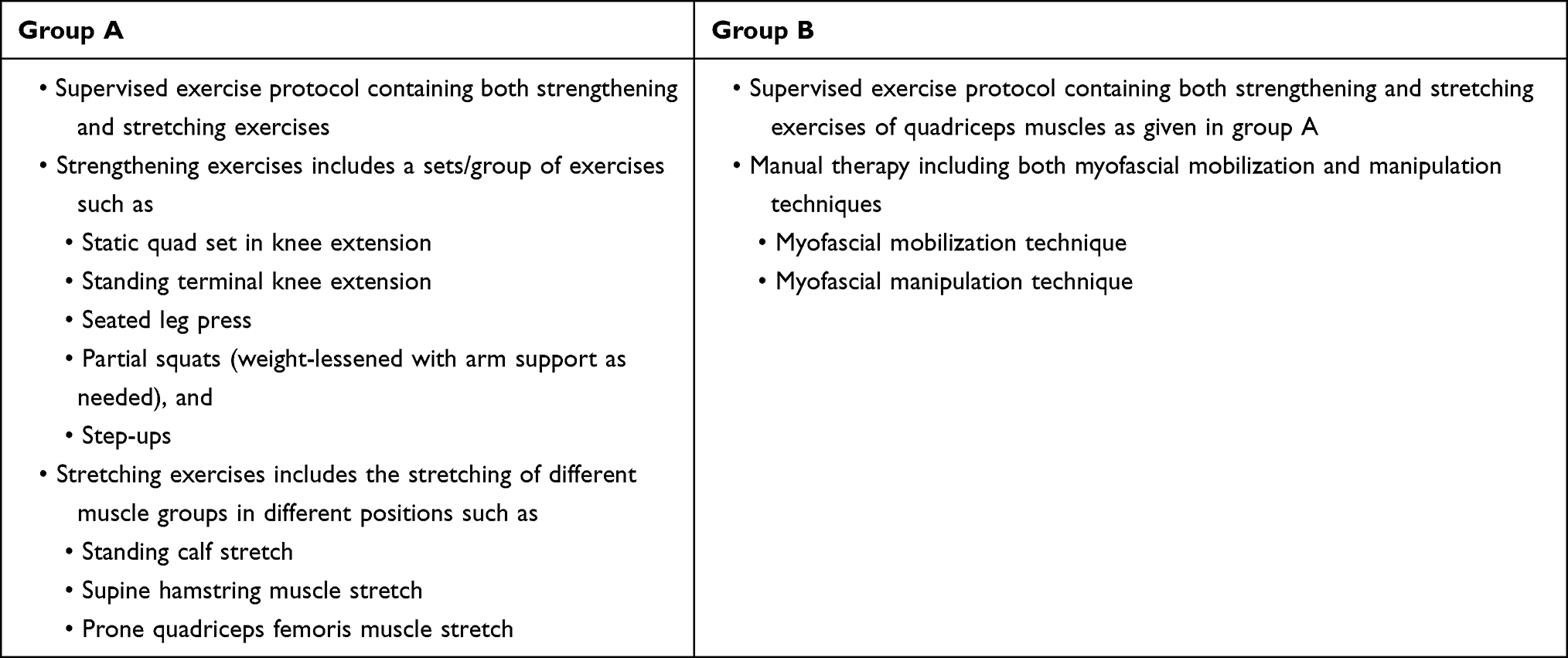 |
Table 1 Details of the Interventions Given to Both Group A and Group B (N=32) |
Each participant was evaluated for pain intensity and functional disability by using NPRS and WOMAC index outcome measures, respectively. Data were collected at baseline (pre-intervention), 2 weeks, and 4 weeks post-intervention by the same assessor who was kept blind to the study.
Interventions
Strengthening Exercises
Strengthening exercises included a set/group of exercises such as a static quad set in knee extension, standing terminal knee extension, seated leg press, partial squats (weight-lessened with arm support as needed), and step-ups.20,36,37
Static quad set in knee extension:36 This was performed by the participant laid in a supine position with the knee in full extension and ankle in dorsiflexion. The participant was asked to contract the quadriceps femoris muscle while pushing the knee down and maintaining the foot in full dorsiflexion. The hold time for this isometric contraction, the resting time between two repetitions, and the number of repetitions were set at 7 to 10 seconds, 10 seconds, and 10 times, respectively. The exercise was performed in 3 sessions on alternate days each week for two weeks.
Standing terminal knee extension exercise:38 This was performed by the participant in standing position with their knee slightly flexed at 30°C. Each participant stood with a cuff from a weighted pulley mechanism behind a slightly flexed knee. He/she was asked to contract the gluteal and quadriceps femoris muscles to fully straighten at the hip and knee joint. The hold time for the isometric contraction was 7 to 10 seconds, repeated 10 times, with resistance applied progressively and as tolerated by the participants. Participants were advised to follow a closed-chain progression from least to most challenging activities that they could completed successfully with minimal or no pain. Patients performed 3 sessions on alternate days each week for two weeks.
Seated leg press:37 This was performed by the participants when sitting on a chair with their back supported and arms resting on either side of the chair arms. Participants were asked to be seated while holding a resistive band in both hands. The patient places their foot against the band, then straightens their knee by pushing the foot down and forward by contracting the gluteal and quadriceps femoris muscles and holds the contraction for 7 to 10 seconds and then releases it and returns to the starting position to allow the muscle to relax. The same action was repeated for 30 bouts. Patients progressed to bands of increasing resistance and additional bouts as tolerated by the participants.
Partial squats (weight-lessened with arm support as needed):39 These were performed in a standing position with arm support as needed. The participants were asked to perform a partial squat, keeping the knees centered over the feet, then returning to a standing position by contracting the quadriceps femoris and gluteal muscles. They were instructed to hold each contraction for 7 to 10 seconds with hips and knees kept as straight as possible and then to repeat this for 30 bouts. This exercise was progressed further to full body weight without support and to add additional bouts.
Step-ups:40 The participants were instructed to stand up in front of a low step, place the foot of their ipsilateral leg on the step and bring their body over the foot in order to stand on the ipsilateral step. Patients used as little push-off assistance from the contralateral foot as possible, then stepped down with the contralateral foot. This was repeated slowly for 30s. This exercise was progressed further to increase the height of the step and to add additional bouts.
Stretching Exercises
Slow, sustained stretching was performed in different positions for different groups of muscles with a holding time 30 seconds and a gap of 1 minute between two repetitions. This was repeated 3 times per session on alternate days for 2 weeks. Stretching was performed for the calf muscle, hamstring muscle, and quadriceps femoris muscle in standing, supine, and prone positions, respectively.40–42
Standing calf stretch:40 This stretch was performed in a standing position for the calf muscle. The participant was instructed to stand in a walking–standing position with the foot of the leg to be stretched in complete contact with the ground behind the body and the other foot in front of the body, keeping the toes pointed straight forward. The participants used the support of wall and leaned forward until a moderate pull was perceived in their calf region.
Supine hamstring muscle stretch:41 This stretch was performed in a supine position, keeping the contralateral lower extremity straight and the ipsilateral hip and knee flexed to 90°. The thigh was stabilized, the lower leg grasped by the therapists’ hand, and the knee was straightened gradually until a moderate pull was perceived in the posterior thigh region.
Prone quadriceps femoris muscle stretch:42 This stretch was performed in a prone position, keeping the ipsilateral knee fully flexed. The therapist grasped the distal end of the thigh and lifted it upward progressively until a moderate pull was perceived in the anterior region of the thigh.
Specified Manual Therapy
Myofascial Mobilization Technique43
The participant laid in a supine position at the lateral edge of the mobilization couch adjacent to the therapist’s side. The specialist physiotherapist sat on the lateral side of the couch with the cephalad thigh under the leg of the involved limb and superior to the knee of the participant. The participant’s lower hamstring area rested on the therapist’s thigh with the knee able to rest at 90 degrees of flexion. The physiotherapist used a reinforced web contact to support the medial and lateral superior poles of the patella. The second position is recommended for therapists with a hyper-mobile thumb. The patient is then instructed to begin actively extending their knee through the pain-free range of motion while the therapist maintains contact at the patella. The force through the patella is applied in the plane at a tangent to the angle of the knee to avoid a compressive load. The patient extends the knee as far as possible in a pain-free manner from the initial starting position. The therapist maintains the contact at the patella during this movement. This was repeated 10 times per session on alternate days each week for 2 weeks.
Myofascial Manipulation Technique44
The participant laid in a supine position at the homolateral edge of the couch with the involved knee overhanging the edge of the couch. The physiotherapist stood on the homolateral side of the couch with the participant’s leg (at the level of the lower calf) gripped between their thighs to apply a distractive force in order to produce traction over the tibiofemoral joint. The therapist held the knee with his/her hands at either side. Both thumbs were placed on the tibial tuberosity and the fingers wrapped firmly around the knee to the distal end of the popliteal space so as to avoid too much digital pressure in the popliteal space. An impulse-type thrust was delivered, directed in the caudal direction to mobilize the joint to a near full extension position.
Statistical Analysis
Statistical analysis was carried out using the statistical software SPSS v.21 (IBM, Inc. USA). An unpaired t-test and repeated measures ANOVA were applied to describe the statistical differences between and within the groups, respectively. Furthermore, a post hoc Scheffe analysis was carried out to describe the pairwise comparison of outcomes within each group and this determined the superiority of one group over another group, if statistically existent. The level of significance (p-value) used for all analyses was 0.05. The results were found to be statistically significant at the 5% level. The statistician responsible for developing the test results was blinded to the group allocation.
Results
In total, 56 participants (30 males, 26 females) were screened for the study. Fourteen participants (9 males, 5 females) did not match the inclusion criteria; 5 participants (5 females) did not take the intervention after baseline measurements and discontinued their participation in the study; 3 participants (1 male, 2 female) said that they were not going to continue after day 2, while 2 participants (1 male, 1 female) left the study without providing any information and did not attend again.
Data from 32 participants were included for statistical analysis. The Shapiro–Wilk test for normality ensured the homogenous distribution of participants’ ages in both the groups. The mean and standard deviation for the demographic characteristics (age, sex) and baseline measurements for all the outcomes (NPRS, WOMAC) are described in Table 2. The mean scores for the outcomes of NPRS and WOMAC at baseline (pre-intervention), 2 weeks and 4 weeks post intervention were represented as NPRS1, NPRS2, and NPRS4 and WOMAC1, WOMAC2, and WOMAC4, respectively, to explain the results in the text as well as in the Tables 3 and 4.
 |
Table 2 Baseline Measurements (Mean±SD) for All the Variables [N=32] Using Unpaired t-Test |
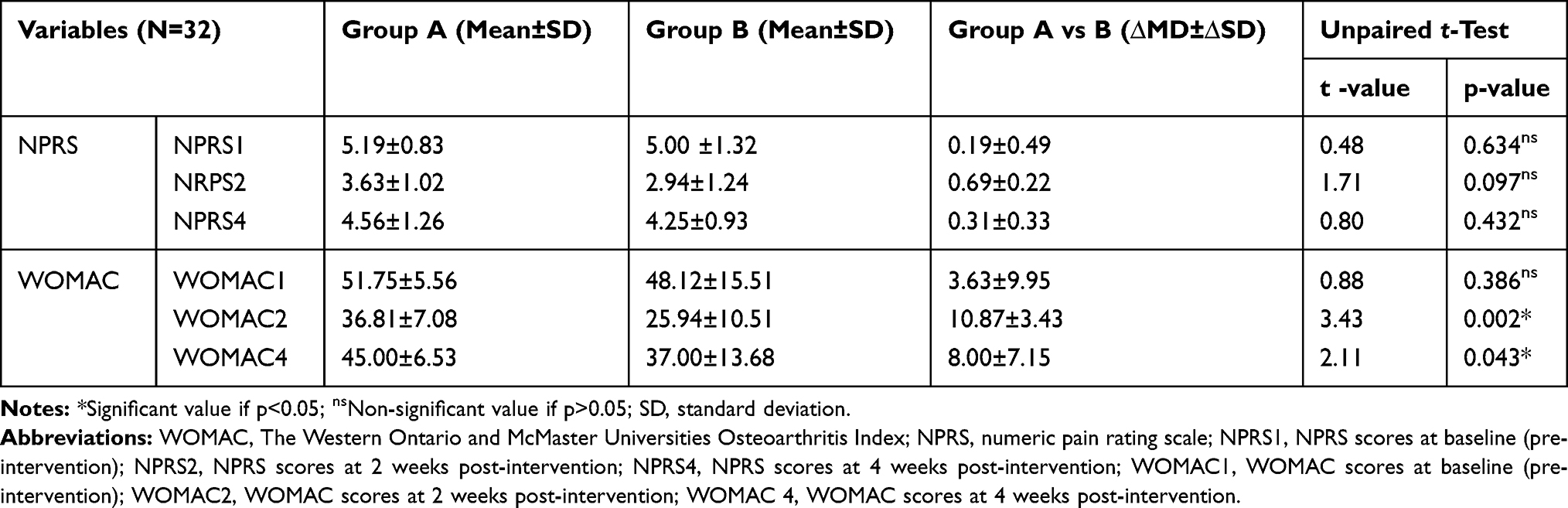 |
Table 3 Comparison (Mean±SD) of the Variables (WOMAC & NPRS) Between the Groups at Different Time-Intervals Using Unpaired t-Test (N=32) |
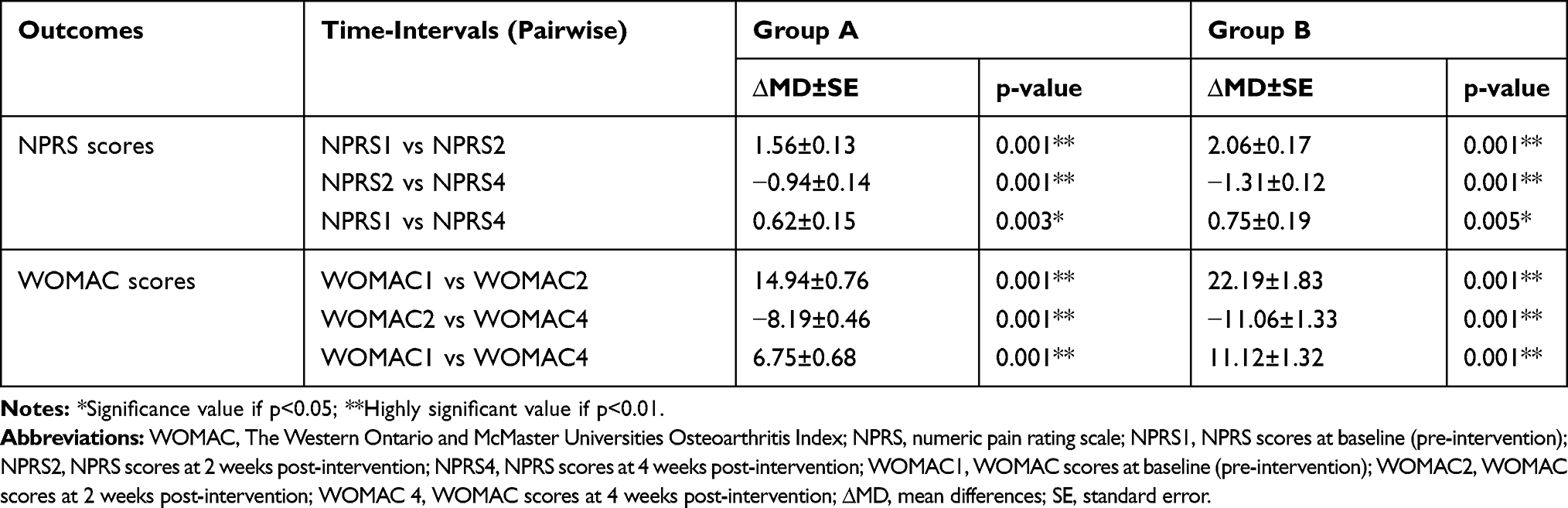 |
Table 4 Pairwise Comparisons of Mean Differences (∆MD) for the Outcomes NPRS and WOMAC Within the Group Using Repeated Measures ANOVA (N=32) |
Comparison Between Groups
When we compared the magnitude of the mean differences (∆MD) between groups A and B, the unpaired t-test revealed an insignificant mean difference for the outcome of the NPRS for the 2-week (∆MD=0.69; t=1.71; p=0.097) and 4-week post-intervention scores (∆MD=0.31; t=0.80; p=0.432). However, a significant mean difference was found between groups A and B for the WOMAC score outcomes at 2 weeks (∆MD=10.87; t=3.43; p=0.002) and 4 weeks post-intervention (∆MD=8.00; t=2.11; p=0.043), as described in Table 3.
Comparison Within Groups
Repeated measures ANOVA revealed a significant improvement for the outcomes within group A (NPRS: F=8.18 and p<0.05; WOMAC: F=18.99 and p<0.05) and group B (NPRS: F=11.18 and p<0.05; WOMAC: F=9.62 and p<0.05). A pairwise comparison of outcomes within group A revealed statistically significant mean differences when we compared the scores at 2 weeks (NPRS2-NPRS0: ∆MD=−1.56 and p=0.001; WOMAC2-WOMAC0: ∆MD=−14.94 and p=0.001) and 4 weeks post-intervention (NPRS4-NPRS0: ∆MD=−0.62 and p=0.003; WOMAC4-WOMAC0: ∆MD=−6.75 and p=0.001) with the baseline scores, and the scores at 4 weeks with the scores at 2 weeks post-intervention (NPRS: ∆MD=0.94 and p=0.001; WOMAC: ∆MD=8.19 and p=0.001). Similarly, in group B, statistically significant mean differences were found when we compared the scores at 2 weeks (NPRS2-NPRS0: ∆MD=−2.06 and p=0.001) and 4 weeks post-intervention (NPRS4-NPRS0: ∆MD=−0.75 and p=0.005; WOMAC4-WOMAC0: ∆MD=−11.12 and p=0.001) with the baseline scores, and the scores at 4 weeks with the scores at 2 weeks post-intervention (NPRS: ∆MD=1.31 and p=0.001; WOMAC: ∆MD=11.06 and p=0.001). Furthermore, the post hoc Scheffe analysis revealed the superiority of group B over group A, achieving a greater effect on the outcomes of the NPRS and WOMAC, as described in Table 4.
Discussion
The study aimed to evaluate the efficacy of specified manual therapies in combination with a supervised exercise protocol in patients with knee OA. Among 32 selected subjects, 19 males and 13 females were included in the study. The selected outcomes were the NPRS and WOMAC indexes. The data obtained were analyzed by repeated measures ANOVA and an unpaired t-test. The results showed that there were significant improvements for the outcomes of NPRS and WOMAC in both the groups.
Significant mean differences were seen in the outcome measures. Both outcomes were decreased maximally when patients received specified manual therapy in addition to a supervised exercise protocol, as compared to the supervised exercised protocol only. Both the groups received their stipulated intervention protocols in 3 sessions on alternate days per week for two weeks. However, the follow-up measurements were taken at 4 weeks from the commencement of the study. There were significant differences revealed after two weeks of receiving the stipulated intervention for each group; moreover, at retention/follow-up 4 weeks post-intervention, there was also a significant difference found for each group. Overall, the magnitude of the mean differences within group B showed more improvement than group A. Although the mean difference scores were found to be significant when we compared the scores at 4 weeks with those collected 2 weeks post-intervention, the mean differences between follow up and 2 weeks post-intervention were found to be less significant than the mean differences obtained when we compared the scores at 2 weeks post-intervention with the baseline scores. This showed that the effect of intervention was retained significantly for the next 2 weeks (until 4 weeks post-intervention), even after the removal of the intervention; however, this decreased gradually over time. This means that the retention effect of the intervention was found to be transient rather than permanent until 4 weeks post-intervention. Moreover, after more than 2 weeks, the retention effect might be insignificant and changes in outcomes might have been reversed. Therefore, future studies are required to increase the duration of the study intervention in order to achieve a permanent or longer-lasting effect.
The difference shown in the scores of the WOMAC index and the NPRS in group B are because, during soft tissue manipulation and slow active stretching, the stimulation of Golgi receptors took place, which lower the firing rate of specified alpha motor neurons, leading to a decrease in the tone of those tissues.32,45 When passive stretching is applied to the muscles and their fascia, a resultant elastic elongation of the muscle fibers takes pace simultaneously. However, this process differs from the active contraction of the muscles, where the function of the Golgi tendon organs is to supply feedback information about the changes that take place within the dynamic forces during muscle contraction.46
Receptors, including Ruffini’s endings and Ruffini’s corpuscles, are more commonly distributed at anterior and posterior ligaments, and capsules around the knee joint. Ruffini’s endings and Ruffini’s corpuscles are responsible for being receptive against tangential forces and lateral stretch, and lowering the activity of the sympathetic nervous system (CNS), respectively.47 This is the reason why slow and deep soft tissue manipulation and mobilization techniques are used on the local tissues and organs. However, Pacinian bodies frequently accumulate at the lateral and medial sides of the ligaments and capsular structures around the knee joint.48
It is possible that the central nervous system (CNS) is triggered by Ruffini’s endings through manual touch (manual therapy) and that this causes changes in the tones of a few motor neuron units present in the muscular tissues under the hand.47 The interstitial receptors and Ruffini’s mechanoreceptors become stimulated via slow or steady deep manual pressure and this increases the vagal activity, which brings about further changes in relation to local fluid dynamics, tissue metabolism and global muscle relaxation, leading to a more peaceful mind, and less emotional arousal.18,47
Previously, a randomized controlled trial study reported that a short-term manual therapy protocol is significantly effective in reducing knee pain and improving self-reported knee function among patients with knee OA immediately after 2 weeks post-intervention.20,49
In another study, researchers evaluated the effect of a moderate exercise program in combination with a modest dietary weight loss program among obese and overweight older adults with knee OA and found that the combination of exercise and a dietary weight loss program is moderately more effective in improving self-reported measures of knee function and pain and performance measures of mobility when compared with either of them (exercise or dietary weight loss) alone.50
Moreover, another study conducted a randomized clinical trial to find out the efficacy of moderate exercise on glycosaminoglycan (GAG) concentration in knee cartilage among patients at risk of knee OA over a period of 4 months and found that a supervised moderate exercise protocol significantly improved the GAG concentration in knee cartilage, while also improving in knee pain and function.28 Thus, their study (and others) indicated that a supervised, modest exercise protocol may contribute significantly in the prevention of disease in patients at risk of developing knee OA.23 These exercises effectively increase the GAG concentration in the knee cartilage, which improves the viscoelastic property of the cartilage (collagen network) in order to protect the knee from uneven compressive forces. However, a low concentration of GAG in the articular cartilage matrix, due to articular cartilage disease, deteriorates the viscoelastic property of the collagen network of the articular cartilage and leads to the progressive disintegration of the collagen molecules, collagen loss, and the subsequent development of OA.23,26,28,51
The study was limited due to the availability of the intervention protocols. We could not carry out the interventions for a long period, such as 4 to 8 weeks, and therefore could not observe the retention effects for a long-term follow-up. Future research is required to create a long-term intervention plan so as to discover the long-term effects as well as the long-term retention effects of the interventions.
Conclusion
The specified manual therapy, including myofascial mobilization and manipulation techniques in combination with a supervised exercise protocol, was found to be more effective than a supervised exercise protocol including strengthening and stretching maneuvers alone for improving the pain intensity and functional status of patients with knee osteoarthritis. However, there was no retention effect for the intervention protocols observed after the 4-week follow-up. Therefore, future studies are suggested in order to elucidate the retention effects of the intervention protocols.
Data Sharing Statement
Data from the study will be available upon reasonable request.
Acknowledgment
The authors are grateful to the Deanship of Scientific Research, King Saud University, for funding this research through the Vice Deanship of Scientific Research Chair.
Author Contributions
All authors have contributed to preparing the manuscript according to the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. All authors contributed to the conception of the research design, data collection, data analysis, manuscript formatting, and drafting and critically revising the paper. All authors have agreed on the journal to which the article will be submitted and gave final approval of the version to be published and agree to be held responsible for all facets of the work.
Funding
This study was funded through the Deanship of Scientific Research, King Saud University.
Disclosure
The authors declare no conflicts of interest related to this study.
References
1. Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheumatol. 1998;41(5):778–799. doi:10.1002/1529-0131(199805)41:5<778::AID-ART4>3.0.CO;2-V
2. Control CfD. Prevention osteoarthritis; 2014. Available from: http:/www.cdcgov/arthritis/basics/osteoarthritoshtm.
3. Damen J, van Rijn RM, Emans PJ, et al. Prevalence and development of hip and knee osteoarthritis according to American College of Rheumatology criteria in the CHECK cohort. Arthritis Res Ther. 2019;21(1):4. doi:10.1186/s13075-018-1785-7
4. Kraus VB, Blanco FJ, Englund M, Karsdal MA, Lohmander LS. Call for standardized definitions of osteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthr Cartil. 2015;23(8):1233–1241. doi:10.1016/j.joca.2015.03.036
5. Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26(3):355–369. doi:10.1016/j.cger.2010.03.001
6. Zeni JA, Rudolph K, Higginson JS. Alterations in quadriceps and hamstrings coordination in persons with medial compartment knee osteoarthritis. J Electromyogr Kinesiol. 2010;20(1):148–154. doi:10.1016/j.jelekin.2008.12.003
7. Warden SJ, Hinman RS, Watson MA
8. Toivanen AT, Heliövaara M, Impivaara O, et al. Obesity, physically demanding work and traumatic knee injury are major risk factors for knee osteoarthritis—a population-based study with a follow-up of 22 years. Rheumatology. 2010;49(2):308–314. doi:10.1093/rheumatology/kep388
9. Petersson IF, Boegård T, Saxne T, Silman AJ, Svensson B. Radiographic osteoarthritis of the knee classified by the Ahlbäck and Kellgren & Lawrence systems for the tibiofemoral joint in people aged 35–54 years with chronic knee pain. Ann Rheum Dis. 1997;56(8):493–496. doi:10.1136/ard.56.8.493
10. Kellgren J, Lawrence J. The Epidemiology of Chronic Rheumatism. Atlas of Standard Radiographs. Vol. 2. Oxford: Blackwell Scientific; 1963.
11. Nunez M, Nunez E, Segur J, et al. The effect of an educational program to improve health-related quality of life in patients with osteoarthritis on waiting list for total knee replacement: a randomized study. Osteoarthr Cartil. 2006;14(3):279–285. doi:10.1016/j.joca.2005.10.002
12. Ondresik M, Azevedo Maia FR, da Silva Morais A, et al. Management of knee osteoarthritis. Current status and future trends. Biotechnol Bioeng. 2017;114(4):717–739.
13. Fernandes L, Hagen KB, Bijlsma JW, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72(7):1125–1135. doi:10.1136/annrheumdis-2012-202745
14. French HP, Cusack T, Brennan A, et al. Exercise and manual physiotherapy arthritis research trial (EMPART): a multicentre randomised controlled trial. BMC Musculoskelet Disord. 2009;10(1):1–12. doi:10.1186/1471-2474-10-9
15. Naka A, Keilani M, Loefler S, Crevenna R. Does transcutaneous electrical nerve stimulation (TENS) have a clinically relevant analgesic effect on different pain conditions? A literature review. Eur J Transl Myol. 2013;23(3):95–104. doi:10.4081/bam.2013.3.95
16. Ettinger WH, Burns R, Messier SP, et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis: the fitness arthritis and seniors trial (FAST). JAMA. 1997;277(1):25–31. doi:10.1001/jama.1997.03540250033028
17. Roddy E, Zhang W, Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann Rheum Dis. 2005;64(4):544–548. doi:10.1136/ard.2004.028746
18. Abbott JH, Robertson MC, McKenzie JE, et al. Exercise therapy, manual therapy, or both, for osteoarthritis of the hip or knee: a factorial randomised controlled trial protocol. Trials. 2009;10(1):11. doi:10.1186/1745-6215-10-11
19. Anwer S, Alghadir A, Zafar H, Brismée J-M. Effects of orthopaedic manual therapy in knee osteoarthritis: a systematic review and meta-analysis. Physiotherapy. 2018;104(3):264–276. doi:10.1016/j.physio.2018.05.003
20. Pollard H, Ward G, Hoskins W, Hardy K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: a randomised controlled trial. J Can Chiropr Assoc. 2008;52(4):229.
21. Gilbert AL, Lee J, Ehrlich-Jones L, et al. A randomized trial of a motivational interviewing intervention to increase lifestyle physical activity and improve self-reported function in adults with arthritis. In Seminars in Arthritis and Rheumatism. Elsevier; 2018:732–740.
22. Altınbilek T, Murat S, Yumuşakhuylu Y, İçağasıoğlu A. Osteopathic manipulative treatment improves function and relieves pain in knee osteoarthritis: a single-blind, randomized-controlled trial. Turk J Ph Med Rehab. 2018;64(2):114. doi:10.5606/tftrd.2018.1384
23. Videman T, Eronen I, Friman C. Glycosaminoglycan metabolism in experimental osteoarthritis caused by immobilization: the effects of different periods of immobilization and follow-up. Acta Orthop Scand. 1981;52(1):11–21. doi:10.3109/17453678108991751
24. Thomas K. Home based exercise programme for knee pain and knee osteoarthritis; randomised controlled trial. Clin J Sport Med. 2003;13(6):388–389. doi:10.1097/00042752-200311000-00010
25. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220–233. doi:10.1002/art.41142
26. Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH. Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain: a randomized trial. Ann Intern Med. 2012;156(1_Part_1):1–10. doi:10.7326/0003-4819-156-1-201201030-00002
27. Marks R, Penton L. Are foot orthotics efficacious for treating painful medial compartment knee osteoarthritis? A review of the literature. Int J Clin Pract. 2004;58(1):49–57. doi:10.1111/j.1368-5031.2004.0084.x
28. Roos EM, Dahlberg L. Positive effects of moderate exercise on glycosaminoglycan content in knee cartilage: a four‐month, randomized, controlled trial in patients at risk of osteoarthritis. Arthritis Rheum. 2005;52(11):3507–3514. doi:10.1002/art.21415
29. Abbott JH, Chapple CM, Fitzgerald GK, et al. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: a randomized clinical trial. J Orthop Sports Phys Ther. 2015;45(12):975–983. doi:10.2519/jospt.2015.6015
30. Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2000;132(3):173–181. doi:10.7326/0003-4819-132-3-200002010-00002
31. Jansen MJ, Viechtbauer W, Lenssen AF, Hendriks EJ, de Bie RA. Strength training alone, exercise therapy alone, and exercise therapy with passive manual mobilisation each reduce pain and disability in people with knee osteoarthritis: a systematic review. J Physiother. 2011;57(1):11–20. doi:10.1016/S1836-9553(11)70002-9
32. Deyle GD, Allison SC, Matekel RL, et al. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys Ther. 2005;85(12):1301–1317. doi:10.1093/ptj/85.12.1301
33. Stratford PW, Spadoni G. Feature articles-the reliability, consistency, and clinical application of a numeric pain rating scale. Physiother Can. 2001;53(2):88–91.
34. Salaffi F, Leardini G, Canesi B, et al. Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) osteoarthritis index in Italian patients with osteoarthritis of the knee. Osteoarthr Cartil. 2003;11(8):551–560. doi:10.1016/S1063-4584(03)00089-X
35. Brosseau L, Balmer S, Tousignant M, et al. Intra-and intertester reliability and criterion validity of the parallelogram and universal goniometers for measuring maximum active knee flexion and extension of patients with knee restrictions. Arch Phys Med Rehabil. 2001;82(3):396–402. doi:10.1053/apmr.2001.19250
36. Shveta K, Quddas N, Vequar Z. Effect of ankle position on isometric quadriceps strengthening in osteoarthritis of knee joint. Physiother Occup Ther. 71.
37. Vincent KR, Vincent HK. Resistance exercise for knee osteoarthritis. PM&R. 2012;4(5):S45–S52. doi:10.1016/j.pmrj.2012.01.019
38. Croce R, Miller J, St Pierre P. Effect of ankle position fixation on peak torque and electromyographic activity of the knee flexors and extensors. Electromyogr Clin Neurophysiol. 2000;40(6):365.
39. Foroughi N, Smith RM, Lange AK, Baker MK, Singh MAF, Vanwanseele B. Lower limb muscle strengthening does not change frontal plane moments in women with knee osteoarthritis: a randomized controlled trial. Clin Biomech. 2011;26(2):167–174. doi:10.1016/j.clinbiomech.2010.08.011
40. Farr JN, Going SB, McKnight PE, Kasle S, Cussler EC, Cornett M. Progressive resistance training improves overall physical activity levels in patients with early osteoarthritis of the knee: a randomized controlled trial. Phys Ther. 2010;90(3):356–366. doi:10.2522/ptj.20090041
41. Reid DA, McNair PJ. Effects of an acute hamstring stretch in people with and without osteoarthritis of the knee. Physiotherapy. 2010;96(1):14–21. doi:10.1016/j.physio.2009.06.010
42. Weng MC, Lee CL, Chen CH, et al. Effects of different stretching techniques on the outcomes of isokinetic exercise in patients with knee osteoarthritis. Kaohsiung J Med Sci. 2009;25(6):306–315. doi:10.1016/S1607-551X(09)70521-2
43. Arroyo-Morales M, Olea N, Martinez M, Moreno-Lorenzo C, Daz-Rodrguez L, Hidalgo-Lozano A. Effects of myofascial release after high-intensity exercise: a randomized clinical trial. J Manipulative Physiol Ther. 2008;31(3):217–223. doi:10.1016/j.jmpt.2008.02.009
44. Tobis JS, Hoehler F. Musculoskeletal manipulation in the treatment of low back pain. Bull N Y Acad Med. 1983;59(7):660.
45. Knoop J, Steultjens M, Van der Leeden M, et al. Proprioception in knee osteoarthritis: a narrative review. Osteoarthr Cartil. 2011;19(4):381–388. doi:10.1016/j.joca.2011.01.003
46. Stuart D, Goslow G, Mosher C, Reinking R. Stretch responsiveness of Golgi tendon organs. Exp Brain Res. 1970;10(5):463–476. doi:10.1007/BF00234263
47. Hassan B, Mockett S, Doherty M. Influence of elastic bandage on knee pain, proprioception, and postural sway in subjects with knee osteoarthritis. Ann Rheum Dis. 2002;61(1):24–28. doi:10.1136/ard.61.1.24
48. Ralphs J, Benjamin M. The joint capsule: structure, composition, ageing and disease. J Anat. 1994;184(Pt 3):503.
49. O’Reilly SC, Muir KR, Doherty M. Effectiveness of home exercise on pain and disability from osteoarthritis of the knee: a randomised controlled trial. Ann Rheum Dis. 1999;58(1):15–19. doi:10.1136/ard.58.1.15
50. Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the arthritis, diet, and activity promotion trial. Arthritis Rheum. 2004;50(5):1501–1510. doi:10.1002/art.20256
51. Yucesoy B, Charles LE, Baker B, Burchfiel CM. Occupational and genetic risk factors for osteoarthritis: a review. Work. 2015;50(2):261–273. doi:10.3233/WOR-131739
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.