")
Back to Journals » Journal of Blood Medicine » Volume 12
Efficacy of rFIXFc versus rIX-FP for the Treatment of Patients with Hemophilia B: Matching-Adjusted Indirect Comparison of B-LONG and PROLONG-9FP Trials
Authors Astermark J, Wojciechowski P , Aballéa S, Hakimi Z, Nazir J, Klamroth R
Received 1 April 2021
Accepted for publication 22 June 2021
Published 14 July 2021 Volume 2021:12 Pages 613—621
DOI https://doi.org/10.2147/JBM.S312885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Jan Astermark,1 Piotr Wojciechowski,2 Samuel Aballéa,3 Zalmai Hakimi,4 Jameel Nazir,4 Robert Klamroth5
1Department of Translational Medicine, Lund University, and Department of Hematology, Oncology and Radiation Physics, Skåne University Hospital, Malmö, Sweden; 2Creativ-Ceutical, Krakow, Poland; 3Creativ-Ceutical, Rotterdam, the Netherlands; 4Swedish Orphan Biovitrum AB, Stockholm, Sweden; 5Department of Internal Medicine, Hemophilia Treatment Centre, Vivantes Klinikum im Friedrichshain, Berlin, Germany
Correspondence: Robert Klamroth Email [email protected]
Purpose: In patients with hemophilia B, treatment with extended half-life (EHL) recombinant factor IX allows for longer dosing intervals while providing equal or superior bleeding protection compared with standard half-life products. This enables flexible, individualized treatment schedules, which reduce the burden of prophylaxis and improve patient outcomes. This analysis compared the efficacy of recombinant factor IX Fc fusion protein (rFIXFc) and recombinant factor IX albumin fusion protein (rIX-FP), two EHL therapies approved for prophylaxis and treatment of bleeding in hemophilia B.
Patients and Methods: Matching-adjusted indirect treatment comparison (MAIC) was used to adjust the between-treatment differences in baseline characteristics. Individual patient data for rFIXFc (B-LONG) were matched to aggregated data for rIX-FP (PROLONG-9FP) followed by statistical comparison for estimated annualized bleeding rate (ABR) using a Poisson regression model with adjustment for over dispersion. Data were analyzed according to treatment regimen prior to study entry: prior prophylaxis (rFIXFc, n=48; rIX-FP, n=40) or prior episodic treatment (n=43 and n=19, respectively). Relative treatment effects are presented as incidence rate ratios (IRR) with 95% confidence intervals (CI).
Results: After adjustment for baseline characteristics, estimated ABR observed for rFIXFc and rIX-FP was not significantly different in patients on prior prophylaxis (1.87 versus 1.58; IRR 1.18, 95% CI 0.67– 2.10) or prior episodic (2.25 versus 2.22; IRR 1.01 95% CI 0.40– 2.57) regimens.
Conclusion: This MAIC analysis shows that the estimated ABR for rFIXFc-treated patients from B-LONG was similar to that of rIX-FP-treated patients from PROLONG-9FP and, therefore, indicates that the two EHL therapies provide similar efficacy when used as prophylaxis for patients with hemophilia B. Trough levels differ between the two products (1– 3% [targeted] versus 20% [observed], respectively), suggesting that trough level is not a surrogate indicator when ABR is used as a criterion for clinical efficacy when comparing these FIX products in hemophilia B.
Keywords: annualized bleeding rate, comparative effectiveness research, factor IX deficiency, factor IX Fc fusion protein, rIX-FP fusion protein, treatment outcome
Introduction
Routine prophylaxis is the optimal standard of care for the management of patients with severe hemophilia B. Prophylaxis with recombinant factor IX (rFIX), especially when initiated early in life, has been shown to result in favorable clinical outcomes.1 Compared with on-demand therapy, regular prophylaxis provides a consistent decrease in both total bleeds and hemarthrosis (joint bleeds), reducing joint deterioration (arthropathy) and consequently improving patients’ quality of life.1 Despite these benefits, the relatively short half-life of standard rFIX products typically necessitates frequent intravenous dosing, at least twice weekly for severe hemophilia B, which represents a substantial burden to patients and their caregivers and families.2 Extended half-life (EHL) rFIX products provide a mean half-life extension 3–5 times that of standard products, which allows for longer dosing intervals while providing equal or superior bleeding protection to standard care.2 This enables the use of flexible treatment schedules to meet individual patient needs, decreases the burden of prophylaxis, and potentially further improves patient outcomes.3
The aim of treating hemophilia is to prevent joint bleeds and, ultimately, arthropathy.4 In hemophilia B, a trough level that prevents all bleeding has not been established and is likely to vary from patient to patient based on a number of factors, including joint status and age.5 Correlation between time spent under target trough levels and bleed rates, including spontaneous, traumatic and joint bleeds, has been demonstrated in patients with severe hemophilia B treated with recombinant FIXFc fusion protein (rFIXFc); as trough level increased, the predicted bleed rate reduced and the predicted probability of being bleed-free improved.6 However, other contributors to the variation in hemostatic and clinical outcomes and response to treatment should be considered when determining the most appropriate prophylaxis regimen,7 including the pharmacokinetic (PK) characteristics of the replacement factor and the patient’s individual PK profile.3 Ideally, the regimen should be individualized, taking the patient’s lifestyle into account, in order to reduce the known heterogeneity in bleeding patterns.3 Furthermore, it is important to remember that, as FIX can enter the extravascular space, trough levels may not reflect FIX tissue levels and, consequently, FIX bleeding prevention ability.8
rFIXFc is an EHL replacement therapy indicated for the treatment and prophylaxis of bleeding episodes, including perioperative management of bleeding, in patients with hemophilia B of all ages.9,10 Approval was based on two Phase 3 studies assessing the efficacy and safety of rFIXFc in previously treated pediatric (<12 years; Kids B-LONG)11 or adolescent/adult (≥12 years; B-LONG)12 patients with hemophilia B.
In both Kids B-LONG and B-LONG, rFIXFc prophylaxis, adjusted to maintain a trough level of 1–3 IU/dL, resulted in low annualized bleeding rates (ABRs).11,12 These results were confirmed in the long-term extension study (B-YOND); in the majority of patients, low ABRs were maintained and extended dosing intervals were sustained for up to 5 years, with a cumulative duration up to 6.5 years.13 Furthermore, a post hoc interim analysis of data from patients (≥12 years) who received rFIXFc prophylaxis with a ≥14-day dosing interval at any time during B-LONG or B-YOND showed that most patients remained well controlled, with ABRs consistent with those observed in the overall study population.14 Therefore, a dosing interval of ≥14 days is an option for some patients,10 offering a broader flexibility of dosing interval and further reducing treatment burden for patients while maintaining bleed protection.
Recombinant FIX albumin fusion protein (rIX-FP) is also indicated for the treatment and prophylaxis of bleeding episodes, including perioperative management of bleeding, in patients of all ages with hemophilia B.15,16 Prophylaxis with rIX-FP has been shown to be effective for bleed prevention and treatment in both pediatric and adolescent/adult patients with hemophilia B, with weekly dosing intervals in children and up to 14-day dosing in adolescents/adults (PROLONG-9FP).17,18 These results were confirmed in long-term extension studies, which also showed that adequate bleed protection could be achieved with extended dosing intervals of 10 or 14 days and 21 days in selected pediatric and adolescent/adult patients, respectively.19,20
Both rFIXFc and rIX-FP have been shown to be effective for the prevention and treatment of bleeds in patients with hemophilia. However, there are no direct comparative studies and in the absence of head-to-head trials an indirect comparison can be made using established methods, such as network meta-analysis21 or matching-adjusted indirect comparison (MAIC).22 MAIC is a widely used, validated method for the comparison of outcomes when there is no common comparator or the comparative studies are not sufficiently homogenous. MAIC matches patient-level data from clinical trials of one treatment with published aggregate data from clinical trials of another treatment, thus reducing observed differences between the trials and providing a balanced patient population for comparison.22 The aim of this analysis was to apply MAIC to compare the efficacy of rFIXFc and rIXFP, two EHL therapies approved for prophylactic treatment of patients with hemophilia B.
Methods
Data Sources and Sample Selection
Source data for the MAIC analysis were extracted from the pivotal phase 3 trials (B-LONG for rFIXFc and PROLONG-9FP for rIX-FP), which provided efficacy and safety data for market authorization. Comparisons were based on the approved dosing regimens for each product (Table 1). The study design and results of these trials have been described in detail elsewhere.12,17 Briefly, both were non-randomized, open-label studies in previously treated male adolescent/adult patients (≥12 years) with severe hemophilia B. In B-LONG, patients (N=119) were treated with one of four rFIXFc regimens: weekly dose-adjusted prophylaxis (group 1: starting at 50 IU/kg; n=63), interval-adjusted prophylaxis (group 2: starting at 100 IU/kg every 10 days; n=29), on-demand treatment as needed for bleeding episodes and dose adjusted according to bleeding severity (group 3: 20–100 IU/kg, n=27) and treatment for perioperative care (group 4).12
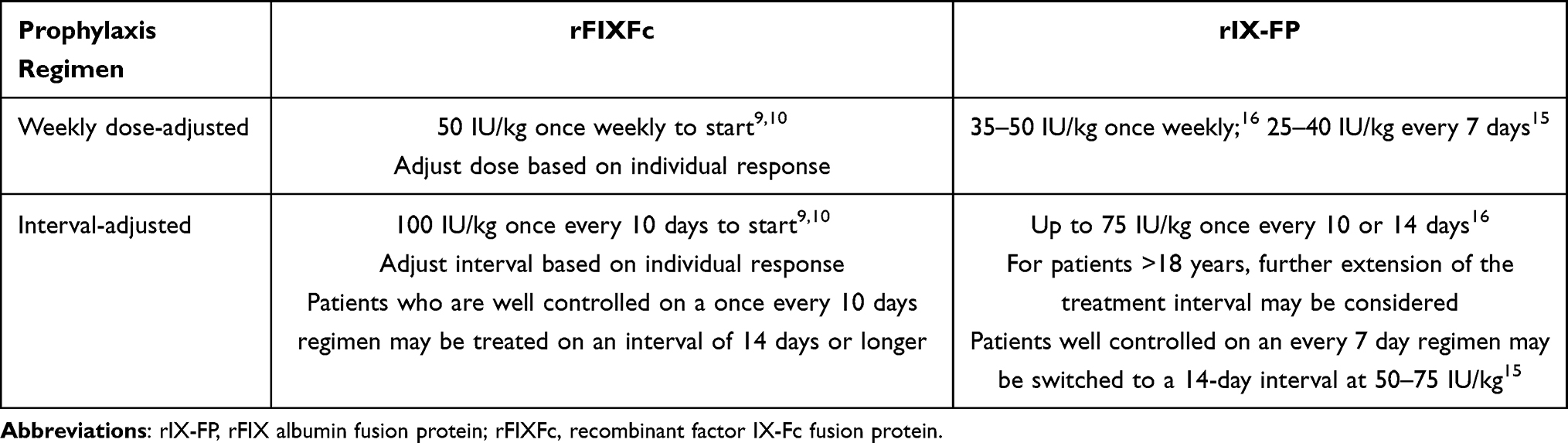 |
Table 1 Approved Dosing Regimens for Long-Term Prophylaxis with rFIXFc or rIX-FP in Adolescent/Adult Patients (≥12 Years) with Hemophilia B |
In PROLONG-9FP, patients (N=63) were treated with one of two rIX-FP regimens.17 Group 1 (n=40) received 35–50 IU/kg once weekly during the first 26 weeks and were then allowed to switch to 75 IU/kg every 10 or 14 days if they had no spontaneous bleeds for ≥4 weeks before switching and were receiving ≤40 IU/kg or ≤50 IU/kg rIX-FP in order to switch to the 14- or 10-day interval, respectively. Group 2 (n=19) received on-demand treatment during the first 26 weeks followed by a fixed dose of 35–50 IU/kg once weekly for ≥26 weeks as determined by the physician.
Several differences between the two trials are worth noting. In B-LONG, but not PROLONG-9FP, patients entering the prophylaxis treatment arms could have been on a previous on-demand regimen; 27.5% of the prophylaxis group in PROLONG-9FP had received previous prophylaxis with rIX-FP before study entry.12,17 In groups 1 and 2 of B-LONG, dose and interval, respectively, were adjusted to maintain a plasma trough level of 1–3 IU/dL or higher in participants who had two breakthrough spontaneous bleeding episodes in a rolling 3-month period. In PROLONG-9FP, the dose could be increased or decreased based on assessment of bleeding phenotype by the treating physician, level of physical activity, or clinical outcome.20 A mean trough FIX activity of 20 and 12 IU/dL was maintained with rIX-FP prophylaxis using 40 IU/kg weekly and 75 IU/kg every 2 weeks, respectively. Lastly, in PROLONG-9FP, after 26 weeks of treatment, patients receiving weekly prophylaxis were evaluated for their eligibility to switch to a longer treatment interval (10 or 14 days) and all patients in the on-demand group switched to weekly prophylaxis for at least an additional 26 weeks.17 In B-LONG, patients received the regimens assigned at enrolment throughout the entire study period.12
Outcome Assessment
The efficacy outcome assessed was mean ABR, a clinically relevant treatment outcome typically evaluated in clinical studies of hemophilia. Median duration of treatment was 51.6 and 58.3 weeks in the dose- and interval-adjusted groups of B-LONG, respectively. In PROLONG-9FP, median duration of treatment was 34.3–55.1 weeks in group 1 and in group 2 was 26.7 weeks during the first 26 weeks of on-demand treatment and 45.1 weeks after switching to a weekly prophylaxis regimen for the remaining time on study.
Data Analysis
MAIC methodology was used to compare estimated ABRs for rFIXFc and rIX-FP, according to recommendations from the National Institute for Health and Clinical Excellence Decision Support Unit (NICE DSU).23 Individual patient data from the B-LONG study were weighted to match the mean baseline characteristics reported for patients in the PROLONG-9FP study, with regard to age (mean, standard deviation [SD]), body weight (mean, SD), ethnicity (proportion of white patients) and mean (SD) number of bleeding events prior to study enrollment. The characteristics selected were the only variables available for comparison due to limited reporting of baseline characteristics across the studies. Matching between two populations with different baseline characteristics always results in a loss of information. The size of the population after matching can be estimated according to the principle provided by the NICE DSU.23 After weighting, the adjusted baseline characteristics of B-LONG participants were the same as those in the population of the PROLONG-9FP study. Adjusted ABRs for rFIXFc were estimated using a Poisson regression model with adjustment for overdispersion and weights calculated through MAIC. Adjusted ABRs can be interpreted as estimates of bleeding frequency if rFIXFc were administered to patients with similar baseline characteristics to those patients recruited in the PROLONG-9FP trial. Finally, estimated ABRs for rFIXFc were compared with the results reported for rIX-FP in the PROLONG-9FP study, and relative treatment effects were presented as incidence rate ratios (IRR) with 95% confidence intervals (CIs). Statistical comparisons were conducted in R v.3.5.5 [https://www.r-project.org/]).
Results
Baseline Characteristics Before Matching
In the current analysis, baseline characteristic data for rFIXFc were extracted from the weekly dose-adjusted (n=63) and interval-adjusted prophylaxis groups (n=29), while those for rIX-FP, which were not reported separately for each arm, were taken from the overall patient population (N=59; 4 of the 23 patients in group 2 received on-demand treatment only and were excluded from the analysis). Data were analyzed according to treatment regimen prior to study entry: prior prophylaxis (rFIXFc, n=48; rIX-FP, n=40) or prior on-demand treatment (n=43 and n=19, respectively).
Patient baseline characteristics from the B-LONG and PROLONG-9FP studies are summarized in Table 2. In the weekly dose-adjusted and interval-adjusted prophylaxis groups of B-LONG, the median age was 28 and 33 years, respectively. The treatment regimen prior to study entry was prophylaxis in 53.2% and 51.7% of patients, respectively, and the proportion of white patients was 65.1% and 62.1%. Furthermore, at baseline, endogenous FIX levels were <1 IU/dL in 79.4% and 75.9% of patients and 1–2 IU/dL in 20.6% and 24.1% of patients, in the weekly dose-adjusted and interval-adjusted prophylaxis groups of B-LONG, respectively.12 Median duration of treatment was 51.6 and 58.3 weeks in the weekly dose-adjusted and interval-adjusted prophylaxis arm, respectively, and the median weekly dose for patients receiving weekly prophylaxis was 45 IU/kg. In the prophylaxis group of PROLONG-9FP, the mean age was 31.6 years, and the proportion of white patients was 82.5%. In the on-demand group, the mean age was 35.3 years, and the proportion of white patients was 82.6%. Endogenous FIX levels were ≤1 IU/dL in 87.5% and 87.0% of patients assigned to the prophylaxis or on-demand groups, respectively, and ≤2 IU/dL in 100% of patients.17 Median duration of treatment was 34.3–55.1 weeks and median consumption was 162.3 and 194.7 IU/kg per month in patients receiving 14-day and 7-day prophylaxis, respectively.
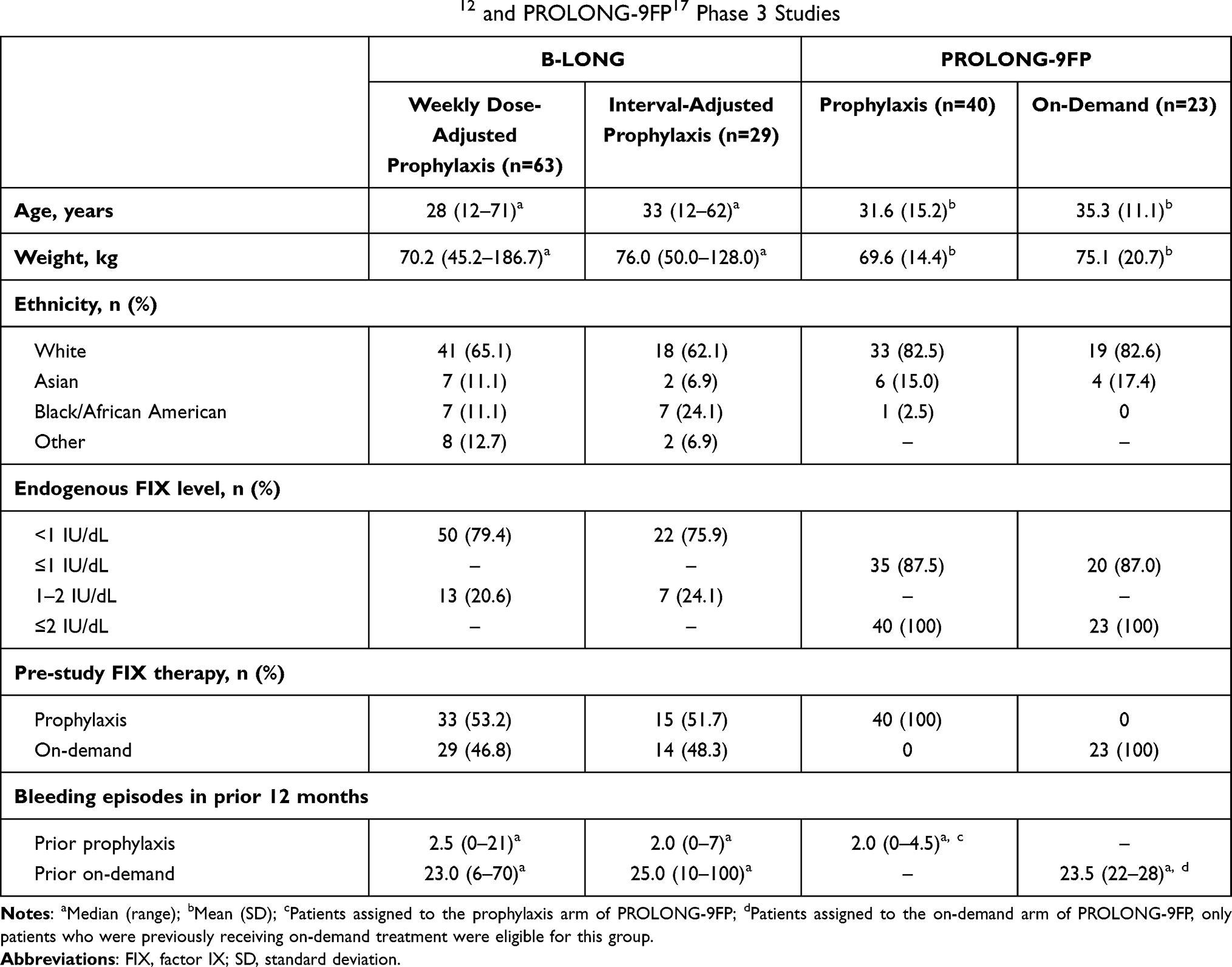 |
Table 2 Baseline Characteristics in the B-LONG12 and PROLONG-9FP17 Phase 3 Studies |
Matching of Baseline Characteristics
Individual patient data from the weekly dose-adjusted and interval-adjusted prophylaxis groups of B-LONG were matched to aggregated data for the participants of PROLONG-9FP regarding baseline age, weight, prior bleeding frequency and ethnicity (Tables 3 and 4). Matching was conducted separately in subsets of patients, who were receiving either prophylaxis or on-demand regimens prior to study enrollment. After matching, the populations of both studies were well balanced regarding all baseline variables and the estimated effective sample size for B-LONG was 26 (63%) for patients who received prior prophylaxis (Table 3) and 10 (26%) for patients who received prior on-demand (Table 4).
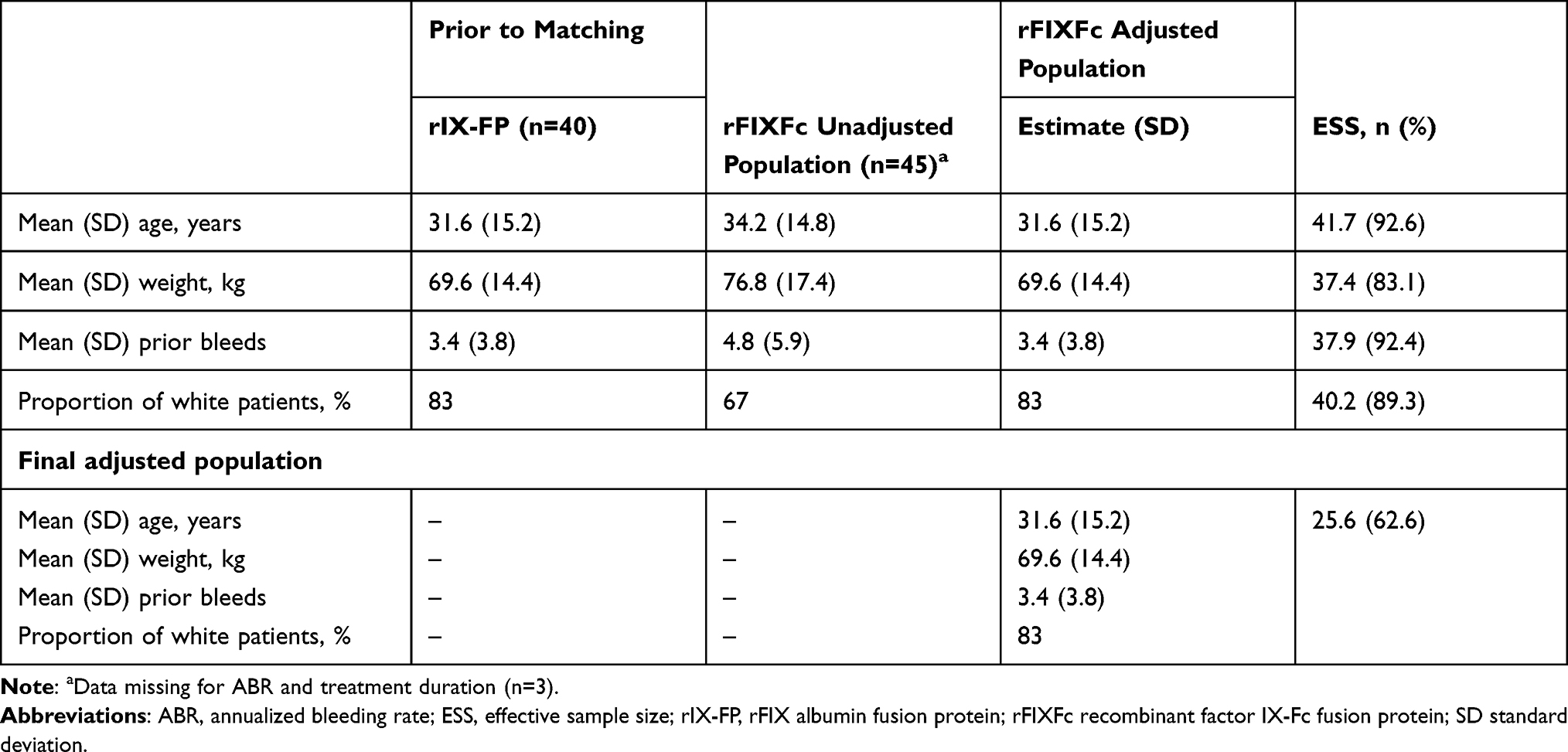 |
Table 3 Balance of Baseline Characteristics and Effective Sample Size Following Matching of Patients on a Prior Prophylactic Regimen from the B-LONG Weekly Dose-Adjusted and Interval-Adjusted Prophylaxis Groups and Group 1 of PROLONG-9FP |
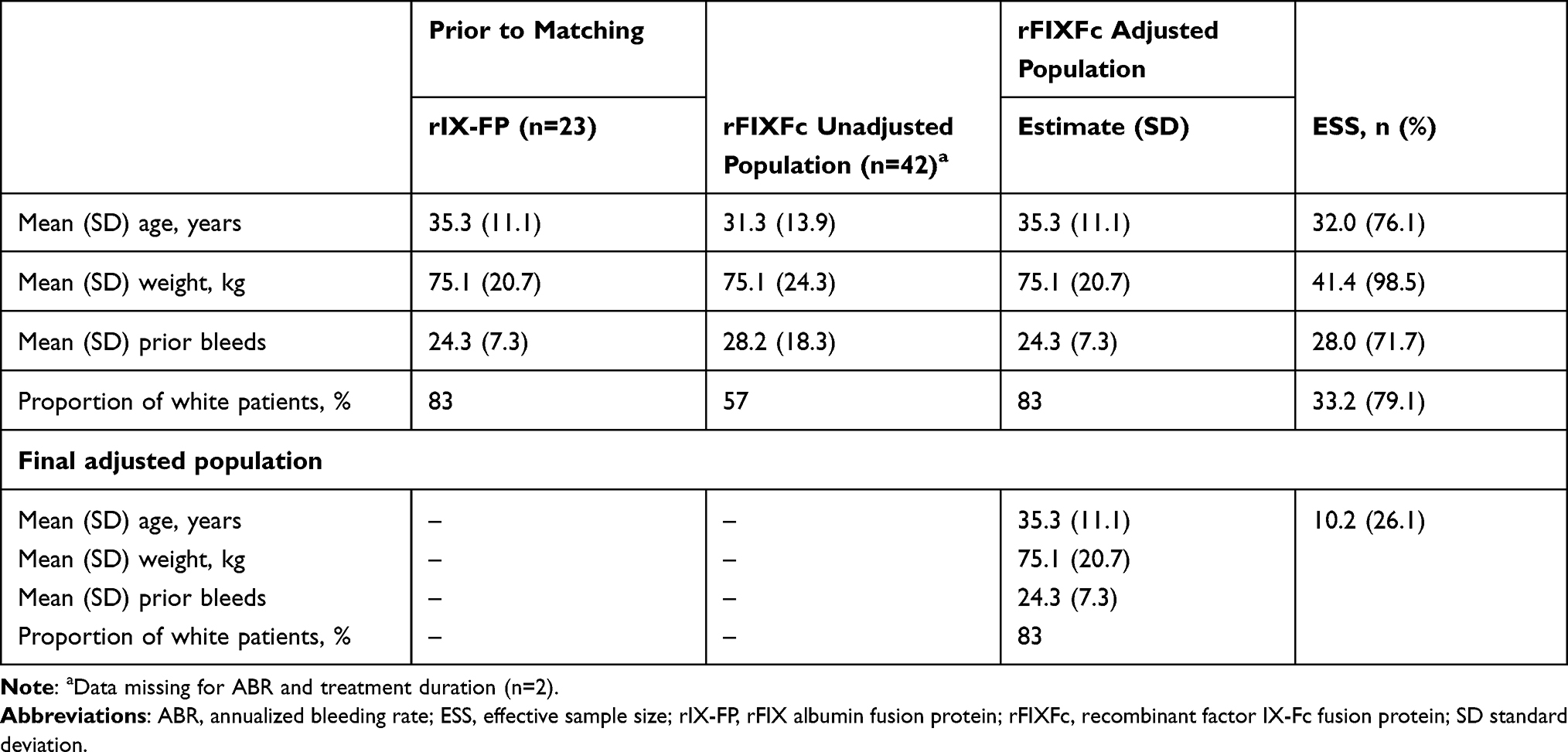 |
Table 4 Balance of Baseline Characteristics and Effective Sample Size Following Matching of Patients on a Prior on-Demand Regimen from the B-LONG Weekly Dose-Adjusted and Interval-Adjusted Prophylaxis Groups and Group 2 of PROLONG-9FP |
Annualized Bleeding Rate
After adjusting for age, weight, prior bleeds, and ethnicity, estimated ABR in patients who received prior prophylaxis was 1.87 for rFIXFc and 1.58 for rIX-FP. The difference between the two treatment groups was not statistically significant (IRR 1.18; 95% CI 0.67–2.10; Figure 1).
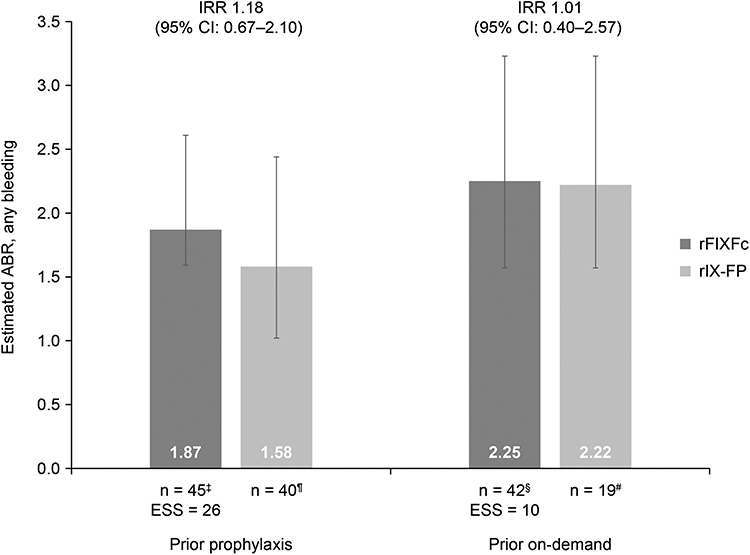 |
Figure 1 Estimated ABR, any bleeding, after matching for all selected baseline variables†. Abbreviations: ABR, annualized bleeding rate; CI, confidence interval; ESS, effective sample size; IRR, incidence rate ratio; rIX-FP, rFIX albumin fusion protein; rFIXFc, recombinant factor IX-Fc fusion protein. Notes: †Age, weight, prior bleeds and ethnicity (proportion of white patients); ‡Data missing for ABR and treatment duration (n=3); ¶Data from PROLONG-9FP; §Data missing for ABR and treatment duration (n=2); #Data from PROLONG-9FP, of the 23 patients receiving prior on-demand only 19 patients transitioned to prophylaxis. |
Similarly, after adjustment, the difference in estimated ABR in patients who received prior on-demand was not statistically significant between rFIXFc and rIX-FP (2.25 versus 2.22, respectively; IRR 1.01, 95% CI 0.40–2.57; Figure 1).
Discussion
The results of this MAIC analysis show that the estimated ABR for rFIXFc-treated patients from B-LONG was similar to that of rIX-FP-treated patients from PROLONG-9FP and, therefore, provides evidence of similar bleed protection between the two EHL FIX products in patients with hemophilia B. This is despite the large difference between target trough levels for rFIXFc (1–3 IU/kg)12 and measured trough levels with rIX-FP (20.0 IU/dL at day 7 during once weekly prophylaxis with 40 IU/kg; 12.4 IU/kg at day 14 during 14-day prophylaxis with 75 IU/kg).17 Higher FIX trough levels may be needed for rIX-FP to achieve similar protection from bleeds as rFIXFc at target trough levels of 1–3 IU/kg, which might be attributed to differences in their physiological (PK/pharmacodynamic) profiles, including extravascular distribution. However, it should be noted that the relationship between targeted and measured trough levels and clinical outcomes cannot be directly compared, owing to differences in the PK characteristics of the two products.
EHL FIX products, such as rFIXFc and rIX-FP, facilitate the use of prophylactic treatment in patients with hemophilia B, by maintaining or improving bleed protection while reducing the injection frequency, versus standard half-life products.2 Therefore, they have the potential to decrease the burden of prophylaxis, improve health outcomes, and allow for a more active lifestyle.2,3 The standard trough level for bleed prevention is generally regarded as 1%, and is based on data, largely from experience with hemophilia A, showing that patients with factor activity levels >1% tend to have fewer joint bleeds and less arthropathy during prophylaxis.24 However, data have shown that some patients experience joint bleeds with trough levels >3%,25 indicating that FIX levels should be determined on a person-to-person basis, and in consideration of the specific molecular characteristics of the FIX product being used.
Current guidelines provide broad recommendations for calculating dosing regimens;26 however, they do not account for inter-patient variability in PK parameters, bleeding phenotype, levels of physical activity, lifestyle and joint status.3 Importantly, although trough level can be used as a surrogate marker for monitoring the efficacy of a prophylaxis regimen, it cannot be compared across patients or products, especially products with different moieties/modifications to extend half-life. Other parameters, such as clinical outcomes (eg, bleed rates, assessment of joint health) should be considered, and therapy tailored to individual patient needs may be the best approach to achieve optimal bleed protection. In addition, long-term effects of these treatments should also be considered; in the rIX-FP extension study, the most frequently reported treatment-emergent adverse event was arthralgia (25 events in 19 [32.2%] patients).20
The study has the following limitations. Although MAIC is the recommended method, as it can account for population differences when comparing treatments assessed in disconnected studies, the method cannot adjust for all possible differences across trials, such as undocumented differences at baseline. Furthermore, the lack of randomization with a placebo arm in B-LONG and PROLONG-9FP hampers adjustments for residual confounding. Another limitation is that estimated sample sizes following assignment of weights were low, and, therefore, the amount of information for the comparison between rFIXFc and rIX-FP was limited, which should be considered when interpreting the results.
Despite the limitations, this indirect treatment comparison provides a useful measure of relative efficacy between these two EHL FIX products for the treatment of patients with hemophilia B.
Conclusions
This MAIC analysis shows that the estimated ABR for rFIXFc-treated patients from B-LONG was similar to that of rIX-FP-treated patients from PROLONG-9FP and, therefore, provides no evidence of a difference in efficacy between rFIXFc and rIX-FP when used as prophylaxis in patients with hemophilia B. This is despite the large difference in trough levels between the two products (target [1–3 IU/dL] versus obtained [20 IU/dL], respectively), suggesting that trough level is not a surrogate indicator when ABR is used as a criterion for clinical efficacy when comparing these FIX products in hemophilia B.
Compliance with Ethics Guidelines
Ethical approval was not required for this analysis as it was based on data from two previously published Phase III trials (B-LONG and PROLONG-9FP). Both the B-LONG and PROLONG-9FP studies were conducted in accordance with the Declaration of Helsinki and local regulations. The protocols were approved by the authorities and the institutional review board/ethics committee at each participating center, and signed informed consent was obtained from all patients. Informed consent for this analysis was not required given the de-identified nature of the B-LONG individualized patient-level data, and the use of aggregated, previously published data from PROLONG-9FP.
Acknowledgments
The project was funded by Swedish Orphan Biovitrum AB (Sobi). Medical writing and editorial support, funded by Sobi, was provided by Rachel Bell, PhD, Bioscript Medical, Macclesfield, UK. The results described in this paper were presented as an eposter at the 14th Annual Congress of the European Association for Haemophilia and Allied Disorders (EAHAD 2021). The poster’s abstract was published in Haemophilia 2021;27(S2):68 (ABS092). Available from: Abstract (https://onlinelibrary.wiley.com/doi/epdf/10.1111/hae.14236).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. The manuscript was reviewed by Sobi and Sanofi before publishing.
Disclosure
J. Astermark reports research support from Sobi, CSL Behring, Takeda/Shire and Bayer; honoraria for consulting from Octapharma, Novo Nordisk, Pfizer, Bayer, Sobi, CSL Behring, Takeda/Shire, BioMarin, uniQure and Spark Therapeutics; and speaker bureau fees from Octapharma, Novo Nordisk, Pfizer, Bayer, Sobi, CSL Behring, Takeda/Shire and BioMarin. R. Klamroth: reports research funding and honoraria for consulting and lectures from Bayer, BioMarin, Biotest, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Roche, Takeda/Shire and Sobi. Piotr Wojciechowski and S. Aballéa are employees of Creativ-Ceutical, a consultancy company that received funding from Sobi for this research. Z. Hakimi and J. Nazir are employees of Sobi. The authors report no other conflicts of interest in this work.
References
1. Iorio A, Marchesini E, Marcucci M, Stobart K, Chan AK. Clotting factor concentrates given to prevent bleeding and bleeding-related complications in people with hemophilia A or B. Cochrane Database Syst Rev. 2011;(9):CD003429.
2. Lambert T, Benson G, Dolan G, et al. Practical aspects of extended half-life products for the treatment of haemophilia. Ther Adv Hematol. 2018;9(9):295–308. doi:10.1177/2040620718796429
3. Castaman G. The benefits of prophylaxis in patients with hemophilia B. Expert Rev Hematol. 2018;11(8):673–683. doi:10.1080/17474086.2018.1489719
4. Jiménez-Yuste V, Auerswald G, Benson G, et al. Achieving and maintaining an optimal trough level for prophylaxis in haemophilia: the past, the present and the future. Blood Transfusion. 2014;12(3):314–319.
5. Walsh C, Coppens M, Escobar M, Wang M. Optimal trough levels in haemophilia B: raising expectations. Haemophilia. 2020;26(6):e334–e336. doi:10.1111/hae.14098
6. Shapiro A, Potts J, Li SV, et al. Association of bleeding tendency with time under target FIX activity levels in severe hemophilia B Patients treated with recombinant factor IX Fc fusion protein [abstract]. Blood. 2013;122(21):2349. doi:10.1182/blood.V122.21.2349.2349
7. Tjärnlund-Wolf A, Lassila R. Phenotypic characterization of haemophilia B - Understanding the underlying biology of coagulation factor IX. Haemophilia. 2019;25(4):567–574.
8. Iorio A, Fischer K, Blanchette V, et al. Tailoring treatment of haemophilia B: accounting for the distribution and clearance of standard and extended half-life FIX concentrates. Thromb Haemost. 2017;117(6):1023–1030. doi:10.1160/TH16-12-0942
9. Sanofi Genzyme. Alprolix Prescribing Information; Published 2017. Available from: http://products.sanofi.us/Alprolix/alprolix.html.
10. European Medicines Agency. Alprolix Summary of Product Characteristics; Published 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/alprolix-epar-product-information_en.pdf.
11. Fischer K, Kulkarni R, Nolan B, et al. Recombinant factor IX Fc fusion protein in children with haemophilia B (Kids B-LONG): results from a multicentre, non-randomised phase 3 study. Lancet Haematol. 2017;4(2):e75–e82. doi:10.1016/S2352-3026(16)30193-4
12. Powell JS, Pasi KJ, Ragni MV, et al. Phase 3 study of recombinant factor IX Fc fusion protein in hemophilia B. N Engl J Med. 2013;369(24):2313–2323. doi:10.1056/NEJMoa1305074
13. Pasi KJ, Fischer K, Ragni M, et al. Long-term safety and sustained efficacy for up to 5 years of treatment with recombinant factor IX Fc fusion protein in subjects with haemophilia B: results from the B-YOND extension study. Haemophilia. 2020;26(6):e262–e271. doi:10.1111/hae.14036
14. Shapiro AD, Pasi KJ, Ozelo MC, et al. Extending recombinant factor IX Fc fusion protein dosing interval to 14 or more days in patients with hemophilia B. Res Pract Thromb Haemost. 2019;3(1):109–113. doi:10.1002/rth2.12163
15. CSL Behring. Idelvion Prescribing Information; Published 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/idelvion-epar-product-information_en.pdf.
16. European Medicines Agency. Idelvion Summary of Product Characteristics; Published 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/idelvion-epar-product-information_en.pdf.
17. Santagostino E, Martinowitz U, Lissitchkov T, et al. Long-acting recombinant coagulation factor IX albumin fusion protein (rIX-FP) in hemophilia B: results of a phase 3 trial. Blood. 2016;127(14):1761–1769. doi:10.1182/blood-2015-09-669234
18. Kenet G, Chambost H, Male C, et al. Long-acting recombinant fusion protein linking coagulation factor IX with albumin (rIX-FP) in children. Results of a phase 3 trial. Thromb Haemost. 2016;116(4):659–668. doi:10.1160/TH16-03-0179
19. Kenet G, Chambost H, Male C, et al. Long-term safety and efficacy of recombinant coagulation factor ix albumin fusion protein (rIX-FP) in previously treated pediatric patients with hemophilia B: results from a Phase 3b extension study. Thromb Haemost. 2020;120(4):599–606. doi:10.1055/s-0040-1705116
20. Mancuso ME, Lubetsky A, Pan-Petesch B, et al. Long-term safety and efficacy of rIX-FP prophylaxis with extended dosing intervals up to 21 days in adults/adolescents with hemophilia B. J Thromb Haemost. 2020;18(5):1065–1074. doi:10.1111/jth.14778
21. Chaimani A, Caldwell DM, Higgins JPT, et al. Chapter 11: undertaking network meta-analyses. In: Higgins JPT, Thomas J, Chandler J, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.1 Ed. Cochrane; 2020.
22. Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940–947. doi:10.1016/j.jval.2012.05.004
23. NICE Decision Support Unit. NICE DSU Technical Support Document 18: methods for population-adjusted indirect comparisons in submissions to NICE; Published 2016. Available from: http://nicedsu.org.uk/technical-support-documents/population-adjusted-indirect-comparisons-maic-and-stc/.
24. Ahlberg A. Haemophilia in Sweden. VII. Incidence, treatment and prophylaxis of arthropathy and other musculo-skeletal manifestations of haemophilia A and B. Acta Orthop Scand Suppl. 1965;Suppl 77:73–132.
25. Ahnstrom J, Berntorp E, Lindvall K, Bjorkman S. A 6-year follow-up of dosing, coagulation factor levels and bleedings in relation to joint status in the prophylactic treatment of haemophilia. Haemophilia. 2004;10(6):689–697. doi:10.1111/j.1365-2516.2004.01036.x
26. Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158. doi:10.1111/hae.14046
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.