")
Back to Journals » International Journal of Women's Health » Volume 8
Efficacy of misoprostol for the treatment of postpartum hemorrhage: current knowledge and implications for health care planning
Received 19 December 2015
Accepted for publication 10 June 2016
Published 29 July 2016 Volume 2016:8 Pages 341—349
DOI https://doi.org/10.2147/IJWH.S89315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Ndola Prata, Karen Weidert
Bixby Center for Population, Health and Sustainability, School of Public Health, University of California at Berkeley, Berkeley, CA, USA
Background: A myriad of interventions exist to treat postpartum hemorrhage (PPH), ranging from uterotonics and hemostatics to surgical and aortic compression devices. Nonetheless, PPH remains the leading cause of maternal mortality worldwide. The purpose of this article is to review the available evidence on the efficacy of misoprostol for the treatment of primary PPH and discuss implications for health care planning.
Data and methods: Using PubMed, Web of Science, and GoogleScholar, we reviewed the literature on randomized controlled trials of interventions to treat PPH with misoprostol and non-randomized field trials with controls. We discuss the current knowledge and implications for health care planning, especially in resource-poor settings.
Results: The treatment of PPH with 800 µg of misoprostol is equivalent to 40 IU of intravenous oxytocin in women who have received oxytocin for the prevention of PPH. The same dose might be an option for the treatment of PPH in women who did not receive oxytocin for the prevention of PPH and do not have access to oxytocin for treatment. Adding misoprostol to standard uterotonics has no additional benefits to women being treated for PPH, but the beneficial adjunctive role of misoprostol to conventional uterotonics is important in reducing intra- and postoperative hemorrhage during cesarean section.
Conclusion: Misoprostol is an effective uterotonic agent in the treatment of PPH. Clinical guidelines and treatment protocols should be updated to reflect the current knowledge on the efficacy of misoprostol for the treatment of PPH with 800 µg sublingually.
Keywords: PPH treatment, uterotonics, low-resource settings, cesarean section, retained placenta
Introduction
The world has witnessed reductions in maternal deaths in the past decade. Kassebaum et al1 reported that the annual rate of change in the maternal mortality ratio was greater than −1% between 2003 and 2013, with the most substantial improvement from 2012 to 2013 at −3.3%. Many of the global gains in reducing maternal mortality can be attributed to developments in preventing and treating postpartum hemorrhage (PPH). In fact, the biggest absolute reduction was in maternal deaths due to hemorrhage.
Yet, PPH remains the most common cause of maternal death globally2 and has persisted in low-income countries with little change since 1990.1 This is in part due to the prevalence of home deliveries and limited access to life-saving uterotonic drugs in these countries.3–5 Meanwhile, there is also evidence that the rate of retained placenta and PPH is increasing in higher-income countries.6,7
PPH is often associated with the failure of the uterus to contract after delivery and categorized as blood loss of 500 mL or more following vaginal delivery or 1,000 mL after cesarean delivery.8,9 PPH is categorized as primary if it occurs within 24 hours of delivery and secondary if excessive blood loss occurs at 24 hours or more after delivery. The reality is that most cases are primary PPH and the time from beginning to death is considerably shorter than other major obstetric complications. Two factors have been identified as significantly affecting the potential for death from PPH. First, the initial hemoglobin (Hb) level of a woman affects her survival rate from PPH.10 The World Health Organization (WHO) defines anemia in pregnancy as Hb level <11 g/dL and reported that anemia among pregnant women in developing countries exceeds 50%.11 Recently, a strong correlation was found between low Hb (Hb <10) and the risk of PPH, as well as an association between severe anemia and emergency hysterectomy.12 Anemia can be detected during pregnancy, but early detection and treatment are not always promising in settings where limited access to quality antenatal care is further compounded by dietary deficiencies and concurrent medical disorders affecting iron absorption.12–14 The second factor that has been identified as contributing to mortality rates from PPH has more levers for influence, as it relates to access to a hospital with functioning facilities for the management of PPH, including blood banks and staff trained to diagnose and treat PPH. Although effective tools for the prevention and treatment of PPH are available, most are not feasible or available for use in the resource-poor countries, where many births still occur at home with untrained birth attendants.10 Meanwhile, the management of PPH is further complicated by timely diagnosis.10 Underestimation of blood loss by 100–150 mL is common when applying visual estimation.15 A study in 13 European countries showed that the use of a blood collector bag has not significantly reduced the rate of PPH, likely due to larger challenges in the management of PPH.16 However, better accuracy in the measurement of postpartum blood loss in developing countries might be an important first step toward improving case management.17
A recent multinational study led by the WHO to explore clinical practices, risks, and maternal outcomes associated with PPH included 275,000 births in 28 low- and middle-income countries. Of all the women included in the analysis, 95.3% received an uterotonic prophylaxis and 1.2% of women reported PPH; with the overall PPH death rate of 38 per 100,000 births. Not only is uterotonic treatment of PPH important in the reduction of adverse maternal outcomes but it can help avert more medical interventions, including the administration of intravenous (IV) fluids, additional drug therapy, blood transfusion, and surgery.18
The role of misoprostol, a prostaglandin E1 analog, in the prevention and treatment of PPH has evolved over time due to its long shelf life and multiple routes of administration, which make it more suitable for low-resource settings with limited skilled providers.19,20 As early as 2007, researchers were supporting the use of misoprostol for treating PPH in cases where other treatments are not available or not working, yet treating PPH in the community with misoprostol has lagged behind its widespread prophylactic use.9,21
The purpose of this article is to review the available evidence on the efficacy of misoprostol for the treatment of primary PPH. A brief historical perspective on the use of misoprostol for PPH and its potential role in treatment is presented as well as implications for management guidelines and health care planning, especially for low-income countries.
Data and methods
We first searched the Cochrane Database of Systematic Reviews for the most recent review of misoprostol for the treatment of PPH. We then searched PubMed for the literature on randomized controlled trials (RCTs) of interventions to treat PPH with misoprostol and reviewed relevant manuscripts not included in the most recent systematic review. Finally, we searched PubMed, Web of Science, and GoogleScholar for non-randomized field trials of interventions to treat PPH with misoprostol. The search covered the period from 2000 until 2015. The following search terms and various combinations were used: “postpartum hemorrhage”, “PPH”, “PPH treatment with misoprostol”, “misoprostol”, “randomized controlled trial”, “RCT”, “operations research”, “field trial”, “interventions to treat PPH”, “vaginal delivery”, “cesarean section”, and “retained placenta”.
Evidence on efficacy is based on the results from RCTs against either placebo or another uterotonic agent with or without active management of the third stage of labor with an uterotonic agent. Since we found only seven randomized controlled studies, we assess them individually. The last systematic review of misoprostol to treat PPH was published in 2005 and included only three of the seven reviewed RCTs. Even though it is not the primary aim of this review, we report on the efficacy of misoprostol for two conditions commonly associated with PPH, cesarean section and retained placenta. For these two conditions, we started with the more recent systematic review and meta-analysis, or Cochrane review published since 2000, and then reviewed individual RCT studies published after the systematic review. Results from non-randomized studies with controls or cohort studies are also reviewed. Current perspectives on PPH treatment are discussed including advances in drug regimens, gaps in current knowledge regarding PPH treatment with misoprostol, and challenges and opportunities for large-scale implementation in low-income countries.
Results
Misoprostol for the treatment of PPH
Over the past decade, key women’s health organizations have promoted the inclusion of misoprostol for the treatment of PPH. As early as 2006, the International Confederation of Midwives and the International Federation of Gynecology and Obstetrics (FIGO) recommended that misoprostol for the treatment of PPH may be appropriate for use in low-resource settings as a stand-alone treatment, in combination with oxytocin, and as a last resort for PPH treatment.22 At the same time, the American Congress of Obstetricians and Gynecologists included misoprostol in the list of uterotonics to be used as the first-line treatment for hemorrhage in the event of decreased uterine atony.23 A few years later, the Royal College of Obstetricians and Gynecologists agreed that misoprostol may be an appropriate alternative for PPH treatment in settings, where parenteral prostaglandins are not available or where there are contraindications.24 In 2012, FIGO published its guidelines for the treatment of PPH with misoprostol: “one dose of misoprostol 800 μg sublingually is indicated for the treatment of PPH when 40 IU IV oxytocin is not immediately available (irrespective of the prophylactic measures)”.25
In 2014, the Cochrane collaboration published a systematic review on the treatment for primary PPH.26 The review assessed the effectiveness and safety of any intervention used for the treatment of PPH. Of the ten RCTs reviewed spanning 4,052 women, seven investigated misoprostol in doses varying from 600 μg to 1,000 μg, using various routes of administration, including a combination of sublingual and rectal. The finding that seven out of ten studies were assessing the efficacy of misoprostol alone suggests that the role of misoprostol has been one of the most studied interventions in the treatment of PPH in recent decades. However, it was not until April 2015 that misoprostol was added to Essential Medicines WHO Model List (EML) for the treatment of PPH. The EML now recommends the use of misoprostol for the “prevention and treatment of PPH where oxytocin is not available or cannot be safely used”.27
Evidence of efficacy of misoprostol for the treatment of PPH
Table 1 presents the results from all the published RCTs on the use of misoprostol for the treatment of primary PPH after vaginal deliveries. The last systematic review of misoprostol to treat PPH was published in 2005 and included three RCTs.28 However, given that only seven trials were available, we decided to show them individually in Table 1. RCTs have used multiple dose regimens and routes, in addition to controlling against placebo or another conventional uterotonic, oxytocin, and/or ergometrine. The first RCT was published in 2001 comparing 800 mg of misoprostol rectally to 5 IU oxytocin and 500 μg ergometrine intramuscular plus 10 IU oxytocin diluted in 500 mL normal saline IV infusion. Results from a relatively small sample size (n=32 in each arm) were promising, indicating that misoprostol is an effective therapy.29 In 2004, Hofmeyr et al30 published a placebo-controlled trial testing a high-dose misoprostol, but the study was underpowered to show significant differences. In the same year, a study by Walraven et al31 combined oral (200 μg) and sublingual (400 μg) routes of misoprostol and also showed the therapeutic potential of misoprostol against a placebo. Four years later, an RCT in Pakistan attempted to ascertain whether sublingual misoprostol had additional benefits to a standard oxytocin regimen. Although significant reductions in blood loss in the misoprostol group were reported, the study did not reach the intended sample size due to much lower PPH rate than expected.32 However, it was not until 2010 that pivotal evidence on the therapeutic potential of misoprostol became available from three RCTs. In a double-blind non-inferiority trial, Blum et al demonstrated that 800 μg of sublingual misoprostol is clinically equivalent to 40 IU IV oxytocin in women who have received prophylactic oxytocin during the third stage of labor. However, while the time to cessation and additional blood loss of 300 mL and 500 mL was equivalent, the number of women in the misoprostol group with >1,000 mL of additional blood loss was significantly higher (relative risk [RR]: 3.6; 95% confidence interval [CI]: 1.02–12.88). The women in the misoprostol group were also more likely to undergo intrauterine clinical exploration under anesthesia (RR: 1.66; 95% CI: 1.00–2.76).33 Results from a similar trial, but among women who have not been exposed to oxytocin during the third stage of labor, showed that misoprostol is slightly inferior to oxytocin.34 Authors conclude that in the absence of oxytocin, misoprostol might be an appropriate first-line treatment for PPH. The third RCT, published in 2010, assessed whether 600 μg of sublingual misoprostol could be used as an adjunct therapy to standard uterotonics. Results showed that when compared to a placebo, misoprostol does not offer additional benefits.35
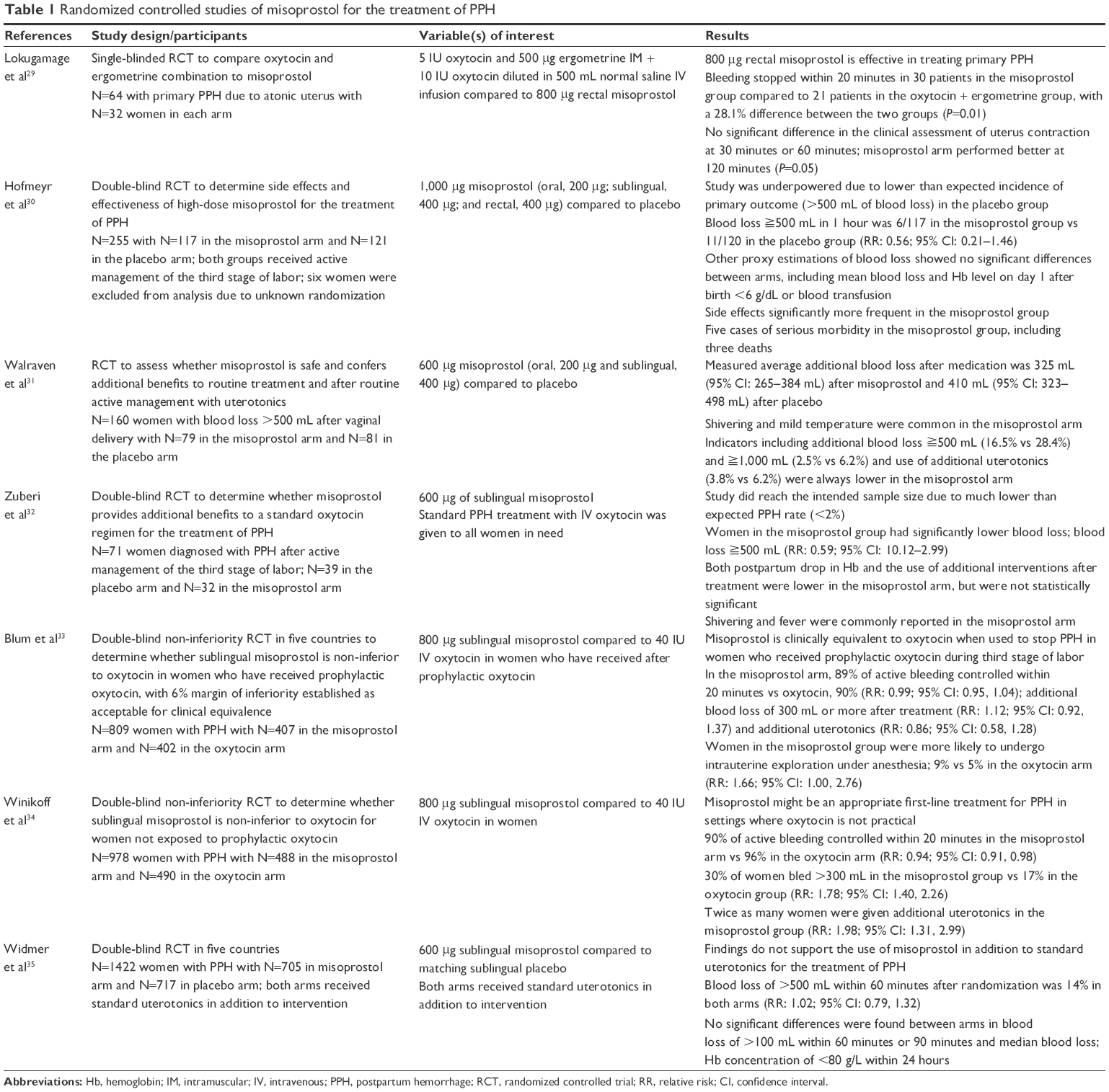 | Table 1 Randomized controlled studies of misoprostol for the treatment of PPH |
Table 2 shows the results from three non-randomized cohort studies with controls. These studies attempted to demonstrate application in home and hospital births. The study by Prata et al,36 the only community-based study with controls for the treatment of PPH, used a high dose (1,000 μg) of rectal misoprostol and demonstrated the potential use of misoprostol for PPH treatment in settings where women were not exposed to conventional uterotonics during the third stage of labor. In fact, Winikoff et al’s34 RCT findings, although with a lower dose and different route, confirmed the value of misoprostol in settings where oxytocin is not available. The use of high-dose rectal misoprostol was also assessed as an adjunct therapy to oxytocin compared to ergometrine using a retrospective cohort study design.37 Results showed no significant differences between the two groups. Based on the results from the 2010 RCT, we now know that misoprostol has no adjunct therapeutic properties.35 A cohort study in three Nigerian hospitals showed that 800 μg of sublingual misoprostol was efficacious in stopping bleeding within 20 minutes of use among women diagnosed with PPH from uterine atony and not exposed to uterotonics during the third stage of labor, suggesting that the application of results of the 2010 RCT in clinical practice produces intended outcomes. Misoprostol stopped bleeding in 85% of the PPH cases, the remaining needed additional uterotonics.38
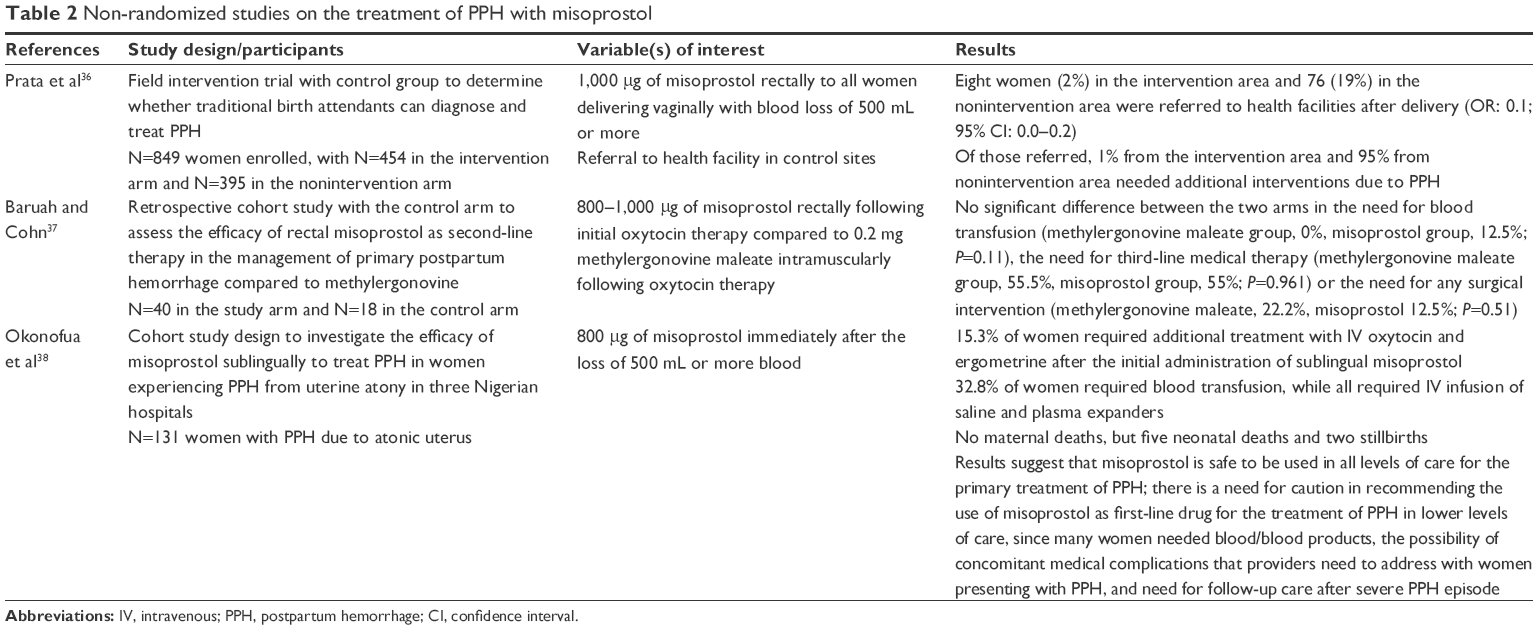 | Table 2 Non-randomized studies on the treatment of PPH with misoprostol |
The safety profile of misoprostol in obstetrics has long been established and is linked to the pharmacokinetic profile of E2 prostaglandin analog.39 In RCTs, misoprostol administered in treatment doses shows increased RR of side effects when compared to placebo. Although side effects were reported as transient and occurring in a small group of women, pooled data from a Cochrane review show average increases in vomiting (RR: 1.84; 95% CI: 1.16–2.95), shivering (RR: 2.25; 95% CI: 1.76–2.88), pyrexia of 38°C (RR: 3.12; 95% CI: 2.66–3.67), and pyrexia of 40°C or more (RR: 13.58; 95% CI: 4.93–37.44).26
Other conditions around labor and delivery associated with PPH
The use of misoprostol in intra- and postoperative hemorrhage, as well as in retained placenta, has been investigated. Results from a systematic review and meta-analysis evaluating the efficacy and safety of misoprostol for reducing intra- and postoperative hemorrhage showed that misoprostol combined with oxytocin seems to be more efficacious than oxytocin alone.40 The systematic review included 17 studies totaling 3,174 women. Seven studies assessed misoprostol vs oxytocin and seven assessed misoprostol plus oxytocin vs oxytocin alone. Subsequent RCTs found similar results when comparing misoprostol and oxytocin to oxytocin alone during cesarean delivery in women at risk of PPH.41,42
A Cochrane review of prostaglandins for the management of retained placenta involving 244 women, of whom 194 received a dose of 800 μg misoprostol, showed that prostaglandins were not superior compared to placebo. No statistically significant differences were found in the manual removal of placenta, severe PPH, need for blood transfusion, or other interventions.43 However, the authors noted that the quality of the evidence was low and called for much larger and sufficiently powered studies to make recommendations.
Implications for management guidelines and health care planning
Although RCTs and non-randomized trials have used different doses and routes of administration, current evidence points to an optimal and effective dose regimen of 800 μg of sublingual misoprostol for the treatment of PPH, which was endorsed by FIGO.25 The safety profile of this dose and route is sufficient, but prostaglandin-related side effects such as shivering and vomiting may occur.26
Misoprostol’s clinical equivalence to 40 IU IV oxytocin, when used for the treatment of PPH in women who have received a prophylactic dose of oxytocin during the third stage of labor, provides unique opportunities for low-resource settings. Where labor wards are ill-equipped to provide sufficient monitoring and quality IV infusion, service providers can use intramuscular oxytocin during the third stage of labor and sublingual misoprostol if a PPH diagnosis is established without hesitation. In addition, given the longer shelf life of misoprostol and relatively better stability in field conditions,39 health service planners, particularly those responsible for drug procurement, can adjust forecasting and purchasing of the drug assuming all estimated primary PPH cases will be treated with misoprostol, making it the first-line treatment.
Current evidence shows that in the absence of oxytocin prophylaxis during the third stage of labor, the drug of choice for the treatment of PPH should be 40 IU IV oxytocin. However, in settings where oxytocin is not available, sublingual misoprostol is an appropriate first-line treatment. This finding is of significance for settings where a large number of women deliver at home without a skilled provider or with a minimally trained one, as well as in settings where delivery begins at home and access to health facilities for referral when PPH is identified is limited due to the lack of transportation, road security at night, and other issues.3
Contrary to expectations based on the evidence prior to 2010, findings from a multicenter RCT do not support the use of misoprostol in addition to standard uterotonics (oxytocin or ergometrine) for the treatment of primary PPH after vaginal deliveries.35 However, RCTs have demonstrated the opposite for cesarean deliveries.40–42 Thus, the adjunct role of misoprostol to conventional uterotonics is important in reducing intra- and postoperative hemorrhage.
In summary, current evidence on misoprostol efficacy is sufficient to move programs forward such that low-income countries, the ones with highest share of PPH-attributed burden of disease, can benefit from the ease of administration and storage of the drug. However, it is also in these contexts where the management of PPH cases is more challenging, despite knowledge of drug efficacy. For example, the efficacy from clinical trials assumes relatively accurate blood loss measurement, leading to a specific point in time when treatment is administered. Thus, standardizing clinical protocols with culturally appropriate ways to measure blood loss after delivery could increase program effectiveness for the treatment of PPH. Task shifting or sharing with providers at lower-level health centers and health posts, including community health workers, should also be considered, especially when referrals to health facilities are difficult. In many countries, where access to misoprostol for PPH is being scaled up,44 providers could benefit from learning not just about prevention but also about the treatment for PPH, including clinical officers providing emergency cesarean sections in rural or district hospitals. Other ways to potentially increase program effectiveness to treat PPH in women who deliver at home would certainly include the use of community health workers and/or traditional birth attendants trained in the recognition of PPH and administration of misoprostol. However, more evidence in this area is still needed.
A Cochrane review with the objective of determining the safety and effectiveness of a system for advanced distribution of misoprostol for the prevention and treatment of PPH found insufficient evidence to support such a system.45 The review identified three studies, and none of them met the inclusion criteria – randomized or quasi RCTs. Thus, the conclusion is based on the lack of evidence rather than results from existing evidence. However, given the current knowledge of PPH-attributed mortality and the role of misoprostol to treat PPH, a randomized placebo-controlled experiment for advance distribution at community level might pose ethical concerns.
The comparison of misoprostol to placebo or to conventional uterotonics would allow programs to make informed decisions about the realm of interventions that are possible to implement in each setting according to provider level and health care system capacity. However, one important question still remains: can misoprostol be given for the treatment of PPH after its use for prevention during the third stage of labor? In addition, even though conventional uterotonics are more commonly used, what is the relative contribution of misoprostol compared to other interventions for PPH treatment, such as the non-pneumatic antishock garment, hemostatic drugs, and surgical interventions? A review of these interventions concluded that more evidence is needed, including the best ways to treat women who do not respond to uterotonics.26
Conclusion
Misoprostol is an effective therapy for primary PPH. Clinical guidelines and treatment protocols should be updated to reflect the current knowledge on the efficacy of 800 μg sublingual misoprostol for the treatment of PPH. However, improvements in PPH treatment, regardless of the uterotonic, should start with a timely and correct diagnosis that can lead to an appropriate case management. Women with prior exposure to prophylactic oxytocin, as well as those without exposure to oxytocin and in settings where oxytocin is not available, could all benefit from the therapeutic properties of this drug. Women undergoing cesarean section and at risk of PPH could also benefit from the efficacy of misoprostol in conjunction with oxytocin.
Disclosure
The authors report no conflicts of interest in this work.
References
Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9947):980–1004. | ||
Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–e333. | ||
Prata N, Passano P, Rowen T, Bell S, Walsh J, Potts M. Where there are (few) skilled birth attendants. J Health Popul Nutr. 2011;29(2):81–91. | ||
Montagu D, Yamey G, Visconti A, Harding A, Yoong J. Where do poor women in developing countries give birth? A multi-country analysis of demographic and health survey data. PLoS One. 2011;6(2):e17155. | ||
Crowe S, Utley M, Costello A, Pagel C. How many births in sub-Saharan Africa and South Asia will not be attended by a skilled birth attendant between 2011 and 2015? BMC Pregnancy Childbirth. 2012;12:4. | ||
Knight M, Callaghan WM, Berg C, et al. Trends in postpartum hemorrhage in high resource countries: a review and recommendations from the International Postpartum Hemorrhage Collaborative Group. BMC Pregnancy Childbirth. 2009;9:55. | ||
Cheung WM, Hawkes A, Ibish S, Weeks AD. The retained placenta: historical and geographical rate variations. J Obstet Gynaecol. 2011;31(1):37–42. | ||
AbouZahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67:1–11. | ||
Mousa HA, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev. 2007;(1):CD003249. | ||
Karoshi M, Keith L. Challenges in managing postpartum hemorrhage in resource-poor countries. Clin Obstet Gynecol. 2009;52(2):285–298. | ||
Candio F, Hofmeyr G. Treatments for Iron-Deficiency Anaemia in Pregnancy: RHL Commentary. The WHO Reproductive Health Library. Geneva: World Health Organization (WHO); 2007. | ||
Frass KA. Postpartum hemorrhage is related to the hemoglobin levels at labor: observational study. Alexandria J Med. 2015;51(4):333–337. | ||
Sanghvi TG, Harvey PW, Wainwright E. Maternal iron-folic acid supplementation programs: evidence of impact and implementation. Food Nutr Bull. 2010;31(2 suppl):S100–S107. | ||
Kalaivani K. Prevalence & consequences of anaemia in pregnancy. Indian J Med Res. 2009;130(5):627–633. | ||
Sloan NL, Durocher J, Aldrich T, Blum J, Winikoff B. What measured blood loss tells us about postpartum bleeding: a systematic review. BJOG. 2010;117(7):788–800. | ||
Zhang W-H, Deneux-Tharaux C, Brocklehurst P, et al; EUPHRATES Group. Effect of a collector bag for measurement of postpartum blood loss after vaginal delivery: cluster randomised trial in 13 European countries. BMJ. 2010;340:c293. | ||
Prata N, Gerdts C. Measurement of postpartum blood loss. BMJ. 2010;340:c555. | ||
Sheldon WR, Blum J, Vogel JP, et al; WHO Multicountry Survey on Maternal and Newborn Health Research Network. Postpartum haemorrhage management, risks, and maternal outcomes: findings from the World Health Organization multicountry survey on maternal and newborn health. BJOG. 2014;121(suppl 1):5–13. | ||
Weeks A. The prevention and treatment of postpartum haemorrhage: what do we know, and where do we go to next? BJOG. 2015;122(2):202–210. | ||
Smith JM, Gubin R, Holston MM, Fullerton J, Prata N. Misoprostol for postpartum hemorrhage prevention at home birth: an integrative review of global implementation experience to date. BMC Pregnancy Childbirth. 2013;13:44. | ||
Blum J, Alfirevic Z, Walraven G, Weeks A, Winikoff B. Treatment of postpartum hemorrhage with misoprostol. Int J Gynaecol Obstet. 2007;99(suppl 2):S202–S205. | ||
International Conferation of Midwives (ICM) and International Federation of Gynaecology and Obstetrics (FIGO). Prevention and Treatment of Post-partum Haemorrhage: New Advances for Low Resource Settings. Joint Statement by ICM and FIGO. The Hague and London: ICM and FIGO; 2006. | ||
American Congress of Obstetricians and Gynecologists (ACOG) Committee on Practice Bulletins. ACOG Practice Bulletin. Clinical Management Guidelines for Obstetrician-Gynecologists. Number 76. Postpartum Hemorrhage. Washington, DC: ACOG; 2006. | ||
Royal College of Obstetricians and Gynaecologists. Green-top Guideline No 52. Prevention and Management of Postpartum Haemorrhage. London: RCOG; 2009. | ||
International Federation of Gynecology, Obstetrics. Treatment of postpartum hemorrhage with misoprostol. Int J Gynecol Obstet. 2012;119(3):215–216. | ||
Mousa HA, Blum J, Abou El Senoun G, Shakur H, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev. 2014;2:Cd003249. | ||
World Health Organization (WHO). Executive Summary: The Selection and Use of Essential Medicines (2015). Report of the 20th WHO Expert Committee on the Selection and Use of Essential Medicines. Geneva: WHO; 2015. | ||
Hofmeyr GJ, Walraven G, Gulmezoglu AM, Maholwana B, Alfirevic Z, Villar J. Misoprostol to treat postpartum haemorrhage: a systematic review. BJOG. 2005;112(5):547–553. | ||
Lokugamage AU, Sullivan KR, Niculescu I, et al. A randomized study comparing rectally administered misoprostol versus Syntometrine combined with an oxytocin infusion for the cessation of primary post partum hemorrhage. Acta Obstet Gynecol Scand. 2001;80(9):835–839. | ||
Hofmeyr GJ, Ferreira S, Nikodem VC, et al. Misoprostol for treating postpartum haemorrhage: a randomized controlled trial [ISRCTN72263357]. BMC Pregnancy Childbirth. 2004;4(1):16. | ||
Walraven G, Dampha Y, Bittaye B, Sowe M, Hofmeyr J. Misoprostol in the treatment of postpartum haemorrhage in addition to routine management: a placebo randomised controlled trial. BJOG. 2004;111(9):1014–1017. | ||
Zuberi NF, Durocher J, Sikander R, Baber N, Blum J, Walraven G. Misoprostol in addition to routine treatment of postpartum hemorrhage: a hospital-based randomized-controlled trial in Karachi, Pakistan. BMC Pregnancy Childbirth. 2008;8:40. | ||
Blum J, Winikoff B, Raghavan S, et al. Treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women receiving prophylactic oxytocin: a double-blind, randomised, non-inferiority trial. Lancet. 2010;375(9710):217–223. | ||
Winikoff B, Dabash R, Durocher J, et al. Treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women not exposed to oxytocin during labour: a double-blind, randomised, non-inferiority trial. Lancet. 2010;375(9710):210–216. | ||
Widmer M, Blum J, Hofmeyr GJ, et al. Misoprostol as an adjunct to standard uterotonics for treatment of post-partum haemorrhage: a multicentre, double-blind randomised trial. Lancet. 2010;375(9728):1808–1813. | ||
Prata N, Mbaruku G, Campbell M, Potts M, Vahidnia F. Controlling postpartum hemorrhage after home births in Tanzania. Int J Gynaecol Obstet. 2005;90(1):51–55. | ||
Baruah M, Cohn GM. Efficacy of rectal misoprostol as second-line therapy for the treatment of primary postpartum hemorrhage. J Reprod Med. 2008;53(3):203–206. | ||
Okonofua FE, Ogu RN, Akuse JT, Ujah IA, Galadanci HS, Fabamwo AO. Assessment of sublingual misoprostol as first-line treatment for primary post-partum hemorrhage: results of a multicenter trial. J Obstet Gynaecol Res. 2014;40(3):718–722. | ||
Elati A, Weeks A. Misoprostol for the management of postpartum haemorrhage. BMJ. 2011;342:d2877. | ||
Conde-Agudelo A, Nieto A, Rosas-Bermudez A, Romero R. Misoprostol to reduce intraoperative and postoperative hemorrhage during cesarean delivery: a systematic review and meta-analysis. Am J Obstet Gynecol. 2013;209(1):40.e41–40.e17. | ||
Chaudhuri P, Majumdar A. Sublingual misoprostol as an adjunct to oxytocin during cesarean delivery in women at risk of postpartum hemorrhage. Int J Gynaecol Obstet. 2015;128(1):48–52. | ||
Ugwu IA, Enabor OO, Adeyemi AB, Lawal OO, Oladokun A, Olayemi O. Sublingual misoprostol to decrease blood loss after caesarean delivery: a randomised controlled trial. J Obstet Gynaecol. 2014;34(5):407–411. | ||
Grillo-Ardila CF, Ruiz-Parra AI, Gaitan HG, Rodriguez-Malagon N. Prostaglandins for management of retained placenta. Cochrane Database Syst Rev. 2014;(5):CD010312. | ||
Prata N, Bell S, Weidert K. Prevention of postpartum hemorrhage in low-resource settings: current perspectives. Int J Womens Health. 2013;5:737–752. | ||
Oladapo OT, Fawole B, Blum J, Abalos E. Advance misoprostol distribution for preventing and treating postpartum haemorrhage. Cochrane Database Syst Rev. 2012;2:Cd009336. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.