")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Efficacy of Eye Movement Desensitization and Reprocessing on the Quality of Life in Patients with Major Depressive Disorder: A Randomized Clinical Trial
Authors Jahanfar A , Fereidouni Z , Behnammoghadam M, Dehghan A , Bashti S
Received 26 September 2019
Accepted for publication 24 December 2019
Published 8 January 2020 Volume 2020:13 Pages 11—17
DOI https://doi.org/10.2147/PRBM.S232589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Abdolhadi Jahanfar,1 Zhila Fereidouni,2 Mohammad Behnammoghadam,1 Azizallah Dehghan,3 Somayeh Bashti1
1Social Determinants of Health Research Center, Yasuj University of Medical Sciences, Yasuj, Iran; 2Department of Medical Surgical Nursing, Nursing School, Fasa University of Medical Sciences, Fasa, Fars, Iran; 3Noncommunicable Diseases Research Center, Fasa University of Medical Sciences, Fasa, Iran
Correspondence: Zhila Fereidouni
Department of Medical Surgical Nursing, Nursing School, Fasa University of Medical Sciences, Fasa, Fars, Iran
Email [email protected]
Mohammad Behnammoghadam
Department of Critical Care Nursing, Yasuj University of Medical Sciences, Yasuj, Iran
Email [email protected]
Introduction: The present study was conducted with the aim of investigating the efficacy of eye movement desensitization and reprocessing (EMDR) on the quality of life (QOL) in patients with major depressive disorder (MDD).
Methods: This is a randomized clinical trial study that investigated the efficacy of EMDR on the QOL in patients with MDD. In this study, all patients suffered from psychological trauma were currently in a major depressive episode and had a history of depression. 70 patients with MDD were selected through convenience sampling. Patients were then assigned to two groups of intervention and control (35 patients in each group). The assignment was performed randomly. For the intervention group, EMDR were performed in eight 90 mins sessions over 3 weeks. For the control group, no intervention was considered. Data on the QOL were collected using the WHO Quality of Life-BREF instrument before and after the treatment, and analysed using descriptive tests, paired t-test, independent t-test, and chi-square with SPSS v19.
Results: This study showed that the QOL in all its domains (physical health, psychological health, social relationships and environments) was significantly improved in patients with MDD in the intervention group after 8 sessions of EMDR. The post-treatment effect for the EMDR condition was 2.11, with a confidence interval of 1.3 to 2.7. Another finding of this study was that there was a statistically significant difference in the QOL scores in patients in the control group before and after the treatment; however, the mean difference in the intervention group was more than the control.
Conclusion: The results of this study showed that EMDR were effective on the QOL in patients with major depressive disorder, and improved individuals’ QOL and all its domains. Treatment team members may use this technique as an effective and supportive one to improve the QOL in patients.
Keywords: major depressive disorder, quality of life, eye movement desensitization and reprocessing
Introduction
Major depressive disorder is a debilitating disease characterized by symptoms including low mood, sadness, loss of interest, low energy, guilt, worthlessness, changes in appetite and sleep patterns, inability to concentrate, and poor quality of life.1 The prevalence of major depressive disorder throughout the world is generally estimated at 3% to 6%,2,3 and the prevalence of this disorder in Iran is reported to range from 5.69% to 73.3%.4
Depression is a strong predictor of impaired quality of life in adults.5,6 The results of previous studies suggested that even mild levels of depression are associated with a significant decrease in quality of life in adults.7 Several studies have also confirmed that major depressive disorder results in impaired quality of life in depressed patients.8 Depressed people have poorer quality of life due to the distresses resulting from negative thoughts and low mood.9 As an important factor, depression can have negative influences on individuals’ quality of life.10,11 Measuring the quality of life in depressed patients is considered a criterion for the efficacy of treatment or relapse of the disorder.12 World Health Organization defines quality of life as an individual’s perception of their position in life in the context of the culture and value systems in which they live. Accordingly, individual’s goals, expectations, standards, and desires are greatly influenced by his/her physical and psychological status, independence, social relationships, and beliefs13.
In one study by Sobocki et al on the quality of life in patients with major depressive disorder, the results showed that it improved by 40% after recovery.14 For depression, both pharmacological and non-pharmacological treatments were used. Although drug therapy applies for all of the patients, about 20% of patients do not follow it, and some patients, who start it, do not complete the treatment.15 Many antidepressants are currently available in the market. In recent years, selective serotonin reuptake inhibitors (SSRIs) have been the first-line therapy for these disorders.16 These drugs are associated with side effects that increase suicidal thoughts and behaviors, and symptoms are likely to return after withdrawal. Thus, the US Food and Drug Administration has warned physicians about the side effects.17 They emphasize on the use of inexpensive, and non-invasive methods. Some studies suggested that patients prefer psychotherapy, cognitive therapy, and behavior therapy over drug therapy.18,19 One of the new techniques is the eye movement desensitization and reprocessing (EMDR), in which the therapist asks the patient to recall disturbing memories as they move their eyes, and as a result, the level of arousal is reduced and thoughts are reorganized.4
EMDR therapy is an empirically validated trauma intervention which can be effective in treating psychological trauma.4 The results of Gauhar YW (2016) study on the efficacy of EMDR in the treatment of depression showed that this technique was effective in treating depressive symptoms in patients with major depressive disorder, and improved their quality of life and unpleasant thoughts.20
Another study was conducted by Salehian et al (2016) that investigated the efficacy of EMDR on the quality of life in patients with myocardial infarction. For the intervention group, the technique was performed in five 90 mins sessions over 2 weeks. The results showed that the quality of life in all its domains was significantly improved in patients in the intervention group compared to the control (p= 0.001).21 Since the treatment of depression has been associated with improved quality of life in these patients, special attention needs to be paid to individuals’ psychological health and appropriate therapeutic measures.22
Therefore, most patients with major depressive disorder have low quality of life, which may delay the return to work and lower the quality of life. However, and treatment of depression and improvement in the quality of life will accelerate recovery, increase life expectancy and reduce economic burden.
Depression affects individuals’ quality of life, and the results of previous studies have confirmed the inverse relationship between depression and the quality of life. Since EMDR is considered an effective therapeutic technique, its effects on the quality of life have not been comprehensively studied. Therefore, the present study was conducted with the aim of investigating the efficacy of EMDR on the quality of life in patients with major depressive disorder.
Methods
The study population of this randomized controlled trial includes all patients with MDD referring to a hospital in Yasuj City.
This is a randomized clinical trial study conducted at Shahid Rajaee Neurology Hospital in Yasuj, in 2018 (Figure 1: consort flow chart). The study was conducted after obtaining the written informed consent and permission from the Ethics Committee of Yasuj University of Medical Sciences (ethics code: ir.yums.rec.1397.074), and giving full explanation to participants on patient confidentiality and EMDR acceptance and this study was conducted in accordance with the Declaration of Helsinki and The researcher assured all the study participants that they were free to withdraw from the study at any stage.
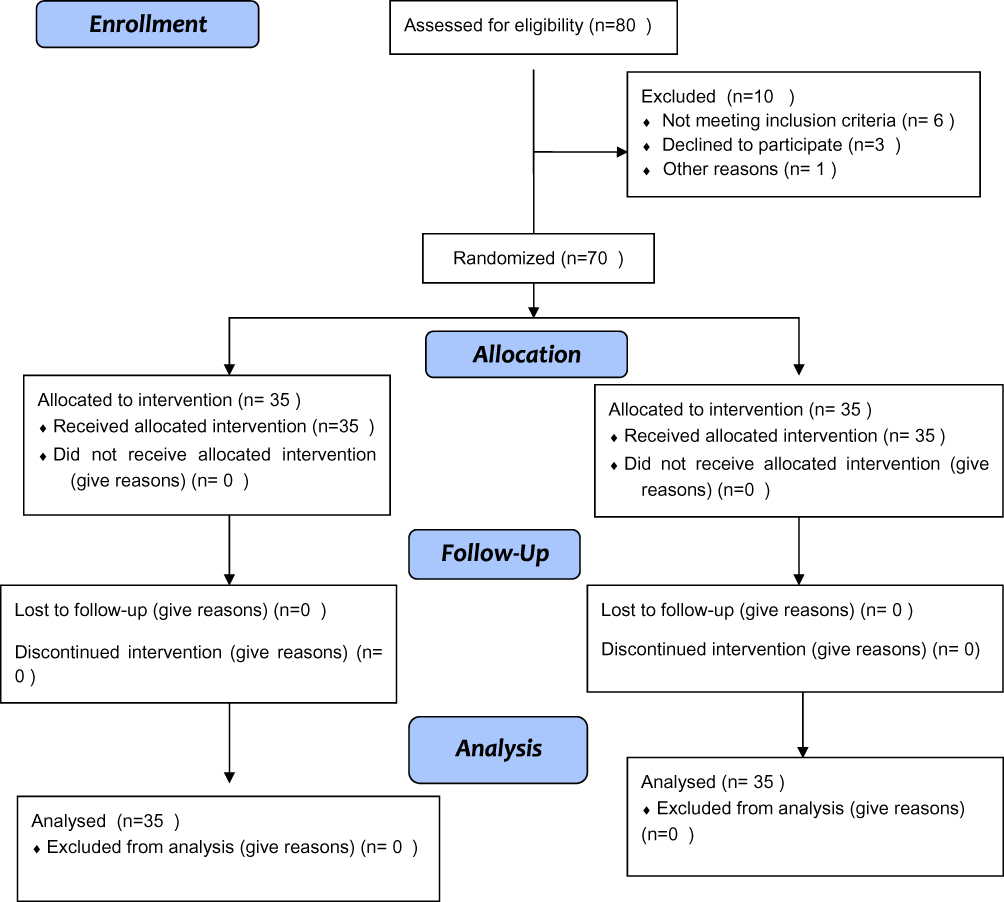 |
Figure 1 Consort Flow Diagram. |
They participated in this study voluntarily and were selected from those with major depressive disorder as diagnosed by a psychiatrist (based on DSM-5 criteria), through convenience sampling. All patients suffered from psychological trauma were currently in a major depressive episode and had a history of depression.
Patients were divided into two groups according to the variables of age, sex, education and type of drug used, and they were then assigned to two groups of intervention and control (35 patients in intervention group, and 35 in the control one) according to random number table (couple or person on the right of the case number).
To determine the sample size, the sample size formula was used to test the difference between the following two means.
Considering the above, the estimated sample size was 35 patients in each group. Patients who had major depressive disorder according to DSM-5 criteria had the ability to read and write, and had no visual disorders, and those whose quality of life score was below the average were included in the study. Exclusion criteria comprised of patients’ not completing the treatment, lack of cooperation with the researcher, being transferred to another hospital, and being absent in the treatment sessions.
Data collection was performed through a checklist for demographic information and a questionnaire on the quality of life questionnaire. The demographic information checklist was comprised of items about patients’ age, sex, education, economic status, marital status, and occupation that was designed by the researcher.
Data on the quality of life were collected using the WHO Quality of Life-BREF instrument. This instrument was comprised of 26 items, which measure the following broad domains: physical health, psychological health, social relationships, and environment. Higher score indicates better quality of life, and the reliability of the instrument is 92% and its validity is 86%.
The patients’ demographic information checklist was completed by the researcher in the first session in two groups. The therapeutic technique was performed by experienced researcher in field of EMDR for each patient in the intervention group individually every other day, over a period of 3 weeks for 8 sessions of 90 mins (According to the protocol, EMDR shows its positive effect through 1 session to 6 sessions). In the first and last sessions of the intervention, the quality of life questionnaire was completed by an independent researcher who was blind to treatment assessment.
All patients in the intervention group were treated with EMDR and there was no dropout during the intervention.
For the control group, no intervention was considered, and only their quality of life in its different domains was measured at the first session and at the end of the third week. All patients were treated with antidepressants such as Fluoxetine, Amitriptyline and Maprotiline. After completing the research process and data collection, data were entered into SPSS v19 for data analysis. Descriptive statistics demonstrated demographic variables, and chi-square test, paired t-test, independent t-test and Logistic Regression were run to compare data.
Results
A total of 70 patients participated in this study, 35 of whom were in the intervention group and 35 in the control group. Patients’ mean age in the intervention group was 35.94±12.29 and in control group, it was 36.51±11.07. According to the results of independent t-test, there was no significant difference between the two groups.
Table 1 shows the distribution of possible confounding variables, namely sex, marital status, residence, education, occupation and economic status in the two groups of intervention and control. As can be seen, the distribution of the mentioned variables was not significantly different between the two groups (p> 0.05).
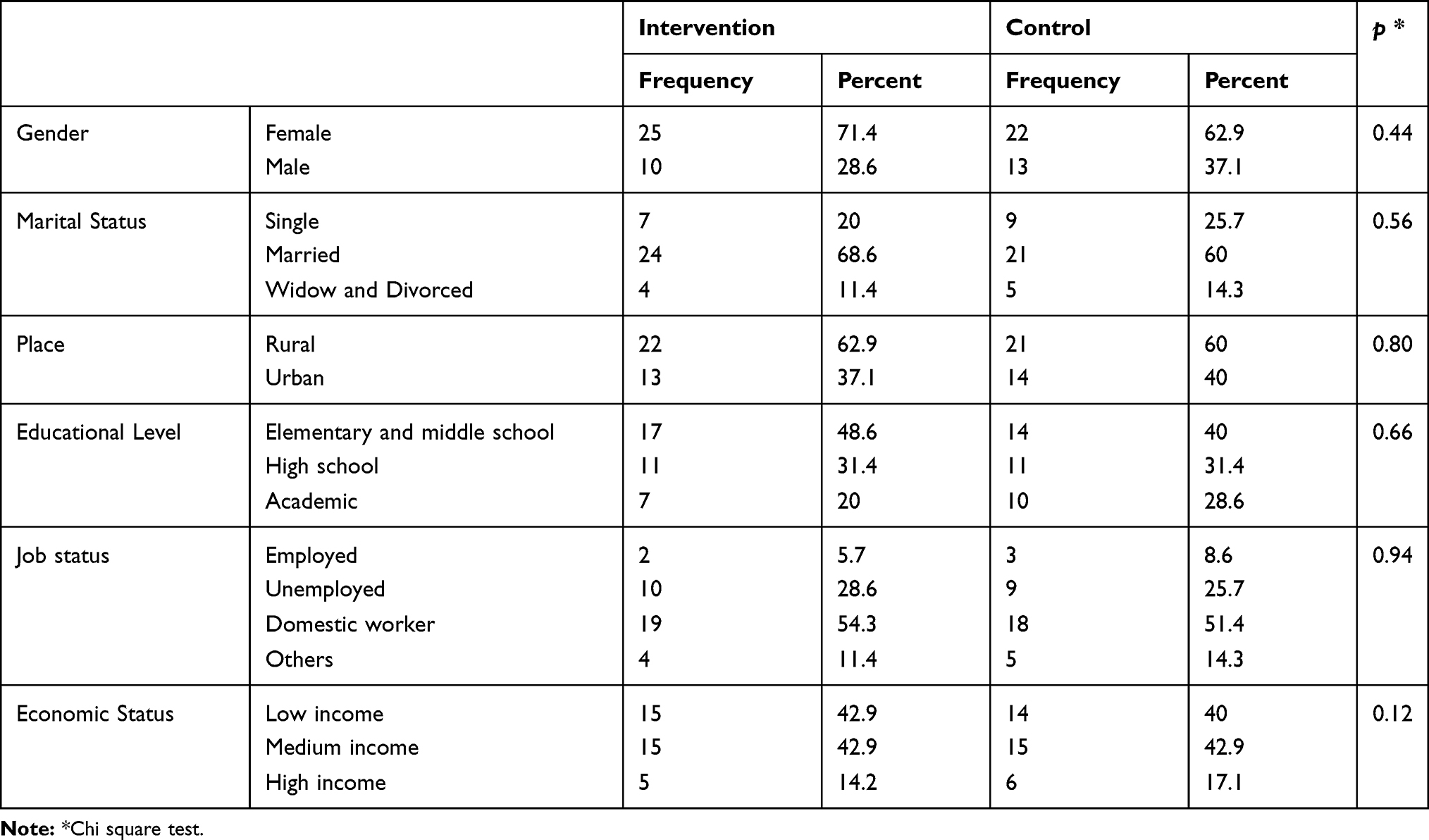 |
Table 1 Comparison of the Distribution of Sex, Marital Status, Residence, Education, Occupation and Economic Status Between the Intervention and Control Groups |
Table 2 shows the mean and standard deviation of the quality of life scores in all its domains (physical health, psychological health, social relationships and environments) in the two groups of intervention and control. As can be seen, no significant difference was observed between the two groups before the intervention regarding the mean score of the quality of life. However, the difference between the two groups was statistically significant after the intervention. The results of paired t-test also showed that the quality of life scores in all its domains were significantly increased in both groups after the intervention. However, the mean difference in the intervention group was significantly greater than the control group. The post-treatment effect for the EMDR condition was 2.11, with a confidence interval of 1.3 to 2.7. The largest increase occurred in the domains of physical and psychological health, and the lowest in the environment.
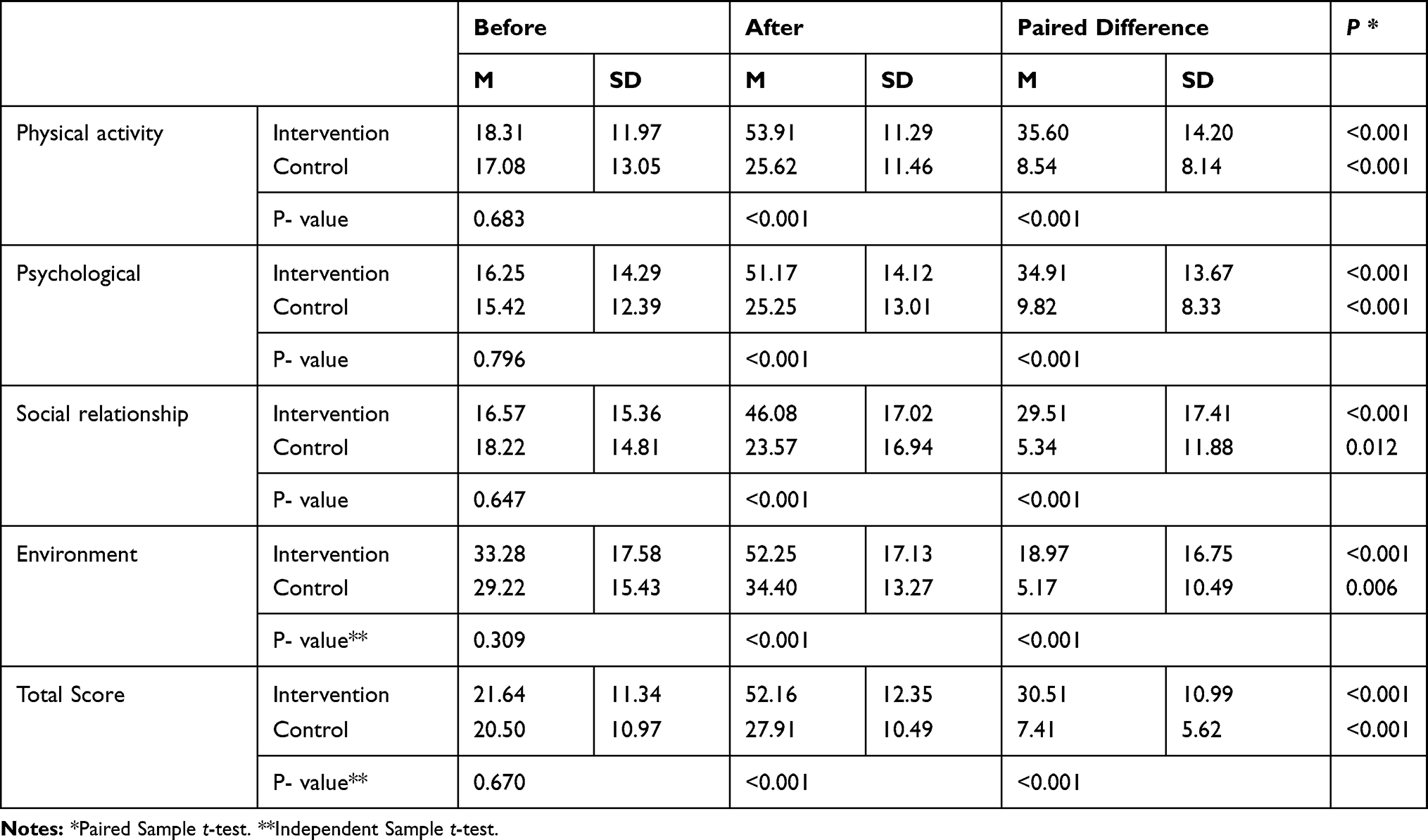 |
Table 2 Comparison of the Mean Scores of the Quality of Life and All Its Domains Among the Intervention and Control Groups Before and After the Intervention as Well as Inter-Group Comparison of the Mean Score of Quality of Life (Before and After Intervention for Each Group) |
Table 3 shows that the chances of elevating the quality of life after intervention in the intervention group were higher in all dimensions and the overall score than the control group.
 |
Table 3 The Effect of Eye Movement Desensitization and Reprocessing on the Quality of Life in Patients with Major Depressive Disorder in Intervention Group Compared to the Control Group |
Overall, the chances of improving the quality of life in the intervention group were 20%, 27%, 11%, 20%, and 47% more than the control in physical, psychological, social environment and overall score, respectively.
Discussion
The present study was conducted with the aim of investigating the efficacy of EMDRon the quality of life in patients with major depressive disorder.
The results of this study showed that the quality of life in all its domains (physical health, psychological health, social relationships and environments) was significantly improved in patients with major depressive disorder in the intervention group after 8 sessions of EMDR. Therefore, the above technique has demonstrated the ability to improve the quality of life in depressed patients. On the other hand, the results of this study in the control group showed that there was a statistically significant difference in the quality of life before and after the intervention; however, the mean difference in the intervention group was more than the control.
Surprisingly, the mean scores of different domains of the quality of life in the control group had a significant increase. The mean difference in different domains of the quality of life in the control group was not significant compared to the intervention group. This slight increase in the quality of life in patients in the control group may be due to a number of reasons, including using antidepressants, and the patients’ personal and spiritual beliefs.
By comparing the mean scores of the quality of life before and after the intervention between the two groups of intervention and control, we can confirm the efficacy of EMDR in improving the quality of life in patients in the intervention group. Therefore, the findings of this study confirmed that EMDR is effective in improving the quality of life in patients with major depressive disorder.
In a study by Kao et al (2018), on the efficacy of EMDR on depression symptoms, quality of life, and heart rate variability in patients with heart failure, the results showed that EMDR improved depression symptoms and the quality of life in these patients,23 which confirms and is consistent with the results of the present study.23 Thus, EMDR can be employed as an effective and supportive technique to improve the quality of life in patients.
Gauhar et al (2016) conducted a study on the efficacy of EMDR in the treatment of 26 depressed patients. The aim of this study was to determine whether EMDR can reduce depression symptoms and improve the quality of life in patients. The results showed that the depression symptoms and trauma were decreased in these patients and their quality of life was improved after EMDR. Consequently, EMDR can be considered an effective and supportive technique along with other techniques for depressed patients. In the mentioned study, the sample size was small and the results could not be generalized to the overall population.20 The results of one review study in 2007 showed that the above technique improves the quality of life in patients with depressive disorder, and EMDR shows its efficacy after a 3- to 6-month follow-up, which is in line with the results of the present study.
In another study by Raboni et al (2014), the efficacy of EMDR was investigated on mood, anxiety, and sleep changes in patients with post-traumatic stress disorder. The results showed that EMDR improved sleep, quality of life, and reduced depression and anxiety symptoms in these patients,24 which confirms its consistency with the results of the present study.
Raboni et al (2006) conducted a study to investigate the efficacy of EMDR on PTSD symptoms including sleep disorders, depression, anxiety and the poor quality of life in Brazil. Seven patients were enrolled, including 2 men and 5 women, who completed high school. EMDR sessions were held once a week for 30 to 90 mins, and the average EMDR sessions were 5 sessions. In general, the results of this study showed that EMDR led to a reduction in depression, anxiety, fatigue, stress symptoms, and improved the quality of life, sleep quality, and general wellbeing,25 which is consistent with the results of the present study.
This technique reduces symptoms faster than other cognitive behavioral techniques and requires fewer sessions (3 to 6 sessions). Rapid improvement of patients’ symptoms and return to their independent function is based on the information processing model, which states that feelings of helplessness and hopelessness are the result of unprocessed trauma memories, which contain perceptions experienced at the time of the accident.26 On the other hand, the eye movements used in EMDR appear to rapidly activate the parasympathetic nervous system and reduce the physiological symptoms.21
When adaptive reprocessing occure as a result of EMDR, traumatic events are desensitized and cognitively reconstructed in an adaptive manner.27
Conclusions
The results of this study showed that EMDR were effective on the quality of life in patients with major depressive disorder, and improved individuals’ quality of life and all its domains. Treatment team members can employ this effective and supportive technique to improve the quality of life in patients.
One limitation of this study was that all patients used drug therapy that might have influenced the results of the study, which was not under the researcher’s control. Another limitation was that we could not evaluate affective/trauma symptoms.
Data Sharing Statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymized data may be granted following review.
Acknowledgments
We would like to sincerely appreciate the cooperation of all officials of Nursing department of Yasuj, and participating patients, without which this study could not be completed.
Disclosure
The authors declare that there is no conflict of interests regarding the publication of this study.
References
1. Organization WH. Global Status Report on Alcohol and Health 2018. World Health Organization; 2019.
2. Bromet E, Andrade LH, Hwang I, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9(1):90. doi:10.1186/1741-7015-9-90
3. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Lippincott Williams & Wilkins; 2011.
4. Fereidouni Z, Behnammoghadam M, Jahanfar A, Dehghan A. The effect of Eye Movement Desensitization and Reprocessing (EMDR) on the severity of suicidal thoughts in patients with major depressive disorder: a randomized controlled trial. Neuropsych Dis Treat. 2019;15.
5. da Silva Lima AFB, de Almeida Fleck MP. Subsyndromal depression: an impact on quality of life? J Affect Disord. 2007;100(1–3):163–169. doi:10.1016/j.jad.2006.10.010
6. Stafford L, Berk M, Reddy P, Jackson HJ. Comorbid depression and health-related quality of life in patients with coronary artery disease. J Psychosom Res. 2007;62(4):401–410. doi:10.1016/j.jpsychores.2006.12.009
7. Chachamovich E, Fleck M, Laidlaw K, Power M. Impact of major depression and subsyndromal symptoms on quality of life and attitudes toward aging in an international sample of older adults. Gerontologist. 2008;48(5):593–596. doi:10.1093/geront/48.5.593
8. Cotrena C, Branco LD, Kochhann R, Shansis FM, Fonseca RP. Quality of life, functioning and cognition in bipolar disorder and major depression: a latent profile analysis. Psychiatry Res. 2016;241:289–296. doi:10.1016/j.psychres.2016.04.102
9. IsHak WW, Greenberg JM, Balayan K, et al. Quality of life: the ultimate outcome measure of interventions in major depressive disorder. Harv Rev Psychiatry. 2011;19(5):229–239. doi:10.3109/10673229.2011.614099
10. Schowalter M, Gelbrich G, Störk S, et al. Generic and disease-specific health-related quality of life in patients with chronic systolic heart failure: impact of depression. Clin Res Cardiol. 2013;102(4):269–278. doi:10.1007/s00392-012-0531-4
11. Hallas CN, Wray J, Andreou P, Banner NR. Depression and perceptions about heart failure predict quality of life in patients with advanced heart failure. Heart Lung. 2011;40(2):111–121. doi:10.1016/j.hrtlng.2009.12.008
12. Jha MK, Greer TL, Grannemann BD, Carmody T, Rush AJ, Trivedi MH. Early normalization of quality of life predicts later remission in depression: findings from the CO-MED trial. J Affect Disord. 2016;206:17–22. doi:10.1016/j.jad.2016.07.012
13. Davidson P, Stewart S, Elliott D, Daly J, Sindone A, Cockburn J. Addressing the burden of heart failure in Australia: the scope for home-based interventions. J Cardiovasc Nurs. 2001;16(1):56–68.
14. Sobocki P, Ekman M, Ågren H, Runeson B, Jönsson B. The mission is remission: health economic consequences of achieving full remission with antidepressant treatment for depression. Int J Clin Pract. 2006;60(7):791–798. doi:10.1111/j.1742-1241.2006.00997.x
15. Amick HR, Gartlehner G, Gaynes BN, et al. Comparative benefits and harms of second generation antidepressants and cognitive behavioral therapies in initial treatment of major depressive disorder: systematic review and meta-analysis. BMJ. 2015;351:h6019. doi:10.1136/bmj.h6019
16. Bandelow B, Andersen HF, Dolberg OT. Escitalopram in the treatment of anxiety symptoms associated with depression. Depress Anxiety. 2007;24(1):53–61. doi:10.1002/da.20141
17. Hammad TA, Laughren T, Racoosin J. Suicidality in pediatric patients treated with antidepressant drugs. Arch Gen Psychiatry. 2006;63(3):332–339. doi:10.1001/archpsyc.63.3.332
18. McHugh RK, Whitton SW, Peckham AD, Welge JA, Otto MW. Patient preference for psychological vs. pharmacological treatment of psychiatric disorders: a meta-analytic review. J Clin Psychiatry. 2013;74(6):595. doi:10.4088/JCP.12r07757
19. Zakerimoghadam M, Shaban M, Mehran A, Hashemi S. Effect of muscle relaxation on anxiety of patients undergo cardiac catheterization. Hayat. 2010;16(2).
20. Gauhar YW. The efficacy of EMDR in the treatment of depression. J EMDR Pract Res. 2016;10(2):59–69. doi:10.1891/1933-3196.10.2.59
21. Salehian T, Saeedinejad S, Behnammoghadam M, et al. Efficacy of eye movements desensitization and reprocessing on the quality of life of the patients with myocardial infarction. Glob J Health Sci. 2016;8(10):56100. doi:10.5539/gjhs.v8n10p112
22. Skevington SM, Lotfy M, O’Connell K. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310. doi:10.1023/B:QURE.0000018486.91360.00
23. Kao C-W, Cheng S-M, Wan F-J, Lin W-S, Chang Y-C. Eye movement desensitization and reprocessing improves depressive symptoms, quality of life, and heart rate variability in patients with heart failure. Neuropsychiatry (London). 2018;8(3):1073–1082.
24. Raboni MR, Alonso FF, Tufik S, Suchecki D. Improvement of mood and sleep alterations in posttraumatic stress disorder patients by eye movement desensitization and reprocessing. Front Behav Neurosci. 2014;8:209. doi:10.3389/fnbeh.2014.00209
25. Raboni MR, Tufik S, Suchecki D. Treatment of PTSD by eye movement desensitization reprocessing (EMDR) improves sleep quality, quality of life, and perception of stress. Ann N Y Acad Sci. 2006;1071(1):508–513. doi:10.1196/annals.1364.054
26. Shapiro F. Getting Past Your Past: Take Control of Your Life with Self-Help Techniques from EMDR Therapy. Rodale; 2012.
27. Zeighami R, Behnammoghadam M, Moradi M, Bashti S. Comparison of the effect of eye movement desensitization reprocessing and cognitive behavioral therapy on anxiety in patients with myocardial infarction. Eur J Psychiatry. 2018;32(2):72.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.