")
Back to Journals » Cancer Management and Research » Volume 13
Efficacy of Drug-Eluting Beads Transarterial Chemoembolization Plus Apatinib Compared with Conventional Transarterial Chemoembolization Plus Apatinib in the Treatment of Unresectable Hepatocellular Carcinoma
Authors Zhang W , Chen L , Cao Y , Sun B, Ren Y, Sun T , Zheng C
Received 8 April 2021
Accepted for publication 23 June 2021
Published 6 July 2021 Volume 2021:13 Pages 5391—5402
DOI https://doi.org/10.2147/CMAR.S314762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Weihua Zhang,1– 3,* Lei Chen,1– 3,* Yanyan Cao,1– 3,* Bo Sun,1– 3 Yanqiao Ren,1– 3 Tao Sun,1– 3 Chuansheng Zheng1– 3
1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 2Hubei Province Key Laboratory of Molecular Imaging, Wuhan, 430022, People’s Republic of China; 3Department of interventional radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuansheng Zheng
Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
Tel +86 027-85726432
Email [email protected]
Objective: The aim of the study was to compare the efficacy and safety of drug-eluting beads TACE plus apatinib (D-TACE-A) with those of conventional TACE plus apatinib (C-TACE-A) for the treatment of unresectable HCC.
Methods: We retrospectively reviewed 187 consecutive patients who received TACE plus apatinib in our institution from January 1, 2017, to July 1, 2019. Among them, 91 patients received C-TACE-A, and 96 patients received D-TACE-A. The primary endpoint was overall survival (OS), and the secondary endpoints were progression-free survival (PFS) and disease control rate (DCR). Propensity score matching (PSM) was used to reduce selection bias.
Results: Before PSM, the median OS was 15 months (95% CI: 12.5– 17.5) and 13 months (95% CI: 11.1– 14.9; P=0.480) in the C-TACE-A and D-TACE-A groups, respectively. The median PFS was 7 months (95% CI: 5.9– 8.1) in the C-TACE-A group and 7 months (95% CI: 5.6– 8.4; p=0.677) in the D-TACE-A group. The DCR was 81.3% in the C-TACE-A group and 72.9% in the D-TACE-A group. Cox regression analysis showed that D-TACE-A did not increase mortality risk or tumor recurrence risk. After PSM, there was no statistically significant difference in median OS or PFS between the two groups. In the subgroup analysis, after adjusting for relative factors, D-TACE-A increased the mortality risk more than C-TACE-A in patients with BCLC stage C (HR: 1.678, 95% CI: 1.129– 2.495; P=0.011), but D-TACE-A lowered the tumor recurrence risk compared with C-TACE-A in patients with Child–Pugh B (HR: 0.210, 95% CI: 0.082– 0.538; P=0.001) and cirrhosis (HR: 0.481, 95% CI: 0.293– 0.791; P=0.004). Grade III and IV adverse events in patients with D-TACE-A were similar to those in patients treated with C-TACE-A (P> 0.05).
Conclusion: Patients with unresectable HCC treated with D-TACE-A might not show increased survival compared with patients treated with C-TACE-A. Advanced HCC patients without cirrhosis may receive greater survival benefits from C-TACE-A than D-TACE-A.
Keywords: hepatocellular carcinoma, drug-eluting beads transarterial chemoembolization, conventional transarterial chemoembolization, apatinib, efficacy
Introduction
Hepatocellular carcinoma (HCC) is one of the most common and fatal cancers in the world.1 Because the early stages are asymptomatic, HCC is usually diagnosed at the intermediate or advanced stage; therefore, only a few patients with HCC are candidates for liver resection or transplantation.
Transcatheter arterial chemoembolization (TACE) is the recommended first-line treatment for intermediate HCC according to the European Association for the Study of the Liver (EASL) guideline.2 Conventional TACE (C-TACE) kills tumors through the intra-arterial injection of lipiodol containing chemotherapeutic drugs and the subsequent embolization of the feeding artery, leading to a combination of cytotoxicity and ischemia.3 However, the technique has some disadvantages. For example, the injection of chemotherapeutic drugs and embolic materials is not synchronous, and lipiodol releases chemotherapeutic drugs in an unsustained manner.
Recently, the use of drug-eluting beads TACE (D-TACE) was proposed in an attempt to overcome these drawbacks.4 D-TACE is a new method of chemoembolization that employs microspheres containing antineoplastic drugs that can promote more sustained drug delivery and stable embolization of tumor-feeding arteries. Previous studies demonstrated that D-TACE resulted in a better treatment response and similar survival benefits, but increased the incidence of short-term adverse events, compared with cTACE.5–7 Farid et al used vascular endothelial growth factor (VEGF) to predict the responses of patients with unresectable HCC after receiving C-TACE or D-TACE. The results showed that VEGF serum levels could predict the patients’ response to therapy with D-TACE or C-TACE, indicating that TACE combined with molecular targeted drugs might be a good combination treatment for some patients with HCC.8
Sorafenib is a multitarget kinase inhibitor approved for the treatment of advanced HCC and has been proven to suppress the growth of tumor vessels and improve median overall survival (mOS) in advanced HCC cases.9–12 Another antiangiogenic drug, Apatinib, is an inhibitor of vascular endothelial growth factor receptor-2 (VEGFR-2) that has shown high antitumor activity and a tolerable safety profile in various tumors, including HCC and gastric cancer.13–15 When combined with TACE, apatinib can improve the survival outcomes of patients with unresectable HCC.16–18 As yet, there have been few studies comparing the efficacy and safety of D-TACE with those of C-TACE when both are combined with apatinib for patients with unresectable HCC. Thus, the study was conducted to compare the efficacy and safety of patients with unresectable HCC who received C-TACE-A with those received D-TACE-A.
Materials and Methods
Patient Selection
We retrospectively reviewed the records of 315 patients who received TACE plus apatinib in our institution from January 1, 2017, to July 1, 2019. We excluded 128 patients from the analysis based on the inclusion and exclusion criteria, leaving 187 patients who were included. The study was approved by the institutional review board and local ethics committee of the institution. The informed consent of patients was waived by the institutional review board because this study was a retrospective study. This study is carried out in compliance with the Helsinki Declaration and the patient data is strictly confidential.
The inclusion criteria were as follows: (1) patients who were diagnosed as having intermediate or advanced HCC based on imaging methods or pathological examination according to the EASL guideline;2 (2) patients who did not receive TACE or molecular targeted drugs before inclusion in the study; (3) patients with Child–Pugh A or B; (4) patients with Eastern Cooperative Oncology Group (ECOG) score 0 or 1 or 2. The exclusion criteria were as follows: (1) patients with platelet counts of less than 40 × 109/L before TACE; (2) patients with diffuse HCC that could not be evaluated; (3) patients who did not receive CT, MRI, or ultrasound examination before TACE or who were checked again after discharge; (4) patients lost to follow up (Figure 1).
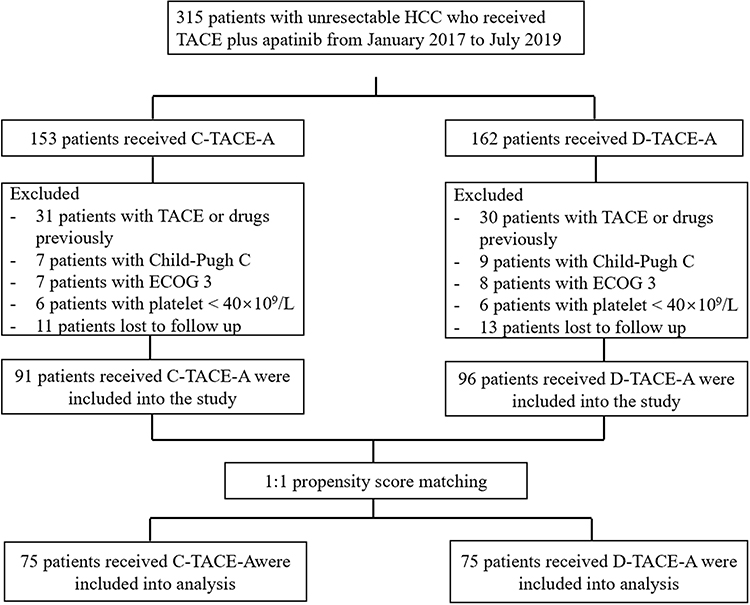 |
Figure 1 Flowchart of patient selection. |
TACE Procedures
C-TACE Procedures
Selective celiac angiography was performed to provide hepatic vascular anatomy and reconfirm the location of the tumor. Then, hepatic arteriography was conducted to identify and ultra-select the tumor-feeding artery. After that, the lipiodol (10–20 mL) and epirubicin (10–30 mg) emulsion were injected into the tumor-feeding arteries for embolization with 500–700 μm absorbable gelatin sponge particles (Alicon Medical Co., Hangzhou, China).
D-TACE Procedures
Selective celiac angiography was performed to provide hepatic vascular anatomy and reconfirm the location of the tumor. Then, hepatic arteriography was conducted to identify and ultra-select the tumor-feeding artery. CalliSphere beads (Jiangsu Hengrui Medicine Co., Ltd., China), with a diameter ranging from 100 μm to 300 μm, were used as the carriers, and epirubicin (80 mg) was used as the chemoembolization reagent. Firstly, epirubicin was dissolved to a concentration of 20 mg/mL, then mixed with the beads using a tee-joint and shaken every 5 minutes for 30 minutes. After that, the non-ionic contrast agent was added to the solution, and the mixture was subsequently injected into the tumor-feeding arteries at a rate of 1 mL/min until stasis.
Apatinib Administration
Each patient in the D-TACE-A group and C-TACE-A group received apatinib at an initial dose of 500 mg/day 3–5 days after each TACE procedure. The apatinib dose was adjusted according to each patient’s tolerance, and a dose reduction to 250 mg/day was permitted in the case of grade III/IV adverse events. If a patient could not tolerate as much as a half dose, apatinib was temporarily stopped. After the adverse events disappeared, apatinib administration was restarted at an initial dose of 250 mg/day.
Endpoints of the Study and Their Definitions
The primary endpoint of the study was overall survival (OS), which was defined to be from the time patients received TACE to patients’ death or the end of the study. The second endpoints were progression-free survival (PFS) and the disease control rate (DCR). PFS was defined as being from the time patients received TACE to the time of tumor progression, patients’ death, or the end of the study. The DCR was defined as the percentage of patients with a response rate as a complete response (CR), partial response (PR) and stable disease (SD) based on the modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria.19
Follow Up
All patients who received TACE in our institution were followed up. Patients were required to undergo a CT or MRI scan and laboratory tests for 2–3 weeks after the initial TACE, and then 2–3 months later. The tumors were evaluated by two radiologists (one with 15 years of radiographic reading experience, and another with 23 years of radiographic reading experience). When there was a residual tumor or the tumor progressed, patients were advised to receive another TACE to control the tumor. The end time of the study was December 30, 2020.
Statistical Analysis
Continuous variables were compared by an independent sample test or Mann–Whitney U-test, and categorical variables were compared by chi-squared test or Fisher’s test between the two groups. The survival curves were plotted using the Kaplan-Meier method, and the efficacy was compared by Log rank test. A Cox proportional risk model was used to exclude potential variables that might influence survival and tumor progression. The variables with P-values less than 0.05 in the univariable analysis were included in the multivariable analysis. The adjusted Cox proportional risk model was used for subgroup analysis.
To reduce selection bias, propensity score matching (PSM) was used. Before PSM, the age, tumor size, and Child–Pugh classification of patients in the two groups were unbalanced. All variables were included in the PSM analysis. We conducted 1:1 ratio matching, and the optimal caliper was set as 0.2. After PSM, 75 pairs of patients were matched, and all variables in the two groups were balanced. P-values of <0.05 in the study were considered statistically significant. All statistical analyses were conducted by SPSS 24.0 and R version 3.6.
Results
Characteristics of Patients
Patients who received TACE combined with apatinib from January 1, 2017, to July 1, 2019, in our institution were included in the study. A total of 187 patients were included, among whom, 91 received D-TACE-A and 96 received C-TACE-A. HCC was diagnosed for 63 patients by pathology. The mean age of patients was 54.3 years in the D-TACE-A group and 49.8 years in the C-TACE-A group. There were 81 male patients and 15 female patients in the D-TACE-A group, and 76 male patients and 15 female patients in the C-TACE-A group (Table 1).
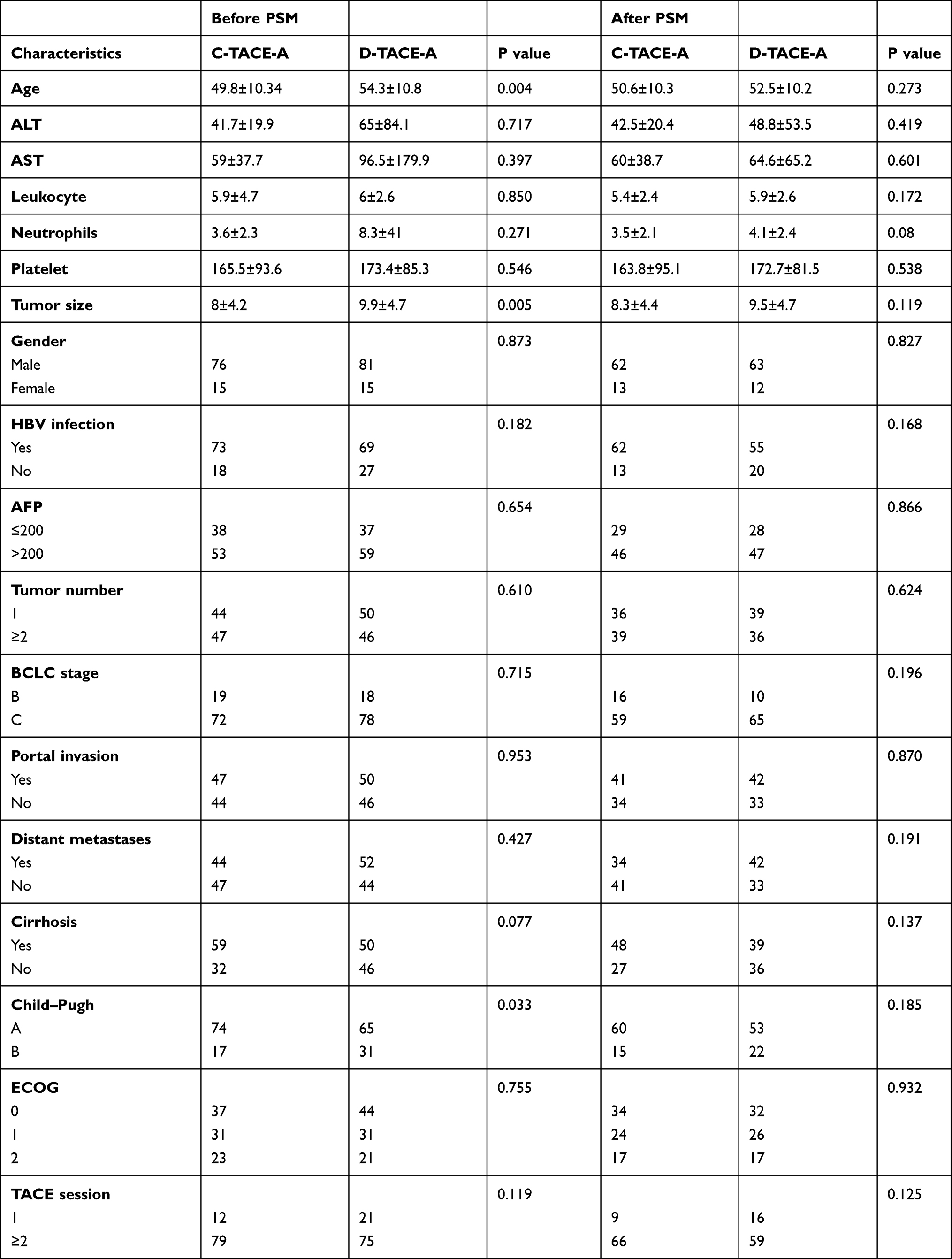 |
Table 1 The Characteristics of Patients Before and After PSM |
Survival and Tumor Response Analysis
Before PSM, the mOS and mPFS of patients in the C-TACE-A group were 13 months (95% CI: 11.1–14.9) and 7 months (95% CI: 5.6–8.4), respectively. In the D-TACE-A group, the mOS and mPFS of patients in the D-TACE-A group were 15 months (95% CI: 12.5–17.5) and 7 months (95% CI: 5.9–8.1), respectively. There were no statistically significant differences in the mOS and mPFS between patients in the C-TACE-A group and those in the D-TACE-A group (P=0.480 and P=0.677) (Figure 2). The DCR was 81.3% (74/91) in the C-TACE-A group and 72.9% (70/96) in the D-TACE-A group (P=0.160). After PSM, similar results were presented: there was no statistically significant difference in mOS (C-TACE-A vs D-TACE-A: 13 months, 95% CI: 10.5–15.5; vs 15 months, 95% CI: 12.5–17.5; P=0.149) or mPFS (C-TACE-A vs D-TACE-A: 6 months, 95% CI: 4.5–7.5; vs 7 months, 95% CI: 5.8–8.2; P=0.316) in the two groups (Figure 3). The DCR in the C-TACE-A group was 82.7% (62/75), while that in the D-TACE-A group was 72% (54/75) (P=0.119).
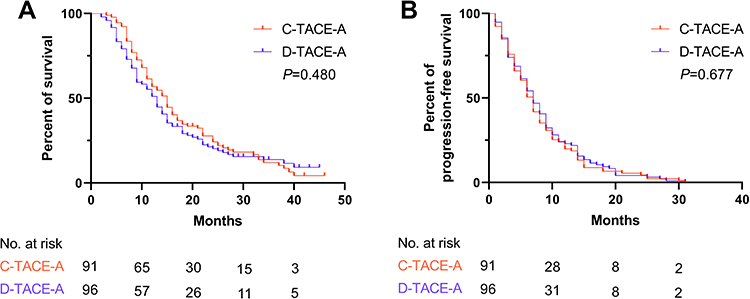 |
Figure 2 Kaplan-Meier curves of OS and PFS in all patients before PSM. (A) Kaplan-Meier curves of OS; (B) Kaplan-Meier curves of PFS. |
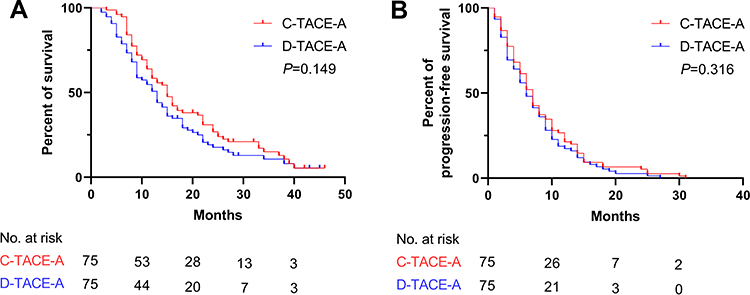 |
Figure 3 Kaplan-Meier curves of OS and PFS in all patients after PSM. (A) Kaplan-Meier curves of OS; (B) Kaplan-Meier curves of PFS. |
Cox Proportional Risk Analysis
Before PSM, univariable analysis showed that the ALT (HR: 1.003, 95% CI: 1.000–1.005; P=0.032), AST (HR: 1.001, 95% CI: 1.001–1.002; P=0.001), leukocytes (HR: 1.055, 95% CI: 1.025–1.085; P<0.001), platelets (HR: 1.003, 95% CI: 1.001–1.005; P<0.001), tumor size (HR: 1.101, 95% CI: 1.064–1.139; P<0.001), AFP level (HR: 1.399, 95% CI: 1.021–1.918; P=0.037), BCLC stage (HR: 20.606, 95% CI: 1.703–3.988; P<0.001), portal invasion (HR: 0.630, 95% CI: 0.462–0.860; P=0.004), distant metastases (HR: 0.545, 95% CI: 0.398–0.746; P<0.001), Child–Pugh Classification (HR: 3.319, 95% CI: 2.216–4.447; P<0.001), ECOG score (1 vs 0: HR: 7.419, 95% CI: 4.822–11.417; P<0.001; 2 vs 0: HR: 20.427, 95% CI: 12.178–34.263; P<0.001), and TACE session (HR: 0.094, 95% CI: 0.059–0.151; P<0.001) were predictors for OS. In the multivariable analysis, the BCLC stage (HR: 1.950, 95% CI: 1.063–3.575; P=0.031), Child–Pugh classification (HR: 2.367, 95% CI: 1.549–3.615; P<0.001), ECOG score (1 vs 0: HR: 8.049, 95% CI: 4.871–13.301; P<0.001; 2 vs 0: HR: 19.174, 95% CI: 10.579–34.751; P<0.001), and TACE session (HR: 0.263, 95% CI: 0.158–0.439; P<0.001) were independent predictors for OS (Table 2). The univariable analysis of PFS showed ALT (HR: 1.003, 95% CI: 1.001–1.005; P=0.013), AST (HR: 1.001, 95% CI: 1.000–1.002; P=0.005), leukocytes (HR: 1.056, 95% CI: 1.024–1.090; P=0.001), platelets (HR: 1.002, 95% CI: 1.001–1.004; P=0.009), tumor size (HR: 1.050, 95% CI: 1.016–1.084; P=0.004), HBV infection (HR: 0.626, 95% CI: 0.441–0.887; P=0.008), portal invasion (HR: 0.713, 95% CI: 0.532–0.956; P=0.024), distant metastases (HR: 0.495, 95% CI: 0.366–0.699; P<0.001), Child–Pugh classification (HR: 1.561, 95% CI: 1.122–2.173; P=0.008), ECOG score (1 vs 0: HR: 2.557, 95% CI: 1.797–3.637; P<0.001; 2 vs 0: HR: 3.064, 95% CI: 2.099–4.471; P<0.001), and TACE session (HR: 0.372, 95% CI: 0.253–0.546; P<0.001) were predictors for tumor progression. The multivariable analysis showed that BCLC stage (HR: 1.927, 95% CI: 1.129–3.289; P=0.016), distant metastases (HR: 0.660, 95% CI: 0.448–0.970; P=0.035), ECOG score (1 vs 0: HR: 2.175, 95% CI: 1.476–3.204; P<0.001; 2 vs 0: HR: 2.271, 95% CI: 1.411–3.655; P=0.001), and TACE session (HR: 0.442, 95% CI: 0.259–0.755; P=0.003) were independent predictors for tumor progression. (Table 3)
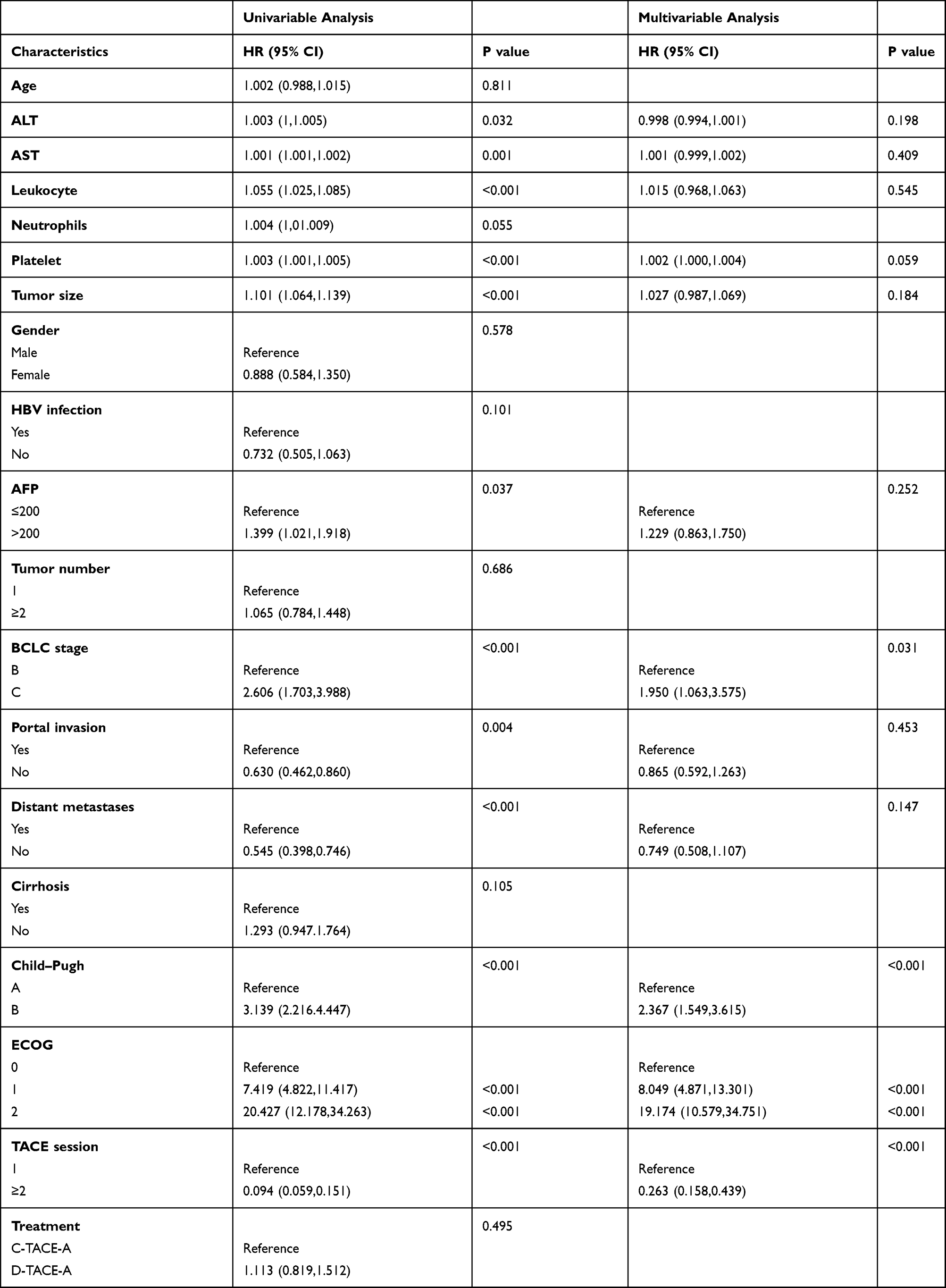 |
Table 2 Univariable and Multivariable Regression Analysis for OS Before PSM |
 |
Table 3 Univariable and Multivariable Regression Analysis for PFS Before PSM |
Subgroup Analysis
Before PSM, age, ALT, AST, leukocytes, neutrophils, platelets, tumor size, gender, HBV infection, AFP level, tumor number, portal invasion, distant metastases, cirrhosis, ECOG score, and TACE session were used in the adjusted Cox proportional analysis. There was no difference in efficacy between D-TACE-A and C-TACE-A treatments of patients with Child–Pugh A or BCLC stage B with regards to overall mortality rate or tumor progression rate. However, in patients with Child–Pugh B, D-TACE-A increased the tumor progression rate, but not the overall mortality rate, compared with C-TACE-A. In patients with BCLC stage C, D-TACE-A increased the overall mortality rate, but did not increase tumor progression rate, compared with C-TACE-A. In patients with cirrhosis, D-TACE-A reduced the tumor progression rate, but not the overall mortality rate, compared with C-TACE-A. While in patients without cirrhosis, D-TACE-A increased the overall mortality rate, but did not increase the tumor progression rate, in comparison with C-TACE-A (Tables 4 and 5).
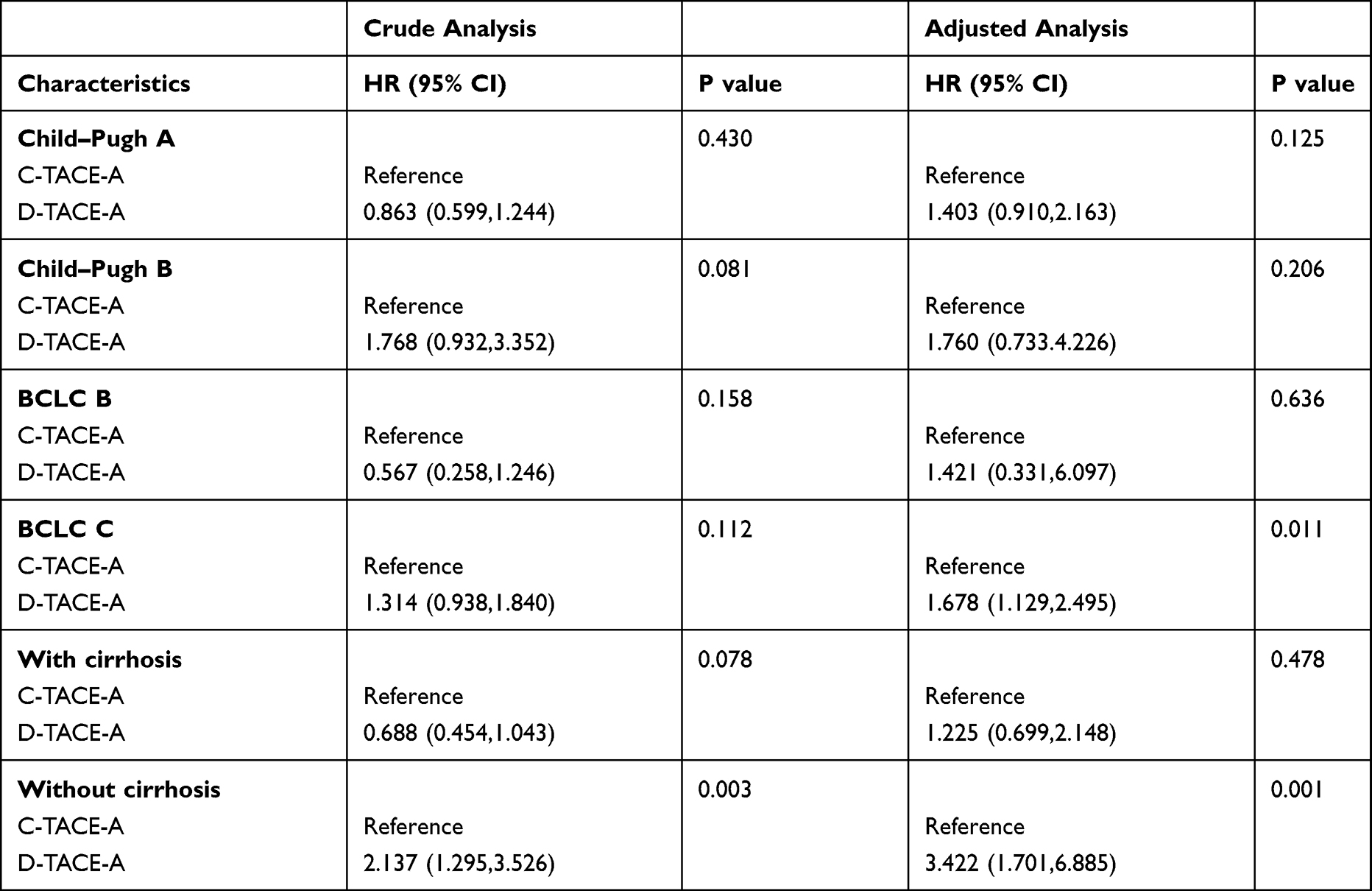 |
Table 4 Subgroup Analysis of Patients with Portal Invasion, Metastases, Cirrhosis for OS Before PSM |
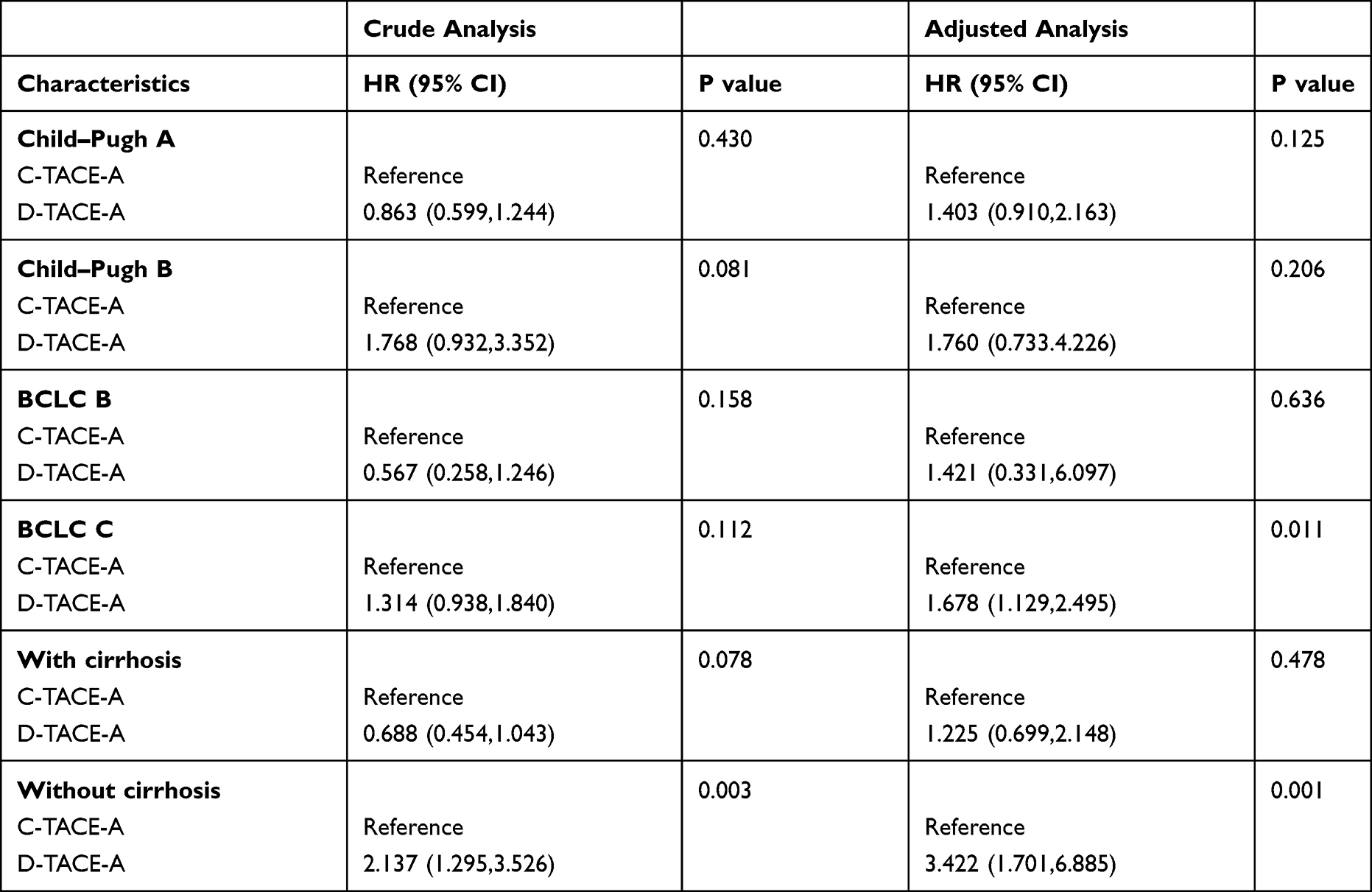 |
Table 5 Subgroup Analysis of Patients with Portal Invasion, Metastases, Cirrhosis for PFS Before PSM |
Adverse Events After Combination Therapy
Before PSM, there were no significant differences in fever (80/96 vs 78/91), fatigue (35/96 vs 34/91), nausea (44/96 vs 46/91), vomiting (33/96 vs 31/91), poor appetite (73/96 vs 68/91), hand-foot response (32/96 vs 28/91), hypertension (14/96 vs 13/91), diarrhea (14/96 vs 13/91), or proteinuria (18/96 vs 13/91) of all grades between the D-TACE-A and C-TACE-A groups (all P>0.05). However, D-TACE-A group patients experienced significantly less abdominal pain of all grades than those in the C-TACE-A group (24/96 vs 47/91; P=0.001). Patients experiencing III and IV grade adverse events in the D-TACE-A group suffered significantly less abdominal pain than those in the C-TACE-A group (2/96 vs 8/91; P=0.036) (Table 6).
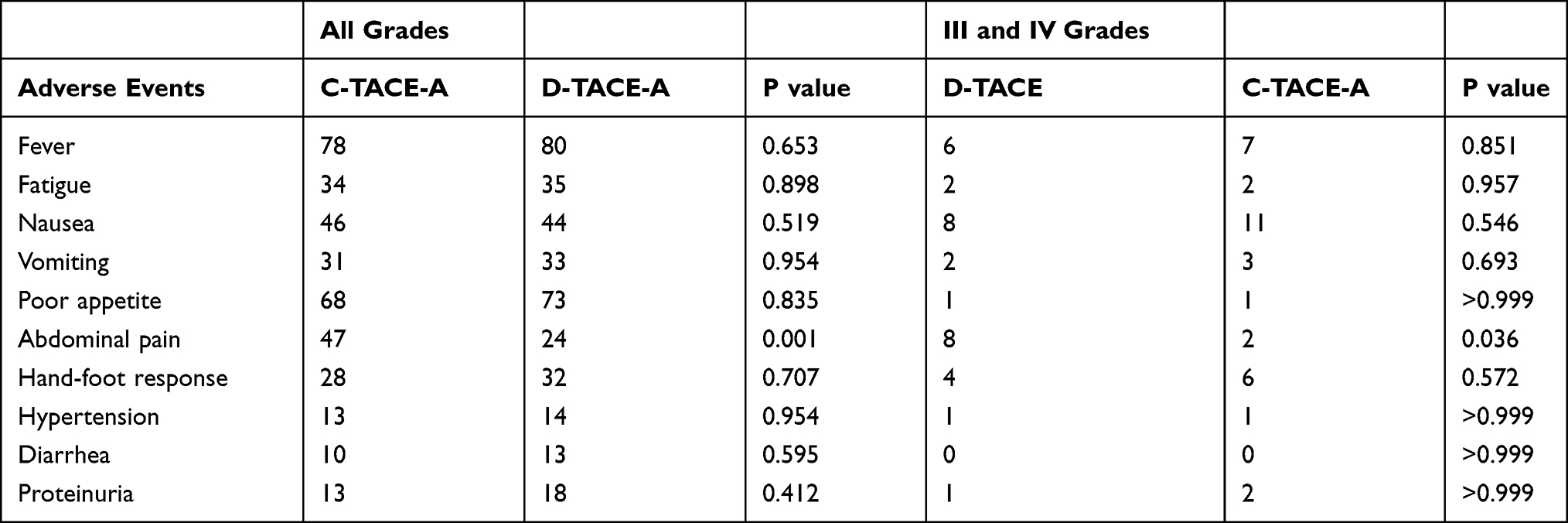 |
Table 6 Adverse Events of Patients After They Receiving TACE or Apatinib Before PSM |
Discussion
The efficacy of D-TACE in the treatment of unresectable HCC has proven to be similar to that of C-TACE,5,20 and some studies showed that patients with unresectable HCC who received TACE combined with apatinib received more survival benefits than those given single treatment.17,18,21 However, whether patients attain more survival benefits from D-TACE or C-TACE when combined with apatinib is still unknown. This study was conducted to compare the efficacy and safety of D-TACE-A compared with C-TACE-A for HCC treatment.
The main finding of the study was that patients with unresectable HCC who received D-TACE-A had similar mOS and mPFS compared with those who received C-TACE-A both before and after PSM. The findings of the study provide new evidence for the optimal treatment of patients with unresectable HCC, and might lead to more selective treatments for these patients. Previous studies have shown that patients with unresectable HCC who received C-TACE-A have mOS from 12.2 months to 18.2 months and mPFS or median time to progression from 4.5 months to 12.5 months.17,21–24 The difference between previous studies and the current study with regards to the mOS and mPFS of patients who underwent C-TACE-A may be due to the heterogeneity of the included patients and the different inclusion criteria. The mOS of patients given C-TACE-A in the current study was slightly higher than that observed in Kan et al’s study, which compared the efficacy of TACE-A to TACE alone for patients with advanced HCC using data from the same institution. This difference may be because Kan et al included patients with advanced HCC, whereas the current study focused on patients with unresectable HCC.21 Only one retrospective study has reported the efficacy of D-TACE-A for patients with HCC, and that study reported that the mOS, mPFS and DCR were 22 months (95% CI: 20.2–23.9), 9.5 months (95% CI: 8.1–10.9), and 90.6% in the third month after the initial therapy.25 The mOS, mPFS, and DCR in that study were all higher than the mOS, mPFS, and DCR in the current one, possibly because the previous study included 18 patients (56.3%) with BCLC stage B, while the current study included 18 (18.8%) patients with BCLC stage B, who received D-TACE-A.
The univariable regression showed that providing patients with D-TACE-A did not increase the mortality rate or tumor progression rate and the data were not included in the multivariable analysis, which showed that patients with unresectable HCC who received D-TACE-A had similar survival benefits compared with those who received C-TACE-A.
Previous studies showed that Child–Pugh classification, BCLC stage, and presence of cirrhosis may influence survival.26–29 Thus, the subgroup analysis was conducted before PSM. An adjusted Cox proportional risk model was used to reduce the impact of potential confounding factors on the results. Patients with BCLC stage C or patients without cirrhosis who received D-TACE-A had a higher mortality rate than those who received C-TACE-A, which meant that C-TACE-A might be more suitable for advanced HCC patients without cirrhosis.
One study demonstrated that HCC patients receiving D-TACE experienced less post-operative pain compared with patients receiving C-TACE.7 In the current study, similar results were presented, as patients in the D-TACE-A group felt less pain of all grades or III and IV grades compared with patients in the C-TACE-A group. All patients with pain after TACE received symptomatic treatment and were relieved. There were no significant differences in TACE-related adverse events or drug-related adverse events between the groups, suggesting that D-TACE-A is safe for patients with unresectable HCC.
There were some limitations apparent in this study. Firstly, this was a retrospective study, which can lead to selection bias; however, PSM was conducted to reduce the risk of selection bias. Secondly, there was a small sample of patients of BCLC stage B, which might have influenced the subgroup analysis. Thus, we hope future studies can be conducted that include more patients to verify the results of this study.
Conclusions
The study showed that advanced HCC patients without cirrhosis obtain more survival benefits from C-TACE-A than C-TACE-A, providing new evidence for clinicians when choosing suitable treatments for patients with unresectable HCC.
Data Deposition and Data Sharing
The data used in the study are available from the correspondence author on reasonable request.
Research Ethics and Consent
This study was approved by ethics committee of Union Hospital of Huazhong University of Science and Technology. Written informed consent was waived by this institution.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81873919).
Disclosure
All authors declare that they have no competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
3. Acunaş B, Rozanes I. Hepatocellular carcinoma: treatment with transcatheter arterial chemoembolization. Eur J Radiol. 1999;32(1):86–89. doi:10.1016/s0720-048x(99)00117-5
4. Varela M, Real MI, Burrel M, et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol. 2007;46(3):474–481. doi:10.1016/j.jhep.2006.10.020
5. Song MJ, Chun HJ, Song DS, et al. Comparative study between doxorubicin-eluting beads and conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J Hepatol. 2012;57(6):1244–1250. doi:10.1016/j.jhep.2012.07.017
6. Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111(2):255–264. doi:10.1038/bjc.2014.199
7. Xie ZB, Wang XB, Peng YC, et al. Systematic review comparing the safety and efficacy of conventional and drug-eluting bead transarterial chemoembolization for inoperable hepatocellular carcinoma. Hepatol Res. 2015;45(2):190–200. doi:10.1111/hepr.12450
8. Farid K, Elalfy H, Abo El-Khair SM, et al. Prognostic value of vascular endothelial growth factor in both conventional and drug eluting beads transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma in HCV patients. Expert Rev Gastroenterol Hepatol. 2020;14(12):1203–1214. doi:10.1080/17474124.2020.1823215
9. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
10. Connock M, Round J, Bayliss S, Tubeuf S, Greenheld W, Moore D. Sorafenib for the treatment of advanced hepatocellular carcinoma. Health Technol Assess. 2010;14(Suppl 1):17–21. doi:10.3310/hta14suppl1-03
11. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a Phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/s1470-2045(08)70285-7
12. Abou-Alfa GK, Schwartz L, Ricci S, et al. Phase II study of sorafenib in patients with advanced hepatocellular carcinoma. J Clin Oncol. 2006;24(26):4293–4300. doi:10.1200/jco.2005.01.3441
13. Kou P, Zhang Y, Shao W, et al. Significant efficacy and well safety of apatinib in an advanced liver cancer patient: a case report and literature review. Oncotarget. 2017;8(12):20510–20515. doi:10.18632/oncotarget.14724
14. Scott LJ. Apatinib: a review in advanced gastric cancer and other advanced cancers. Drugs. 2018;78(7):747–758. doi:10.1007/s40265-018-0903-9
15. Wang Y, Gou Q, Xu R, Chen X, Zhou Z. Efficacy and safety of sorafenib versus apatinib in the treatment of intermediate and advanced hepatocellular carcinoma: a comparative retrospective study. Onco Targets Ther. 2018;11:3407–3413. doi:10.2147/ott.S161023
16. Lu W, Jin XL, Yang C, et al. Comparison of efficacy between TACE combined with apatinib and TACE alone in the treatment of intermediate and advanced hepatocellular carcinoma: a single-center randomized controlled trial. Cancer Biol Ther. 2017;18(6):433–438. doi:10.1080/15384047.2017.1323589
17. Chen S, Yu W, Zhang K, Liu W. Comparison of the efficacy and safety of Transarterial chemoembolization with and without Apatinib for the treatment of BCLC stage C hepatocellular carcinoma. BMC Cancer. 2018;18(1):1131. doi:10.1186/s12885-018-5081-3
18. Zhu Y, Feng B, Mei L, Sun R, Guo C, Zhu J. Clinical efficacy of TACE combined with Apatinib in the treatment of advanced hepatocellular carcinoma. J BUON. 2019;24(2):608–614.
19. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216. doi:10.1093/jnci/92.3.205
20. Gorodetski B, Chapiro J, Schernthaner R, et al. Advanced-stage hepatocellular carcinoma with portal vein thrombosis: conventional versus drug-eluting beads transcatheter arterial chemoembolization. Eur Radiol. 2017;27(2):526–535. doi:10.1007/s00330-016-4445-9
21. Kan X, Liang B, Zhou G, et al. Transarterial chemoembolization combined with apatinib for advanced hepatocellular carcinoma: a propensity score matching analysis. Front Oncol. 2020;10:970. doi:10.3389/fonc.2020.00970
22. Yang Z, Chen G, Cui Y, et al. The safety and efficacy of TACE combined with apatinib on patients with advanced hepatocellular carcinoma: a retrospective study. Cancer Biol Ther. 2019;20(3):321–327. doi:10.1080/15384047.2018.1529099
23. Fan W, Yuan G, Fan H, et al. Apatinib combined with transarterial chemoembolization in patients with hepatocellular carcinoma and portal vein tumor thrombus: a multicenter retrospective study. Clin Ther. 2019;41(8):1463–1476. doi:10.1016/j.clinthera.2019.04.036
24. Shen L, Chen S, Qiu Z, et al. Transarterial chemoembolization combined with apatinib versus transarterial chemoembolization alone for hepatocellular carcinoma with macroscopic vascular invasion: a propensity score matching analysis. J Cancer Res Ther. 2020;16(5):1063–1068. doi:10.4103/jcrt.JCRT_801_19
25. Liu J, Xu J, Zhang W, et al. Safety and efficacy of drug-eluting bead transarterial chemoembolization combined with apatinib in patients with advanced hepatocellular carcinoma. Acad Radiol. 2020;27(5):704–709. doi:10.1016/j.acra.2019.07.003
26. Cancer of the Liver Italian Program (CLIP) Investigators. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology. 1998;28(3):751–755. doi:10.1002/hep.510280322
27. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
28. Wu S, Zeng N, Sun F, et al. Hepatocellular carcinoma prediction models in chronic hepatitis B: a systematic review of 14 models and external validation. Clin Gastroenterol Hepatol. 2021. doi:10.1016/j.cgh.2021.02.040
29. Dawood RM, Salum GM, El-Meguid MA, et al. Development of a gene signature for predicting cirrhosis risk score of chronic liver disease associated with HCV infection in Egyptians. Microb Pathog. 2021;153:104805. doi:10.1016/j.micpath.2021.104805
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.