")
Back to Journals » Clinical Ophthalmology » Volume 13
Efficacy of carbomer sodium hyaluronate trehalose vs hyaluronic acid to improve tear film instability and ocular surface discomfort after cataract surgery
Authors Caretti L, La Gloria Valerio A, Piermarocchi R, Badin G , Verzola G, Masarà F , Scalora T, Monterosso C
Received 10 March 2019
Accepted for publication 5 June 2019
Published 9 July 2019 Volume 2019:13 Pages 1157—1163
DOI https://doi.org/10.2147/OPTH.S208256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
L Caretti,1 A La Gloria Valerio,1 R Piermarocchi,1 G Badin,1 G Verzola,1 F Masarà,1 T Scalora,2 C Monterosso3
1Ophthalmology Unit, Santa Maria della Misericordia Hospital, Rovigo, Italy; 2Neurosciences Department, Ophthalmology Unit, University of Padua, Padua, Italy; 3Ophthalmology Unit, Dell’Angelo Hospital, Meste, Italy
Purpose: To evaluate the effects of carbomer sodium hyaluronate trehalose (CHT) and sodium hyaluronate eye drops on tear film stability and ocular discomfort after cataract surgery.
Setting: Santa Maria della Misericordia Hospital, Rovigo, Italy.
Design: Prospective randomized case-control study.
Patients and methods: This study enrolled sixty patients scheduled for unilateral cataract surgery. After phacoemulsification, subjects received carbomer sodium hyaluronate trehalose (trehalose group) or sodium hyaluronate tears (HG group) substitute and were assessed through objective (break up time, corneal and conjunctival staining) and subjective (OSDI questionnaire) clinical evaluations after a two times a day topical administration. Outcome measures were collected preoperatively (baseline), one week (day 7) and 1 month (day 30) after surgery. Finally, each patient was asked to give his personal treatment satisfaction score.
Results: Trehalose group showed a steeper break up time (BUT) increase compared to patient treated with hyaluronic acid (P<0.001). OSDI questionnaire presented a opposite trend, trehalose patients evidenced a significantly major improvement (P<0.001), and in seven days mean values reduced by more than three times. Fluorescein staining reduction was documented with both treatments, although there was no statistically significant difference between groups. Finally CHT resulted in a significantly greater global satisfaction score (P<0.001).
Conclusions: CHT was effective and well tolerated in reducing dry eye disease symptoms and improving the clinical outcome after cataract surgery. On some parameters (BUT, OSDI), this new formulation was more effective than commonly used sodium hyaluronate in treating ocular irritation and tear film alterations.
Keywords: cataract surgery, tear film instability, artificial tears, trehalose
Phacoemulsification is the surgical procedure most commonly performed worldwide, and the number of treated patients is continuously increasing. Although most patients achieve excellent postoperative visual acuity, tear film dysfunction and dry eye symptoms associated with surgical procedures remain a major challenge.1–4 The onset or the exacerbation of dry eye after cataract surgery is related to a multifactorial process. Corneal sensitivity is reduced by the interruption of the corneal nerves,5 a phototoxic damage derives from the exposure to the microscopic light,6 corneal irrigation may damage the epithelium,7 and inflammatory cytokines elevation in the lacrimal tear have also been demonstrated.8 Finally, the use of topical anesthesia and preservative containing topical eye drops administered after surgery would also have a role in patient ocular surface discomfort.9 All these risk factors could have a negative impact even on the ocular surface of an apparently healthy individual, leading to a short-term tear film instability and eye irritation. Usually, the severity of dry eye alterations peaked 7 days after phacoemulsification, although the eye involvement can improve over time.10 The exact tear film dysfunction after cataract surgery remains under investigation. Oh et al demonstrated that goblet cell density does not recover at 3 months after cataract surgery, which may be responsible for ocular discomfort and dry eye symptoms.11 In addition, corneal denervation associated with surgical injuries may lead to blinking and tearing reflexes impairment resulting in corneal epithelium damage.12 Corneal sensitivity can be also decreased by inflammatory cytokines released during corneal incision healing causing tear film instability.13 Han et al14 evaluated dry eye and meibomian gland dysfunction after cataract surgery demonstrating that ocular symptoms increased at 1 month and 3 month postoperatively together with the worsening of break up time and lid margin abnormalities.
It is postulated that intra-operative measures can minimize surface damage. Kasetsuwan et al suggested that using light filters, decreasing exposure time proper irrigation and soft manipulation of the ocular surface tissue may reduce complications associated with surgery.9 Pathophysiology of perioperative dry eye postulates that an external irritating factor can induce tear film or corneal and conjunctival epithelium abnormalities, leading to ocular discomfort or visual functional disturbance. The tear film covers the epithelium to protect its functions, and it acts as a barrier from desiccation. The function of the tear film and corneal and conjunctival epithelium completes each other; and therefore, damage to either the tear film or the epithelium results in a vicious cycle which may ultimately result in dry eye symptoms.15
Patients usually complain dryness, pain, irritation, burning, foreign body sensation, and it has been demonstrated that cataract surgery can lead to worsening subjective symptoms scores.7
On the basis of the recent understanding of dry eye pathophysiology, there has been a shift in treatment from simply water adding medications to complex and effective artificial tears products. Trehalose is a naturally occurring alpha-linked disaccharide, formed of two molecules of glucose, that in recent years has been considerably investigated for its biological and chemical properties in living organisms. Trehalose is synthesized by many organisms, including insects, plant and fungi in response to prolonged periods of desiccation and it replaces water in the organism by hydrogen bonding interactions with polar groups on membrane lipids and proteins.16 Furthermore, trehalose has the feature to protect from denaturation cellular membrane phospholipids keeping them in liquid phase even in absence of water, to stabilize labile cellular proteins and to protect these structures from oxidative stress.17–19
Carbomer sodium hyaluronate trehalose (CHT) is a novel preservative-free artificial tear preparation containing three active agents: trehalose (3%), a natural substance which protect the eye’s surface from dryness and desiccating conditions; sodium hyaluronate (0.15%) that acts holding water to hydrate and lubricate the eye; carbomer that allows the product to stay on the surface of the eye longer. In this study, carbomer sodium hyaluronate trehalose (CHT) eye drops was compared with hyaluronic acid solution (HA), with particular reference to tear film stability and patient satisfaction.
Patients and methods
Study design
The study was a single center prospective randomized case-control study. Carbomer sodium hyaluronate trehalose was compared with hyaluronic acid treatment, an established and effective artificial tears treatment for dry eye symptoms. The study was approved by the Ethical Committee for Clinical Investigation of Rovigo Hospital and was conducted according to the Declaration of Helsinki (2008) and Good Clinical Practice (GCP). All patients submitted a written informed consent before participating in the study.
Patients
Sixty patients (60 eyes) with very mild to severe dry eye symptoms (OSDI score from 5 to 62.5), scheduled for unilateral cataract surgery, were enrolled at Rovigo Hospital Ophthalmology Unit (140, Tre Martiri Street, 45,100, Rovigo, Italy) from August 2017 to May 2018 (Table 1). Best corrected visual acuity less than 1/10, severe blepharitis, dry eye secondary to eyelid malposition, corneal dystrophy, filamentous keratitis, corneal neovascularization, use of contact lenses, a history of herpes virus within the last 3 months or hypersensitivity to any component of the investigative substances were considered exclusion criteria. At baseline (before surgery), 1 week and 1 month after phacoemulsification, patients underwent a full anterior segment evaluation, including visual acuity testing with correction, slit lamp biomicroscopy, tear film stability (Break Up Time), fluorescein straining, Schirmer test with anesthesia (performed 30 mins after fluorescein instillation). Subjective symptoms were investigated by OSDI questionnaire. Finally, each patient was asked to give his personal treatment satisfaction score (from 0 to 100).
 |
Table 1 Mean values and standard deviations divided by group and period |
Treatment
After surgery, 30 eyes received carbomer sodium hyaluronate trehalose eye drops (Thealoz Gel®, Thea Laboratoires, Clermont-Ferrand, France) (trehalose group), while the other 30 eyes were treated with sodium hyaluronate (Hydrabak®, Thea Laboratoires, Clermont-Ferrand, France) (Hyaluronate group, HG). Patients in both groups administered the treatment 2 times a day for one month after the surgery in association with topical steroid-antibiotic combination and topical nonsteroidal anti-inflammatory drugs (NSAIDs). Patients were allocated into groups with a randomized double-blind approach.
CHT is an artificial tear preparation containing three active ingredients: trehalose, hyaluronate and carbomer. Trehalose is a naturally occurring disaccharide of glucose that appears to function in an anhydrobiotic capacity in many organisms. Hyaluronate is a widely distributed anionic glycosaminoglycan polysaccharide with biological roles associated with its lubricative and water-retaining properties. Finally, carbomer induces a long-lasting stability of the product on the ocular surface.
Primary efficacy variables
Tear stability
Break up time (BUT) test was performed using fluorescein strips, which were introduced into the conjunctival fornix with minimal stimulation. The patient was asked to blink several times and then to keep the eyes open. Cornea was examined under cobalt blue filter on the slit lamp. The dry area was indicated by the presence of black spots. The time between the last blink and the appearance of a random dry spot was recorded in seconds, as the tear film breakup time. The test was repeated three times and the average value was recorded.
Dry eye symptoms
Subject symptoms were assessed using OSDI questionnaire. This test is comprised of 12 questions and evaluates the frequency of symptoms over the preceding week. The questionnaire requires approximately 5 mins for the patient to complete; it was administered to subjects before each ophthalmic examination and the scores range from 0 to 100.
Secondary efficacy variables
Corneal and conjunctival staining
Epithelial damage was assessed by fluorescein staining according to Oxford scale score (grading from 0 to 5).
Tear production
Abnormality in tear volume was assessed by Schirmer test. The evaluation was performed, with anesthesia, in each visit.
Visual acuity
BCVA was evaluated with Snellen chart in each visit.
Global satisfaction
Patient satisfaction was evaluated at day 7 and day 30 by a 0 (“no satisfaction”) to 100 (“maximal satisfaction”) visual analog scale.
Surgical procedure
One surgeon performed all cataract surgeries with patients under topical anesthesia. Before surgery, the eye was prepared and draped using sterile techniques. Phacoemulsification was performed with a 2.2-mm superior clear corneal incision and a side port of about 1 mm 90-degree incision away from the main incision. The range of phacoemulsification time was 5–10 mins and foldable intraocular lens were inserted thereafter. There were no intraoperative complications in all cases. After surgery, all patients instilled topical steroid-antibiotic combination and FANS eye drops.
Statistical method
Statistical analysis was performed using R software (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was proven with both parametric and nonparametric tests, ANOVA and permutational ANOVA.
Results
Sixty eyes of sixty patients were recruited and data were analyzed considering 2 main parameters (BUT and OSDI score), 2 secondary variables (Fluorescein staining, Schirmer test) and a global treatment satisfaction score. All parameters were assessed at baseline (before surgery), day 7 and day 30 after phacoemusification (Table 1). In both tests applied (ANOVA and permutational ANOVA), the difference between periods was significant for all considered variable (P<0.001). Furthermore, the interaction between group and period was also significant for Oxford (P<0.001), BUT (P<0.001) and OSDI (P<0.001, Tables 2 and 3).
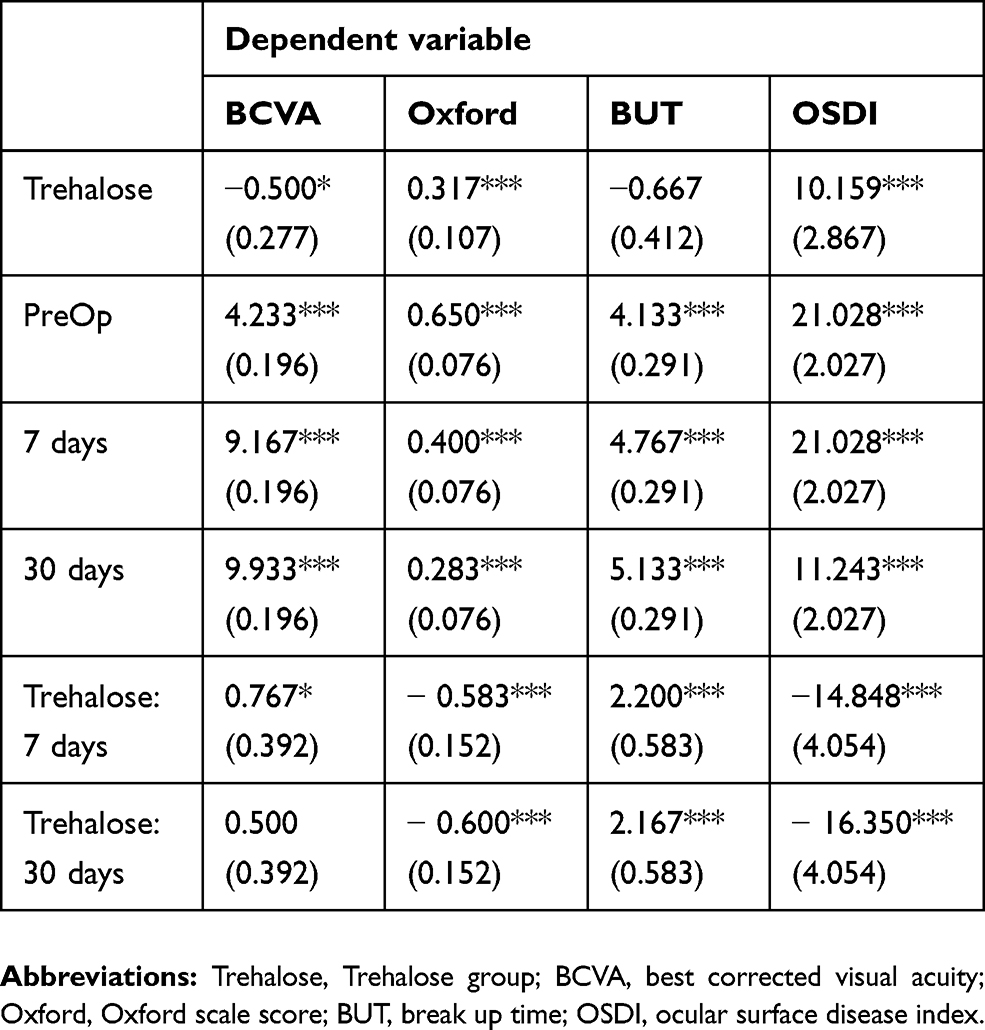 |
Table 2 Linear models for the four variables considered |
 |
Table 3 P for mean BCVA, Oxford scale score, BUT, OSDI difference divided for group and period |
Efficacy
Break-up time
In trehalose group, BUT increases by a factor of 2.2 in the first postoperative check (7 days) and of 2.17 in the second assessment (30 days) compared to the control group. At baseline, the mean BUT value was 3.47 seconds, and a statistically significant improvement was seen at day 7 (6.30 s) and day 30 (6.67) (P<0.001). Also in HG group, a time growth can be demonstrated (baseline 4.13 s; day 7 4.77 s; day 30 5.13 s); however, the improvement was minor compared to patients treated with carbomer sodium hyaluronate trehalose (P<0.001, Figure 1).
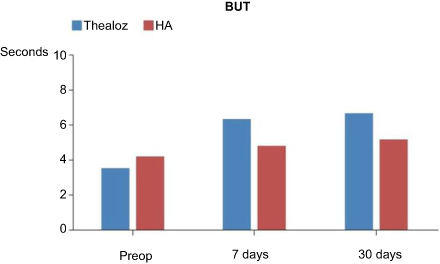 |
Figure 1 Mean TBUT pre-operatively and seven days and 30 days post-operatively. The bars represent standard deviation of the mean.Abbreviations: HG, Hyaluronate group; Trehalose, Trehalose group; BUT, break up time. |
OSDI
Mean OSDI score decreased from 31.19 at baseline to 5.05 on day 30 in CHT group. In HG subjects it changed from 21.3 at baseline to 14.37 on day 7, and to 11.24 on day 30 (Figure 2).
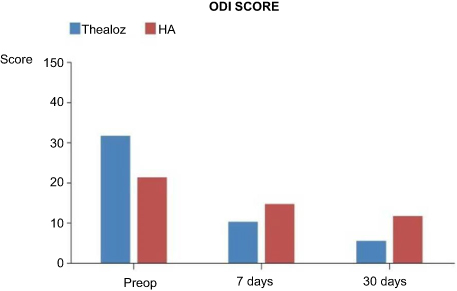 |
Figure 2 Mean OSDI score pre-operatively and seven days and 30 days post operatively. The bars represent standard deviation of the mean.Abbreviations: HG, Hyaluronate group; Trehalose, Trehalose group; OSDI, ocular surface disease index. |
Cornea-conjunctival staining
Although there were no statistically significant differences between the groups, fluorescein staining test improved with both treatments during the postoperative evaluations (P<0.05, Figure 3).
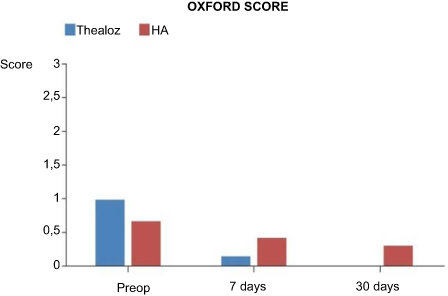 |
Figure 3 Mean Oxford score pre-operatively and seven days and 30 days post-operatively. The bars represent standard deviation of the mean.Abbreviations: HG, Hyaluronate group; Trehalose, Trehalose group; Oxford, Oxford scale score. |
Tear production
Schirmer test values did not show any statistically significant difference between baseline and day 30 in both groups.
Visual acuity
BCVA assessment demonstrated a steep increase of visual function compared to preoperative values; however, no statistically significant difference was found between groups.
Patient global satisfaction
Patient treatment global satisfaction was 97.3±4.95 under carbomer sodium hyaluronate trehalose (CHT) eye drops compared to of 87.4±8.96 under hyaluronic acid (HA) solution treatment. The difference between CHT and HA medication was statistically significant (P<0.001).
Discussion
Dry eye symptoms are a distressing ocular condition that can arise even in healthy individuals after some anterior segment surgical procedure as phacoemulsification. Prolonged eye irritation can have a negative impact on patient quality of life reducing global satisfaction despite an uncomplicated ocular surgery. In recent years, an increasing attention has been paid to tear film instability after phacoemulsification, and the research of an ideal lacrimal substitute is still open. Trehalose-containing eyedrops have previously shown to be effective in vitro,20 ex vivo,21 in vivo animal evaluations22 and in a few clinical studies.23–25 Advantages of this formulation are deep hydration, stabilizing both lipid membranes and labile proteins against desiccation, a protective effect against oxidative insult and promoting epithelial cells recovery. The combination of trehalose and hyaluronic acid has increased benefits on tear film stability due to its viscoelastic properties; however, the time of permanence on the ocular surface is still improvable. This study investigates the effects of a new carbomer adding sodium hyaluronate trehalose formulation compared to hyaluronic acid through objective and subjective clinical evaluations after a 2 times a day topical administration. The analysis shows that all the considered variables (BUT, OSDI, staining, BCVA) have the same trend in both groups. BCVA and BUT values gradually grow during postoperative assessments, while fluorescein staining and OSDI score show the opposite behavior. Treatment efficacy documented in both groups seems to be in line with the recent scientific literature, since the utility of hyaluronate-containing eyedrops is well established in dry eye therapy.26
Focusing on treatment effects on tear stability, break-up time test underlines a quicker improvement in trehalose group, where the time recorded almost doubles after 7 days of drops administration. On the other hand, in HA group, we found only a slight improvement after 1 week, and an overall gain of just one second (from 4.13 at baseline to 5.13 on day 30), compared to a value of three times more in trehalose group (from 3.47 at baseline to 6.67 on day 30). Considering that usually the severity of dry eye alterations peaks 7 days after phacoemulsification, a faster action in the immediate postoperative time can better reduce the eye irritation impact on patient quality of life. Finally, CHT application seems to be more effective in stabilizing tear film even if baseline BUT mean values are lower in trehalose group compared to controls. There is still no gold-standard model for determining dry eye severity; however, the Odissey European Consensus Group developed an algorithm that identifies the most relevant criteria involved in the ocular surface evaluation.27 Focusing on break up time, values less than 3 s are diffusely considered a severe tear film instability, the interval between 3 and 6 is associated with moderate alterations, while if more than 6 but less than 10 the parameter is often defined borderline. Baseline values of both studied groups are inside moderately altered BUT interval, but the effect of the treatment is significantly different. In fact, HA patients do not move from the initial range; on the contrary, trehalose subjects were able to overcome the 6 seconds threshold, reaching the borderline step.
The Ocular Surface Disease Index (OSDI) is one of the most widely used questionnaires to determine dry eye subjective symptoms. The OSDI has been shown to well correlate with disease severity and corneal staining.10 It is generally accepted that an OSDI score of around 30 or over is necessary for diagnosis of severe eye irritation. Again, in the analyzed sample, the questionnaire scores decrease faster in trehalose patients, and in seven days mean values reduced by more than three times. In HA group an improvement was also present, but it was minor and slower. In our opinion, this data are relevant especially because the baseline CHT OSDI score is classified as severe, and consequently associated to serious subjective symptoms. At day 30, the final score reached an optimal value (5.05), showing the efficacy of the CHT treatment despite the severe preoperative conditions.
The corneal and conjunctival staining assessment showed a progressive epithelial damage reduction during postoperative evaluations, but data were not significantly different between the considered groups. This evidence could be related to the low grade of epithelial involvement and the tendency of mean values recorded to be close to zero. Nevertheless, focusing on trehalose patients, we can observe higher baseline Oxford scale scores (0.97) compared to HA subjects (0.65), and a greater improvement after the treatment period. Furthermore, only in trehalose patients, a complete epithelial recovery can be documented (0 score on day 30), while in HA group a mild punctate staining can be still detected (0.28 score at day 30).
Finally, this study indicates that patient global satisfaction improved with both carbomer sodium hyaluronate trehalose and hyaluronic acid eye drops, although CTH resulted in a significantly greater appreciation score.
Although some parameters (BCVA, staining) did not show statistical significance, the trend's direction was consistent; and where statistically significant differences between groups were observed (OSDI, BUT, global satisfaction score), they were all in favor of trehalose group. In our opinion, these evidences can be related to the small number of daily treatment medications. Probably the carbomer component present in CHT allows the product to stay longer on the ocular surface, and the effects on tear film stability and ocular discomfort are satisfying even with a two times a day instillation, improving patient compliance.
To conclude this study highlights that eyedrops containing both trehalose, hyaluronate and carbomer seem at least as effective and, on some parameters, more effective than commonly used sodium hyaluronate in treating ocular irritation and tear film alteration after cataract surgery.
What was known
- Cataract surgery can have a negative impact even on the ocular surface of an apparently healthy individual, leading to a short-term tear film instability and eye irritation.
- Trehalose and hyaluronic acid was proven to be an effective combination of two active ingredients for the treatment of dry eye symptoms; however, number of administration and patient compliance are still a major challenge.
What this paper adds
- Carbomer sodium hyaluronate trehalose is a novel artificial tear preparation that seems to be effective in reducing ocular irritation and tear film dysfunction even with a short number of daily administrations
- To our knowledge, no other studies regarding safety and efficacy of this new formulation have been published.
Synopsis
Carbomer sodium hyaluronate trehalose administered two times a day after cataract surgery showed a statistically significant higher improvement in tear film stability and ocular discomfort compared to hyaluronic acid solution.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Iglesias E, Sajnani R, Levitt RC, Sarantopoulos CD, Galor A. Epidemiology of persistent dry eye-like symptoms after cataract surgery. Cornea. 2018;37(7):893–898. doi:10.1097/ICO.0000000000001491
2. Szakáts I, Sebestyén M, Tóth É, Purebl G. Dry eye symptoms, patient-reported visual functioning, and health anxiety influencing patient satisfaction after cataract surgery. Curr Eye Res. 2017;42(6):832–836. doi:10.1080/02713683.2016.1262429
3. Kim JS, Lee H, Choi S, Kim EK, Seo KY, Kim TI. Assessment of the tear film lipid layer thickness after cataract surgery. Semin Ophthalmol. 2018;33(2):231–236. doi:10.1080/08820538.2016.1208764
4. Sutu C, Fukuoka H, Afshari NA. Mechanisms and management of dry eye in cataract surgery patients. Curr Opin Ophthalmol. 2016;27(1):24–30. doi:10.1097/ICU.0000000000000227
5. Kissner A, Kohlhaas M, Spörl E, Pillunat LE. Corneal aberrations before and after corneal and corneoscleral small incision cataract surgery. Klin Monbl Augenheilkd. 2007;224(2):95–100. doi:10.1055/s-2006-927390
6. Hwang HB, Kim HS. Phototoxic effects of an operating microscope on the ocular surface and tear film. Cornea. 2014;33(1):82–90. doi:10.1097/ICO.0000000000000001
7. Li XM, Hu L, Hu J, Wang W. Investigation of dry eye disease and analysis of the pathogenic factors in patients after cataract surgery. Cornea. 2007;26(9Suppl 1):S16–20. doi:10.1097/ICO.0b013e31812f67ca
8. Simone JN, Whitacre MM. Effects of anti-inflammatory drugs following cataract extraction. Curr Opin Ophthalmol. 2001;12(1):63–67.
9. Kasetsuwan N1, Satitpitakul V, Changul T, Jariyakosol S. Incidence and pattern of dry eye after cataract surgery. PLoS One. 2013;8(11):e78657. doi:10.1371/journal.pone.0078657
10. Sullivan BD, Whitmer D, Nichols KK, et al. An objective approach to dry eye disease severity. Invest Ophthalmol Vis Sci. 2010;51(12):6125–6130. doi:10.1167/iovs.10-5390
11. Oh T, Jung Y, Chang D, Kim J, Kim H. Changes in the tear film and ocular surface after cataract surgery. Jpn J Ophthalmol. 2012;56(2):113–118. doi:10.1007/s10384-012-0117-8
12. Gayton JL. Etiology, prevalence, and treatment of dry eye disease. Clinical Ophthalmol. 2009;3:405–412. doi:10.2147/opth.s5555
13. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669–676. doi:10.1016/j.ophtha.2014.10.004
14. Han KE, Yoon SC, Ahn JM, et al. Evaluation of dry eye and meibomian gland dysfunction after cataract surgery. Am J Ophthalmol. 2014;157(6):1144–1150. doi:10.1016/j.ajo.2014.02.036
15. International Dry Eye WorkShop. 2007 Report of the international dry eye workshop (DEWS). Ocular Surf. 2007;5(2):65–202.
16. Crowe JH. Trehalose and anhydrobiosis: the early work of J. S. Clegg. J Exp Biol. 2008;211:2899–2900. doi:10.1242/jeb.012476
17. Elbein AD, Pan YT, Pastuszak I, Carroll D. New insights on trehalose: a multifunctional molecule. Glycobiology. 2003;13:17R–27R. doi:10.1093/glycob/cwg047
18. Jain NK, Roy I. Effect of trehalose on protein structure. Protein Sci. 2009;18:24–36. doi:10.1002/pro.3
19. Benaroudj N, Lee DH, Goldberg AL. Trehalose accumulation during cellular stress protects cells and cellular proteins from damage by oxygen radicals. J Biol Chem. 2001;276:24261–24267. doi:10.1074/jbc.M101487200
20. Chen W, Zhang X, Liu M, et al. Trehalose protects against ocular surface disorders in experimental murine dry eye through suppression of apoptosis. Exp Eye Res. 2009;89(3):311–318. doi:10.1016/j.exer.2009.03.015
21. Hovakimyan M, Ramoth T, Löbler M, et al. Evaluation of protective effects of trehalose on desiccation of epithelial cells in three dimensional reconstructed human corneal epithelium. Curr Eye Res. 2012;37(11):982–989. doi:10.3109/02713683.2012.700754
22. Li J, Roubeix C, Wang Y, et al. Therapeutic efficacy of trehalose eye drops for treatment of murine dry eye induced by an intelligently controlled environmental system. Mol Vis. 2012;18:317–329.
23. Matsuo T, Tsuchida Y, Morimoto N. Trehalose eye drops in the treatment of dry eye syndrome. Ophthalmology. 2002;109(11):2024–2029.
24. Matsuo T. Trehalose versus hyaluronan or cellulose in eyedrops for the treatment of dry eye. Jpn J Ophthalmol. 2004;48(4):321–327. doi:10.1007/s10384-004-0085-8
25. Ramoth T, Hovakimyan M, Guthoff RF, Stachs O. Charakterisierung der ranenfilmdynamik am Beispiel einer Trehaloseapplikation zur Behandlung des Trockenen Auges. [Characterisation of tear film dynamics after application of trehalose for treatment of dry eye]. Klin Monbl Augenheilkd. 2013;230(12):1220–1224. German. doi:10.1055/s-0033-1351069
26. Baeyens V, Bron A, Baudouin C, Vismed/Hylovis Study Group. Efficacy of 0.18% hypotonic sodium hyaluronate ophthalmic solution in the treatment of signs and symptoms of dry eye disease. J Fr Ophtalmol. 2012;35(6):412–419. doi:10.1016/j.jfo.2011.07.017
27. Baudouin C, Aragona P, Van Setten G, et al; ODISSEY European Consensus Group members. Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168–1176. doi:10.1136/bjophthalmol-2013-304619
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.