")
Back to Journals » Psoriasis: Targets and Therapy » Volume 11
Efficacy of Brodalumab and Guselkumab in Patients with Moderate-to-Severe Plaque Psoriasis Who are Inadequate Responders to Ustekinumab: A Matching Adjusted Indirect Comparison
Authors Hampton P , Borg E, Hansen JB, Augustin M
Received 25 June 2021
Accepted for publication 19 October 2021
Published 3 November 2021 Volume 2021:11 Pages 123—131
DOI https://doi.org/10.2147/PTT.S326121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Uwe Wollina
Philip Hampton,1 Emma Borg,2 Jes Birger Hansen,2 Matthias Augustin3
1Department of Dermatology, The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle, UK; 2LEO Pharma A/S, Ballerup, Denmark; 3Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf (UKE), Hamburg, Germany
Correspondence: Philip Hampton
Department of Dermatology, The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle, NE7 7DN, UK
Email [email protected]
Purpose: Both brodalumab and guselkumab improve skin clearance in patients with moderate-to-severe plaque psoriasis after inadequate response to ustekinumab. In the absence of a direct head-to-head comparison, the relative efficacy of brodalumab and guselkumab in non-responders to ustekinumab were compared using a matching-adjusted indirect comparison (MAIC).
Patients and Methods: Individual patient data for brodalumab (n = 121) were pooled from the AMAGINE-2 and -3 trials and adjusted using a propensity score reweighting method, so that baseline and week 16 characteristics matched the aggregate published data of patients with an inadequate response to ustekinumab who switched to guselkumab (n = 135) in the NAVIGATE trial.
Results: After inadequate response to ustekinumab, brodalumab resulted in significantly higher psoriasis area and severity index (PASI) 90 rates versus guselkumab at post-treatment switch week 12 (62.7% vs 48.1%, relative difference 14.6% [95% confidence interval [CI] 5.3– 23.9], p = 0.002 [number needed to treat [NNT] = 6.8]) and week 36 (63.7% vs 51.1%; relative difference 12.6% [95% CI 4.1– 21.0]; p = 0.004 [NNT = 7.9]) and PASI 100 rate at week 36 (40.3% vs 20.0%; relative difference 20.3% [95% CI 11.8– 28.7]; p < 0.001 [NNT = 4.9]).
Conclusion: In this MAIC, brodalumab was associated with greater improvements than guselkumab in inadequate responders to ustekinumab. Switching to brodalumab in such patients may be a more effective strategy than switching to guselkumab.
Keywords: brodalumab, guselkumab, psoriasis
Introduction
Improved understanding of the pathogenesis of plaque psoriasis has resulted in significant advances in the treatment of patients through the development of targeted biological therapies. These therapies include the tumor necrosis factor (TNF)-α inhibitors, which were the first biologics to be widely used, as well as newer agents, such as ustekinumab, which targets the interleukin (IL)-12/23 pathway and, more recently, IL-17 inhibitors, including secukinumab and ixekizumab, which bind only to the IL-17A ligand, and brodalumab, which targets the IL-17-receptor A, as well as IL-23 inhibitors, including guselkumab, tildrakizumab, and risankizumab. IL-17 and IL-23 inhibitors have shown improved efficacy with higher rates of skin clearance than TNF-α inhibitors or ustekinumab in comparative studies.1–8
However, despite the efficacy of biological therapies, many patients fail to respond initially or discontinue therapy due to loss of response over time or treatment-related adverse effects. In these patients, switching to an alternative biological agent may be an option. Given the increasing number of biologics available for the treatment of psoriasis, data on the relative efficacy of available treatment options in different patient populations, including those who have switched from another biological agent, are important to help optimize clinical decision making. However, there are few direct head-to-head studies comparing different biologic therapies, especially in biologic failures.
In the absence of comparative randomized controlled trials, indirect comparisons can be used to estimate the relative efficacy of treatments. One such method is the use of matching-adjusted indirect comparison (MAIC), which can assess the comparative efficacy of two treatments using data from different trials.9,10 This approach requires individual patient-level data (IPD) for one of the treatments, which can then be reweighted to match aggregate published data for a comparative treatment in a similar population. Reweighting involves matching the mean baseline characteristics of patients with IPD with those reported for the trial without IPD. This approach is a form of propensity score weighting in which patients with IPD are weighted by their inverse odds of being in that group versus the other treatment group (in this case the trial with only published aggregate data). MAIC can be used in the absence of a common comparator arm, in which case it is described as an unanchored comparison, and can adjust for cross-trial differences in baseline characteristics, reduce sensitivity to effect measures, resolve differences in study outcome definitions and deal with incomplete evidence networks. This methodology has previously been described in detail by Signorovitch et al9,10 and has been widely employed to provide comparative clinical efficacy data, especially in health care technology appraisal,11 and has previously been used to compare treatments for psoriasis where no direct comparison is available.5,12,13
Both brodalumab and guselkumab have been reported to improve skin clearance outcomes in inadequate responders to ustekinumab compared with continued ustekinumab treatment.6,14 However, they have not been directly compared in a randomized trial. In this MAIC, aggregate data from the NAVIGATE trial of guselkumab6 and pooled IPD from the AMAGINE 2/3 trials of brodalumab1 were used to provide a robust comparison of the relative efficacy of the two treatments in patients with moderate-to-severe plaque psoriasis and an inadequate response to ustekinumab.
Methods
Aggregate data for guselkumab were derived from the published NAVIGATE trial (NCT02203032)6 and IPD for brodalumab were pooled from the AMAGINE-2 (NCT01708603) and AMAGINE-3 trials (NCT01708629).1 All three trials included patients aged 18–75 years who were candidates for biologic therapy for stable moderate-to-severe plaque psoriasis (minimum 6 months’ duration) with a psoriasis area and severity index (PASI) score of ≥12, a physician’s global assessment (PGA) or investigator’s global assessment (IGA) score of ≥3, and involvement of ≥10% of body surface area.
NAVIGATE was a Phase III, randomized, double-blind trial that evaluated skin clearance in patients treated with guselkumab who previously had an inadequate response to ustekinumab (Figure 1). Patients received ustekinumab 45 or 90 mg at weeks 0 and 4 of a 16-week open-label run-in period. Patients with an inadequate response at week 16 were randomized to continued ustekinumab or guselkumab 100 mg (at weeks 16, 20, 28, 36 and 44).
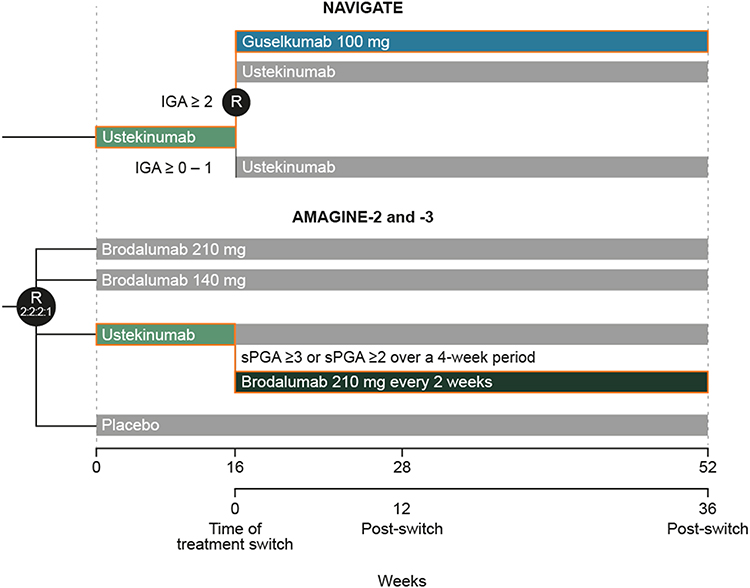 |
Figure 1 Trial designs of NAVIGATE and AMAGINE 2/3. In AMAGINE-2 and −3, at week 12, patients who were originally randomized to brodalumab underwent repeat randomization (2:2:2:1) to one of four maintenance regimens: brodalumab at 210 mg every 2 weeks, 140 mg every 2 weeks, 140 mg every 4 weeks, or 140 mg every 8 weeks. Patients who were originally randomized to placebo were switched to brodalumab at a dose of 210 mg every 2 weeks. Patients who were originally randomly assigned to receive ustekinumab and had an adequate response continued to receive ustekinumab every 12 weeks until week 52. These details are reported in more detail in Lebwohl et al 2015. Abbreviations: IGA, investigator’s global assessment; sPGA, static physician’s global assessment. |
AMAGINE-2 and −3 were two Phase III trials, identical in design, in which patients were randomized (2:2:1:1) to double-blind treatment with brodalumab 140 mg, brodalumab 210 mg, ustekinumab 45 mg (if body weight ≤100 kg) or 90 mg (if body weight >100 kg), or placebo (Figure 1). Patients receiving ustekinumab who did not have an adequate response at week 16, were switched to rescue treatment of brodalumab 210 mg every 2 weeks. Rescue treatment was blinded until the study was unblinded.
In the AMAGINE 2/3 trials, inadequate response to ustekinumab at week 16 was defined as a single static PGA (sPGA) ≥3 or sPGA ≥2 over a 4-week period. The sPGA that was used had a 6-point scale (0 to 5). In the NAVIGATE trial, the definition of inadequate response was an IGA ≥2, using a 5-point scale (0 to 4) at week 16. Full details of these studies have been previously reported.1,6
This MAIC was unanchored due to the absence of an appropriate common comparator trial arm and was conducted according to the statistical methodology described by Signorovitch et al9,10 Pooled IPD from the AMAGINE-2 and −3 trials were adjusted using a propensity score reweighting method such that baseline and week 16 characteristics matched the aggregate published data of patients with an inadequate response with ustekinumab who switched to guselkumab in in the NAVIGATE trial.
Baseline characteristics of patients that were matched were age, sex, body mass index, presence of psoriatic arthritis, duration of disease, previous topical treatment, previous phototherapy, previous systemic treatment, and previous anti-TNF treatment. Mean PASI and Dermatology Life Quality Index (DLQI) score at time of switch from ustekinumab (week 16) were also matched.
All statistical analyses were performed using SAS version 9.4 or higher (SAS Institute Inc., Cary, North Carolina, USA). The Newton–Raphson algorithm was applied to determine appropriate weighting of matching variables using the NLPNRA subroutine within the PROC IML. The distribution of weights for each analysis was inspected to check for the presence of any extreme weights.
Efficacy endpoints were the proportions of patients who achieved PASI 90 at weeks 12 and 36 post-treatment switch (ie, weeks 28 and 52 since baseline, respectively), PASI 100 (week 36), PGA success (weeks 12 and 36), defined as PGA score of 0/1 with ≥2 grade improvement from time of switching, and DLQI score of 0/1 (week 36). Weighted analysis of these endpoints was conducted with the brodalumab IPD and guselkumab aggregated data and adjusted proportions and risk differences were calculated using a multivariate linear regression model. Numbers needed to treat (NNT) for the difference between brodalumab and guselkumab were also calculated for each endpoint. Missing data were accounted for by non-responder imputation ie, patients with missing data were counted as no response.
Results
In the NAVIGATE trial,6 871 patients received open-label ustekinumab (45 mg or 90 mg) at weeks 0 and 4. At week 16, 268 patients had an inadequate response to ustekinumab and were randomized to double-blind treatment with continued ustekinumab (n = 133) or to guselkumab 100 mg (n = 135); the 135 patients who switched from ustekinumab to guselkumab were included in this analysis.
In the AMAGINE-2 and −3 trials,1 124 of 590 patients (21.0%) had an inadequate response to ustekinumab at week 16 (70 with a single sPGA ≥3 at week 16 and 54 with a sPGA ≥2 over a 4-week period) and were switched to brodalumab; three patients had missing data and were excluded from the analyses. After reweighting, the effective sample size was 90 patients for PASI 90 and PASI 100, 89 for PGA and 75 for DLQI.
Baseline characteristics of patients before and after reweighting are shown in Table 1. Cross-trial differences between brodalumab and guselkumab treatment arms existed before reweighting, with brodalumab patients having higher mean PASI and DLQI scores, and a higher proportion of patients having received prior biologic treatment with anti-TNF agents. After reweighting, baseline characteristics were similar. Patients had a mean age of 44 years, 70% were male, mean duration of psoriasis was 18 years and mean PASI score at time of treatment switch was 9.8.
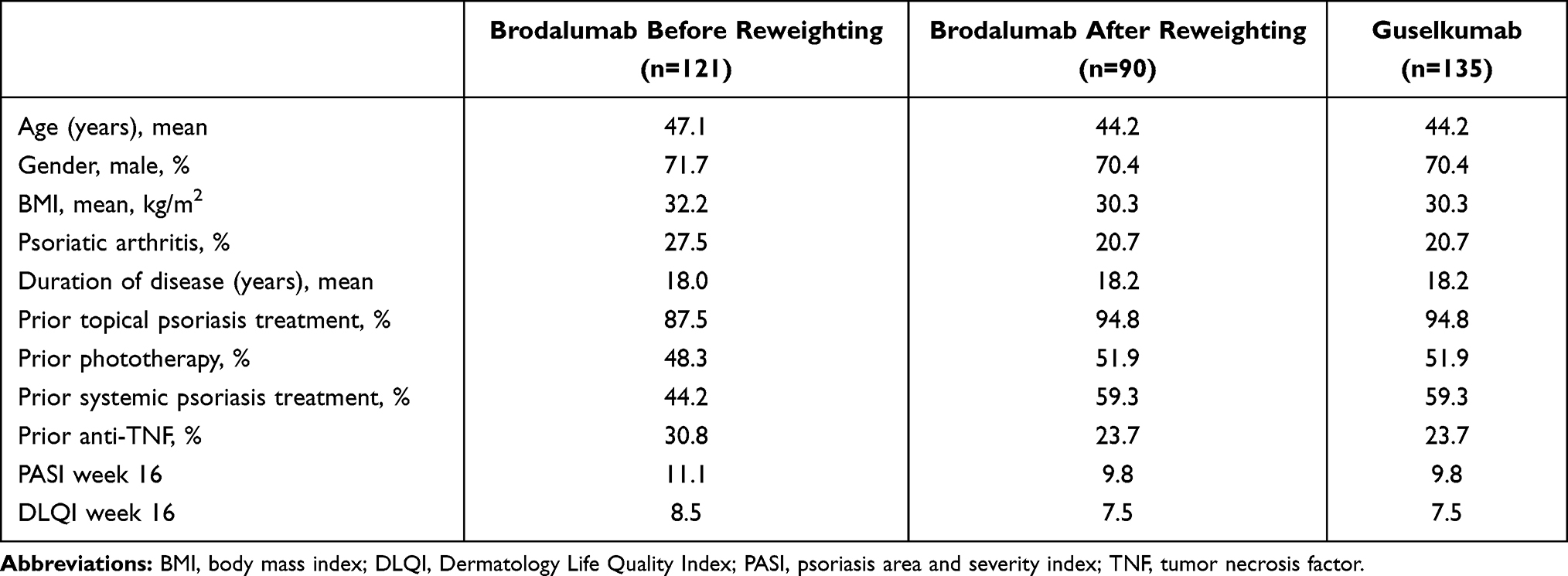 |
Table 1 Baseline Characteristics of Patients |
Overall, brodalumab was associated with significantly higher efficacy response rates compared to guselkumab. After an inadequate response to ustekinumab, brodalumab resulted in statistically significant higher PASI 90 rates compared to guselkumab at post-treatment switch week 12 (62.7% vs 48.1%, relative difference [RD] 14.6% [95% confidence interval [CI] 5.3–23.9], p = 0.002, [NNT for the difference between brodalumab and guselkumab 6.8]) and week 36 (63.7% vs 51.1%; RD 12.6% [95% CI 4.1–21.0]; p = 0.004, [NNT 7.9]) and PASI 100 rate at week 36 (40.3% vs 20.0%; RD 20.3% [95% CI 11.8–28.7]; p < 0.001, [NNT 4.9]) (Table 2/Figure 2).
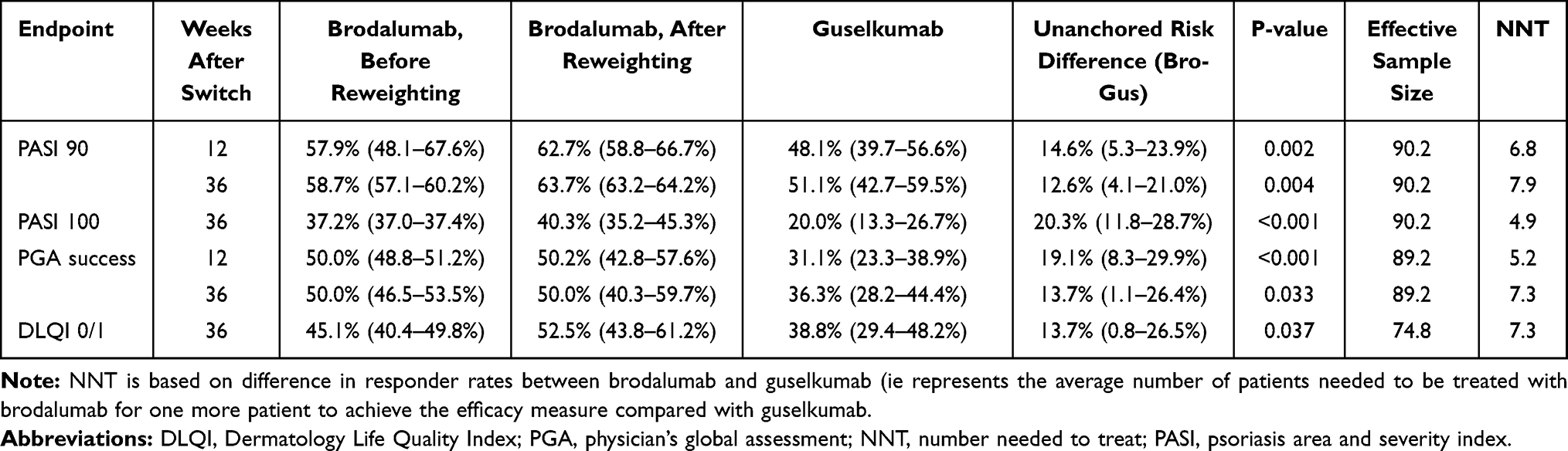 |
Table 2 PASI 90, PASI 100, PGA and DLQI Rates with Brodalumab and Guselkumab After Switching from Ustekinumab |
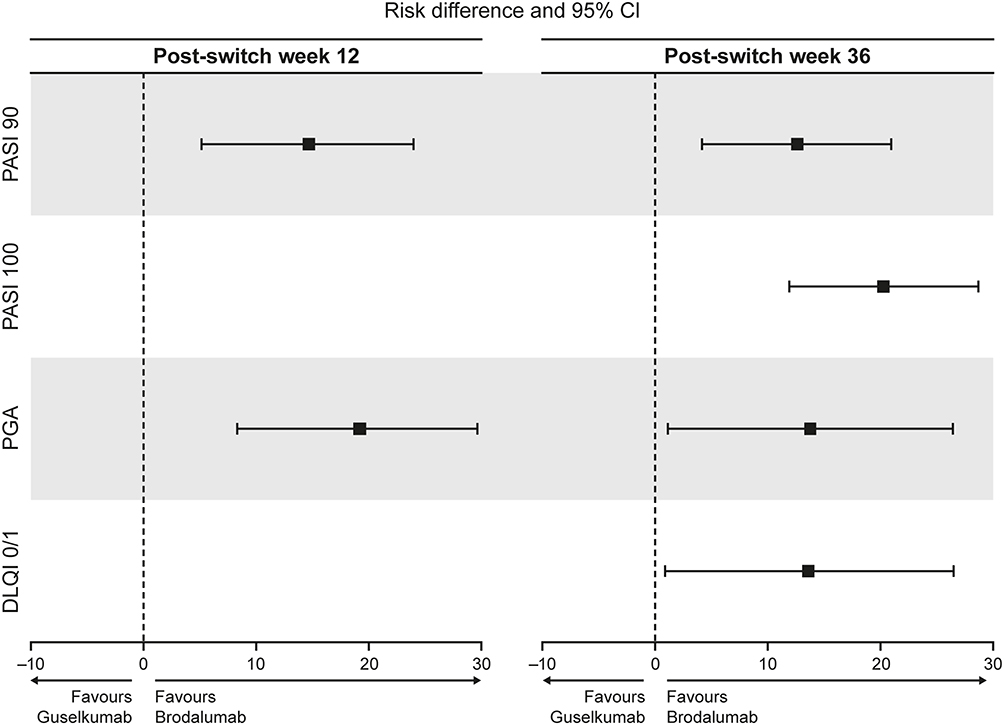 |
Figure 2 Forest plot of PASI 90, PASI 100, PGA success and DLQI 0/1 rates at 12 and 36 weeks after switching from ustekinumab. Abbreviations: CI, confidence interval; DLQI, Dermatology Life Quality Index; PASI, psoriasis area and severity index; PGA, physician’s global assessment. |
Brodalumab also resulted in significantly higher PGA success rates at week 12 (50.2% vs 31.1%; RD 19.1% [95% CI: 8.3–29.9]; p < 0.001 [NNT 5.2]) and week 36 (50.0% vs 36.3% RD 13.7% [95% CI 1.1–26.4]; p = 0.033 [NNT 7.3]). More patients had DLQI scores 0/1 at week 36 with brodalumab (52.5% vs 38.8%; RD 13.7% [95% CI 0.8–26.5]); p = 0.037 [NNT 7.3] (Figure 2).
Because of the difference between trials in the definition of an inadequate response, efficacy in patients switching from ustekinumab to brodalumab was assessed according to PGA score at week 16 (Table 3). There was a clear trend towards fewer patients with higher PGA scores at time of treatment switch achieving PASI 90/100 at 36 weeks. There was little difference between proportions of patients with a PGA of 2/3 achieving PGA success (0/1) at 12 or 36 weeks; however, fewer patients with PGA of 4/5 at time of treatment switch achieved PGA success.
 |
Table 3 PASI 90, PASI 100, and PGA Rates According to PGA Score at Time of Switching from Ustekinumab to Brodalumab |
Discussion
In this MAIC, brodalumab was associated with statistically significantly higher complete clearance rates (PASI 100), PASI 90 and PGA/IGA responder rates compared to guselkumab at 36 weeks after an inadequate response to ustekinumab. NNT for brodalumab versus guselkumab ranged from 4.9 for PASI 100 at week 36 to 7.9 for PASI 90 at week 36.
Comparative controlled trials have shown the superior efficacy of brodalumab and guselkumab versus other psoriasis treatments.1,3,15,16 In patients with moderate-to-severe plaque psoriasis, week 12 PASI 100 response rates were significantly higher with brodalumab 210 mg than with ustekinumab in the AMAGINE-2 (44% vs 22%, P < 0.001) and AMAGINE-3 studies (37% vs 19%, P < 0.001).1 Previous use of biologics did not impact the efficacy of brodalumab, with similar results in patients with or without previous exposure.17 Brodalumab has also been reported to result in significant improvement in patients who failed on IL-17A inhibitors.18 This may reflect its different mode of action since it binds to the IL-17 receptor A and directly inhibits the action of multiple pro-inflammatory IL-17 family cytokines (IL-17A, A/F, F, C and E), whereas secukinumab and ixekizumab bind to the IL-17A ligand.19–22 Guselkumab has shown superior efficacy compared with secukinumab15 and adalimumab, including in adalimumab non-responders.3,16 In the NAVIGATE trial, patients treated with ustekinumab who did not achieve an IGA score of 0/1 by week 16 derived significant benefit from switching to guselkumab.6 Brodalumab and guselkumab have also shown effectiveness in long-term, real-world settings, including in patients with failure to anti-IL17 therapies.23–26
In the absence of direct comparative trials of biological therapies for psoriasis, several network meta-analyses have been performed. In one of these, both brodalumab and guselkumab were shown to have greater short-term efficacy (ie, 10–16 weeks) when given as induction therapy than tildrakizumab, ustekinumab, TNF-α inhibitors and non-biologic systemic treatments at inducing all levels of PASI response.27 In addition, brodalumab, but not guselkumab, was significantly more effective than secukinumab and no significant differences in efficacy were reported between brodalumab and guselkumab.27 Another network meta-analysis to determine the relative efficacy and safety of guselkumab compared to other biologics as induction therapy also concluded no difference to brodalumab with regard to achieving PASI 90.28 A network meta-analysis of 60 randomized clinical trials of approved biological and oral treatments for psoriasis that assessed both short-term (10–16 weeks) as well as long-term efficacy (44–60 weeks) reported the highest PASI response rates at both timepoints with risankizumab, brodalumab, guselkumab and ixekizumab.29 Similarly, a network meta-analysis reported that brodalumab and guselkumab, along with risankizumab, were the most effective biologics in achieving PASI outcomes at one year, with no significant difference between these therapies.30 A network meta-analysis of clinical benefit over the first 16 weeks of therapy, based on area-under-the-curve for PASI 75, PASI 90, and PASI 100, suggested consistently greater benefit with the anti-IL-17 biologics ixekizumab and brodalumab versus IL-23 inhibitors, suggesting a more rapid onset of action.31
No previous studies have involved a direct head-to-head comparison of brodalumab and guselkumab in any patient group. This MAIC was conducted in the absence of an appropriate common comparator arm (ie, analysis was unanchored) and aimed to address a gap in clinical data by reweighing IPD for brodalumab versus aggregate published data for guselkumab to compare their relative efficacy in inadequate responders to ustekinumab. The potential for a small effective sample size following matching is a known limitation of MAIC, so IPD data were pooled from the AMAGINE-2 and −3 studies. Pooling IPD data is a recognized methodology to increase the potential effective sample size in MAIC.32 The effective sample size was not much lower than the number of patients with IPD, providing a sufficient number for a robust comparison and confirming that the brodalumab and guselkumab study populations were comparable.
Statistically significantly higher response rates were seen for brodalumab compared with guselkumab for all assessed endpoints. Importantly, a higher proportion of patients achieved complete and almost complete skin clearance with brodalumab, an endpoint that is increasingly recognized as a clinically achievable outcomes for many patients.33 At 36 weeks after switching from ustekinumab, NNT for PASI 100 was 4.9, meaning that on average one more will achieve complete skin clearance with brodalumab compared with guselkumab when 5 additional patients have been treated with brodalumab. These skin improvements were accompanied by a significantly greater improvement in quality-of-life with brodalumab (NNT of 7.3 for DLQI 0/1 at 36 weeks).
One possible limitation is that MAIC is based on the assumption that all effect modifiers and prognostic factors have been accounted for in the analysis. If this is not the case, the results can be affected by residual bias. Results may be confounded by differences between patient populations that were not measured or reweighted (eg, geographic regions where studies were conducted, co-morbidities, concomitant medications, etc) and unobserved differences between patient populations. The MAIC approach also assumes that the studied cohort (ie, after reweighing and matching of IPD from one trial to aggregate data from the other trial) is representative of the overall target study population.
One important difference between studies was the definition of an inadequate response to ustekinumab at 16 weeks. In the AMAGINE-2 and −3 trials,1 this was defined as a single sPGA ≥3 or sPGA ≥2 over a 4-week period, using a 6-point scale, whereas in the NAVIGATE trial [6], the definition of inadequate response was an IGA ≥2 using a 5-point scale. Although it is likely that both treatment groups were generally well-aligned, it may be that the brodalumab treatment arm included patients with slightly more severe disease. Analysis of patients switching from ustekinumab to brodalumab suggests that those with higher PGA scores at time of switch were less likely to achieve PASI 90 or 100, suggesting a potential bias in favor of guselkumab in the comparison. However, reweighting of characteristics related to disease severity should have addressed this slight imbalance.
In addition, this indirect comparison was based on efficacy endpoints only and does not take into account any potential differences between treatments in safety and tolerability, which need to be considered in therapy choice. However, previous meta-analyses have suggested both treatments are generally well tolerated with a similar safety profile.34 Also, patients only received treatment for 36 weeks after switching and long-term comparison of maintenance treatment would be useful.
Conclusions
In conclusion, this MAIC provides indirect evidence that brodalumab is associated with greater improvements than guselkumab in inadequate responders to ustekinumab after 12 and 36 weeks of treatment. Although the sample size is small, a trend was seen that indicates a higher PGA score at switch resulted in less patients achieving the efficacy outcomes. Switching to the IL-17 receptor inhibitor brodalumab in patients who fail to achieve a response with ustekinumab may be a more effective strategy than switching to the IL-23 inhibitor guselkumab, although a direct comparative randomized controlled trial is needed to provide more definitive evidence.
Ethics Approval and Informed Consent
The NAVIGATE, AMAGINE-2 and AMAGINE-3 trials were conducted in accordance with applicable country and International Conference on Harmonisation (ICH) Good Clinical Practice (GCP) regulations/guidelines. Institutional review boards at each participating centre approved the study protocols. No ethical approval was needed for this analysis because data were retrieved and analysed from previous published studies in which informed consent was obtained by primary investigators.
Acknowledgments
Medical writing and editorial assistance were provided by Andy Bond of Spirit Medical Communications Group Ltd., funded by LEO Pharma A/S. We also thank Dr José-Manuel Carrascosa (Hospital Universitari Germans Trias i Pujol, Barcelona, Spain) for his assistance. These data were in part previously presented at the ISPOR Europe 2019 Congress, 2–6 November 2019, Copenhagen, Denmark.
Author Contributions
All authors contributed to the conception, design, and execution, acquisition of data, or analysis and interpretation of data; drafted or critically revised the article for important intellectual content; have agreed on the journal to which the article has been submitted; have provided final approval of the version to be published; and agree to take responsibility and be accountable for the contents of the article.
Funding
This analysis and manuscript development was funded by LEO Pharma A/S.
Disclosure
PJH has received unrestricted research grants, educational grants and served on advisory boards for LEO Pharma, AbbVie, Lilly Pharma and Janssen. MA has served as consultant and/or paid speaker for and/or has received research grants and/or honoraries for consulting and/or scientific lectures for and/or got travel expenses reimbursed and/or participated in clinical trials sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Almirall, Amgen, Biogen (Biogen Idec), Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Galderma, Janssen-Cilag, LEO Pharma, Medac, MSD, Mundipharma, Novartis, Pfizer, Sandoz, Xenoport. EB is an employee of LEO Pharma and JBH is a former employee of LEO Pharma A/S (employee at time of data analysis and manuscript preparation). The authors report no other conflicts of interest in this work.
References
1. Lebwohl M, Strober B, Menter A, et al. Phase 3 studies comparing brodalumab with ustekinumab in psoriasis. N Engl J Med. 2015;373(14):1318–1328. doi:10.1056/NEJMoa1503824
2. Thaçi D, Blauvelt A, Reich K, et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J Am Acad Dermatol. 2015;73(3):400–409. doi:10.1016/j.jaad.2015.05.013
3. Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417. doi:10.1016/j.jaad.2016.11.041
4. Papp KA, Blauvelt A, Bukhalo M, et al. Risankizumab versus ustekinumab for moderate-to-severe plaque psoriasis. N Engl J Med. 2017;376(16):1551–1560. doi:10.1056/NEJMoa1607017
5. Papp KA, Yang M, Sundaram M, et al. Comparison of adalimumab and etanercept for the treatment of moderate to severe psoriasis: an indirect comparison using individual patient data from randomized trials. Value Health. 2018;21(1):1–8. doi:10.1016/j.jval.2017.05.025
6. Langley RG, Tsai TF, Flavin S, et al. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: results of the randomized, double-blind, phase III NAVIGATE trial. Br J Dermatol. 2018;178(1):114–123. doi:10.1111/bjd.15750
7. Paul C, Griffiths CEM, van de Kerkhof PCM, et al. Ixekizumab provides superior efficacy compared with ustekinumab over 52 weeks of treatment: results from IXORA-S, a phase 3 study. J Am Acad Dermatol. 2019;80(1):70–79.e3. doi:10.1016/j.jaad.2018.06.039
8. Reich K, Gooderham M, Thaçi D, et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet. 2019;394(10198):576–586. doi:10.1016/S0140-6736(19)30952-3
9. Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. PharmacoEconomics. 2010;28(10):935–945. doi:10.2165/11538370-000000000-00000
10. Signorovitch JE, Sikirica V, Haim Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15:940–947. doi:10.1016/j.jval.2012.05.004
11. Phillippo DM, Dias S, Elsada A, Ades AE, Welton NJ. Population adjustment methods for indirect comparisons: a review of national institute for health and care excellence technology appraisals. Int J Technol Assess Health Care. 2019;35(3):221–228. doi:10.1017/S0266462319000333
12. Warren RB, Brnabic A, Saure D, et al. Matching-adjusted indirect comparison of efficacy in patients with moderate-to-severe plaque psoriasis treated with ixekizumab vs. secukinumab. Br J Dermatol. 2018;178(5):1064–1071. doi:10.1111/bjd.16140
13. Bewley AP, Shear NH, Calzavara-Pinton PG, Hansen JB, Nyeland ME, Signorovitch J. Calcipotriol plus betamethasone dipropionate aerosol foam vs. apremilast, methotrexate, acitretin or fumaric acid esters for the treatment of plaque psoriasis: a matching-adjusted indirect comparison. J Eur Acad Dermatol Venereol. 2019;33(6):1107–1115. doi:10.1111/jdv.15369
14. Langley RG, Armstrong AW, Lebwohl MG, et al. Efficacy and safety of brodalumab in patients with psoriasis who had inadequate responses to ustekinumab: subgroup analysis of two randomized phase III trials. Br J Dermatol. 2019;180(2):306–314. doi:10.1111/bjd.17318
15. Reich K, Armstrong AW, Langley RG, et al. Guselkumab versus secukinumab for the treatment of moderate-to-severe psoriasis (ECLIPSE): results from a phase 3, randomised controlled trial. Lancet. 2019;394(10201):831–839. doi:10.1016/S0140-6736(19)31773-8
16. Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–431. doi:10.1016/j.jaad.2016.11.042
17. Papp KA, Gordon KB, Langley RG, et al. Impact of previous biologic use on the efficacy and safety of brodalumab and ustekinumab in patients with moderate-to-severe plaque psoriasis: integrated analysis of the randomized controlled trials AMAGINE-2 and AMAGINE-3. Br J Dermatol. 2018;179(2):320–328. doi:10.1111/bjd.16464
18. Kimmel G, Chima M, Kim HJ, et al. Brodalumab in the treatment of moderate to severe psoriasis in patients when previous anti-interleukin 17A therapies have failed. J Am Acad Dermatol. 2019;81(3):857–859. doi:10.1016/j.jaad.2019.05.007
19. Roman M, Chiu MW. Spotlight on brodalumab in the treatment of moderate-to-severe plaque psoriasis: design, development, and potential place in therapy. Drug Des Devel Ther. 2017;11:2065–2075. doi:10.2147/DDDT.S113683
20. Kyntheum. Summary of product characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/kyntheum-epar-product-information_en.pdf.
21. Cosentyx. Summary of product characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/cosentyx-epar-product-information_en.pdf.
22. Taltz. Summary of product characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/taltz-epar-product-information_en.pdf.
23. Galluzzo M, Caldarola G, De Simone C, et al. Use of brodalumab for the treatment of chronic plaque psoriasis: a one-year real-life study in the Lazio region, Italy. Expert Opin Biol Ther. 2021;21(9):1299–1310. doi:10.1080/14712598.2021.1941862
24. Fargnoli MC, Esposito M, Dapavo P, et al. Brodalumab for the treatment of moderate-to-severe plaque-type psoriasis: a real-life, retrospective 24-week experience. J Eur Acad Dermatol Venereol. 2021;35(3):693–700. doi:10.1111/jdv.16931
25. Megna M, Fabbrocini G, Cinelli E, Camela E, Ruggiero A. Guselkumab in moderate to severe psoriasis in routine clinical care: an Italian 44-week real-life experience. J Dermatolog Treat. 2020;4:1–5. doi:10.1080/09546634.2020.1800577
26. Ruggiero A, Fabbrocini G, Cinelli E, Megna M. Efficacy and safety of guselkumab in psoriasis patients who failed ustekinumab and/or anti-interleukin-17 treatment: a real-life 52-week retrospective study. Dermatol Ther. 2021;34(1):e14673. doi:10.1111/dth.14673
27. Sawyer LM, Malottki K, Sabry-Grant C, et al. Assessing the relative efficacy of interleukin-17 and interleukin-23 targeted treatments for moderate-to-severe plaque psoriasis: a systematic review and network meta-analysis of PASI response. PLoS One. 2019;14(8):e0220868. doi:10.1371/journal.pone.0220868
28. Cameron C, Druchok C, Hutton B, et al. Guselkumab for the treatment of moderate-to-severe plaque psoriasis during induction phase: a systematic review and network meta-analysis. J Psoriasis Psoriatic Arthritis. 2018;4(2):81–92. doi:10.1177/2475530318818816
29. Armstrong AW, Puig L, Joshi A, et al. Comparison of biologics and oral treatments for plaque psoriasis: a meta-analysis. JAMA Dermatol. 2020:156258–156269. doi:10.1001/jamadermatol.2019.4029
30. Yasmeen N, Sawyer LM, Malottki K, Levin L, Didriksen Apol E, Jemec GB. Targeted therapies for patients with moderate-to-severe psoriasis: a systematic review and network meta-analysis of PASI response at 1 year. J Dermatolog Treat. 2020;2:1–15. doi:10.1080/09546634.2020.1743811
31. Warren RB, Gooderham M, Burge R, et al. Comparison of cumulative clinical benefits of biologics for the treatment of psoriasis over 16 weeks: results from a network meta-analysis. J Am Acad Dermatol. 2019:
32. Strand V, McInnes I, Mease P, et al. Matching-adjusted indirect comparison: secukinumab versus infliximab in biologic-naive patients with psoriatic arthritis. J Comp Eff Res. 2019;8(7):497–510. doi:10.2217/cer-2018-0141
33. Korman NJ, Malatestinic W, Goldblum OM, et al. Assessment of the benefit of achieving complete versus almost complete skin clearance in psoriasis: a patient’s perspective. J Dermatolog Treat. 2020;1:1–7. doi:10.1080/09546634.2020.1772454
34. Bilal J, Berlinberg A, Bhattacharjee S, Trost J, Bin Riaz I, Kurtzman DJB. A systematic review and meta-analysis of the efficacy and safety of the interleukin (IL)-12/23 and IL-17 inhibitors ustekinumab, secukinumab, ixekizumab, brodalumab, guselkumab and tildrakizumab for the treatment of moderate to severe plaque psoriasis. J Dermatolog Treat. 2018;29(6):569–578. doi:10.1080/09546634.2017.1422591
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.