")
Back to Journals » OncoTargets and Therapy » Volume 11
Efficacy of bevacizumab versus epidermal growth factor receptor inhibitors for wild-type RAS metastatic colorectal cancer: a meta-analysis
Authors Jiang W, Yu Q , Ning R, Zhao W, Wei C
Received 20 March 2018
Accepted for publication 24 May 2018
Published 24 July 2018 Volume 2018:11 Pages 4271—4281
DOI https://doi.org/10.2147/OTT.S168695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Wei Jiang,1,* Qitao Yu,1,* Ruiling Ning,1 Wenhua Zhao,1 Changyuan Wei2
1Department of Medical Oncology, Tumor Hospital Affiliated to Guangxi Medical University, Nanning, People’s Republic of China; 2Department of Breast Surgery, Tumor Hospital Affiliated to Guangxi Medical University, Nanning, People’s Republic of China
*These authors contributed equally to this work
Background: Results from several prospective clinical trials comparing anti-epidermal growth factor receptor (EGFR) therapy and anti-vascular endothelial growth factor (VEGF) therapy plus chemotherapy for wild-type RAS metastatic colorectal cancer (mCRC) have been inconsistent. This meta-analysis aims to investigate the optimal choice for these target agents.
Methods: We searched for clinical trials in both electronic databases from inception until January 2018 and recent conference abstracts to identify prospective clinical studies comparing the efficacy of a VEGF inhibitor (bevacizumab) versus EGFR inhibitors (cetuximab or panitumumab) on wild-type RAS (including its subset KRAS) mCRC. All analyses were conducted using RevMan 5.3 software.
Results: A total of 5 studies were included. EGFR inhibitors were associated with a significant benefit in terms of overall survival (OS) compared with VEGF inhibitors in wild-type KRAS or wild-type RAS populations, with hazard ratios (HRs) equal to 0.86 (95% CI: 0.78, 0.95; p=0.003) and 0.83 (95% CI: 0.72, 0.95; p=0.007), respectively. This survival benefit was limited to the first-line setting. No difference was found for progression-free survival (PFS), whereas the objective response rate (ORR) was significantly increased in the wild-type RAS population (OR: 0.64; 95% CI: 0.50, 0.82; p=0.0004). No difference in OS was noted between EGFR inhibitors versus a VEGF inhibitor plus the FOLFIRI regimen, whereas superior survival was noted for EGFR inhibitors plus the mFOLFOX6 regimen versus a VEGF inhibitor (HR: 0.75; 95% CI: 0.57, 0.98; p=0.04). PFS was significantly prolonged (HR: 1.48; 95% CI: 1.14, 1.92; p=0.003), whereas a trend favoring OS (HR: 1.23; 95% CI: 0.93, 1.63; p=0.14) was noted for a VEGF inhibitor in patients with right-sided tumors, with no difference in the ORR (OR: 0.85; 95% CI: 0.52, 1.38; p=0.51). However, left-sided tumors exhibited superior OS (HR: 0.71; 95% CI: 0.59, 0.85; p=0.0002), PFS (HR: 0.84; 95% CI: 0.72, 0.98; p=0.03), and ORR (OR: 0.66; 95% CI: 0.48, 0.92; p=0.01) for EGFR inhibitors.
Conclusion: This meta-analysis suggests the superiority of anti-EGFR therapy compared with anti-VEGF therapy for mCRC with wild-type RAS. Primary tumor location should be taken into account in target drug selection. Further research is still needed to confirm which inhibitor may be a better choice when combined with different chemotherapy regimens.
Keywords: bevacizumab, cetuximab, panitumumab, colorectal cancer, meta-analysis
Introduction
Fluorouracil- and folinic acid-based cytotoxic chemotherapeutic combinations with either oxaliplatin (mFOLFOX6 regimen) or irinotecan (FOLFIRI regimen) have significantly increased the life expectancy of patients with mCRC.1,2 Currently, therapies combining the mFOLFOX6 regimen or FOLFIRI regimen with biologic monoclonal antibodies further improve survival and are standard first-line treatments.3–5
Bevacizumab is one of the major targeting agents that block the activity of VEGF-A and play an important antiangiogenesis role in tumors. Several studies have demonstrated that the addition of bevacizumab to traditional chemotherapeutic cytotoxic drugs provides survival benefits to patients with mCRC.3,6
EGFR inhibitors represent another essential class of targeted drugs used in mCRC. Cetuximab and panitumumab are examples of EGFR inhibitors currently approved by the US Food and Drug Administration (FDA). EGFR inhibitors can competitively and specifically bind to the receptor and block downstream signaling. However, mutations in RAS, a downstream gene, can induce constitutive activation of the intracellular pathway of the EGFR signaling cascade independent of EGFR, resulting in tumor proliferation, diffusion, and primary anti-EGFR therapy resistance. The major RAS genes, KRAS, NRAS, and HRAS, are the most common oncogenes in CRC. A sizable body of research indicates that patients with a mutation in codons 12 and 13 of KRAS exon 2 do not respond to anti-EGFR therapy.4,7 Therefore, these agents are not suggested for the treatment of mCRC patients with KRAS mutations based on FDA recommendations. More recent studies have provided further evidence that KRAS mutations outside of exon 2 and NRAS mutations are also negative predictive markers for the efficacy of cetuximab and panitumumab therapy.8,9 A meta-analysis concluded that EGFR inhibitors provided significant clinical benefit in patients with wild-type RAS mCRC.10
Although the addition of a VEGF inhibitor or EGFR inhibitors to standard chemotherapy yields greater activity than cytotoxic chemotherapy alone and although this combination regimen is commonly used in first- or second-line therapy, which inhibitor offers superior efficacy in combination with chemotherapy for patients with wild-type KRAS, even wild-type RAS, mCRC remains controversial. Here, we performed this meta-analysis to review available clinical trial data to evaluate the efficacy of chemotherapy in combination with a VEGF inhibitor versus EGFR inhibitors in patients with wild-type RAS mCRC, including wild-type KRAS mCRC.
Methods
Literature search
We searched for clinical trials published in electronic databases (PubMed, Embase, and the Cochrane databases) from inception until January 2018. The following 4 search terms were used: “metastatic colorectal cancer”, “bevacizumab”, “cetuximab”, and “panitumumab”. We also manually searched conference abstracts from the ASCO and ESMO to update included studies and to search for additional eligible trials. We also assessed the references of the included studies for other potentially eligible studies.
Study selection criteria
Eligible studies were required to meet the following inclusion criteria: 1) prospective clinical studies that compare the efficacy of VEGF inhibitor (bevacizumab) and EGFR inhibitors (cetuximab or panitumumab) in mCRC patients regardless of the study regimen and number of previous treatments; and 2) articles that were published in English.
Data extraction and quality assessment
The Cochrane Collaboration Guidelines guided the quality assessment of the studies, data collection, risk of bias evaluation, and analysis. Two review authors independently assessed all relevant articles retrieved for inclusion. All disagreements between the 2 reviewers were resolved by consensus or by a third investigator. The data of feasible studies were extracted according to the protocol of Cochrane. For each study, we extracted the following standard information from 2 populations (wild-type KRAS and wild-type RAS): the trial title, first author, year of publication, phase, target agents, combination chemotherapeutic regimen, number of included patients, number of previous treatments, primary tumor location, and main outcome of the treatment. Given that all published information adequately addressed the main questions, we did not ask for individual data.
Definitions of outcomes
The ORR was assessed according to the RECIST. PFS was defined as the time of study entry until the first evidence of disease progression or death for any cause, whichever occurred first. The time of study entry until death was defined as OS.
Statistical analyses
All analyses were conducted using the program Review Manager Version 5.3, which was developed and is freely available from the Cochrane Collaboration. In this meta-analysis, dichotomous data (ORR) were assessed for statistical efficacy analysis using the odds ratio (OR) with 95% CI. Survival variables were evaluated using the hazard ratio (HR). Heterogeneity across studies was assessed using the I2 statistic. An I2 value <25% indicated minimal heterogeneity, whereas a value from 25% to 50% indicated moderate heterogeneity. In this case, the fixed-effect model was used for the meta-analysis. If there was a significant heterogeneity (I2>50%), a random-effects model was used. For all analyses, p-values <0.05 were considered statistically significant. Publication bias was judged using funnel plots. The quality of the studies was assessed using the Jadad quality score.
Results
Search result
After the initial search of network databases, a total of 1,010 publications were identified according to the search strategy. An additional 28 publications were identified from conference abstracts. Of these results, 1,018 publications were duplicates or not relevant to the topic and therefore excluded after screening the titles and abstracts. Of the 20 possibly eligible publications, 3 were reviews and 3 were meta-analyses. Hence, the full texts of 14 publications were assessed in detail. One study26 was ongoing. In addition, 7 publications originated from the same study (FIRE-3),12,13 and 3 publications originated from another study (PEAK).14,15 Finally, 5 studies were included in this analysis. Figure 1 presents the PRISMA Statement diagram for selection of results. Table 1 summarizes the characteristics of the included studies. Of the 5 studies considered for the analysis, 2 publications were Phase III trials, and 3 publications were Phase II trials. CALGB/SWOG 80405,11 FIRE-3,12,13 and PEAK14,15 were first-line studies comparing the treatment efficacy of chemotherapy combined with EGFR inhibitors versus a VEGF inhibitor in mCRC, whereas SPIRITT16 and WJOG 6210G17 were designed to evaluate treatment outcomes between EGFR inhibitors and a VEGF inhibitor in mCRC refractory to first-line chemotherapy plus bevacizumab. All included studies were considered high-quality trials, with quality scores of all equal to 3.
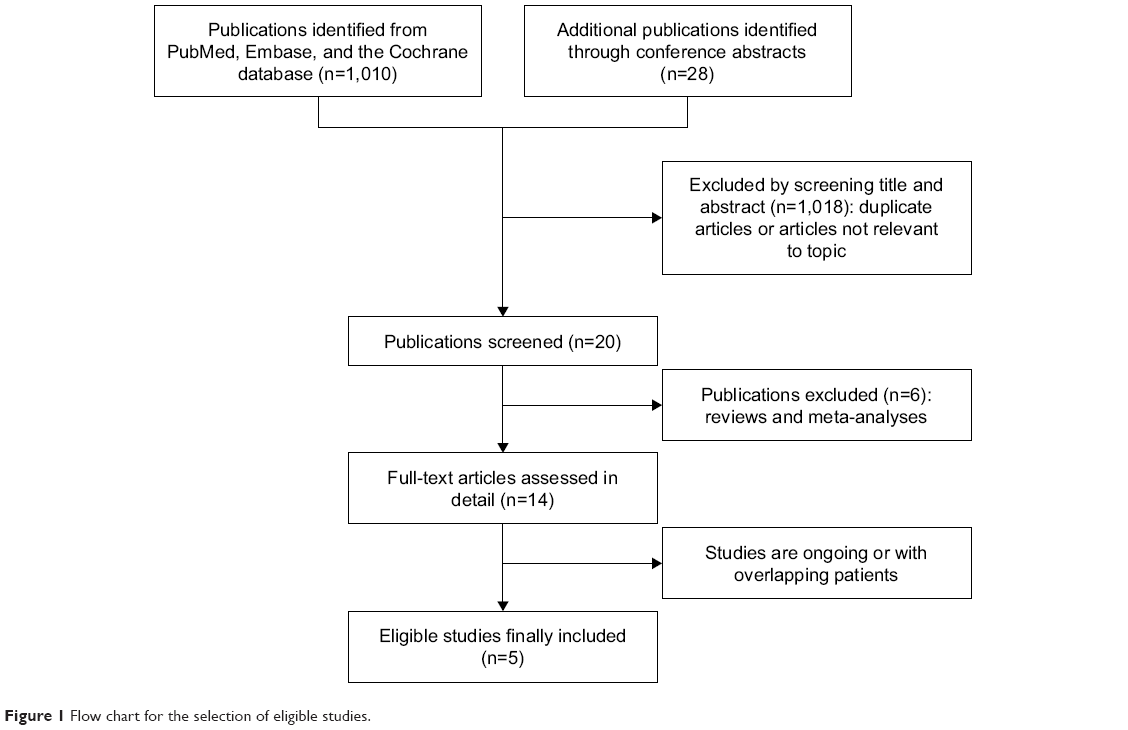 | Figure 1 Flow chart for the selection of eligible studies. |
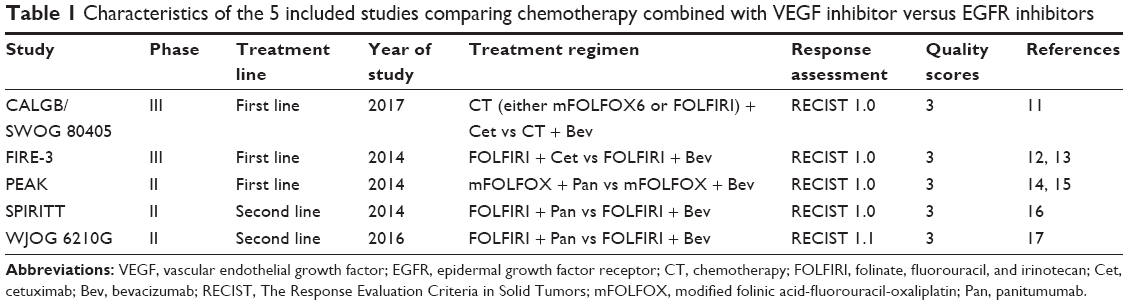 | Table 1 Characteristics of the 5 included studies comparing chemotherapy combined with VEGF inhibitor versus EGFR inhibitors |
Outcome of meta-analysis
All of the included studies were initially designed to investigate treatment outcomes of anti-EGFR therapy versus anti-VEGF therapy in a wild-type KRAS population and reported key efficacy data (Table 2). Therefore, we performed a meta-analysis of efficacy in this ITT population first. For the wild-type KRAS population, OS was significantly prolonged in patients receiving EGFR inhibitors compared to that in patients receiving a VEGF inhibitor, with a pooled HR equal to 0.86 (95% CI: 0.78, 0.95; p=0.003) (Figure 2A). However, no significant difference in PFS was observed (HR: 0.98; 95% CI: 0.90, 1.08; p=0.71) (Figure 2B). To eliminate heterogeneity, analyses of the ORR excluded second-line studies. A trend of increased ORR was noted for EGFR inhibitors, with a pooled OR of 1.10 (95% CI: 1.00, 1.43; p=0.05) (Figure 2C).
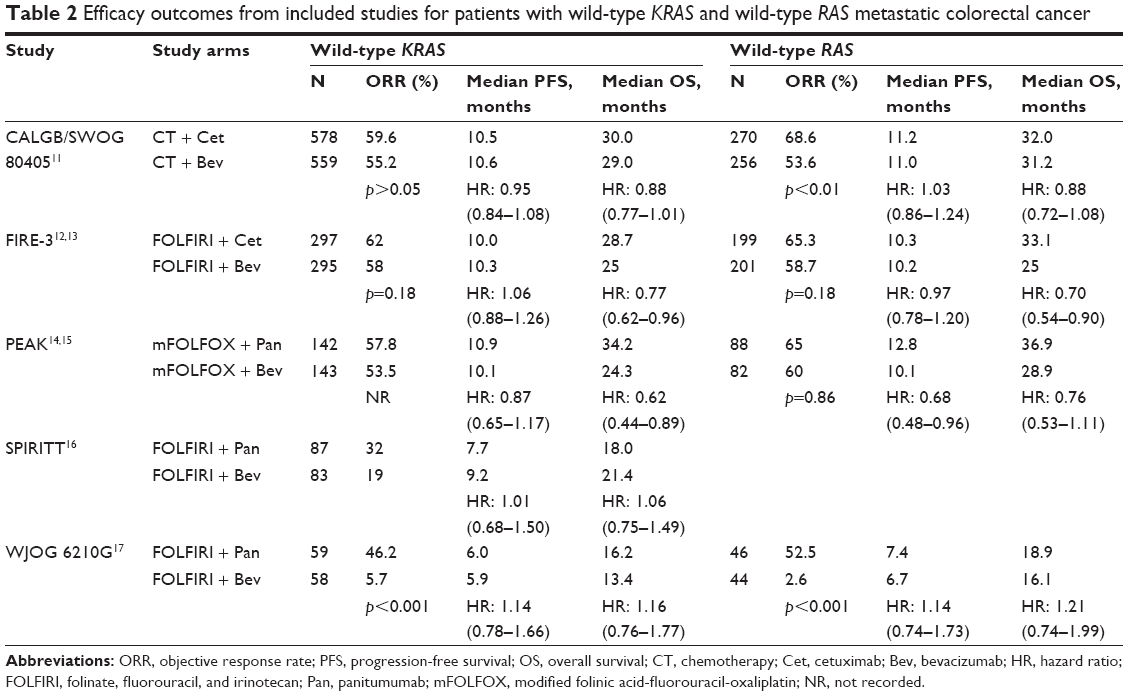 | Table 2 Efficacy outcomes from included studies for patients with wild-type KRAS and wild-type RAS metastatic colorectal cancer |
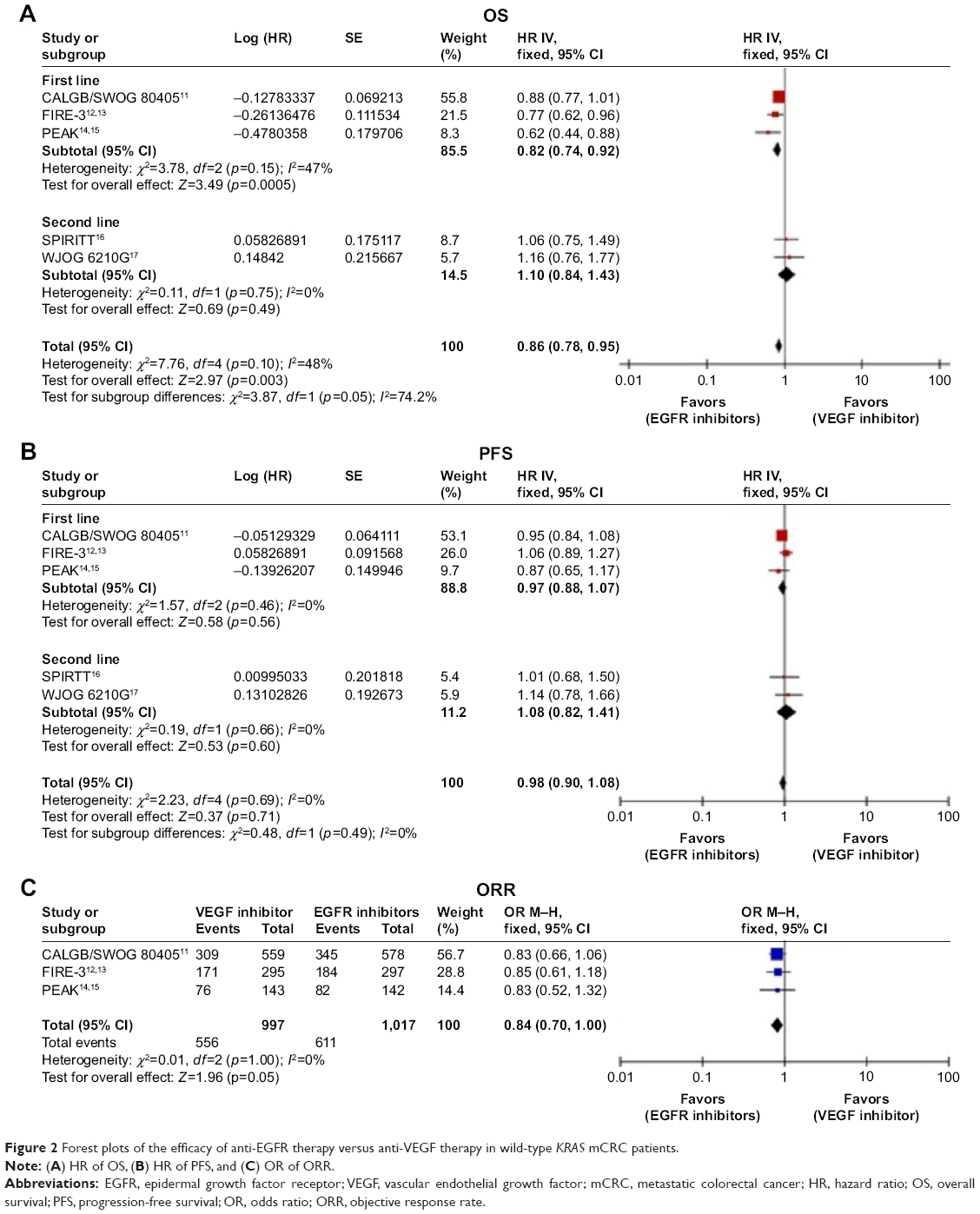 | Figure 2 Forest plots of the efficacy of anti-EGFR therapy versus anti-VEGF therapy in wild-type KRAS mCRC patients. |
In subgroup analyses, OS remained prolonged for wild-type KRAS patients treated with EGFR inhibitors as first-line therapy (HR: 0.82; 95% CI: 0.74, 0.92; p=0.0005). However, this survival benefit disappeared in second-line therapy (HR: 1.10; 95% CI: 0.84, 1.43; p=0.49). Neither first-line nor second-line studies revealed significant differences in PFS, with HRs equal to 0.97 (95% CI: 0.88, 1.07; p=0.56) and 1.08 (95% CI: 0.82, 1.41; p=0.60), respectively.
With regard to chemotherapy regimen, no difference in OS was observed between EGFR inhibitors and a VEGF inhibitor combined with the FOLFIRI regimen (Figure 3A), whereas the analysis indicated a survival benefit for EGFR inhibitors combined with the mFOLFOX6 regimen compared with a VEGF inhibitor (HR: 0.75; 95% CI: 0.57, 0.98; p=0.04). Given the significant heterogeneity (I2=54%), a random-effects model was used (Figure 3B).
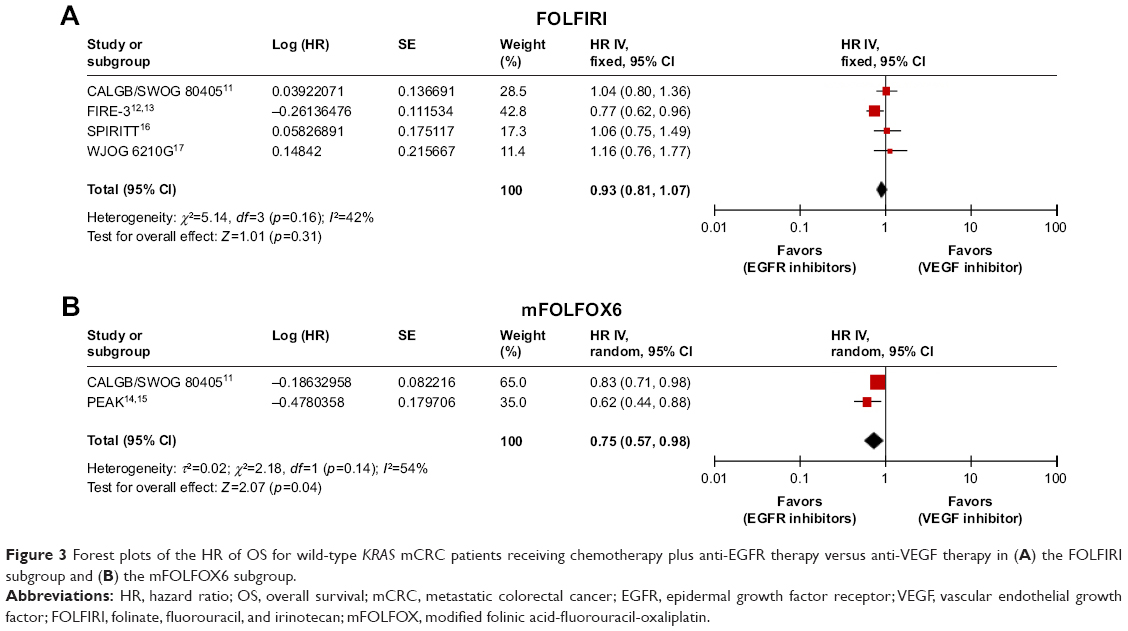 | Figure 3 Forest plots of the HR of OS for wild-type KRAS mCRC patients receiving chemotherapy plus anti-EGFR therapy versus anti-VEGF therapy in (A) the FOLFIRI subgroup and (B) the mFOLFOX6 subgroup. |
Of the 5 included studies, 4 studies reported the efficacy data of the wild-type RAS (Table 2). EGFR inhibitors also demonstrated a superior survival benefit in this population (HR: 0.83; 95% CI: 0.72, 0.95; p=0.007) (Figure 4A), but no difference in PFS was observed (HR: 0.97; 95% CI: 0.85, 1.09; p=0.58) (Figure 4B). After the exclusion of a second-line study (WJOG 6210G17) to minimize heterogeneity, the ORR was significantly increased in wild-type RAS mCRC treated with EGFR inhibitors compared with that treated with a VEGF inhibitor (OR: 0.64; 95% CI: 0.50, 0.82; p=0.0004) (Figure 4C).
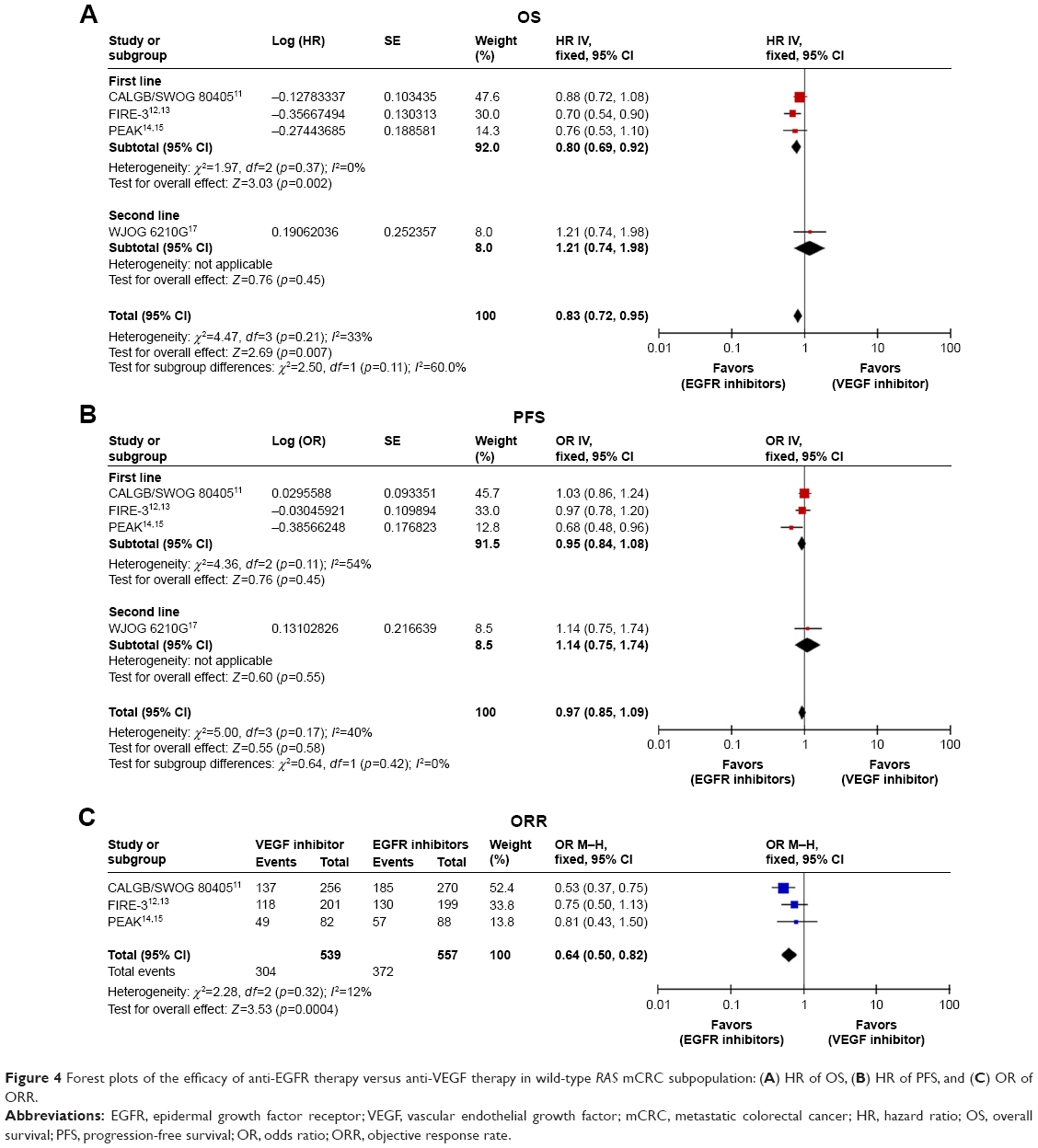 | Figure 4 Forest plots of the efficacy of anti-EGFR therapy versus anti-VEGF therapy in wild-type RAS mCRC subpopulation: (A) HR of OS, (B) HR of PFS, and (C) OR of ORR. |
Given the definite prognostic and predictive value, primary tumor location was also assessed as a stratified factor (Figure 5). The analyses were performed based on 3 studies (Table 3). In the wild-type RAS setting where the primary tumor originated on the right side, PFS was significantly prolonged (HR: 1.48; 95% CI: 1.14, 1.92; p=0.003), with a trend favoring OS (HR: 1.23; 95% CI: 0.93, 1.63; p=0.14) when a VEGF inhibitor was administered. However, no difference in the ORR (OR: 0.85; 95% CI: 0.52, 1.38; p=0.51) was noted for the VEGF inhibitor. In contrast, left-sided primary tumors demonstrated superior OS (HR: 0.71; 95% CI: 0.59, 0.85; p=0.0002), PFS (HR: 0.84; 95% CI: 0.72, 0.98; p=0.03), and ORR (OR: 0.66; 95% CI: 0.48, 0.92; p=0.01) with EGFR inhibitors.
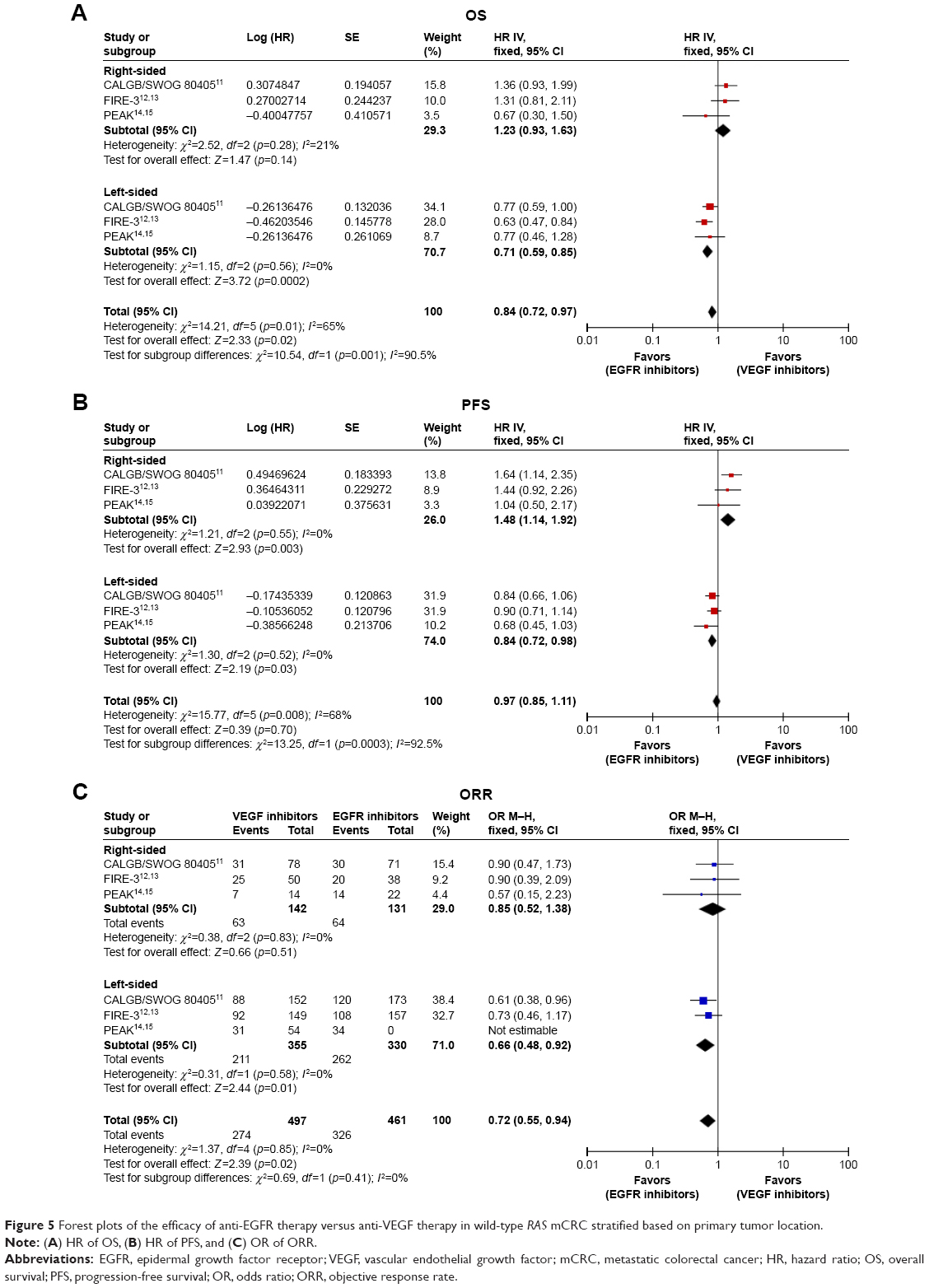 | Figure 5 Forest plots of the efficacy of anti-EGFR therapy versus anti-VEGF therapy in wild-type RAS mCRC stratified based on primary tumor location. |
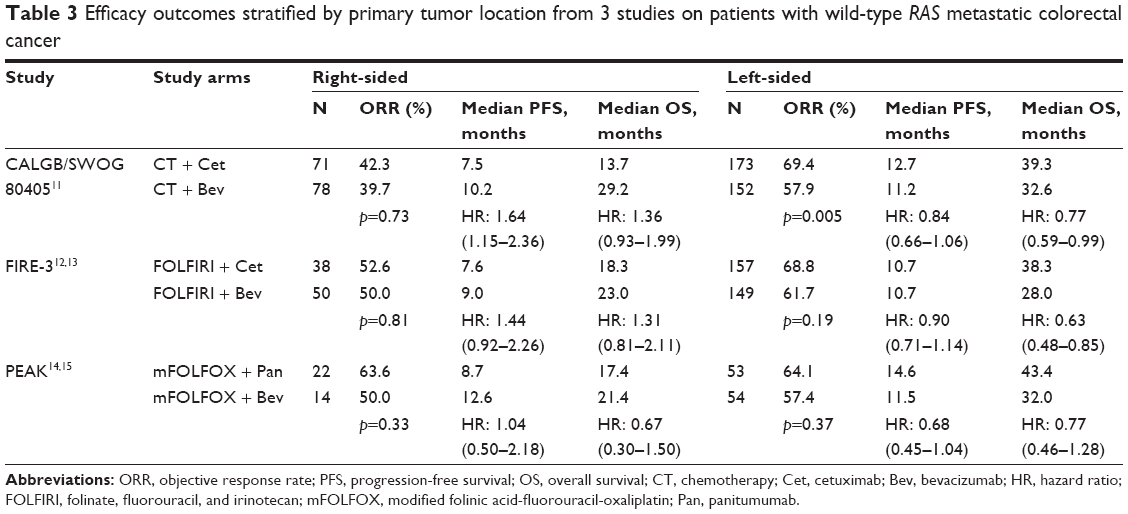 | Table 3 Efficacy outcomes stratified by primary tumor location from 3 studies on patients with wild-type RAS metastatic colorectal cancer |
Discussion
EGFR and VEGF inhibitors are both monoclonal antibodies sharing equal importance in mCRC treatment, but these inhibitors utilize completely different mechanisms. Anti-VEGF therapy blocks the activity of VEGF-A and inhibits tumor angiogenesis. In CRC, RAS gene mutations upregulate VEGF expression and promote tumor angiogenesis. Thus, a VEGF inhibitor may be effective in either mutant or wild-type RAS CRC. However, EGFR is upstream of RAS, and RAS gene mutations could activate the downstream signaling cascade independent of EGFR. Although EGFR is blocked, its downstream pathway remains active. Thus, EGFR inhibitors exhibit treatment benefits exclusively in wild-type RAS CRC. With these questions clarified, the clinical trials comparing treatment efficacy between EGFR inhibitors and VEGF inhibitors gradually included only wild-type RAS patients. However, the optimal target therapy remains less clear, specifically in wild-type RAS mCRC.
This meta-analysis indicates the survival benefit of OS in wild-type RAS populations receiving EGFR inhibitors plus chemotherapy compared with VEGF inhibitors; no differences with respect to PFS were noted. Although the superiority in OS was comparable between the wild-type KRAS and RAS populations in our analysis, most published studies present evidence that exclusion of patients with any other RAS mutations allowed for the more selective use of EGFR inhibitors within a narrower group of mCRC patients who are most likely to benefit from treatment. Considering that 2 trials of second-line therapies recruited patients progressing on chemotherapy plus bevacizumab, we did not include these trials in the ORR analysis. A nonsignificant trend toward an improved ORR was demonstrated in the wild-type KRAS population with the addition of EGFR inhibitors, and this improvement became more pronounced in the wild-type RAS population, as expected.
The ITT population of all included trials was the wild-type KRAS population, but the primary analysis of this setting revealed conflicting results based on efficacy data. Although extended RAS testing excluded more EGFR inhibitor-insensitive patients from the ITT population, the conclusions from subgroup analysis of the expanded wild-type RAS cohort remain inconsistent. Three additional meta-analyses compared the treatment effect of EGFR inhibitors versus a VEGF inhibitor. Specifically, 2 of these studies were conducted in a first-line setting and indicated a superior ORR and OS in wild-type RAS mCRC patients receiving EGFR inhibitors.18,19 Wang reported additional results including retrospective studies and second-line studies that demonstrated the advantage of anti-EGFR therapy versus anti-VEGF therapy for OS and ORR as a first-line therapy for wild-type KRAS and RAS mCRC.20 The present meta-analysis adds to this information by updating efficacy data from randomized trials, not considering retrospective studies, taking primary tumor location into account, and providing more power and a valuable assessment. Of note, longer OS correlated with treatment line. A clear OS advantage was demonstrated in first-line therapy favoring EGFR inhibitors, but this improvement was not noted in second-line therapy, with an increased ORR and no significant effect on PFS. We attribute the cause of the discrepancy among OS, PFS, and ORR to 3 reasons. First, the mechanism may involve the sequence of different target drugs. In vitro and in vivo, acquired resistance to EGFR inhibitors is related to upregulation of VEGF, and inhibition of VEGF signaling could overcome the resistance.21,22 Regarding treatment strategy, these results may support the administration of anti-VEGF therapy after resistance emerges to first-line EGFR inhibitors. Second, the accuracy of RECIST in the evaluation of the treatment outcome of target therapy remains controversial. This criterion cannot detect changes in tumor biology after anti-VEGF and anti-EGFR therapy. Finally, many clinical studies have demonstrated that earlier and better tumor response indicates better OS.
This meta-analysis has several limitations. Clinical and histologic features differ between right-sided and left-sided CRCs, which probably lead to the disparity in treatment outcomes based on the primary tumor site.23 CALGB/SWOG 8040511 revealed that OS and PFS were prolonged in patients with wild-type KRAS mCRC originating on the left side who received cetuximab and in patients with primary tumors originating on the right side who received bevacizumab; however, OS and PFS were reduced in patients with primary tumors originating on the right side who received cetuximab.24 A retrospective analysis of FIRE-325 based on tumor side revealed results similar to those of CALGB/SWOG 80405.24 Our stratification analysis also provided evidence that EGFR inhibitors exhibited superior efficacy in patients with left-sided primary tumor. Although our research based on primary tumor side only included 3 studies, target therapy is recommended based on location per current guidelines. Given that this additional covariate was not anticipated to affect the efficacy of target agents, another limitation of our study is that it relied on an unknown or imbalanced status of treatment arms based on tumor side distribution or between trials of included studies. In terms of the chemotherapy backbone, the imbalance in mFOLFOX6 and FOLFIRI regimens between treatment arms or included studies should also be taken into account. Interestingly, this analysis indicated that the treatment outcomes of EGFR and VEGF inhibitors were comparable when combined with the FOLFIRI regimen. However, improved survival was noted for anti-EGFR therapy in combination with the mFOLFOX6 regimen. However, the mFOLFOX6 regimen was only administered in the PEAK study14,15 and to the majority of patients (73%) in CALGB/SWOG 80405.11 Therefore, the possibility that the survival benefits of EGFR inhibitors in the entire patient population are derived from the mFOLFOX6 regimen setting should be further explored. Given the possible interaction between chemotherapy regimens and target agents, this limitation of our study should be considered. Given that only 2 trials were included and that heterogeneity was present, it remains quite difficult to draw a definite conclusion that EGFR inhibitors are more effective than VEGF inhibitor in combination with mFOLFOX6. Whether anti-EGFR therapy represents a better choice for combination with the mFOLFOX6 regimen requires further validation. Finally, there is insufficient information regarding subsequent therapy from each included trial, which would potentially affect our results, if an imbalance existed.
Conclusion
This meta-analysis suggests the superiority of anti-EGFR therapy compared with anti-VEGF therapy for treating wild-type RAS mCRC, particularly for primary tumors that originate on the left side. Further research is still needed to confirm whether anti-EGFR or anti-VEGF represents a better choice when combined with different chemotherapy regimens and to identify predictive markers of treatment efficacy.
Abbreviations
EGFR, epidermal growth factor receptor; VEGF, vascular endothelial growth factor; mCRC, metastatic colorectal cancer; OS, overall survival; PFS, progression-free survival; ORR, objective response rate; ITT, intention-to-treat; ASCO, American Society of Clinical Oncology; ESMO, European Society for Medical Oncology; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses Statement; RECIST, Response Evaluation Criteria in Solid Tumors.
Acknowledgment
The authors indicate no funding sources.
Disclosure
The authors report no conflicts of interest in this work.
References
Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 2000;343(13):905–914. | ||
de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000;18(16):2938–2947. | ||
Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. | ||
Van Cutsem E, Kohne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408–1417. | ||
Peeters M, Price TJ, Cervantes A, et al. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol. 2010;28(31):4706–4713. | ||
Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013–2019. | ||
Amado RG, Wolf M, Peeters M, et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J Clin Oncol. 2008;26(10):1626–1634. | ||
Douillard JY, Oliner KS, Siena S, et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med. 2013;369(11):1023–1034. | ||
Peeters M, Oliner KS, Parker A, et al. Massively parallel tumor multigene sequencing to evaluate response to panitumumab in a randomized phase III study of metastatic colorectal cancer. Clin Cancer Res. 2013;19(7):1902–1912. | ||
Sorich MJ, Wiese MD, Rowland A, Kichenadasse G, McKinnon RA, Karapetis CS. Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: a meta-analysis of randomized, controlled trials. Ann Oncol. 2015;26(1):13–21. | ||
Venook AP, Niedzwiecki D, Lenz HJ, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced or metastatic colorectal cancer: a randomized clinical trial. JAMA. 2017;317(23):2392–2401. | ||
Heinemann V, von Weikersthal LF, Decker T, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(10):1065–1075. | ||
Stintzing S, Modest DP, Rossius L, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): a post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol. 2016;17(10):1426–1434. | ||
Schwartzberg LS, Rivera F, Karthaus M, et al. PEAK: a randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J Clin Oncol. 2014;32(21):2240–2247. | ||
Rivera F, Karthaus M, Hecht JR, et al. Final analysis of the randomised PEAK trial: overall survival and tumour responses during first-line treatment with mFOLFOX6 plus either panitumumab or bevacizumab in patients with metastatic colorectal carcinoma. Int J Colorectal Dis. 2017;32(8):1179–1190. | ||
Hecht JR, Cohn A, Dakhil S, et al. SPIRITT: a randomized, multicenter, phase II study of panitumumab with FOLFIRI and bevacizumab with FOLFIRI as second-line treatment in patients with unresectable wild type KRAS metastatic colorectal cancer. Clin Colorectal Cancer. 2015;14(2):72–80. | ||
Shitara K, Yonesaka K, Denda T, et al. Randomized study of FOLFIRI plus either panitumumab or bevacizumab for wild-type KRAS colorectal cancer-WJOG 6210G. Cancer Sci. 2016;107(12):1843–1850. | ||
Khattak MA, Martin H, Davidson A, Phillips M. Role of first-line anti-epidermal growth factor receptor therapy compared with anti-vascular endothelial growth factor therapy in advanced colorectal cancer: a meta-analysis of randomized clinical trials. Clin Colorectal Cancer. 2015;14(2):81–90. | ||
Heinemann V, Rivera F, O’Neil BH, et al. A study-level meta-analysis of efficacy data from head-to-head first-line trials of epidermal growth factor receptor inhibitors versus bevacizumab in patients with RAS wild-type metastatic colorectal cancer. Eur J Cancer. 2016;67:11–20. | ||
Wang H, Ma B, Gao P, et al. Efficacy and safety of anti-epidermal growth factor receptor therapy compared with anti-vascular endothelial growth factor therapy for metastatic colorectal cancer in first-line and second-line therapies: a meta-analysis. Onco Targets Ther. 2016;9:5405–5416. | ||
Viloria-Petit A, Crombet T, Jothy S, et al. Acquired resistance to the antitumor effect of epidermal growth factor receptor-blocking antibodies in vivo: a role for altered tumor angiogenesis. Cancer Res. 2001;61(13):5090–5101. | ||
Ciardiello F, Bianco R, Caputo R, et al. Antitumor activity of ZD6474, a vascular endothelial growth factor receptor tyrosine kinase inhibitor, in human cancer cells with acquired resistance to antiepidermal growth factor receptor therapy. Clin Cancer Res. 2004;10(2):784–793. | ||
Schrag D, Weng S, Brooks G, et al. The relationship between primary tumor sidedness and prognosis in colorectal cancer. J Clin Oncol. 2016;34:Supplement 15. | ||
Venook AP, Niedzwiecki D, Innocenti F, et al. Impact of primary (1°) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): analysis of CALGB/SWOG 80405 (Alliance). J Clin Oncol. 2016;34:Supplement 15. | ||
Tejpar S, Stintzing S, Ciardiello F, et al. Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. Epub 2016 Oct 10. | ||
Muro K, Uetake H, Tsuchihara K, et al. PARADIGM study: A multicenter, randomized, phase III study of mFOLFOX6 plus panitumumab or bevacizumab as first-line treatment in patients with RAS (KRAS/NRAS) wildtype metastatic colorectal cancer. J Clin Oncol. 2016;34:Supplement 15. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.