")
Back to Journals » Drug Design, Development and Therapy » Volume 12
Efficacy of atorvastatin on the prevention of contrast-induced acute kidney injury: a meta-analysis
Authors Liu L, Liu Y, Wu M, Sun Y, Ma F
Received 14 August 2017
Accepted for publication 7 October 2017
Published 2 March 2018 Volume 2018:12 Pages 437—444
DOI https://doi.org/10.2147/DDDT.S149106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qiongyu Guo
Ling-Yun Liu,1 Yang Liu,2 Mei-Yan Wu,2 Yan-Yan Sun,3 Fu-Zhe Ma2
1Department of Andrology, 2Department of Nephrology, the First Hospital of Jilin University, 3Department of Nephrology, the Fourth Hospital of Jilin University, Changchun, China
Background: Results of studies on the efficacy of atorvastatin pretreatment on reducing the prevalence of contrast-induced acute kidney injury (CIAKI) in patients undergoing coronary angiography (CAG) or percutaneous coronary intervention (PCI) have been controversial.
Objective: We undertook a meta-analysis to evaluate the efficacy of atorvastatin on contrast-induced nephropathy (CIN) after CAG or PCI.
Materials and methods: We undertook a systematic search of electronic databases (PubMed, Embase, and the Cochrane Library) up to June 2017. A meta-analysis was carried out including randomized controlled trials (RCTs) that compared atorvastatin pretreatment with pretreatment with a low-dose statin or placebo for CIAKI prevention in patients undergoing CAG. The main endpoint was CIN prevalence.
Results: Nine RCTs were included in our meta-analysis. Atorvastatin pretreatment reduced the prevalence of CIN significantly (odds ratio [OR] 0.46; 95% confidence interval [95% CI] 0.27–0.79; p=0.004). The benefit of high-dose atorvastatin pretreatment was consistent when compared with the control group (OR 0.45; 95% CI 0.21–0.95; p=0.04).
Conclusion: At high doses, atorvastatin pretreatment was associated with a significant reduction in the prevalence of CIAKI in patients undergoing CAG. Pretreatment with high-dose atorvastatin could be employed to prevent CIAKI.
Keywords: atorvastatin, contrast-induced acute kidney injury, coronary angiography, percutaneous coronary intervention, contrast-induced nephropathy, meta-analysis
Introduction
Contrast-induced acute kidney injury (CIAKI) is a well-recognized vasoconstriction of renal arteries triggered by contrast media. CIAKI is a major contributor to hospital-acquired acute renal failure and is associated with mortality. Patients with acute coronary syndrome, baseline renal insufficiency, and those undergoing percutaneous coronary intervention (PCI) carry a higher risk for CIAKI, which may be a common cause of persistent worsening of renal function.1,2
Recently, interventional cardiologists have paid close attention to post-PCI CIAKI. Several studies have been carried out to explore the pathogenesis of contrast-induced nephropathy (CIN). Some studies have suggested that a potential interaction between oxidative stress, inflammation, reduction in renal blood flow, and direct damage to tubular cells by contrast media might be involved in CIN pathogenesis.3 Other mechanisms of action include delayed intra-renal transit of the contrast agent caused by vasoconstriction resulting in damage by oxidative stress and direct damage to tubular cells due to receptor-mediated tubular reabsorption of filtered contrast.4,5
Several approaches have examined how to prevent CIAKI. Among those approaches, pharmacologic prophylactic strategies based on antioxidant properties have garnered considerable interest. Studies using N-acetylcysteine have been debated widely.6 Unfortunately, the development of treatments has shown little clinical efficacy for CIAKI prevention.7
Statins are prescribed frequently for the treatment of cardiovascular disease. However, they have recently been suggested to enhance endothelial function as well as reduce oxidative stress and inflammation.8 It has been reported that short-term pretreatment with statins can achieve lipid-lowering pleiotropic effects such as a reduction in the prevalence of myocardial damage during PCI,9–12 possibly via antioxidant, anti-inflammatory effects,9 as well as their tendency to reduce endothelin secretion.13 Inflammatory mechanisms and oxidative stress may also affect the pathogenesis of CIN.14,15 Moreover, statins may reduce the reabsorption of contrast agents in renal tubules, thereby reducing toxicity within them.5,16 Therefore, statins are considered to be promising candidate agents to prevent CIN. However, a consensus on the beneficial effects of statins on CIAKI prevention is lacking.
Several randomized clinical trials (RCTs) have failed to show that statins exert beneficial effects on CIAKI prevention.17–22 Conversely, some studies have reported that atorvastatin pretreatment can reduce the prevalence of CIN more effectively than other statins because it can reduce inflammation and oxidative stress to a greater extent.
Atorvastatin may work through different mechanisms to prevent activation of an intrinsic apoptotic pathway. Prospective studies have suggested that atorvastatin may have effects on CIN, but the results are conflicting. Hence, we undertook a meta-analysis to evaluate the role of atorvastatin in the prevention of CIAKI compared with control groups.
Materials and methods
Search strategy
A systematic search of PubMed, Embase, and the Cochrane Library databases up to June 2017 was carried out using the keywords “atorvastatin” and “contrast-induced acute kidney injury”. Relevant medical subject heading terms were utilized. The reference lists of all articles were also checked for potential additional eligible studies.
Eligibility criteria
Studies were included in the meta-analysis 1) if they were original studies evaluating the effectiveness of atorvastatin pretreatment in reducing the prevalence of CIAKI in patients undergoing PCI; 2) if they offered information about CIAKI; 3) if the main endpoint was the prevalence of CIN; 4) if they contained reference groups composed of participants who were prescribed atorvastatin compared with a control group; and 5) if the articles were written in English.
Assessment of the quality of studies
Two investigators rated the quality of eligible RCTs independently. We chose the risk of bias items for RCTs as recommended by the Cochrane Handbook for Systematic Reviews of Interventions.
Data extraction
Two independent investigators extracted the data from included studies. Differing conclusions were resolved by consensus. For each of the eligible studies, the main categories were the name of the first author, characteristics of the RCT, study design, year of publication, number of study patients, patient age, eligibility criteria of each RCT, and definition of CIAKI in each RCT.
“High-dose atorvastatin” was defined as atorvastatin administered at a daily dose of ≥80 mg. “Low-dose atorvastatin” was defined as atorvastatin administered at a daily dose of <80 mg.
Statistical analyses
All endpoint comparisons were calculated using Review Manager v5.3 (Revman; the Cochrane Collaboration, Oxford, UK). Odds ratios (ORs) and their 95% confidence intervals (CIs), or relevant data for their calculation, were used to assess the prevalence of CIN events between the atorvastatin group and control group. The OR and its 95% CI were also mentioned in the summary statistics for the pooled analysis of the effect to assess the prevalence of CIN events between the high-dose atorvastatin group and control group. Statistical variables were pooled directly if they were described in the literature; otherwise, the variables were calculated based on the available numerical data in the articles according to the methods described by Parmar et al.23
The endpoint was considered as a weighted average of the individual estimate of the OR in each included study using the inverse variance method.
A sensitivity analysis was also carried out to examine the impact on the overall results depending on the heterogeneity across the included studies. The I2 test was carried out to assess the heterogeneity of the results.24 Studies with an I2 of 25%–50%, 50%–75%, or >75% were considered to have “low”, “moderate”, or “high” heterogeneity, respectively.25 If there was low heterogeneity among the studies, the fixed-effects model was used. Otherwise, the random-effects model was used. p<0.05 was considered significant.
Results
Overview of the literature search and study characteristics
A total of 326 studies were found based on the inclusion criteria stated earlier. Eighteen publications were evaluated in more detail, but some did not provide the endpoint of the study.
Finally, nine RCTs were included.20,22,26–32 The literature search is described in Figure 1. All included studies were considered to be of moderate quality at least. Table 1 shows the detailed medication protocols of the eligible studies in more detail.
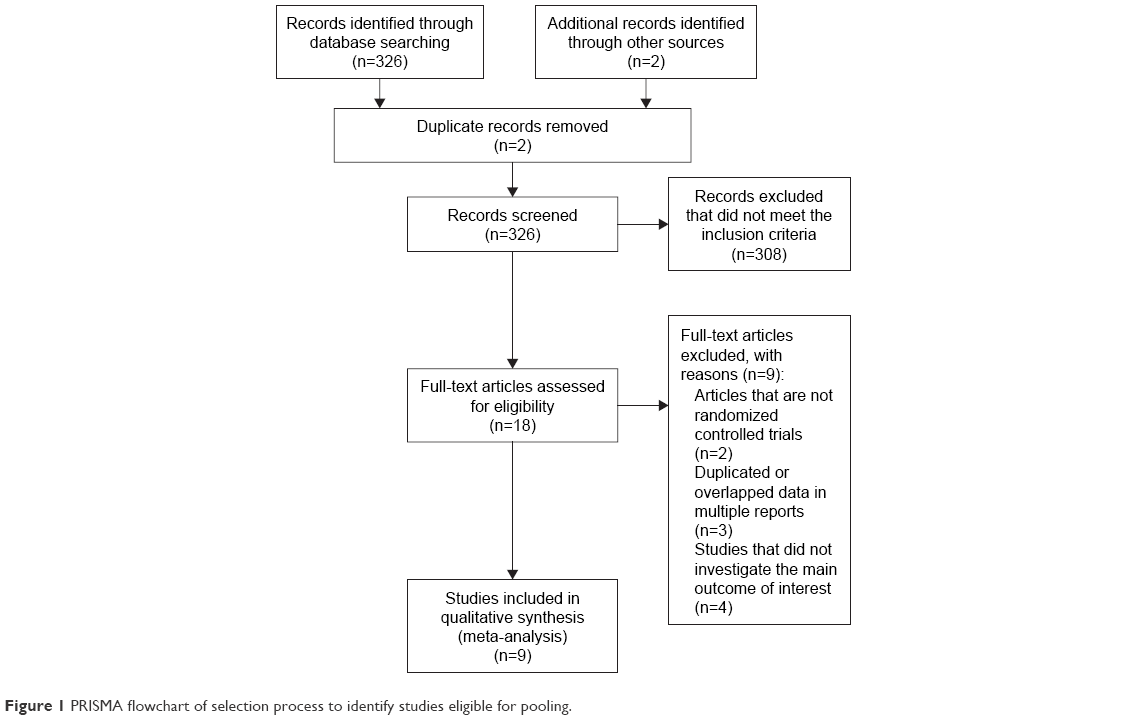 | Figure 1 PRISMA flowchart of selection process to identify studies eligible for pooling. |
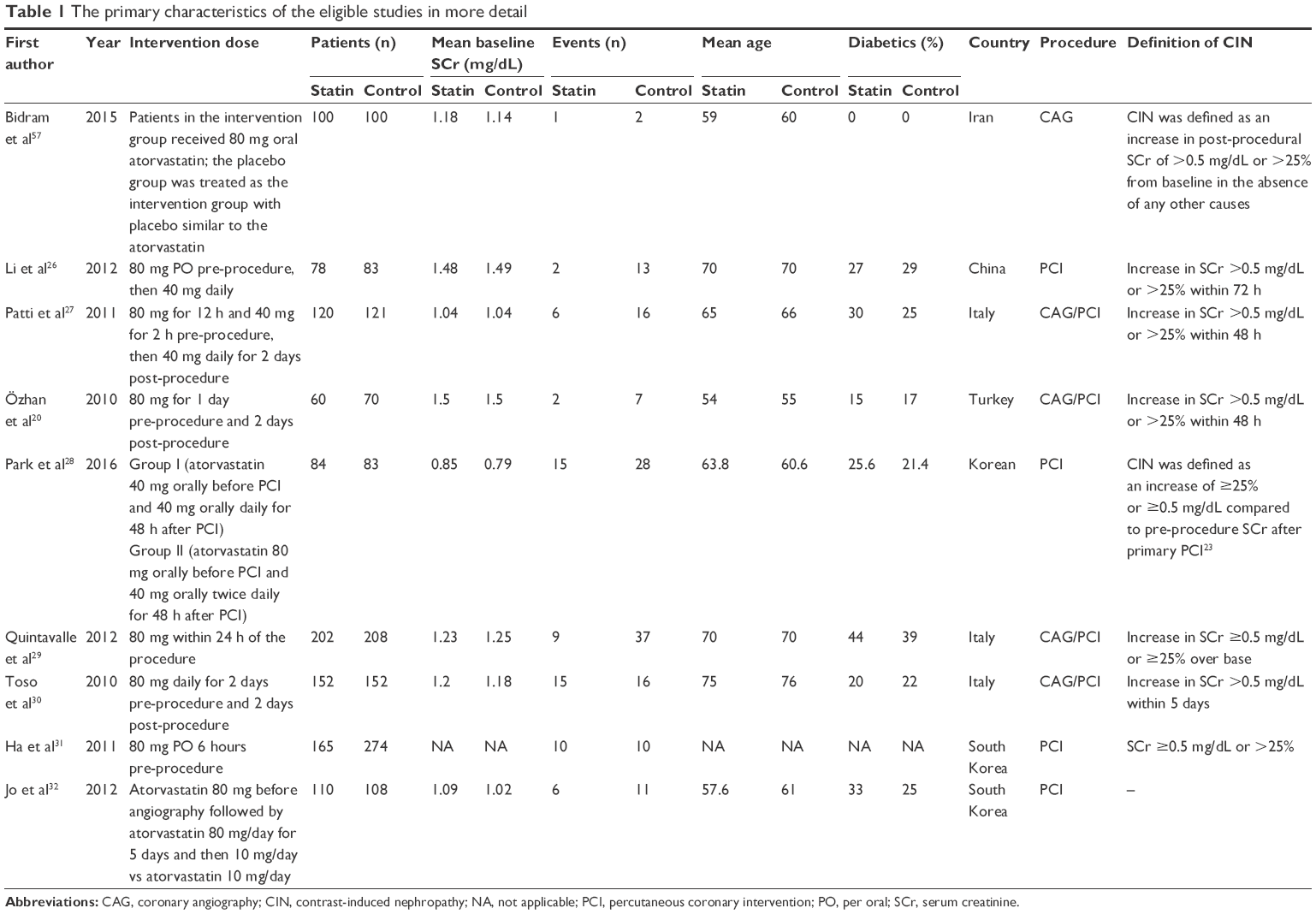 | Table 1 The primary characteristics of the eligible studies in more detail |
Effect of atorvastatin on CIAKI prevalence
Pooling the data from all nine RCTs showed that atorvastatin could reduce the risk of CIAKI (OR 0.46; 95% CI 0.27–0.79; p=0.004) compared with the control group (Figure 2).
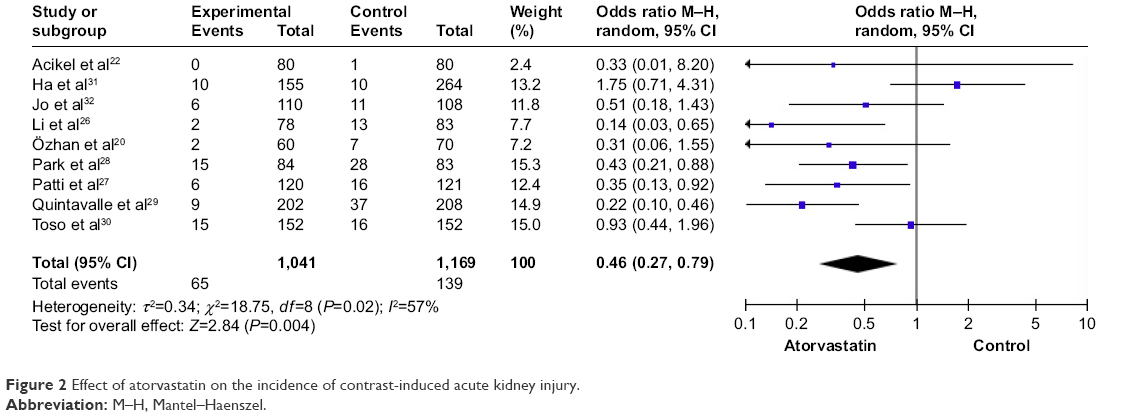 | Figure 2 Effect of atorvastatin on the incidence of contrast-induced acute kidney injury. |
Effect of high-dose atorvastatin on CIAKI prevalence
High-dose atorvastatin reduced the risk of CIAKI (OR 0.45; 95% CI 0.21–0.95; p=0.04) when compared with the placebo group (Figure 3). Only two RCTs reported data on high-dose atorvastatin compared with low-dose atorvastatin, so a meta-analysis could not be carried out.
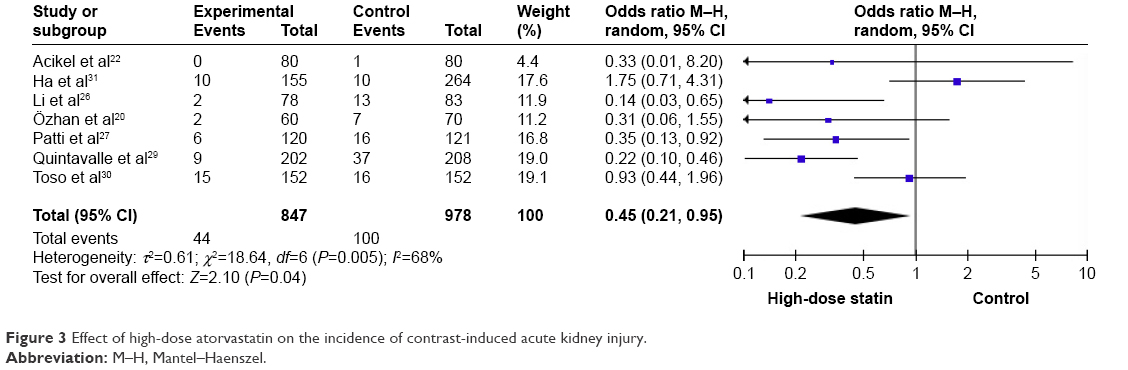 | Figure 3 Effect of high-dose atorvastatin on the incidence of contrast-induced acute kidney injury. |
Discussion
Contrast media induce decreasing production of local prostaglandin-mediated vasodilatation and the damage caused by oxygen radicals, known as CIN.15 CIN is reported to be a leading cause of in-hospital acute renal failure. The prevalence of CIN differs widely across RCTs depending on the risk profiles of different patients, such as advanced age, diabetes mellitus, cardiovascular disease, and preexisting renal dysfunction.33–35 Development of CIN after PCI in patients with normal renal function or further deterioration in renal function in those with chronic renal failure might be followed by in-hospital adverse events and a higher risk of late cardiovascular events and mortality.33–35 Thus, prevention of CIN may translate into improved clinical outcome during follow-up.
A large number of drugs have been used to prevent kidney injury following PCI,36–38 including statins, but the optimal regimen for preventing CIN is not known. Various mechanisms are involved in CIN pathogenesis, and several studies have reported that statins may be effective in preventing CIN.39,40 Inflammation and reactive oxygen species (ROS) production may contribute to CIAKI pathogenesis. Clinical and experimental results have clearly shown that hypoxia and increased production of ROS within the kidney following administration of contrast media affect CIN development.41
Previously, the possible role of statins in the prevention of renal deterioration in patients undergoing diagnostic or therapeutic angiographic procedures has been investigated. Statins have been used widely for primary and secondary prevention of coronary artery disease. Studies have reported the cholesterol-independent or pleiotropic effects of statins, including amelioration of endothelial function, stabilization of atherosclerotic plaques, as well as reduction of systemic inflammation and oxidative stress.42
Several RCTs have reported that statins have beneficial effects on reducing CIAKI prevalence.43,44 The underlying pathophysiologic mechanisms are complex. In addition to their impact on cholesterol, statins may help to prevent CIAKI causing direct toxicity to renal tubules, oxidative stress, and ischemic injury,45 but some conflicting results have been obtained.46,47
Among the statins available, atorvastatin has multiple beneficial pleiotropic effects of 3-hydroxy-3-methyl-glutaryl-CoA reductase inhibitors. Atorvastatin can improve endothelial function, stabilize coronary plaques, suppress the proliferation of smooth muscle cells in vessels and platelet aggregation, and reduce inflammation and oxidative stress.42
Recently, the possible role of atorvastatin in preventing renal deterioration in patients undergoing diagnostic or therapeutic angiographic procedures has been investigated. Atorvastatin may modulate kidney hypoperfusion after radiocontrast exposure by downregulating expression of angiotensin receptors and reducing synthesis of endothelin-1.48 Also, the anti-inflammatory effect of atorvastatin may prevent damage to renal cells by reducing the expression of pro-inflammatory cytokines. This phenomenon can induce the expression of tissue factors by macrophages and activate the nuclear factor-kappa B pathway,49 and renal protection by atorvastatin after PCI is probably due to such attenuation of expression (though other pleiotropic effects may be responsible). However, observational reports on this topic have produced conflicting results. In our meta-analysis, atorvastatin treatment was shown to reduce the prevalence of CIN significantly.
The effective dose of high-dose atorvastatin for CIAKI prevention is not known. Results from studies focusing on the efficacy of high-dose statin pretreatment to prevent CIAKI are inconsistent.50,51 Recently, three RCTs with relatively large cohorts (NAPLES II, PRATO-ACS, TRACK-D) reported promising results, suggesting that high-dose statins can reduce the prevalence of CIAKI.29,52,53 Considering the beneficial effects of pretreatment with high-dose statins, we evaluated the efficacy of pretreatment with high-dose atorvastatin in reducing the prevalence of CIAKI. The pooled analysis showed that high-dose atorvastatin reduced the risk of CIN in patients undergoing coronary angiography with iodinated contrast media compared with control (placebo or low-dose statin).
Although administration of a high-dose statin clearly showed a beneficial effect in preventing CIAKI, the adverse effects of high-dose statins may result in lasting damage. In the TRACK-D trial,52 the authors reported that the prevalence of adverse effects such as muscle pain, gastrointestinal disorders, liver-function abnormalities, edema, or rash was not significantly different between high-dose statin and control groups. Data on adverse events in the RCTs included in our meta-analysis were limited, so we could not calculate the hazard ratios of pretreatment with high-dose atorvastatin. Also, there are insufficient RCT data to ascertain reliably if higher doses of statin therapy are more efficacious than lower doses. Data from two RCTs have reported conflicting results.28,32
Our meta-analysis is the first study to compare the effect of atorvastatin for CIAKI prevention in patients undergoing coronary angiography. Previous meta-analyses on similar topics have shown inconsistent results about the efficacy of statin pretreatment mainly because of the limited sample sizes of included trials.54–56 However, two inherent flaws of our meta-analysis must be mentioned because they could have led to biases. First, all RCTs included in our meta-analysis used different definitions of CIAKI. Second, due to a lack of patient-level data, we could not adjust for patient-level confounders. Hence, clinical heterogeneity among trials should be taken into consideration when interpreting our findings.
Conclusion
At high doses, atorvastatin pretreatment was associated with a significant reduction in the prevalence of CIAKI in patients undergoing coronary angiography. Pretreatment with high-dose atorvastatin could be employed to prevent CIAKI.
Disclosure
The authors report no conflicts of interest in this work.
References
McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Am J Cardiol. 2006;98:5–13. | ||
Klein LW, Sheldon MW, Brinker J, et al. The use of radiographic contrast media during PCI: a focused review: a position statement of the Society of Cardiovascular Angiography and Interventions. Catheter Cardiovasc Inter. 2009;74:728–746. | ||
McCullough PA. Multimodality prevention of contrast-induced acute kidney injury. Am J Kidney Dis. 2008;51:169–172. | ||
McCullough PA. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2008;51:1419–1428. | ||
Verhulst A, D’Haese PC, De Broe ME. Inhibitors of HMG-CoA reductase reduce receptor-mediated endocytosis in human kidney proximal tubular cells. J Am Soc Nephrol. 2004;15:2249–2257. | ||
Kelly AM, Dwamena B, Cronin P, Bernstein SJ, Carlos RC. Meta-analysis: effectiveness of drugs for preventing contrast-induced nephropathy. Ann Int Med. 2008;148:284–294. | ||
Kitzler TM, Jaberi A, Sendlhofer G, et al. Efficacy of vitamin E and N-acetylcysteine in the prevention of contrast induced kidney injury in patients with chronic kidney disease: a double blind, randomized controlled trial. Wien Klin Wochenschr. 2012;124:312–319. | ||
Farmer JA. Pleiotropic effects of statins. Curr Atheroscler Rep. 2000;2:208–217. | ||
Patti G, Chello M, Pasceri V, et al. Protection from procedural myocardial injury by atorvastatin is associated with lower levels of adhesion molecules after percutaneous coronary intervention: results from the ARMYDA-CAMs (Atorvastatin for Reduction of MYocardial Damage during Angioplasty-Cell Adhesion Molecules) substudy. J Am Coll Cardiol. 2006;48:1560–1566. | ||
Pasceri V, Patti G, Nusca A, et al. Randomized trial of atorvastatin for reduction of myocardial damage during coronary intervention: results from the ARMYDA (Atorvastatin for Reduction of MYocardial Damage during Angioplasty) study. Circulation. 2004;110:674–678. | ||
Patti G, Pasceri V, Colonna G, et al. Atorvastatin pretreatment improves outcomes in patients with acute coronary syndromes undergoing early percutaneous coronary intervention: results of the ARMYDA-ACS randomized trial. J Am Coll Cardiol. 2007;49:1272–1278. | ||
Di Sciascio G, Patti G, Pasceri V, Gaspardone A, Colonna G, Montinaro A. Efficacy of atorvastatin reload in patients on chronic statin therapy undergoing percutaneous coronary intervention: results of the ARMYDA-RECAPTURE (Atorvastatin for Reduction of Myocardial Damage During Angioplasty) randomized trial. J Am Coll Cardiol. 2009;54:558–565. | ||
Zhang B-C, Li W-M, Xu Y-W. High-dose statin pretreatment for the prevention of contrast-induced nephropathy: a meta-analysis. Can J Cardiol. 2011;27:851–858. | ||
Goldenberg I, Matetzky S. Nephropathy induced by contrast media: pathogenesis, risk factors and preventive strategies. Can Med Assoc J. 2005;172:1461–1471. | ||
Wong PCY, Li Z, Guo J, Zhang A. Pathophysiology of contrast-induced nephropathy. Int J Cardiol. 2012;158:186–192. | ||
Leoncini M, Toso A, Maioli M, Tropeano F, Bellandi F. Statin treatment before percutaneous coronary intervention. J Thorac Dis. 2013;5:335–342. | ||
Kandula P, Shah R, Singh N, Markwell SJ, Bhensdadia N, Navaneethan SD. Statins for prevention of contrast-induced nephropathy in patients undergoing non-emergent percutaneous coronary intervention. Nephrology. 2010;15:165–170. | ||
Wang H, Chen H, Pan Y, Yang S. Effect of atorvastatin on renal function in patients given contrast medium after interventional procedures. Medical Journal of the Chinese People’s Armed Police Forces. 2009;20:919–922. | ||
Galal H, Nammas W, Samir A. Impact of high dose versus low dose atorvastatin on contrast induced nephropathy in diabetic patients with acute coronary syndrome undergoing early percutaneous coronary intervention. The Egyptian Heart Journal. 2015;67:329–336. | ||
Özhan H, Erden I, Ordu S, et al. Efficacy of short-term high-dose atorvastatin for prevention of contrast-induced nephropathy in patients undergoing coronary angiography. Angiology. 2010;61:711–714. | ||
Oliveira MSD, Martins KBA, Costa JR Jr, et al. Impact on renal function of rosuvastatin preload prior to elective percutaneous coronary intervention in chronic statin users. Revista Brasileira de Cardiologia Invasiva (English Edition). 2012;20:303–308. | ||
Acikel S, Muderrisoglu H, Yildirir A, et al. Prevention of contrast-induced impairment of renal function by short-term or long-term statin therapy in patients undergoing elective coronary angiography. Blood Coagul Fibrinolysis. 2010;21:750–757. | ||
Parmar MKB, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17:2815–2834. | ||
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–1558. | ||
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. | ||
Li W, Fu X, Wang Y, et al. Beneficial effects of high-dose atorvastatin pretreatment on renal function in patients with acute ST-segment elevation myocardial infarction undergoing emergency percutaneous coronary intervention. Cardiology. 2012;122:195–202. | ||
Patti G, Ricottini E, Nusca A, et al. Short-term, high-dose atorvastatin pretreatment to prevent contrast-induced nephropathy in patients with acute coronary syndromes undergoing percutaneous coronary intervention (from the ARMYDA-CIN [Atorvastatin for Reduction of MYocardial Damage during Angioplasty–Contrast-Induced Nephropathy] trial). Am J Cardiol. 2011;108:1–7. | ||
Park SH, Jeong MH, Park IH, et al. Effects of combination therapy of statin and N-acetylcysteine for the prevention of contrast–induced nephropathy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Int J Cardiol. 2016;212:100–106. | ||
Quintavalle C, Fiore D, De Micco F, et al. Impact of a high loading dose of atorvastatin on contrast-induced acute kidney injury. Circulation. 2012;126:3008–3016. | ||
Toso A, Maioli M, Leoncini M, et al. Usefulness of atorvastatin (80 mg) in prevention of contrast-induced nephropathy in patients with chronic renal disease. Am J Cardiol. 2010;105:288–292. | ||
Ha SJ, Maioli M, Leoncini M, et al. Usefulness of statin pretreatment to prevent contrast-induced nephropathy in patients undergoing elective percutaneous coronary intervention in real world. Eur Heart J. 2011;32:1041. | ||
Jo S-H, Hahn JY, Lee SY, et al. TCT-147 high dose atorvastatin pretreatment for preventing contrast-induced nephropathy in patients receiving primary percutaneous coronary intervention: prespecified substudy of a prospective randomized clinical trial. J Am Coll Cardiol. 2012;60:B42–B43. | ||
Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention. J Am Coll Cardiol. 2004;44:1393–1399. | ||
Gruberg L, Mintz GS, Mehran R, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol. 2000;36:1542–1548. | ||
Mehran R, Brar S, Dangas G. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2010;55:2210–2211. | ||
Zhang J, Fu X, Jia X, et al. B-type natriuretic peptide for prevention of contrast-induced nephropathy in patients with heart failure undergoing primary percutaneous coronary intervention. Acta Radiol. 2010;51:641–648. | ||
Thiele H, Hildebrand L, Schirdewahn C, et al. Impact of high-dose N-acetylcysteine versus placebo on contrast-induced nephropathy and myocardial reperfusion injury in unselected patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. The LIPSIA-N-ACC (Prospective, Single-Blind, Placebo-Controlled, Randomized Leipzig Immediate PercutaneouS Coronary Intervention Acute Myocardial Infarction N-ACC) Trial. J Am Coll Cardiol. 2010;55:2201–2209. | ||
Motohiro M, Kamihata H, Tsujimoto S, et al. A new protocol using sodium bicarbonate for the prevention of contrast-induced nephropathy in patients undergoing coronary angiography. Am J Cardiol. 2011;107:1604–1608. | ||
Stacul F, Adam A, Becker CR, et al. Strategies to reduce the risk of contrast-induced nephropathy. Am J Cardiol. 2006;98:59–77. | ||
Barrett BJ, Parfrey PS. Preventing nephropathy induced by contrast medium. N Engl J Med. 2006;354:379–386. | ||
Katholi RE, Woods WT Jr, Taylor GJ, et al. Oxygen free radicals and contrast nephropathy. Am J Kidney Dis. 1998;32:64–71. | ||
Liao JK, Laufs U. Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol. 2004;45:89–118. | ||
Attallah N, Yassine L, Musial J, Yee J, Fisher K. The potential role of statins in contrast nephropathy. Clin Nephrol. 2004;62:273–278. | ||
Khanal S, Attallah N, Smith DE, et al. Statin therapy reduces contrast-induced nephropathy: an analysis of contemporary percutaneous interventions. Am J Med. 2005;118:843–849. | ||
Haller C, Hizoh I. The cytotoxicity of iodinated radiocontrast agents on renal cells in vitro. Invest Radiol. 2004;39:149–154. | ||
Zhao J-L, Yang YJ, Zhang YH, You SJ, Wu YJ, Gao RL. Effect of statins on contrast-induced nephropathy in patients with acute myocardial infarction treated with primary angioplasty. Int J Cardiol. 2008;126:435–436. | ||
Yoshida S, Kamihata H, Nakamura S, et al. Prevention of contrast-induced nephropathy by chronic pravastatin treatment in patients with cardiovascular disease and renal insufficiency. J Cardiol. 2009;54:192–198. | ||
Ichiki T, Takeda K, Tokunou T, et al. Downregulation of angiotensin II type 1 receptor by hydrophobic 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors in vascular smooth muscle cells. Arterioscl Thromb Vasc Biol. 2001;21:1896–1901. | ||
Bonetti PO, Lerman LO, Napoli C, Lerman A. Statin effects beyond lipid lowering – are they clinically relevant? Eur Heart J. 2003;24:225–248. | ||
Pappy R, Stavrakis S, Hennebry TA, Abu-Fadel MS. Effect of statin therapy on contrast-induced nephropathy after coronary angiography: a meta-analysis. Int J Cardiol. 2011;151:348–353. | ||
Jo S-H, Koo BK, Park JS, et al. Prevention of radiocontrast medium–induced nephropathy using short-term high-dose simvastatin in patients with renal insufficiency undergoing coronary angiography (PROMISS) trial – a randomized controlled study. Am Heart J. 2008;155:499.e491–499.e498. | ||
Han Y, Zhu G, Han L, et al. Short-term rosuvastatin therapy for prevention of contrast-induced acute kidney injury in patients with diabetes and chronic kidney disease. J Am Coll Cardiol. 2014;63:62–70. | ||
Leoncini M, Toso A, Maioli M, Tropeano F, Villani S, Bellandi F. Early high-dose rosuvastatin for contrast-induced nephropathy prevention in acute coronary syndrome. J Am Coll Cardiol. 2014;63:71–79. | ||
Takagi H, Umemoto T. A meta-analysis of randomized trials for effects of periprocedural atorvastatin on contrast-induced nephropathy. Int J Cardiol. 2011;153:323–325. | ||
Zhang L, Zhang L, Lu Y, et al. Efficacy of statin pretreatment for the prevention of contrast-induced nephropathy: a meta-analysis of randomised controlled trials. Int J Clin Pract. 2011;65:624–630. | ||
Zhang T, Shen LH, Hu LH, He B. Statins for the prevention of contrast-induced nephropathy: a systematic review and meta-analysis. Am J Nephrol. 2011;33:344–351. | ||
Bidram P, Roghani F, Sanei H, et al. Atorvastatin and prevention of contrast induced nephropathy following coronary angiography. J Res Med Sci. 2015;20(1):1–6. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.