")
Back to Journals » Clinical Ophthalmology » Volume 16
Efficacy of a One-Piece Aberration Neutral Hydrophobic Acrylic Toric Intraocular Lens
Authors Buckhurst PJ , Lau G, Williams JI, Packer M
Received 9 September 2022
Accepted for publication 31 October 2022
Published 15 November 2022 Volume 2022:16 Pages 3763—3774
DOI https://doi.org/10.2147/OPTH.S386551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Phillip J Buckhurst,1 George Lau,2 Jon I Williams,2 Mark Packer3
1School of Health Professions, University of Plymouth, Plymouth, UK; 2Bausch and Lomb Surgical, Bausch and Lomb Bridgewater, New Jersey, NJ, USA; 3Mark Packer Consulting, Boulder, CO, USA
Correspondence: Phillip J Buckhurst, School of Health Professions, University of Plymouth, Plymouth, UK, Tel +44 1752 588884, Email [email protected]
Purpose: To assess the refractive outcomes, intraocular centration and rotational stability of the enVista toric intraocular lens (IOL).
Patients and Methods: This study was a prospective, multi-centre, double-masked, partially randomized and partially controlled clinical trial. A total of 191 participants were implanted with toric IOL (1.25, 2.00, or 2.75D) or non-toric IOL (control). The lowest range of corneal astigmatic eyes were randomized to 1.25D toric or control. Higher astigmatic powers were allocated to the treatment arm. Subjects were assessed immediately postoperatively, 1– 2 (V1), 7– 14 (V2), 30– 60 (V3) and 120– 180 (V4) days postoperatively. Unaided (UDVA) and distance corrected visual acuity (CDVA), manifest refraction and corneal curvature were assessed. Vector analysis was used to calculate surgically induced refractive correction (SIRC), correction ratio (CR), error magnitude (EM) and error vector (EV). Slit-lamp photography was used to measure centration and rotational stability.
Results: UDVA was better in the low toric IOL group in comparison with the control group at V4 (p< 0.001). There was an undercorrection in the control group, whereas the average CR for all toric subjects was 1.00 ± 0.32: V2, 0.98 ± 0.34: V3 and 0.98 ± 0.35: V4. The absolute IOL rotational stability in comparison to the position of the IOL at V1 was 1.35° ± 0.97°: V2, 1.35° ± 1.07°: V3 and 1.38° ± 1.25°: V4. Decentration was generally inferior (V1: 0.04 ± 0.22mm, V2: 0.05± 0.20mm, V3: 0.08 ± 0.22mm, V4: 0.04 ± 0.21mm) and nasal (V1: 0.19 ± 0.23mm, V2: 0.20 ± 0.20mm, V3: 0.20 ± 0.21mm, V4: 0.17 ± 0.22mm).
Conclusion: Participants with low levels of corneal astigmatism achieved superior vision and refractive outcomes in the low toric group over the control. Moderate and high levels of astigmatism achieved excellent refractive outcomes. The toric IOL demonstrated high levels of both rotational and centrational stability.
Keywords: IOL, astigmatism, cataract, enVista, toric
Introduction
Corneal astigmatism greater than 1.50 diopters (D) is present in approximately 15 to 22% of patients presenting for cataract surgery.1–4 Unless corrected, this corneal astigmatism will translate to residual refractive astigmatism, which has a detrimental effect on levels of both objective vision and subjective quality of life even as low as 1.00 D of cylinder.5 Every diopter of refractive astigmatism reduces the chances of spectacle independence6 and increases the lifetime cost of refractive correction for an individual.7 Toric intraocular lenses are widely considered the most reliable method of correcting corneal astigmatism following cataract surgery as they are not dependent on the cornea healing in a predictable manner.8
The enVista One-Piece Hydrophobic Acrylic Toric IOL (MX60T IOL) incorporates a toric surface on the posterior optic. The MX60T IOL optic is based upon the parent spherical aberration neutral enVista monofocal (MX60) IOL. The safety analysis from this pivotal trial has previously been published.9 This paper describes the efficacy of outcome measures acquired during this trial focusing on the refractive outcomes as well as the intraocular rotational stability and centration of the IOL.
Materials and Methods
Study Design
This study was a prospective, multicenter, partially controlled, double-masked, parallel group, partially randomized clinical trial. The study protocol adhered to the Declaration of Helsinki and ethical approval was obtained by a central Institutional Review Board (The IRB Company, Buena Park, CA, USA) prior to commencement of the trial. The study was registered with clinicaltrials.gov (NCT01852084), and written consent was obtained from all subjects.
Subjects
Potential participants were recruited from nine sites within the United States (US) on a consecutive basis according to the study inclusion/exclusion criteria, which can be found in detail in a previous publication.9 In summary, participants needed to be over 18 years of age with clinically significant cataract and with a predicted postoperative corneal astigmatism between 0.90 D and 2.4 D.
A single eye was designated by the Investigator as the study eye for the purposes of the study. In cases of bilateral cataracts, the eye with the worst best-corrected distance visual acuity (BCDVA) was selected as the study eye. Where BCDVA was equal, the right eye was assigned as the study eye.
Eyes within the lowest cylinder correction range were randomly assigned to be implanted with either the study toric IOL (1.25 D) or with the spherical MX60 control lens in a 1:1 ratio (approximately 80 eyes/treatment group). Randomization occurred during the operative visit after all toric lens calculations had been conducted, and phacoemulsification had been completed. Subjects within the ranges of the higher toric powers were not randomized and were assigned higher power toric lenses (2.00 D or 2.75D).
Enrolled subjects attended 6 study visits: Preoperative Visit (Pre-OP: Day −90 to −2), Operative Visit (OP: Day 0), visit 1 (V1: Postoperative Day 1–2), visit 2 (V2: Postoperative Day 7–14), visit 3 (V3: Postoperative Day 30–60), and visit 4 (V4: Postoperative Day 120–180).
Masking
All postoperative study outcome measures at each site relating to visual acuity and manifest refraction were collected by a study investigator who was masked to the allocation of a subject to a specific study group. Subjects in the low astigmatic groups (MX60T 1.25 D IOL or MX60 parent monofocal IOL) were also masked to their grouping allocation and were only informed of the type of lens implanted once they had completed the study.
Study Lenses
The Bausch & Lomb enVista One-Piece Hydrophobic Acrylic Toric IOL (Model MX60T) is a toric version of the enVista MX60 One-Piece Hydrophobic Acrylic control IOL with cylinder axis marks on the posterior surface of the lens. Test and control lenses were available in spherical equivalent powers +16.0 to +27.0 D, with toric cylinder powers for test lenses of 1.25 D, 2.00 D, and 2.75 D.
Presurgical and Surgical Technique
The enVista Toric Calculator (Bausch & Lomb) was used to calculate the predicted postoperative corneal astigmatism and the recommended toric IOL cylinder power and axis, using preoperative keratometry and the personalized surgically induced astigmatism (SIA) determined for each investigator. All surgeries were performed using standard small-incision phacoemulsification with the primary incision constructed on the steep keratometric axis determined by the IOL Master (Carl Zeiss Meditec, Dublin, CA).
The enVista toric IOLs are marked with two lines at the edge of the optic of the lens. It was required to align the lens with the predicted postoperative steep axis of the cornea as indicated by the Bausch & Lomb Toric Calculator. Superficial reference markings for axis placement were made on the cornea using a needle or Sinskey hook, not penetrating the anterior limiting laminar (Bowman’s) membrane.
Outcome Measures
Snapshots from the surgical video were used to identify the location of the toric axis markings and the location of the intended axis (as determined by the corneal reference markings). At each subsequent visit subjects’ pupils were dilated (1% tropicamide and 2.5% phenylephrine) and retro-illuminated images were acquired for the assessment of rotational stability and the determination of IOL decentration. The centre of the cornea was used as the reference location for the centre of the IOL. Image analysis of the retro-illuminated images was conducted using the methodology described by Wolffsohn and Buckhurst.10
All assessments of visual acuity were conducted at 4 m using a standard Early Treatment Diabetic Retinopathy Study (ETDRS) chart at an illumination of approximately 85 cd/m2. Uncorrected distance visual acuity (UCDVA) was assessed at all visits, and manifest subjective refraction was determined at V2-V4 following which BCDVA was measured.
Statistical Analysis
Astigmatic corneal and refractive power was broken down into two vector components (J0 and J45) and was also expressed as double angle polar plots. Polar plots incorporated the vector means calculated using J0 and J45 along with ellipsoids representing the standard deviation in the J0 and J45 directions. These data were then used to quantify the target-induced astigmatism (TIA), surgical-induced astigmatism (SIA) and the correction ratio (CR):11 TIA was the vector difference between the preoperative corneal astigmatism and the target postoperative refractive astigmatism. SIA was defined as the difference between the preoperative corneal astigmatism (in vector form) and the postoperative refractive astigmatism. CR is calculated as SIA/IRC and represents the ratio of the achieved magnitude of correction relative to the intended correction. A ratio of 1 is desired with undercorrection expressed as a result smaller than 1 and overcorrection expressed as greater than 1. Comparison of means testing was conducted between the control group and the 1.25 D toric group using Student’s t-test or a two-way repeated measures ANOVA given that these two groups were randomized. Descriptive data for all group (including the 2.00 D, and 2.75 D toric groups) were expressed as mean ± standard deviation.
Results
Patient Demographics
A total of 191 subjects aged 70.1 ± 8.7 years were enrolled in this study (47% male). There were 159 of these subjects who were randomized to the low toric IOL group or the monofocal IOL control group: 79 subjects in the control IOL arm and 80 subjects in the low toric IOL group. A further 20 subjects were non-randomly implanted with the 2.00 D toric IOL and 12 subjects with the 2.75 D toric IOL. The demographics and magnitude of preoperative refractive corneal cylinder were similar between the control and low toric groups.
Refraction
The magnitude of preoperative corneal keratometric cylinder was similar for the control (1.57 D ± 0.16 D) and the low toric (1.55 D ± 0.17 D) IOL groups (P = 0.467). The mean magnitude was 1.99 D ± 0.14 D for the 2.00 D toric IOL group and 2.59 D ± 0.18 D for the 2.75 D toric IOL group (Figure 1).
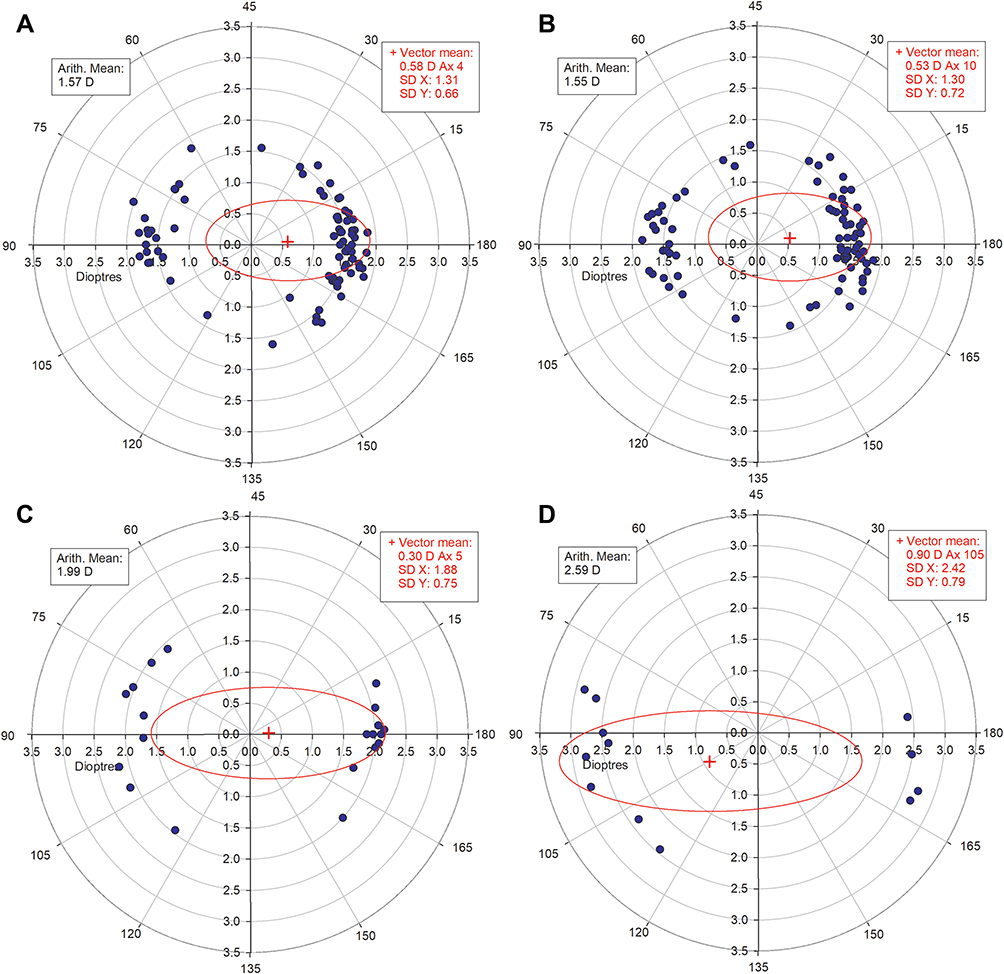 |
Figure 1 Preoperative corneal astigmatism: (A) control group, (B) 1.25 D toric group, (C) 2.00D toric group, (D) 2.75 toric group. The vector means are plotted as a red cross (in double-angle vector space) and the standard deviations in the X and Y directions are used to produce the red ellipsoids for each image and are displayed for each image in an embedded image box. |
The mean target spherical equivalent (‒0.11 D ± 0.14 D) was similar to the achieved spherical equivalent at V2 (‒0.05 ± 0.43 D; P = 0.065) and V3 (‒0.05 ± 0.43 D; P = 0.058). At V4 (0.03 D ± 0.42 D), a statistically significant difference between means was found (P < 0.01) but this was not clinically significant. There were 99%, 83% and 55% of eyes by V4 that had spherical equivalent within ±1.00 D, ±0.50 D and ±0.25 D of emmetropia, respectively (Figure 2).
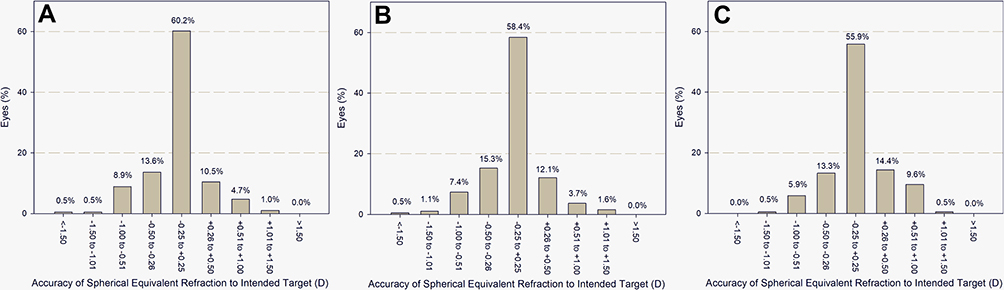 |
Figure 2 Mean spherical equivalent as determined by manifest refraction at (A) V1, (B) V2, (C) V3. |
Preoperative BCDVA was similar (P = 0.509) between the control IOL arm (0.48 ± 0.23 LogMAR) and 1.25 D toric IOL group (0.50 ± 0.19 LogMAR). Following implantation, there was a significant difference between the two groups, with better UCDVA found in the 1.25 D toric group. BCDVA was statistically similar at all postoperative visits between all toric IOL treatment groups and the control IOL group (Table 1).
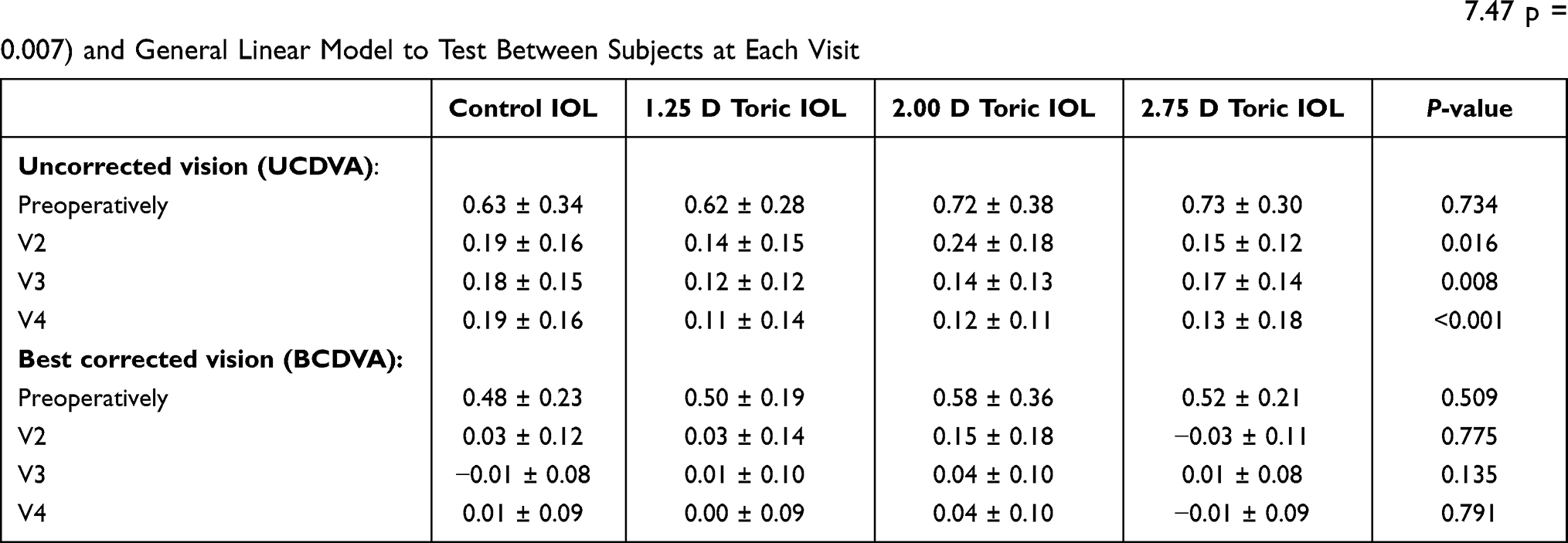 |
Table 1 Pre- and Post-Operative Visual Acuities (UCDVA and BCDVA) Data are Mean ± Standard Deviation. Preoperative Significance Was Tested Between the Control and 1.25 Toric Lenses Using a Two-Way Repeated Measures ANOVA (F2,37.47 p = 0.007) and General Linear Model to Test Between Subjects at Each Visit |
The absolute magnitude of postoperative refractive astigmatism was significantly lower in the 1.25 D toric arm in comparison with the control arm (p < 0.001). The absolute residual astigmatic magnitude at visit 4 for the control group was less than or equal to 0.50 D of cylinder in 29% of cases, less than or equal to 1.00 D in 54% of cases and less than or equal to 1.50 D in 77% of cases. For the combined results from all toric IOL subjects, 52% had less than or equal to 0.50 D of cylinder, 85% had less than or equal to 1.00 D, and 97% had less than or equal to 1.50 D. The magnitude of target astigmatic correction (TIA) was similar in the monofocal IOL control group (1.34 D ± 0.11 D) and 1.25 D toric IOL group (1.34 D ± 0.06 D). The TIA can be visualized in Figure 3 as a relatively uniform band circling the polar plots around the 1.34 D magnitude. As expected, the surgically induced refractive correction (SIRC) was significantly lower than the desired TIA at all visits within the monofocal non-toric control IOL group (p < 0.001) (Figure 3A–C), while the magnitude of SIRC and TIA were similar in the 1.25 D toric group (V2, p = 0.496; V3, p = 0.310; V4, p = 0.329) (Figure 3D–F). The ellipsoid surrounding the SIRC values demonstrates the difference in correction between the toric and control groups with the toric groups demonstrating progressively greater astigmatic correction and hence wider ellipsoid values. This is further elucidated by examining the location of SIRC data points within the plots: the 1.25 D, 2.00 D and 2.75 D SIRC plots conform to the locations of the TIA whilst the control group’s SIRC data points lie more central.
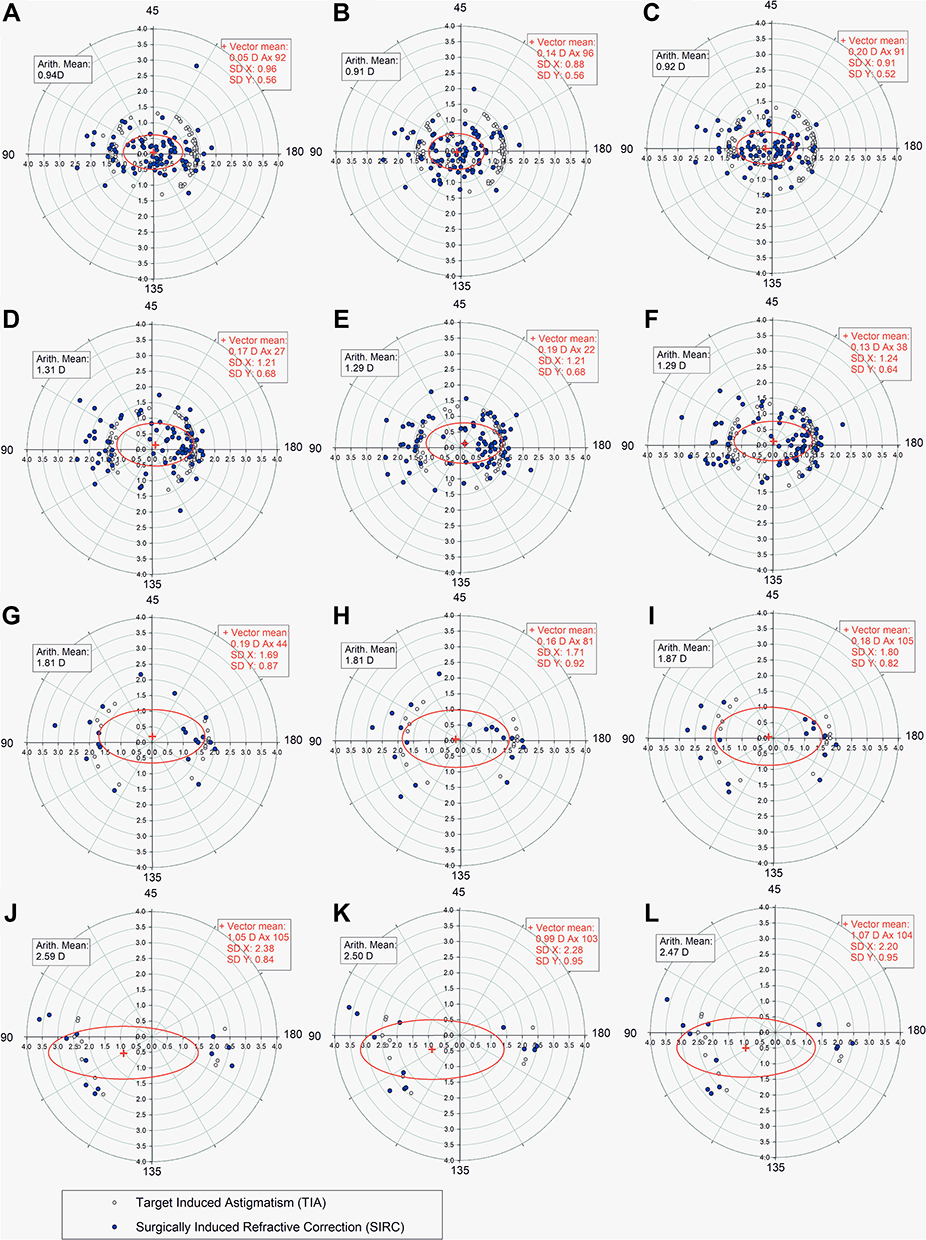 |
Figure 3 Target Induced Astigmatism (TIA) and Surgically Induced Refractive Astigmatism for (A) Spherical control group V2, (B) Spherical control group V3, (C) Spherical control group V4, (D) 1.25 D toric group V2, (E) 1.25 D toric group V3, (F) 1.25 D toric group V4, (G) 2.00 D toric group V2, (H) 2.00 D toric group V3, (I) 2.00 D toric group V4, (J) 2.75 D toric group V2, (K) 2.75 D toric group V3, (L) 2.75 D toric group V4. The vector means are plotted as a red cross (in double-angle vector space) and the standard deviations in the X and Y directions are used to produce the red ellipsoids for each image and are displayed for each image in the embedded image box. |
The results of calculating the mean correction ratio (SIA/TIA) for each treatment group highlight an undercorrection for all visits when examining the control arm (V2, 0.70 ± 0.44; V3, 0.69 ± 0.41; V4, 0.69 ± 0.40). The average correction ratio for all toric IOL subjects by contrast was very close to unity at all study visits (V2, 1.00 ± 0.32; V3, 0.98 ± 0.34; V4, 0.98 ± 0.35) (Figure 4).
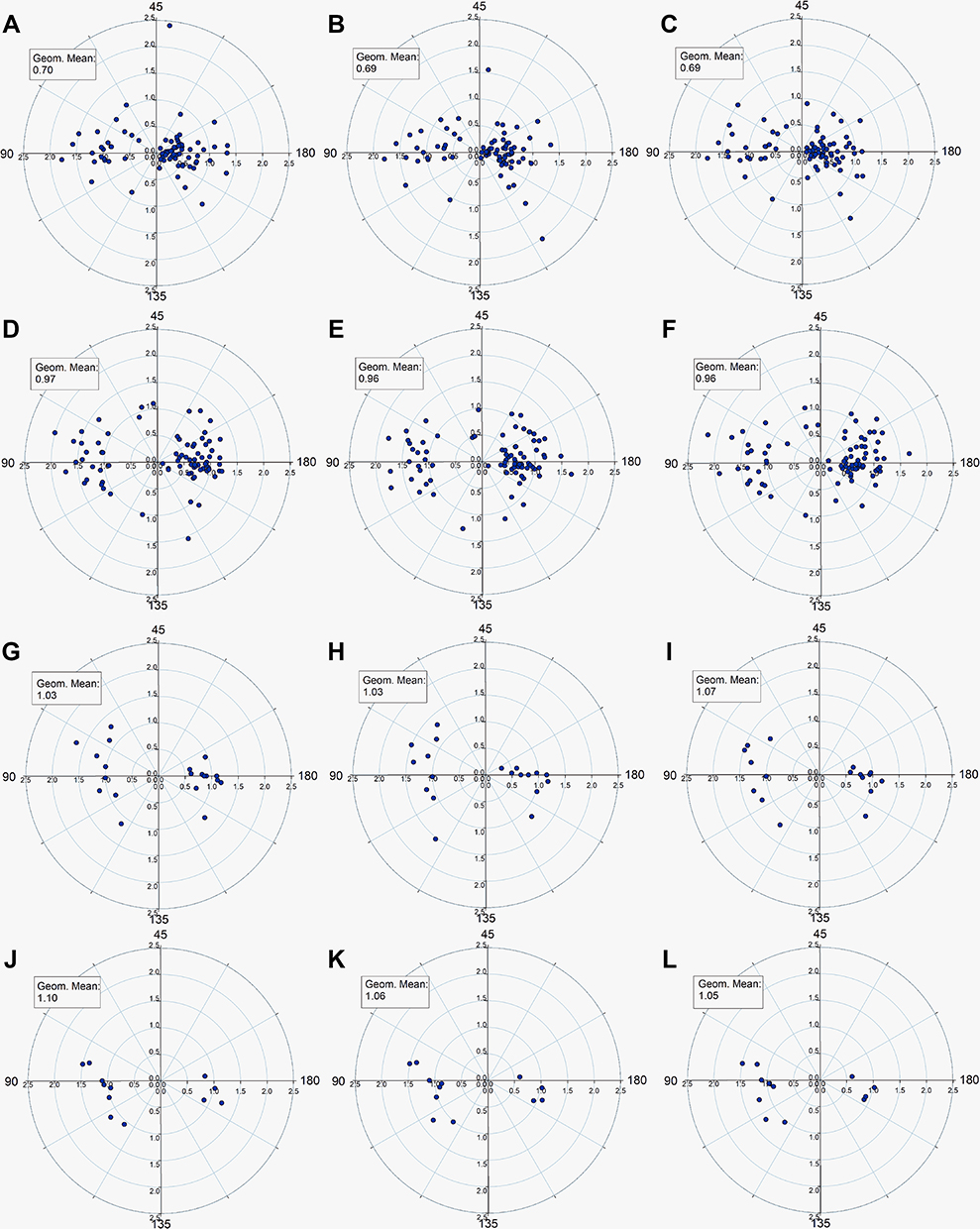 |
Figure 4 Correction ratio: (A) Spherical control group V2, (B) Spherical control group V3, (C) Spherical control group V4, (D) 1.25 D toric group V2, (E) 1.25 D toric group V3, (F) 1.25 D toric group V4, (G) 2.00 D toric group V2, (H) 2.00 D toric group V3, (I) 2.00 D toric group V4, (J) 2.75 D toric group V2, (K) 2.75 D toric group V3, (L) 2.75 D toric group V4. |
The toric IOL subjects were then categorized as with-the-rule (within 20 degrees of vertical; 36 eyes), against-the-rule (within 20 degrees of horizontal; 62 eyes) or oblique (14 eyes). The correction ratios were significantly different for the different subpopulations at all visits (with-the-rule 1.28 ± 0.29; against-the-rule 0.82 ± 0.29; oblique 1.07 ± 0.25). Analysis of these differences with a one-way ANOVA yields statistically significant variance F-statistics among these three subpopulations at all study visits (V2 F4.102, p < 0.001; V3 F4.122, p < 0.001; V4 F4.842, p < 0.001) and analysis with the Tukey post-hoc pairwise statistical test reveals a higher correction ratio of the with-the-rule eyes in comparison with both the against-the-rule (p < 0.001) and the oblique eyes (p < 0.001).
Rotational Stability
Absolute rotational stability in comparison to the position of the 1.25 D toric IOL at V1 was (mean value [± SD]) 1.34° (±0.98°) at V2, 1.31° (±1.03°) at V3 and 1.41° (±1.27°) at V4. Mean rotational stability was determined from multiple images for each study eye relative to the corneal markings and was less than or equal to 5° at each visit in comparison with the position at V1 (Figure 5).
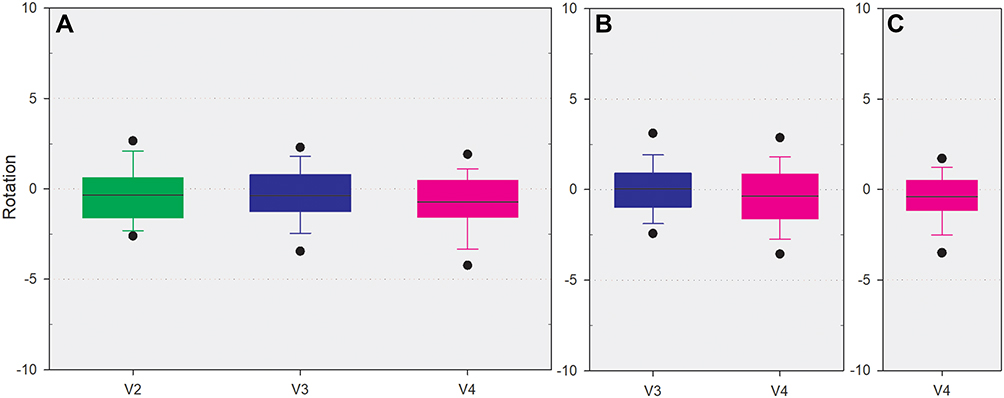 |
Figure 5 Rotational stability, Circular symbols represent the 5/95 percentile. (A) Rotation relative to the V1 position, (B) Rotation relative to the V2 position, (C) Rotation relative to the V3 position. |
Misalignment was defined as the position of the toric IOL at each visit when compared with markings made on the cornea prior to the start of surgery. Mean absolute misalignment was 4.68° ± 7.30° at V4, with 93% of lenses within 10 degrees of the corneal markings. All lenses that were misaligned by more than 10 degrees at V4, including two subjects with 1.25 D toric IOLs that had more than 30° lens axis misalignment, remained in position and did not rotate following the V1 visit. UCDVA at Visit 4 was 20/25 and 20/40 for the two subjects with the worst misalignment and neither subject required secondary IOL repositioning.
Centration
Mean decentration for all toric IOLs was generally inferior (V1: 0.04 ± 0.22 mm, V2: 0.05 ± 0.20 mm, V3: 0.08 ± 0.22 mm, V4: 0.04 ± 0.21 mm) and nasal (V1: 0.19 ± 0.23mm, V2: 0.20 ± 0.20 mm, V3: 0.20 ± 0.21 mm, V4: 0.17 ± 0.22 mm) relative to the limbal centre (Figure 6). The mean total absolute vectorial decentration was 0.33 ± 0.16 mm at V1, 0.32 ± 0.14 mm at V2, 0.32 ± 0.17 mm at V3 and 0.29 ± 0.17 mm at V4.
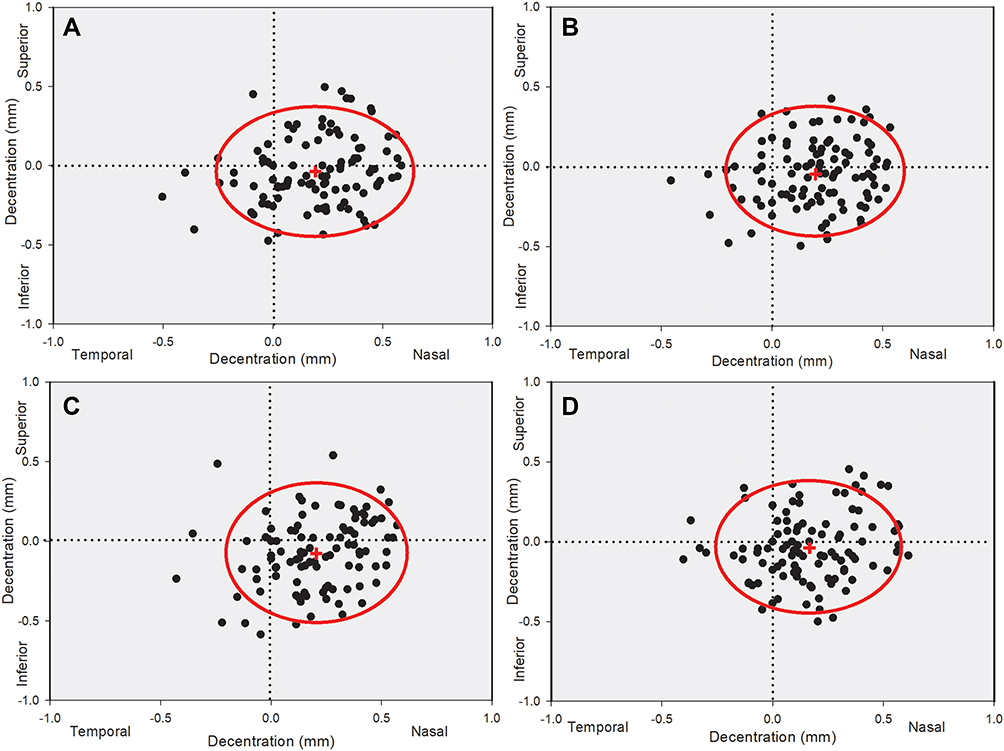 |
Figure 6 Scattergram showing decentration of the centre of IOL relative to the limbal centre with horizontal decentration represented on the x and vertical on the y axis. The red cross is an expression of the mean vertical and horizontal location with the ellipsoid representing the 95% confidence interval in these directions and hence enveloping the greatest proportion of eyes. (A) V1, (B) V2, (C) V3, (D) V4. |
Discussion
The purpose of toric IOL implantation is to minimize postoperative residual astigmatism and provide optimum uncorrected distance visual acuity. Ultimately, patients seeking correction of astigmatism are seeking to reduce their spectacle dependence. As expected, the best corrected visual acuity was similar between the randomized toric and control group whilst uncorrected visual acuity was significantly better in the toric group at all visits. This is illustrated by the fact that 45% of subjects achieved 20/20 or better UCDVA in the 1.25 D toric IOL group whilst only 16.7% of subjects in the control group achieved this level of UCDVA improvement. The low astigmatic group was randomized to receive either a toric or a spherical control IOL. In all subjects, an “on-axis” incision was used to ensure some level of astigmatic reduction would be achieved in the control group and to increase treatment standardization between subjects. This created a relatively unique homogeneity of preoperative corneal astigmatism, as evidenced by a relatively narrow preoperative distribution of astigmatism in subjects within the lower astigmatic range (1.55 D ± 0.17 D for 1.25 D toric IOL subjects and 1.57 D ± 0.16 D for control IOL subjects). Despite the similar preoperative corneal profiles, the low toric group achieved superior refractive outcomes based on the mean correction ratio values (0.61, control IOLs; 0.94, 1.25 D toric IOLs, P < 0.001).
This study was designed and initiated prior to the general acceptance that the influence of the posterior corneal surface results in an overcorrection of with-the-rule and undercorrection of against-the-rule astigmatism as first highlighted by Koch and associates.12 Careful examination of the correction ratio polar plots supports the conclusions of Pantanelli et al13 who demonstrated that the EVO toric calculator, which combines theoretical posterior corneal astigmatism with thick lens modelling, performs better than the enVista legacy calculator used in the present study.
There are three main intraocular mechanisms that may result in the rotation of an IOL. The first is a lack of adequate friction between the IOL and capsular bag during the initial early period post-implantation. The relative sizes and shapes of the IOL haptics and capsule as well as the presence of residual ophthalmic viscoelastic device (OVD) influence this first mechanism. Plate haptic IOLs have been linked to a greater rotation in the early postoperative period given their reduced overall diameter.14 Simply increasing the size of a plate haptic is not a solution as this can cause distortion of the capsular bag and zonules15 and a reliable relationship between the capsular bag and ocular biometry has not been established.16 Kent et al17 demonstrated, in animal eyes, that the addition of mini polyimide haptics to a plate haptic significantly improved capsular bag fixation. These findings were supported by a large in-vivo study involving a presbyopia correcting IOL with mini polyimide haptics (Trulign toric) which exhibited high levels of rotational stability.18 Material properties of the IOL are a major source of influence on the friction between the IOL and capsular bag, with poly(methyl methacrylate) IOLs providing the greatest haptic adhesion, followed by foldable acrylic, with silicone having the least.19 The presence of OVD may also reduce friction, and it has been proposed that the type of OVD used may influence the amount of rotation.20
A second contributing factor is ocular trauma and anterior chamber instability related to postoperative intraocular pressure (IOP) changes. Hypotony can occur even with uneventful cataract surgery,21 and this causes destabilization of the anterior chamber and can result in a higher risk for rotation.22 Postoperative trauma can also cause IOL rotation if the force on the eye is sufficient to cause significant wound leakage.22 Haptic fenestration holes can anchor an IOL in place, allowing capsule fibrosis and proliferation of lens cortical material to migrate through the holes. Larger fenestration holes can be expected to lead to greater migration of native lens material, thereby increasing long-term IOL stability and resisting the effects of traumatic forces. The enVista toric IOL incorporates two fenestration holes, which are present at the haptic-optic junction on either side of the IOL. It is important to note that this fibrosis takes approximately two weeks post implantation23 and so if a toric IOL is misaligned, it should be repositioned before this fibrosis occurs.24
A third possible mechanism for IOL stabilization occurs in the late post-surgical stage and is caused by compression of the IOL haptics due to capsular bag shrinkage. When compressed, a plate haptic IOL has no preference in the direction of rotation and demonstrates good stability.25 However, in-vitro studies15,26 have demonstrated that early open-loop haptic IOL designs rotate clockwise under capsule contraction (assuming the haptics are directed counterclockwise). If insufficient friction is present, the haptics slip, causing counterclockwise rotation.27 The present study with enVista toric IOLs demonstrated excellent late stage rotational stability (stability two weeks post implantation), and rotational stability may be attributable to the higher rigidity of the enVista IOL when compared to other hydrophobic acrylic materials. Bozukova et al demonstrated through in-vitro bench testing that the enVista IOL provided a high level of resistance to compressive forces.28 It is also likely that the design and size of the enVista IOL fenestration holes provide a cushioning and countervailing effect on compression forces.
Assessment of IOL decentration can be accomplished through a variety of methods10,29–31 and poses some challenges. Decentration describes the difference between the center of an IOL and another reference point. The center of the pupil, center of limbus, and predicted line of vision have all been used as reference points for centration. Despite the reference for centration differing among the pupil and corneal center or visual axis, centration results in this study based on the limbal center compare well to expected results and show low levels of decentration at last study visits. These levels of decentration are not significant enough to result in unwanted higher-order aberrations.32
One of the main limitations of this study is the use of slit-lamp images for the assessment of decentration. Unlike phakometry, this method uses the centre of the cornea as a reference point rather than the visual axis. This may explain the tendency for the IOL to locate nasally. The use of phakometry would allow a more detailed assessment of the alignment of the IOL including tilt, but it was not feasible to implement phakometry in a large multisite clinical trial given the bespoke nature of the devices that have been developed. The study also adopted an agnostic approach to the selection of OVD, and this is a limitation of the study given that it has been suggested that the choice of OVD can influence stability.8
Conclusion
In conclusion, the enVista Toric IOL reduces the effects of preoperative corneal astigmatism on postoperative refraction following cataract surgery, demonstrating excellent rotational stability, minimizing post-surgical decentration and providing improved distance vision.
Data Sharing Statement
No further data beyond those provided will be shared.
Acknowledgments
Investigative support from the enVista Toric Clinical Study Group (Chad L. Betts, MD, Fayetteville, AK; Keith Charles, MD, Mount Dora, FL; Gary Foster, MD, Fort Collins, CO; Luther L. Fry, MD, Garden City, KS; Joseph Gira, MD, St Louis, MO; James A. Katz, MD, Des Plaines, IL; Kevin Lavery, MD, Jackson, MI; John Millin, MD, Louisville, KY; Farrell C. Tyson, MD, Cape Coral, FL; Robert Weinstock, MD, Largo, FL).
Funding
The study was sponsored by Bausch and Lomb.
Disclosure
Dr. Buckhurst reports grants from Bausch and Lomb during the conduct of the study; grants from Medicontur Medical Engineering and Zeiss outside the submitted work. Dr. Packer is a consultant to Advanced Vision Science, Inc. (Santen), Alcon Research Institute, Beaver Visitec International, PhysIOL, Bausch Health Co., Inc., Keranova S.A., LENSAR, Inc., Olympic Ophthalmics, Inc., Promedica International Corp., Precision for Medicine, Inc., Rayner Intraocular Lenses, Ltd., SOLX, Inc., and University of Colorado; as a consultant to and investor in Cassini Technologies B.V., ClearSight LLC, International BioMedical Devices, Inc., Ira, Inc., Refocus Group, Inc., LensGen, STAAR Surgical Co., Tarsus Pharmaceuticals, Inc., and Visant Medical, Inc.; and as an investor in Aerie Pharmaceuticals, Iantech, Inc., STAAR Surgical Co., Transcend Medical, Inc., TrueVision Systems, Inc., and WaveTec Vision Systems, Inc. Dr Lau and Dr Williams are employees of Bausch and Lomb. The authors report no other conflicts of interest in this work.
References
1. Ferrer-Blasco T, Montes-Mico R, Peixoto-de-Matos SC, Gonzalez-Meijome JM, Cervino A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70–75. doi:10.1016/j.jcrs.2008.09.027
2. Day AC, Dhariwal M, Keith MS, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103(7):993–1000. doi:10.1136/bjophthalmol-2018-312025
3. Hoffer KJ. Biometry of 7500 cataractous eyes. Am J Ophthalmol. 1980;90(3):360–368. doi:10.1016/S0002-9394(14)74917-7
4. Ninn-Pedersen K, Stenevi U, Ehinger B. Cataract patients in a defined Swedish population 1986–1990. II. Preoperative observations. Acta Ophthalmol. 1994;72(1):10–15. doi:10.1111/j.1755-3768.1994.tb02729.x
5. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37(3):454–460. doi:10.1016/j.jcrs.2010.09.022
6. Wilkins MR, Allan B, Rubin G; Moorfields IOLSG. Spectacle use after routine cataract surgery. Br J Ophthalmol. 2009;93(10):1307–1312. doi:10.1136/bjo.2008.151829
7. Pineda R, Denevich S, Lee WC, Waycaster C, Pashos CL. Economic evaluation of toric intraocular lens: a short- and long-term decision analytic model. Arch Ophthalmol. 2010;128(7):834–840. doi:10.1001/archophthalmol.2010.127
8. Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA. Surgical correction of astigmatism during cataract surgery. Clin Exp Optom. 2010;93(6):409–418. doi:10.1111/j.1444-0938.2010.00515.x
9. Packer M, Williams JI, Feinerman G, Hope RS. Prospective multicenter clinical trial to evaluate the safety and effectiveness of a new glistening-free one-piece acrylic toric intraocular lens. Clin Ophthalmol. 2018;12:1031–1039. doi:10.2147/OPTH.S167726
10. Wolffsohn JS, Buckhurst PJ. Objective analysis of toric intraocular lens rotation and centration. J Cataract Refract Surg. 2010;36(5):778–782. doi:10.1016/j.jcrs.2009.12.027
11. Eydelman MB, Drum B, Holladay J, et al. Standardized analyses of correction of astigmatism by laser systems that reshape the cornea. J Refract Surg. 2006;22(1):81–95. doi:10.3928/1081-597X-20060101-16
12. Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803–1809. doi:10.1016/j.jcrs.2013.06.027
13. Pantanelli SM, Kansara N, Smits G. Predictability of residual postoperative astigmatism after implantation of a toric intraocular lens using two different calculators. Clin Ophthalmol. 2020;14:3627–3634. doi:10.2147/OPTH.S276285
14. Patel CK, Ormonde S, Rosen PH, Bron AJ. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 1999;106(11):2190–2195; discussion 2196. doi:10.1016/S0161-6420(99)90504-3
15. Lim SJ, Kang SJ, Kim HB, Apple DJ. Ideal size of an intraocular lens for capsular bag fixation. J Cataract Refract Surg. 1998;24(3):397–402. doi:10.1016/S0886-3350(98)80330-1
16. Khng C, Osher RH. Evaluation of the relationship between corneal diameter and lens diameter. J Cataract Refract Surg. 2008;34(3):475–479. doi:10.1016/j.jcrs.2007.10.043
17. Kent DG, Peng Q, Isaacs RT, Whiteside SB, Barker DL, Apple DJ. Mini-haptics to improve capsular fixation of plate-haptic silicone intraocular lenses. J Cataract Refract Surg. 1998;24(5):666–671. doi:10.1016/S0886-3350(98)80263-0
18. Pepose JS, Hayashida J, Hovanesian J, et al. Safety and effectiveness of a new toric presbyopia-correcting posterior chamber silicone intraocular lens. J Cataract Refract Surg. 2015;41(2):295–305. doi:10.1016/j.jcrs.2014.05.043
19. Oshika T, Nagata T, Ishii Y. Adhesion of lens capsule to intraocular lenses of polymethylmethacrylate, silicone, and acrylic foldable materials: an experimental study. Br J Ophthalmol. 1998;82(5):549–553. doi:10.1136/bjo.82.5.549
20. Chang DF. Early rotational stability of the longer Staar toric intraocular lens: fifty consecutive cases. J Cataract Refract Surg. 2003;29(5):935–940. doi:10.1016/S0886-3350(02)01843-6
21. Shingleton BJ, Rosenberg RB, Teixeira R, O’Donoghue MW. Evaluation of intraocular pressure in the immediate postoperative period after phacoemulsification. J Cataract Refract Surg. 2007;33(11):1953–1957. doi:10.1016/j.jcrs.2007.06.039
22. Pereira FA, Milverton EJ, Coroneo MT. Miyake-Apple study of the rotational stability of the Acrysof Toric intraocular lens after experimental eye trauma. Eye. 2010;24(2):376–378. doi:10.1038/eye.2009.150
23. Mamalis N, Omar O, Veiga J, Tanner D, Pirayesh A, Fernquist DS. Comparison of two plate-haptic intraocular lenses in a rabbit model. J Cataract Refract Surg. 1996;22(Suppl 2):1291–1295. doi:10.1016/S0886-3350(96)80087-3
24. Chang DF. Repositioning technique and rate for toric intraocular lenses. J Cataract Refract Surg. 2009;35(7):1315–1316. doi:10.1016/j.jcrs.2009.02.035
25. Jampaulo M, Olson MD, Miller KM. Long-term Staar toric intraocular lens rotational stability. Am J Ophthalmol. 2008;146(4):550–553. doi:10.1016/j.ajo.2008.05.040
26. Werblin TP. Do three-piece PMMA IOLs rotate after implantation in the capsular bag? J Refract Surg. 1995;11(6):468–471. doi:10.3928/1081-597X-19951101-13
27. Parssinen O, Raty J, Vainikainen J, Timonen J, Lyyra AL. Compression forces of haptics of freely rotating posterior chamber intraocular lenses. J Cataract Refract Surg. 1998;24(3):415–425. doi:10.1016/S0886-3350(98)80334-9
28. Bozukova D, Pagnoulle C, Jerome C. Biomechanical and optical properties of 2 new hydrophobic platforms for intraocular lenses. J Cataract Refract Surg. 2013;39(9):1404–1414. doi:10.1016/j.jcrs.2013.01.050
29. Guyton DL, Uozato H, Wisnicki HJ. Rapid determination of intraocular lens tilt and decentration through the undilated pupil. Ophthalmology. 1990;97(10):1259–1264. doi:10.1016/S0161-6420(90)32422-3
30. Rosales P, Marcos S. Phakometry and lens tilt and decentration using a custom-developed Purkinje imaging apparatus: validation and measurements. J Opt Soc Am a Opt Image Sci Vis. 2006;23(3):509–520. doi:10.1364/JOSAA.23.000509
31. Wang X, Dong J, Wang X, Wu Q, Li T. IOL tilt and decentration estimation from 3 dimensional reconstruction of OCT image. PLoS One. 2013;8(3):e59109. doi:10.1371/journal.pone.0059109
32. Baumeister M, Buhren J, Kohnen T. Tilt and decentration of spherical and aspheric intraocular lenses: effect on higher-order aberrations. J Cataract Refract Surg. 2009;35(6):1006–1012. doi:10.1016/j.jcrs.2009.01.023
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.