")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Efficacy and toxicity of cladribine for the treatment of refractory acute myeloid leukemia: a meta-analysis
Authors Zhou A, Han Q, Song H, Zi J, Ma J, Ge Z
Received 3 March 2019
Accepted for publication 26 April 2019
Published 29 May 2019 Volume 2019:13 Pages 1867—1878
DOI https://doi.org/10.2147/DDDT.S207425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Anqi Zhou, Qi Han, Huihui Song, Jie Zi, Jinlong Ma, Zheng Ge
Department of Hematology, Zhongda Hospital Southeast University, Institute of Hematology Southeast University, Nanjing 210009, People’s Republic of China
Purpose: To investigate the overall efficacy and toxicity of cladribine and cladribine-based chemotherapy in the treatment of patients with refractory acute myeloid leukemia (AML) based on meta-analysis.
Methods: PubMed, EMBASE database, and the Cochrane Library were searched for relevant studies. Eligible studies were clinical trials of refractory AML assigned to cladribine with data on efficacy including complete remission (CR) rate, overall response rate (ORR) and overall survival. Toxicity was evaluated based on the early death rate and the incidence of grade 3 and 4 adverse events (AEs).
Results: A total of 10 clinical trials including 422 refractory AML patients were analyzed. The overall CR rate was 42.2% (95% CI: 31.0–54.3%). And the ORR of seven trials including 235 patients was 49.7% (95% CI: 33.5–66.0%). The overall early death rate of 260 patients enrolled in five trials was 6.8% (95% CI: 4.3–10.6%). Thrombocytopenia, anemia, neutropenia, and infection were the most common grade 3 and 4 AEs.
Conclusion: Cladribine is effective for refractory AML, and its efficacy can be increased with the combination of cladribine, cytarabine, and granulocyte-colony stimulating factor regimen.
Keywords: cladribine, acute myeloid leukemia, refractory AML, meta-analysis
Introduction
Although significant progress has been made for the treatment of acute myeloid leukemia (AML) in the last decade, 10–40% of newly diagnosed patients with AML are not able to achieve complete remission (CR) with standard or intensive induction therapy, and among those who have achieved first CR (CR1) 50–70% of patients tend to relapse. Primary refractory or resistant AML can hardly be cured by conventional salvage therapy, therefore novel therapies acting as bridges to hematopoietic stem cell transplantation are urgently needed.1–3
Cladribine is an adenosine deaminase resistant analog of adenosine which has proved to be a relatively novel cytotoxic agent.4 Several in vitro pharmacological studies have demonstrated the anti-leukemia activity of cladribine. These data in vitro have shown that AML samples especially AML FAB M5 were more sensitive to cladribine. Therefore as a therapy for refractory or drug-resistance AML, cladribine is proved to be valid either as alternatives to Ara-c or in combination therapy.5,6 As a purine nucleoside analog, cladribine has the ability to inhibit DNA synthesis, DNA repair and induce apoptosis in the end, acting cytotoxically either in the mitotic or quiescent cell cycle phase.7,8
As a single drug, cladribine has antileukemic activity in patients with AML.9–11 It is also suggested that cladribine (CdA), cytarabine (Ara-C), and granulocyte-colony stimulating factor (G-CSF) (CLAG) regimen may also improve the prognosis of refractory AML.12–14 In addition, adding mitoxantrone (MIT) to the CLAG regimen may create synergies in the activity of antileukemic.15,16
In recent years, the efficacy of cladribine monotherapy or cladribine-based combination regimens for the treatment of refractory AML has been demonstrated through multiple prospective studies, despite its hematologic toxicity with severe neutropenia and thrombocytopenia.17
Materials and methods
We performed a systematic review of data from nine published studies with the methods described in the Cochrane Handbook for Systematic Reviews of Interventions.18
Literature search strategy
The online databases PubMed, EMBASE, and Cochrane Library were searched from their inception until October 2018 for potentially eligible studies. A combination of the following terms was employed in the search strategy: {(“acute myeloid leukemia” or “AML” or “acute myeloid leukemias” or “AMLs” or “acute myeloid leukaemia” or “Leukemia, Myeloid, Acute” [MeSH]) and [“cladribine” or “2-chlorodeoxyadenosine” or “CdA” or “2-CdA”] and [“refractory” or “resistant” or “resist”]}. We applied the wild-card term“*” during the literature search and evaluated the reference lists for additional eligible trials and reviews.
Study selection and endpoints
Eligible studies should have met the following criteria: 1) included patients with a diagnosis of primary refractory or drug-resistance AML, consistent with the WHO classification for AML; 2) were prospective studies with cladribine monotherapy or cladribine in combination with other chemotherapy drugs; 3) investigated the outcomes for patients treated with cladribine monotherapy or combination strategies.
The primary outcomes of these studies were CR rate and overall response rate (ORR). CR referred to bone marrow (BM) blast count <5% and normal peripheral blood cell count; partial response (PR) was defined as BM blasts with a percentage between 5% and 25%. ORR comprised both CR and PR. Secondary outcomes included overall survival (OS) and disease-free survival (DFS) for all evaluable patients. Hematologic and non-hematologic toxicity data were also analyzed where available.
Data extraction
Two investigators independently reviewed the original papers and extracted data from the eligible studies using a standardized data-extraction form. Data connecting with study characteristics (first author, number of patients and treatment protocols), patient characteristics (age, sex, and blasts in the BM), outcome measures (CR rate, ORR, the median time of OS and DFS and early death rate) were collected.
Quality assessment
A modified version of the Newcastle-Ottawa Scale for cohort studies was used to assess the quality of studies.19,20 The quality and risk of bias for all eligible papers in this systematic review were evaluated independently by two investigators. Publication bias was assessed by the visual assessment of funnel plots where the primary or secondary endpoint involving 10 or more studies.
Statistical analysis
Statistical analysis was performed with meta-analysis software “Comprehensive Meta-Analysis 2.0” (Biostat, Englewood, NJ, USA). The chi-squared test and I2 statistic were used to analyze the statistical heterogeneity across studies. This criterion was used to determine whether a fixed- or random-effects model should be employed to the following data analysis. Subgroup analysis for response rate was performed if the heterogeneity (I2>75%) was too great for a summary estimate. Estimated proportions with 95% CIs were calculated for all ratio outcomes. Subgroup analysis for response rate was performed based on cladribine monotherapy or cladribine in combinations if relevant data were available.
Results
Search results
Our initial electronic search of PubMed, EMBASE, and Cochrane Library retrieved a total of 255 publications. The PRISMA flow diagram of study selection is shown in Figure 1. After removal of duplicates, 231 articles were screened for eligibility. After the screening of titles and abstracts, 16 were identified for full-text review. Finally, the reviewers identified 10 publications for qualitative and quantitative analysis. Reasons for exclusion of studies not included in the final review were an evaluation of patients with high risk rather than refractory AML, heterogeneous populations with other hematologic malignancies (including ALL), no record of survival outcomes and multiple presentations of the same study.
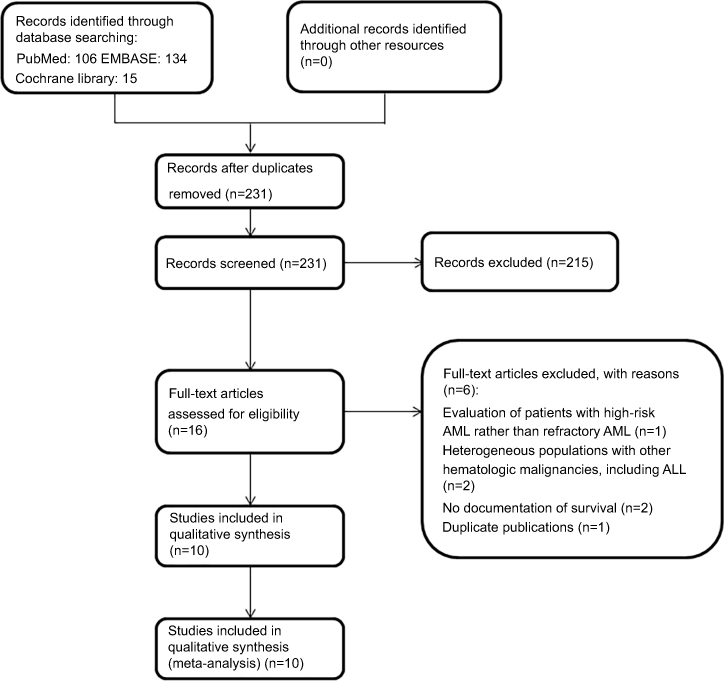 | Figure 1 PRISMA flow diagram of the study selection process. Abbreviations: AML, acute myeloid leukemia; ALL, acute lymphoid leukemia. |
Study characteristics and the risk of bias
There were a total of 422 patients in the 10 included studies.11–17,21–23 Characteristics of the included studies are shown in Table 1. Ten studies included in this meta-analysis are all prospective studies. There were no randomized clinical trials that met the inclusion criteria. The studies included in this meta-analysis showed high variability in terms of sample size, ranging from 14 to 114. The median age for refractory AML patients in these studies ranged from 42 to 69 years. CR rate was reported by all the 10 studies and the ORR was also reported by seven studies, of which quantitative analysis could be done. Median OS and DFS were provided the median time and a corresponding 95% CI by several studies. Three of the 10 trials use the cladribine or cladribine-base treatment protocol.11,17,21 The remaining seven trials used CLAG or CLAG-based treatment protocol, of which three trials were standard CLAG chemotherapy (2-CdA 5 mg/m2 iv d1–5, Ara-C 2 g/m2 iv d1–5, G-CSF 300 µg sc d0–5).12–14 And the other four trials were CLAG in a combination of another chemotherapy drug like MIT, imatinib mesylate, and topotecan.15,16,22,23
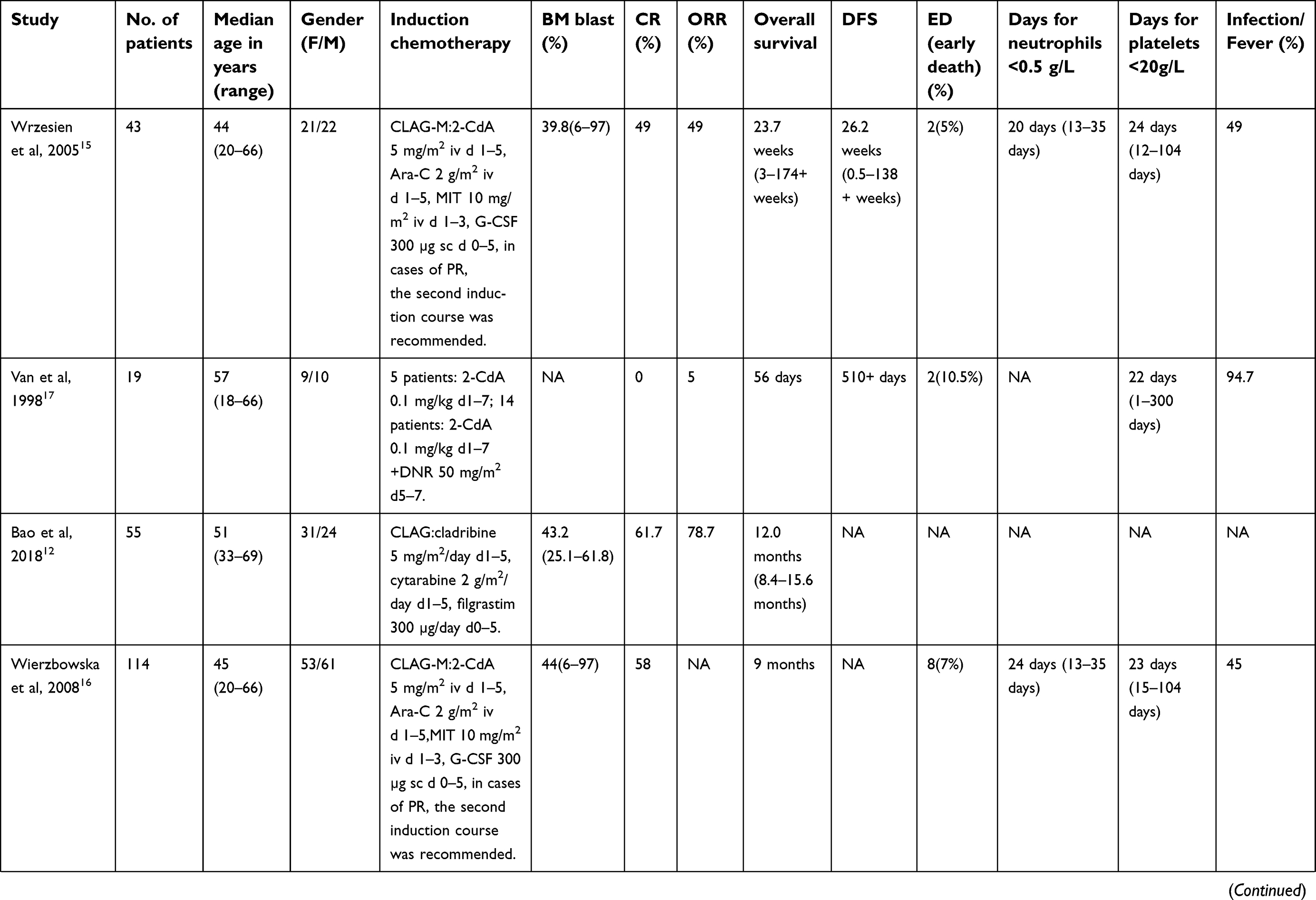 | Table 1 Characteristics of the studies included in this meta-analysis |
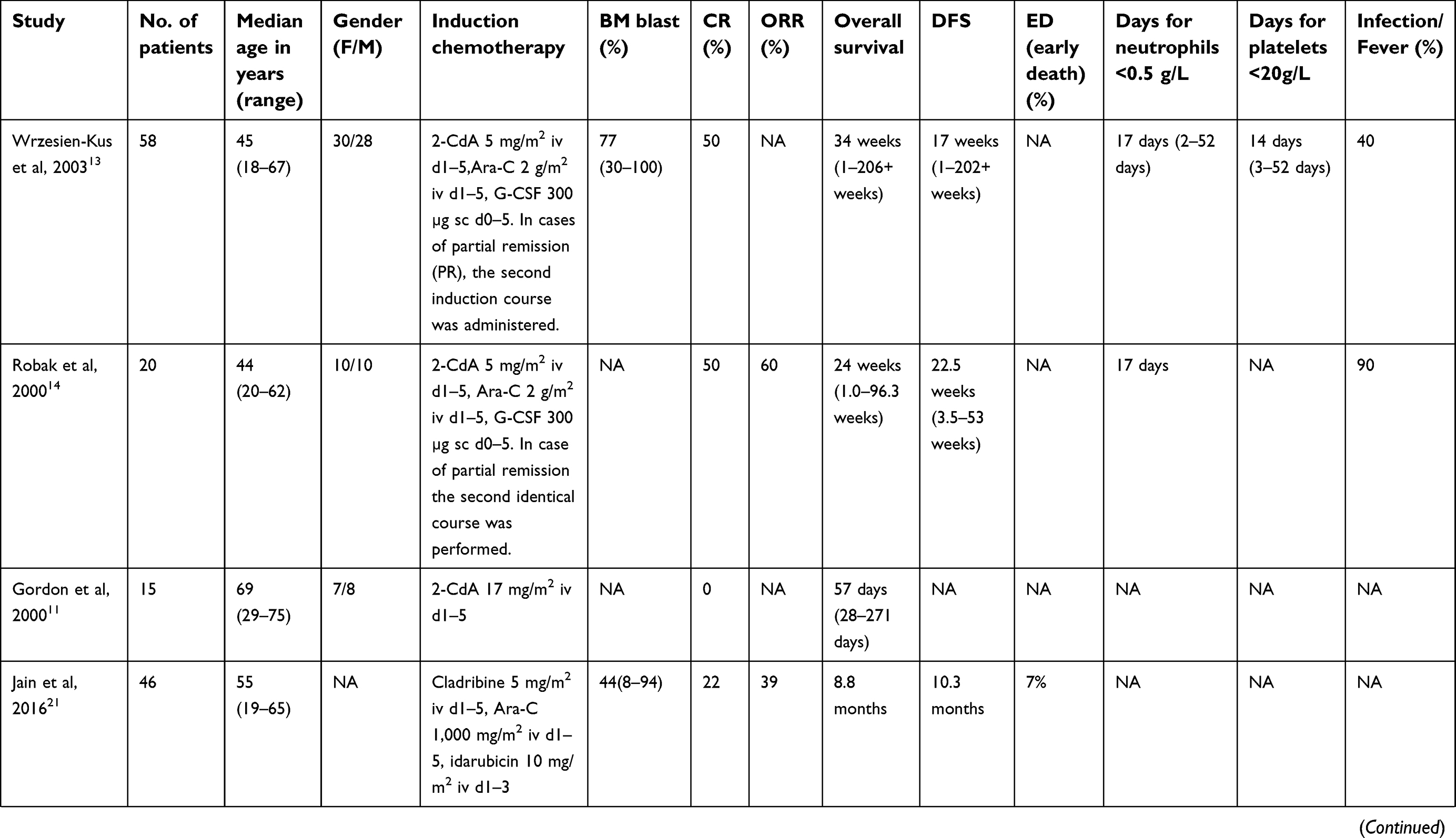 | Table 1 (Continued). |
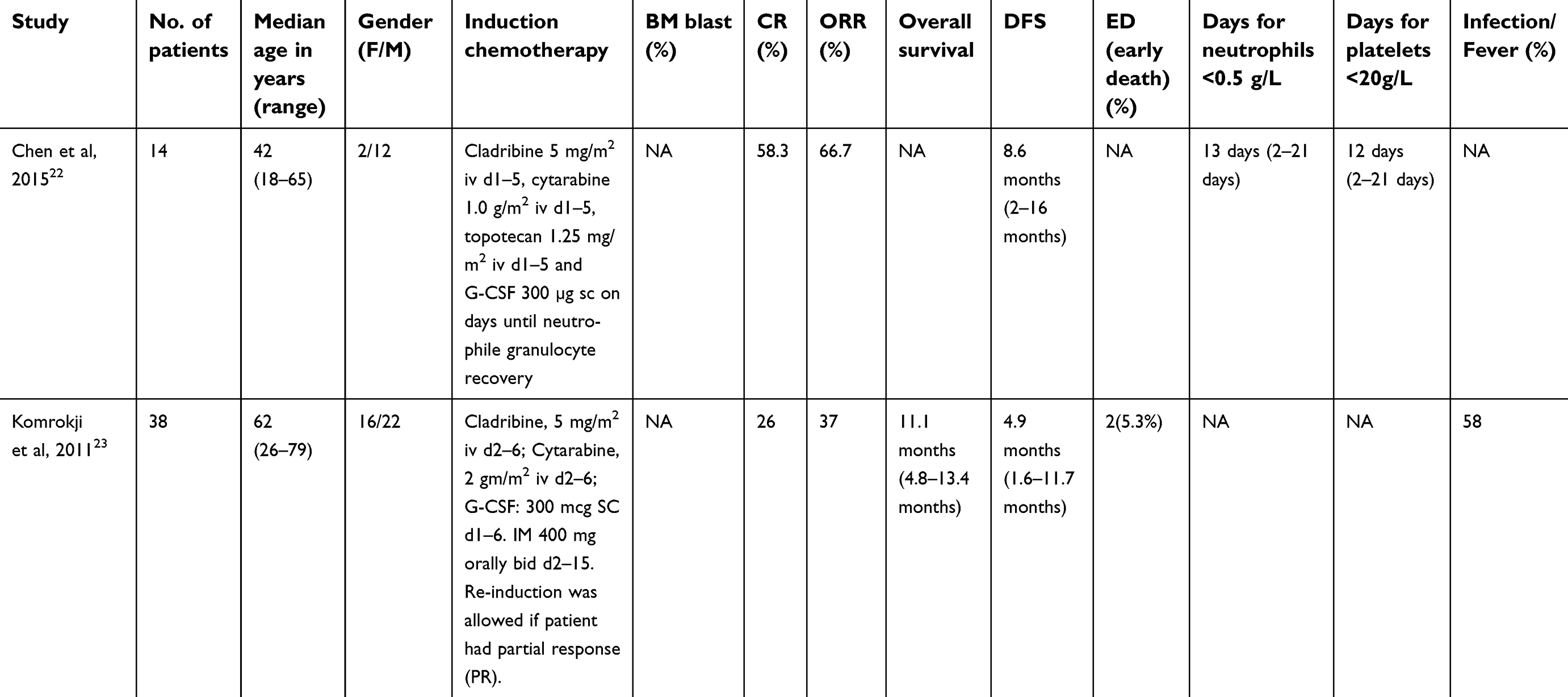 | Table 1 (Continued). |
The 10 included studies were evaluated by the modified Newcastle-Ottawa Scale. Publication bias was assessed graphically with funnel plots. There appeared to be an element of publication bias in terms of the primary outcomes of this meta-analysis.
Efficacy
Both CR and ORR rate were analyzed in this meta-analysis. Data for CR rate were available for analysis from a total of 10 trials including 422 patients. The CR rate ranged from 0% to 61.7%, with the lowest one in the cladribine-based schedule,11,17 and the highest one in the standard CLAG chemotherapy.12 The overall rate of CR was 42.2% (95% CI: 31.0–54.3%) as determined by the random-effects model since the CR rates of 10 trials were highly heterogeneous (Q=38.846, I2=76.82, P<0.001, Figure 2).
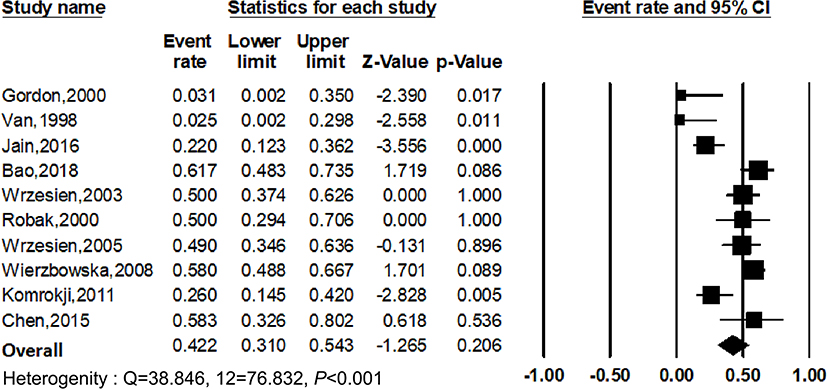 | Figure 2 Forest plot of the estimated proportions (95% CI) for complete remission (CR) rate in patients. |
For the ORR rate, data of 235 patients enrolled in seven trials were available for meta-analysis. The ORR rate ranged from 5% to 78.7%, with the lowest rate in the cladribine-based schedule,17 and the highest one in the standard CLAG chemotherapy.12 The ORR rate of seven trials was also highly heterogeneous (Q=30.332, I2=80.219, P<0.001, Figure 3). Thus, the overall rate of ORR which determined by the random-effects model was 49.7% (95% CI: 33.5–66.0%).
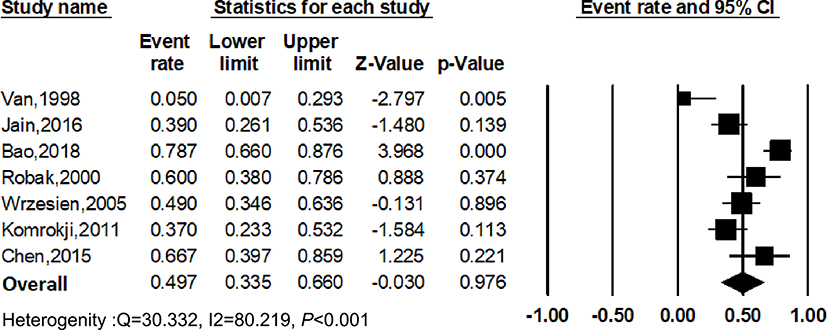 | Figure 3 Forest plot of the estimated proportions (95% CI) for overall response rate (ORR) in patients. |
The OS of refractory AML patients treated with cladribine or cladribine-related protocols was reported in nine studies. Overall, the median OS ranged from 56 days to 12 months (Table 1).
Subgroup analysis
To explore the heterogeneity of the included studies, subgroup analysis according to different treatment protocols was constructed. The results showed that CR rate of cladribine monotherapy was 2.8% (95% CI: 0.4–17.4%; Figure 4A) and that of CLAG-based chemotherapy was 50.9% (95% CI: 42.2–59.4%; Figure 4B), which suggested that CLAG-based treatment protocol had higher effects in refractory AML patients. However, the subgroup analysis of CLAG-based protocol still presented moderate heterogeneity (Q=13.914, I2=55.287, P=0.037), therefore we did further statistical analyses. The results turned out that CR rate of CLAG or CLAG-M chemotherapy was 55.2% (95% CI: 49.4–60.8%; Figure 4C), and that of standard CLAG chemotherapy was 54.8% (95% CI: 46.2–63.1; Figure 4D), which were both determined by the fixed-effect model since no heterogeneity existed.
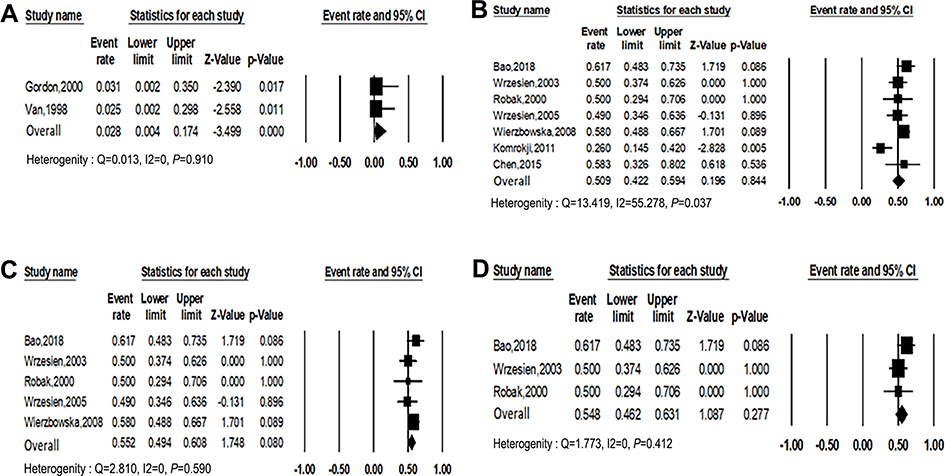 | Figure 4 Forest plots of the estimated proportions of complete remission (CR) rate by cladribine monotherapy (A), CLAG-based chemotherapy (B), CLAG/CLAG-M chemotherapy (C), standard CLAG chemotherapy (D). |
In addition to the above, we also performed a subgroup analysis of cytogenetic risk in five trials which contained efficacy analysis of different risk stratification. The results showed that CR rate of favorable risk was 86.6% (95% CI: 63.0–90.1%; Figure 5A), while that of intermediate risk and unfavorable risk decreased to 58.3% (95% CI: 49.2–66.8%; Figure 5B) and 42.5% (95% CI: 30.5–55.4%; Figure 5C) separately, suggesting that escalating cytogenetic risk could decrease the efficacy of cladribine-based regimen.
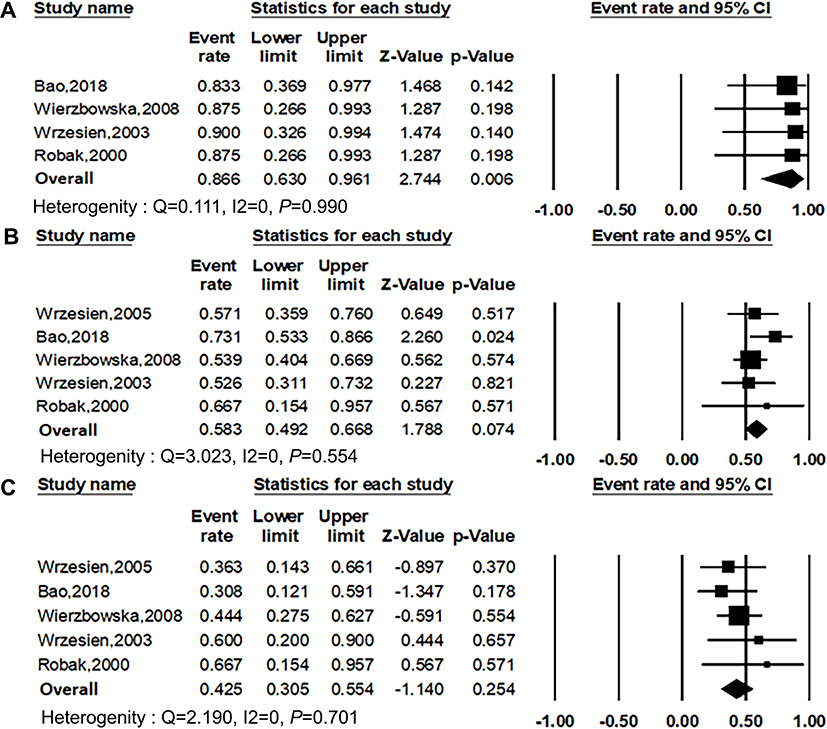 | Figure 5 Forest plots of the estimated proportions of complete remission (CR) rate by favorable risk (A), intermediate risk (B), unfavorable risk (C). |
Toxicity
Toxicities associated with cladribine-based treatment protocol were mentioned in nine articles, including both hematological and non-hematological toxicities.11,13–17,21–23 For patients treated with cladribine-related chemotherapy, thrombocytopenia, anemia, and neutropenia were the most common grade 3 and 4 adverse events (AEs). Almost all the patients experienced peripheral blood cytopenia. As for the non-hematological toxicity, the infection was presented in all these studies, which is a major cause of death for patients after chemotherapy. The median time of neutropenia (neutrophils <0.5 g/L) were reported in five studies, ranged from 13 to 24 days.13–16,22 And the mean duration of thrombocytopenia ranged from 12 to 24 days as described in clinical results.13,15–17,22
For the early death rate, data of 260 patients enrolled in five trials were available. The overall early death rate was 6.8% (95% CI: 4.3–10.6%) as determined by the fixed-effects model (heterogeneity analysis: Q=0.765, I2=0, P=0.943; Figure 6). Taken together, the major cause of the early death of the patients was severe infectious complications.
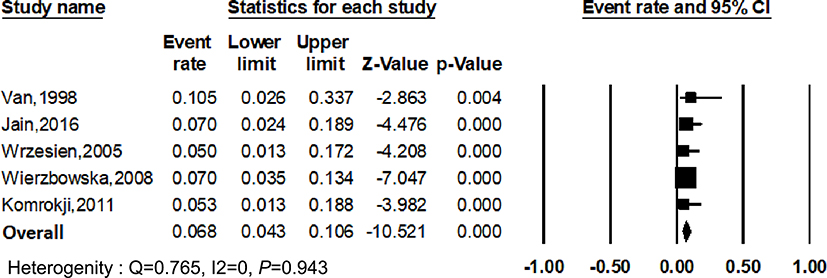 | Figure 6 Forest plot of the estimated proportions (95% CI) for early death rate in patients. |
Overall, hematological toxicity and infections were the most prominent toxicities regardless of the subgroups of the treatment protocol. There was no specific quantitative data on the toxicity of cladribine monotherapy, and the side effects of cladribine-based regimens were tolerable and mostly reversible. Compared with CLAG alone, the addition of MIT to CLAG influenced neither the mean duration of neutropenia nor the median time of hospitalization.
Discussion
Cladribine, as a single agent, has shown its anti-leukemic activity in patients with AML. A better outcome was achieved in pediatric patients rather than in adults.9,24 This study showed that the effect of cladribine and its combination on CR and ORR rate of refractory AML patients were 42.2% (95% CI: 31.0–54.3%) and 49.7% (95% CI: 33.5–66.0%), respectively. The results confirm the effectiveness of cladribine-based treatment protocol in refractory AML patients although significant heterogeneity exists in these trials enrolled, which may decrease the credibility of the final results to some extent. Substantial efforts have been made to explore the possible causes for heterogeneity of these included trials, and it turns out that the diversity of the treatment protocols may be the major cause of the significant heterogeneity. Thus, in our analysis, we used the random-effects model to minimize the bias and also employed the subgroup analysis based on the therapeutic schedule to reduce heterogeneity and improve the reliability of the results. Our studies found the superiority of CLAG-based chemotherapy on CR, ORR, and survival comparing to that of cladribine-based treatment in refractory AML patients.
It is reported that pretreatment with cladribine increased the rate of Ara-CTP accumulation in leukemic blasts by 50–65% in vitro and in vivo pharmacological studies, and the addition of G-CSF may further improve the effects of cladribine in combination with Ara-C.25,26 Our analyzed data here also indicated the superiority of CLAG-based induction chemotherapy in refractory AML patients compared to cladribine monotherapy. Moreover, cladribine combined regimens with Ara-C and/or other agents were also used in de novo adult patients with AML.27–29 Holowiecki et al found that the CR rate in the treatment group with daunorubicine, cytarabine, and cladribine (DAC) arm was higher than that of the DA arm (67.5% v 56%; P=0.01), which further resulted in the reduced incidence of resistant disease in the DAC group than DA group (21% v 34%; P=0.004) in a cohort study with new-diagnosed AML patients; and, a survival advantage of the DAC arm over the DA arm was also observed among patients age 50 years or older (P=0.005) in this study.29,30 Consistent with other reports, our analyzed data showed that the addition of cladribine to the standard induction regimen is superior to the standard induction regimen alone. Therefore, cladribine combined with standard drugs should be more widely utilized as a frontline and salvage treatment for AML patients since its advantage in increasing the CR rate and extending the lifespan of untreated adult AML patients.
Our results found that adding MIT to the standard CLAG treatment protocol may have a slight advantage in increasing the CR rate of refractory AML patients. However, not all the anti-leukemia drugs can exert a synergistic effect with CLAG chemotherapy. For example, it is reported that the CLAG protocol combined with imatinib or topotecan could decrease the CR rate of patients and largely influenced the therapeutic effects of the original scheme. Based on those, it requires more pharmacological experiments and pre-clinical trials to support whether or not adding MIT to CLAG scheme.
Cladribine is a purine analog that is converted to its active triphosphate form in cells with high levels of deoxycytidine kinase and low 5′-nucleotidase activity.31 The triphosphate form resists degradation and accumulates to cytotoxic levels inside cells, which inhibits DNA synthesis, prevents DNA repair, and induces programmed cell death.32,33 Several studies have demonstrated that cladribine increases the cellular uptake of Ara-C and the accumulation of its active cytotoxic metabolite (Ara-CTP) in leukemic blasts.25,26 MIT is able to inhibit both DNA replication and DNA-dependent RNA synthesis by intercalating into DNA and causing crosslinking and strand breaks. It can also inhibit topoisomerase II and consequently interfere with DNA repair.34 Therefore, the addition of MIT to the CLAG regimen may exert synergy effects and strengthen the inhibition of DNR repair, which accelerates the apoptosis of leukemic blasts and induces remission of refractory AML.
Toxicities related to cladribine-related treatment were not specifically analyzed in this paper because of very limited data availability. Authors used various criteria to measure the incidence of AEs and the observed clinical outcomes varied from each other. Some trials only gave a rough summary of hematologic and non-hematologic AEs without specific data. The most common hematologic toxicities included neutropenia and thrombocytopenia, and the most common non-hematologic toxicities included nausea/vomiting, diarrhea, mucositis, and hemorrhage.
This study has several limitations. None of the randomized controlled trials was included, even the cohort studies were very few. Most of the studies included in the final quantitative analysis here were single-arm Phase II clinical trials, which may be in the range of the relatively low confidence. Another limitation is significant heterogeneity. To make the baseline characteristics of included patients more comparable, we selected the adult patients (≥18 years) suffering from refractory AML with a normal heart, lung, renal, and hepatic function in our study, in addition, to reduce the significant heterogeneity by using the random-effects model. The possible causes for heterogeneity are possibly mainly because of the different schedules and the various average daily dose applied in these trials; we included all the prospective studies using treatment protocols containing cladribine without the requirement of identical combination strategies and doses of the drugs. Therefore, in the subgroup analysis including a similar treatment protocol and drug dose, the significant heterogeneity was disappeared. Besides, all patients included have previously received at least a standardized first-line treatment; some even have accepted allogeneic or autologous stem cell transplantation before. And the number of prior chemotherapy courses of patients included in our analysis ranged from 1 to 9, which may also contribute to the heterogeneity. Additionally, publication bias may exist since unpublished articles were not included in our meta-analysis, and the number of patients and trials enrolled in this study was relatively small, therefore, more large-sample and high-quality clinical trials are needed to increase the reliability of our findings. Whatever our study has provided a comprehensive evaluation of cladribine-based chemotherapy as an effective treatment of refractory AML.
Conclusion
Our meta-analysis observed that nearly half of the refractory AML patients responded to cladribine-based treatments, which demonstrated that cladribine-based therapies are effective in refractory AML with an overall CR rate of 42.2% (95% CI: 31.0–54.3%) and ORR rate of 49.7% (95% CI: 33.5–66.0%). Based on the combined schedule of CLAG achieves much significantly higher efficacy than cladribine monotherapy in CR rate, it is strongly recommended to use the cladribine-based combined therapy in refractory AML and also it is valuable to explore the best cladribine-based therapeutic approach for refractory AML in future.
Acknowledgments
This work is supported in part by The National Natural Science Foundation of China (81770172); Key Research & Technology Projects in Jiangsu Province (BE2017747); Milstein Medical Asian American Partnership (MMAAP) Foundation Research Project Award in Hematology (2017).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Robak T, Wrzesien-Kus A. The search for optimal treatment in relapsed and refractory acute myeloid leukemia. Leuk Lymphoma. 2002;43:281–291. doi:10.1080/10428190290006053
2. Edenfield WJ, Gore SD. Stage-specific application of allogeneic and autologous marrow transplantation in the management of acute myeloid leukemia. Semin Oncol. 1999;26:21–34.
3. Thol F, Schlenk RF, Heuser M, Ganser A. How I treat refractory and early relapsed acute myeloid leukemia. Blood. 2015;126:319–321. doi:10.1182/blood-2014-10-551911
4. Freyer CW, Gupta N, Wetzler M, Wang ES. Revisiting the role of cladribine in acute myeloid leukemia: an improvement on past accomplishments or more old news? Am J Hematol. 2015;90:62–72. doi:10.1002/ajh.23862
5. Lofgren C, Albertioni F, Paul C. High activity and incomplete cross resistance of nucleoside analogues cladribine and fludarabine versus Ara-C on leukemic cells from patients with AML. Ther Drug Monit. 2005;27:641–646.
6. Hubeek I, Peters GJ, Broekhuizen R, et al. In vitro sensitivity and cross-resistance to deoxynucleoside analogs in childhood acute leukemia. Haematologica. 2006;91:17–23.
7. Parker WB. Enzymology of purine and pyrimidine antimetabolites used in the treatment of cancer. Chem Rev. 2009;109:2880–2893. doi:10.1021/cr900028p
8. Robak T, Lech-Maranda E, Korycka A, Robak E. Purine nucleoside analogs as immunosuppressive and antineoplastic agents: mechanism of action and clinical activity. Curr Med Chem. 2006;13:3165–3189.
9. Vahdat L, Wong ET, Wile MJ, Rosenblum M, Foley KM, Warrell RP. Therapeutic and neurotoxic effects of 2-chlorodeoxyadenosine in adults with acute myeloid leukemia. Blood. 1994;84:3429–3434.
10. Santana VM, Mirro J, Kearns C, Schell MJ, Crom W, Blakley RL. 2-Chlorodeoxyadenosine produces a high rate of complete hematologic remission in relapsed acute myeloid leukemia. J Clin Oncol. 1992;10:364–370. doi:10.1200/JCO.1992.10.3.364
11. Gordon MS, Young ML, Tallman MS, et al. Phase II trial of 2-chlorodeoxyadenosine in patients with relapsed/refractory acute myeloid leukemia: a study of the Eastern Cooperative Oncology Group (ECOG), E5995. Leuk Res. 2000;24:871–875.
12. Bao Y, Zhao J, Li ZZ. Comparison of clinical remission and survival between CLAG and FLAG induction chemotherapy in patients with refractory or relapsed acute myeloid leukemia: a prospective cohort study. Clin Transl Oncol. 2018;20:870–880. doi:10.1007/s12094-017-1798-8
13. Wrzesien-Kus A, Robak T, Lech-Marańda E, et al. A multicenter, open, non-comparative, phase II study of the combination of cladribine (2-chlorodeoxyadenosine), cytarabine, and G-CSF as induction therapy in refractory acute myeloid leukemia - a report of the Polish Adult Leukemia Group (PALG). Eur J Haematol. 2003;71:155–162.
14. Robak T, Wrzesień-Kuś A, Lech-Marańda E, Kowal M, Dmoszyńska A. Combination regimen of cladribine (2-chlorodeoxyadenosine), cytarabine and G-CSF (CLAG) as induction therapy for patients with relapsed or refractory acute myeloid leukemia. Leuk Lymphoma. 2000;39:121–129. doi:10.3109/10428190009053545
15. Wrzesien-Kus A, Robak T, Wierzbowska A, et al. A multicenter, open, noncomparative, phase II study of the combination of cladribine (2-chlorodeoxyadenosine), cytarabine, granulocyte colony-stimulating factor and mitoxantrone as induction therapy in refractory acute myeloid leukemia: a report of the Polish Adult Leukemia Group. Ann Hematol. 2005;84:557–564. doi:10.1007/s00277-005-1046-0
16. Wierzbowska A, Robak T, Pluta A, et al. Cladribine combined with high doses of arabinoside cytosine, mitoxantrone, and G-CSF (CLAG-M) is a highly effective salvage regimen in patients with refractory and relapsed acute myeloid leukemia of the poor risk: a final report of the Polish Adult Leukemia Group. Eur J Haematol. 2008;80:115–126. doi:10.1111/j.1600-0609.2007.00988.x
17. Van Den Neste E, Martiat P, Mineur P, et al. 2-Chlorodeoxyadenosine with or without daunorubicin in relapsed or refractory acute myeloid leukemia. Ann Hematol. 1998;76:19–23.
18. Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0. The Cochrane Collaboration. 2011. Available from:
19. Wells GA, Tugwell P, O’Connell D, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. 2012. Available from:
20. Xie CH, Wei M, Yang F-Y, et al. Efficacy and safety of lenalidomide for the treatment of acute myeloid leukemia: a systematic review and meta-analysis. Cancer Manag Res. 2018;10:3637–3648. doi:10.2147/CMAR.S168610
21. Jain P, Kantarjian HM, Ravandi F, et al. Cladribine combined with idarubicin and Ara-C (CLIA) as a frontline and salvage treatment for young patients (<65 yrs) with acute myeloid leukemia. Blood. 2018;132:4039.
22. Chen X, Weng J, Wang Y, et al. Combination of cladribine, cytarabine and topotecan (CLAT) for relapsed or refractory acute myeloid leukemia. Blood. 2015;126:4897.
23. Komrokji RS, Pinilla-Ibarz J, Yu D, et al. A phase II study of CLAG regimen in combination with imatinib mesylate in relapsed or refractory acute myeloid leukemia. Blood. 2011;118:2604. doi:10.1182/blood-2011-02-334870
24. Krance RA, Hurwitz CA, Head DR, et al. Experience with 2-chlorodeoxyadenosine in previously untreated children with newly diagnosed acute myeloid leukemia and myelodysplastic disease. J Clin Oncol. 2001;19:2804–2811. doi:10.1200/JCO.2001.19.11.2804
25. Kornblau SM, Gandhi V, Andreeff HM, et al. Clinical and laboratory studies of 2-chlorodeoxyadenosine + cytosine arabinoside for relapsed or refractory acute myelogenous leukemia in adults. Leukemia. 1996;10:1563–1569.
26. Gandhi V, Estey E, Keating MJ, Chucrallah A, Plunkett W. Chlorodeoxyadenosine and arabinosylcytosine in patients with acute myelogenous leukemia: pharmacokinetic, pharmacodynamic and molecular interactions. Blood. 1996;87:256–264.
27. Martin MG, Welch JS, Augustin K, Hladnik L, DiPersio JF, Abboud CN. Cladribine in the treatment of acute myeloid leukemia: a single-institution experience. Clin Lymphoma Myeloma. 2009;9:298–301. doi:10.3816/CLM.2009.n.058
28. Juliusson G, Lofgren C, Mollgard L, et al. No additional toxicity from cladribine (CdA) as primary treatment of acute myeloid leukemia in elderly patients: results from a randomized phase II study from the Leukemia Group of Middle Sweden (LGMS). Blood. 2001;98:518.
29. Hołowiecki J, Grosicki S, Robak T, et al. Addition of cladribine to daunorubicin and cytarabine increases complete remission rate after a single course of induction treatment in acute myeloid leukemia. Multicenter phase III study. Leukemia. 2004;18:989–997. doi:10.1038/sj.leu.2403336
30. Holowiecki J, Grosicki S, Giebel S, et al. Cladribine, but not fludarabine, added to daunorubicin and cytarabine during induction prolongs survival of patients with acute myeloid leukemia: a multicenter, randomized phase III study. J Clin Oncol. 2012;30:2441–2448. doi:10.1200/JCO.2011.37.1286
31. Kawasaki H, Carrera CJ, Piro LD, Saven A, Kipps TJ, Carson DA. Relationship of deoxycytidine kinase and cytoplasmic 5′-nucleotidase to the chemotherapeutic efficacy of 2-chlorodeoxyadenosine. Blood. 1993;81:597–601.
32. Griffig J, Koob R, Blakley RL. Mechanisms of inhibition of DNA synthesis by 2-chlorodeoxyadenosine in human lymphoblastic cells. Cancer Res. 1989;49:6923–6928.
33. Carrera CJ, Terai C, Lotz M, et al. Potent toxicity of 2-chlorodeoxyadenosine toward human monocytes in vitro and in vivo. A novel approach to immunosuppressive therapy. J Clin Invest. 1990;86:1480–1488. doi:10.1172/JCI114865
34. Levine S, Gherson J. Morphologic effects of mitoxantrone and a related anthracenedione on lymphoid tissues. Int J Immunopharmacol. 1986;8:999–1007.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.