")
Back to Journals » Clinical Ophthalmology » Volume 10
Efficacy and tolerability of benzalkonium chloride-free travoprost in glaucoma patients switched from benzalkonium chloride-preserved latanoprost or bimatoprost
Authors García-Feijoo J, Muñoz-Negrete FJ , Hubatsch DA, Rossi GC
Received 13 May 2016
Accepted for publication 26 July 2016
Published 21 October 2016 Volume 2016:10 Pages 2085—2091
DOI https://doi.org/10.2147/OPTH.S112711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Julian García-Feijoo,1 Francisco J Muñoz-Negrete,2 Douglas A Hubatsch,3 Gemma C Rossi4
On behalf of the study investigators
1Department of Ophthalmology, Instituto de Investigación Sanitaria del Hospital Clínico San Carlos, Universidad Complutense, OFTARED, 2Hospital UniversItario Ramón y Cajal, Universidad de Alcalá, IRYCIS, OFTARED, Madrid, Spain; 3Alcon Laboratories, Inc., Fort Worth, TX, USA; 4Department of Ophthalmology, University Eye Clinic, IRCCS Policlinico San Matteo Foundation, Pavia, Italy
Introduction: The preservative benzalkonium chloride (BAK) is used to preserve several topical, intraocular pressure (IOP)-lowering glaucoma medications but can cause tolerability concerns that may lead to decreased adherence to treatment and ultimately diminish the effectiveness of IOP control. The study aimed to determine the efficacy and tolerability of BAK-free travoprost preserved with polyquaternium-1 in glaucoma patients switched from BAK-preserved latanoprost or bimatoprost.
Methods: This 12-week, open-label study was conducted in Europe between December 2011 and February 2013. We enrolled adult patients with open-angle glaucoma or ocular hypertension who were receiving BAK-preserved latanoprost 0.005% or bimatoprost 0.01% and, in the opinion of the investigator, would benefit from transition to BAK-free travoprost 0.004% preserved with polyquaternium-1 because of tolerability concerns. Assessments included IOP, proportion of patients with IOP ≤18 mmHg, ocular surface status, hyperemia, patient treatment preference, and adherence. Adverse events were recorded throughout the study.
Results: Of the 202 patients screened, 187 patients were included in the intent-to-treat population (mean age, 66.6 years; range, 19–90 years). The mean IOP significantly reduced from baseline (17.0 mmHg) to week 6 (mean change, -1.17 mmHg; P<0.001) and week 12 (-1.16 mmHg; P<0.001). At week 12, more patients achieved IOP ≤18 mmHg (81.2% versus 73.3% at baseline), and ocular surface disease severity improved from baseline to week 12. Most patients preferred BAK-free travoprost (74.9%) versus their previous medication and were very confident in their adherence (84.1%). Reduced visual acuity and eye pruritus were the most common adverse events (2.5% each).
Conclusion: BAK-free travoprost 0.004% preserved with polyquaternium-1 was efficacious and well tolerated and may be an advantageous prostaglandin analog option for patients with open-angle glaucoma or ocular hypertension who are intolerant to BAK-preserved latanoprost or bimatoprost.
Keywords: benzalkonium chloride, intraocular pressure, polyquad, polyquaternium-1, prostaglandin analog, switch, travoprost
Introduction
Glaucoma is a progressive disease affecting the optic nerve1 and is the second leading cause of blindness worldwide.2 The etiology of glaucoma is multifactorial, but elevated intraocular pressure (IOP) has been associated with the risk and progression of the disease, resulting in visual field loss and optic disk cupping.1,3–5 Reduction of IOP is the only evidence-based treatment strategy for slowing glaucoma progression.1 To reduce IOP to target levels, the European Glaucoma Society and previous studies recommend a therapy with topical medications as initial treatment.6–8
Several topical, IOP-lowering medications are available, but prostaglandin analogs (eg, latanoprost, bimatoprost, tafluprost, and travoprost), which reduce IOP by increasing uveoscleral outflow of aqueous humor, are recommended as the first-line therapies by the European Glaucoma Society and previously reported studies because of their efficacy, favorable side-effect profile, and convenience.6–9 Latanoprost, bimatoprost, and travoprost provide greater IOP reduction than β-blockers; however, this increased efficacy is accompanied by a greater incidence of ocular hyperemia.10–13 A randomized, parallel-group, single-masked study (n=410) showed similar IOP-lowering efficacies of bimatoprost, latanoprost, and travoprost.14 Travoprost has been shown to maintain a mean IOP reduction of 30% throughout a 24-hour dosing interval15 and was more efficacious than latanoprost over a 48-hour period after the last dose.16 Among prostaglandin analogs, peak percentage reductions in IOP were similar with bimatoprost (33%), latanoprost (31%), and travoprost (29%),17 with higher rates of ocular hyperemia reported with travoprost 0.004% and bimatoprost 0.03% compared with latanoprost 0.005%.10,12,17
Benzalkonium chloride (BAK) is the most commonly used preservative in ophthalmic medications and has been associated with various ocular surface symptoms, including hyperemia, burning, stinging, punctate keratitis, foreign body sensation, and dry eye.18–20 Bimatoprost 0.01% and latanoprost 0.01% each contain 0.02% BAK, and travoprost 0.004% contains 0.015% BAK. These BAK concentrations have been shown to exert cytotoxic effects on cultured conjunctival and corneal epithelial cells and trabecular meshwork cell lines21,22 and cause pathologic alterations in corneal and conjunctival morphologies in animal models.23
In an effort to reduce ocular symptoms and avoid the corneal damage and tear film disruption associated with chronic BAK exposure,24 a BAK-free formulation of travoprost 0.004% containing the preservative polyquaternium-1 has been developed. In a randomized, multicenter, parallel-group, double-masked study, BAK-free travoprost preserved with polyquaternium-1 provided IOP control equivalent to that with BAK-preserved travoprost, with a lower incidence of ocular hyperemia.25 Limited data are available regarding the comparisons of polyquaternium-1-preserved travoprost with BAK-preserved formulations of other prostaglandin analogs.
The present study aimed to assess the efficacy and tolerability of BAK-free travoprost 0.004% preserved with polyquaternium-1 in patients with open-angle glaucoma or ocular hypertension who were intolerant to BAK-preserved latanoprost 0.005% or bimatoprost 0.01%.
Methods
This 12-week, open-label, single-group study (ClinicalTrials.gov ID, NCT01493427; EudraCT ID, 2011-003816-21) was performed in Belgium, Spain, Italy, and Sweden between December 2011 and February 2013. The study was approved by the ethical committees of the following institutions: Hospital Clinico San Carlos-IdISSC, Hospital Ramon y Cajal, and Policlinico San Mateo, and was compliant with the Health Insurance Portability and Accountability Act and the ethical standards set forth by the Declaration of Helsinki and Good Clinical Practice. All patients provided written informed consent before any screening procedures were performed.
Patients eligible for inclusion were aged ≥18 years with open-angle glaucoma or ocular hypertension who were receiving treatment with BAK-preserved latanoprost 0.005% or bimatoprost 0.01% (branded or generic) for ≥4 weeks and who, in the opinion of the investigator, would benefit from a therapeutic switch because of tolerability concerns (based at the discretion of the study investigators). IOP in both eyes must have been safe in the opinion of the investigator such that vision and optic nerve integrity were maintained. In addition, IOP must have been <30 mmHg while receiving latanoprost or bimatoprost. If the nonstudy eye required a pharmacologic therapy for IOP control, it was required to be controlled with the study medication alone (ie, BAK-free travoprost 0.004%). A best-corrected visual acuity of at least 6/60 Snellen (1.0 logMAR) was required in both eyes. All patients had to be willing and able to provide informed consent and discontinue other ocular hypotensive medications.
Women who were pregnant or lactating were not allowed to participate. Patients with any abnormality that prevented reliable applanation tonometry; patients with corneal dystrophy, conjunctivitis, keratitis, uveitis, or progressive retinal or optic nerve disease; and patients who had an intraocular or laser surgery ≤3 months before screening were excluded. Use of punctal plugs, punctal cautery, cyclosporine ophthalmic emulsion (Restasis®; Allergan, Inc., Irvine, CA, USA), or topical ocular corticosteroids for dry eye or keratoconjunctivitis sicca was not allowed. Systemic medications capable of altering IOP were permitted but must have been stabilized for ≥7 days before screening.
Eligible patients discontinued latanoprost or bimatoprost and self-administered one drop of BAK-free travoprost 0.004% preserved with polyquaternium-1 (Travatan® preserved with POLYQUAD®; Alcon Laboratories, Inc., Fort Worth, TX, USA) every evening at ~8 pm for 12 weeks. No washout period was planned between medications. If only one of the patient’s eyes was dosed, the dosed eye was selected for analysis. If both eyes were dosed, then the worse evaluable eye was selected for analysis. The worse eye was the eye with the higher IOP at the screening visit. If both eyes were equal, then the right eye was selected for analysis.
IOP was assessed using Goldmann applanation tonometry at the screening/baseline visit and during on-therapy visits at weeks 6 (±3 days) and 12 (±3 days), at approximately the same time of day (±1 hour). To minimize confounding variables, all IOP measurements for individual patients were performed by the same operator using the same tonometer.
The primary efficacy endpoint was mean IOP change from baseline at week 12; IOP change from baseline to week 6 provided supportive data. The proportion of patients who achieved a target IOP of ≤18 mmHg at week 12 was a secondary endpoint; all other assessments were considered exploratory.
Adverse events (AEs) were recorded at each study visit and coded based on the Medical Dictionary for Regulatory Activities Version 15.0.
Descriptive statistics was provided for all study endpoints. The mean IOP change from baseline at week 12 was analyzed using a paired t-test. To assess the effect of time on IOP, the mean IOP at baseline, week 6, and week 12 was analyzed using a mixed model that included visit and current treatment (ie, latanoprost 0.005% and bimatoprost 0.01%) as fixed effects and the visit by treatment interaction and patients as random effects. Differences in the ocular symptom surveys from baseline to week 12 were analyzed using Wilcoxon signed-rank tests. Global preference responses were analyzed using an exact binomial test. Statistical analysis was performed using the SAS® 9.1.3 software (SAS Institute, Cary, NC, USA), with P-values <0.05 considered statistically significant.
Results
Of the 202 patients screened, 201 patients were eligible for participation and 179 patients completed the study (Figure 1). Two patients withdrew consent and did not receive the study drug; thus, 199 patients received ≥1 dose of the study medication (safety population). Of these, 187 patients completed ≥1 on-therapy visit and were defined as the intent-to-treat (ITT) population. Patients who received study medication, completed all study visits, and satisfied inclusion and exclusion criteria were included in the per-protocol population (n=144).
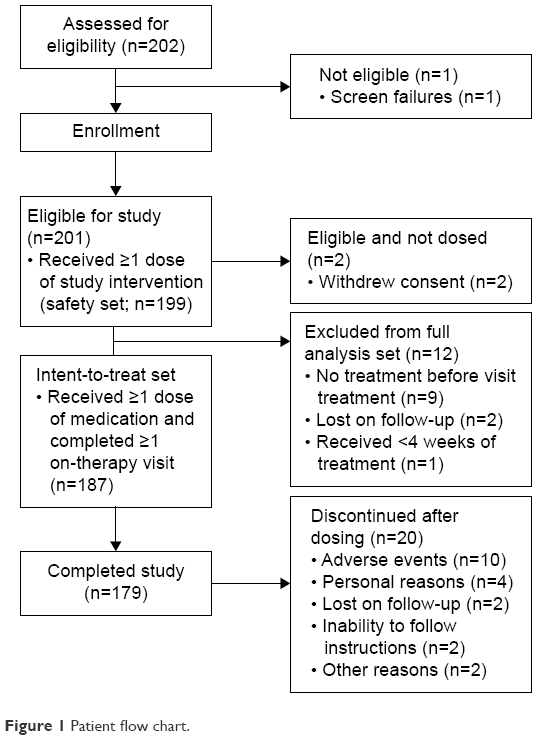 | Figure 1 Patient flow chart. |
The mean patient age was 66.6 years (range, 19–90 years; Table 1). Most patients were women (58.8%) and received latanoprost before transition to travoprost (78.4%).
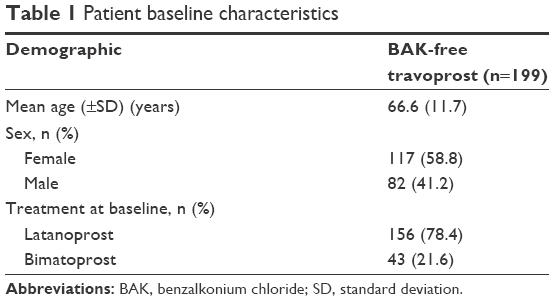 | Table 1 Patient baseline characteristics |
Efficacy results were similar in the ITT and per-protocol data sets; results for the ITT population are reported. The mean IOP was significantly reduced by 5.85% from baseline to week 12 (−1.16 mmHg; P<0.001; Figure 2); a similar IOP reduction was evident at week 6. Patients who had previously received latanoprost or bimatoprost at baseline had similar reductions in IOP at both time points (latanoprost: −1.24 mmHg to −1.50 mmHg; bimatoprost: −1.05 mmHg to −1.16 mmHg; P≤0.004 versus baseline for all time points and previous treatment groups). The proportion of patients who achieved an IOP of ≤18 mmHg was greater at week 6 (80.0%; n=144/180) and week 12 (81.2%; n=147/181) compared with that at baseline (73.3%; n=137/187).
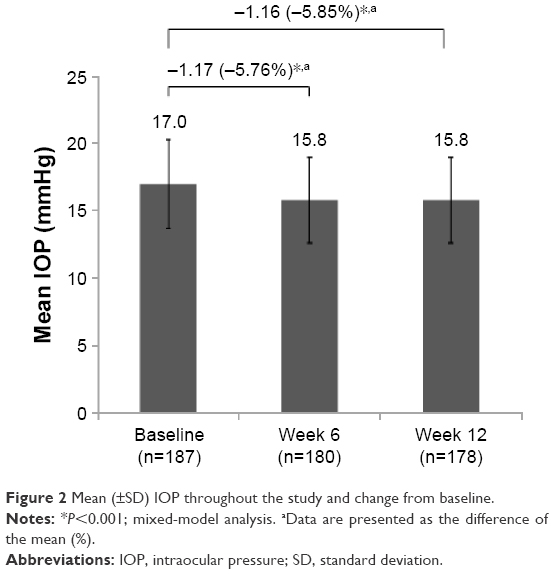 | Figure 2 Mean (±SD) IOP throughout the study and change from baseline. |
When asked to select between study medication and their previous medication, 74.9% of the patients (n=125/167) preferred BAK-free travoprost over previous latanoprost or bimatoprost (25.1%; n=42/167; P<0.001). Most patients were “very confident” that they would adhere to their treatment regimen if they were prescribed their preferred medication (84.1%; n=143/170) or a medication not associated with burning or stinging (69.4%; n=118/170; Figure 3).
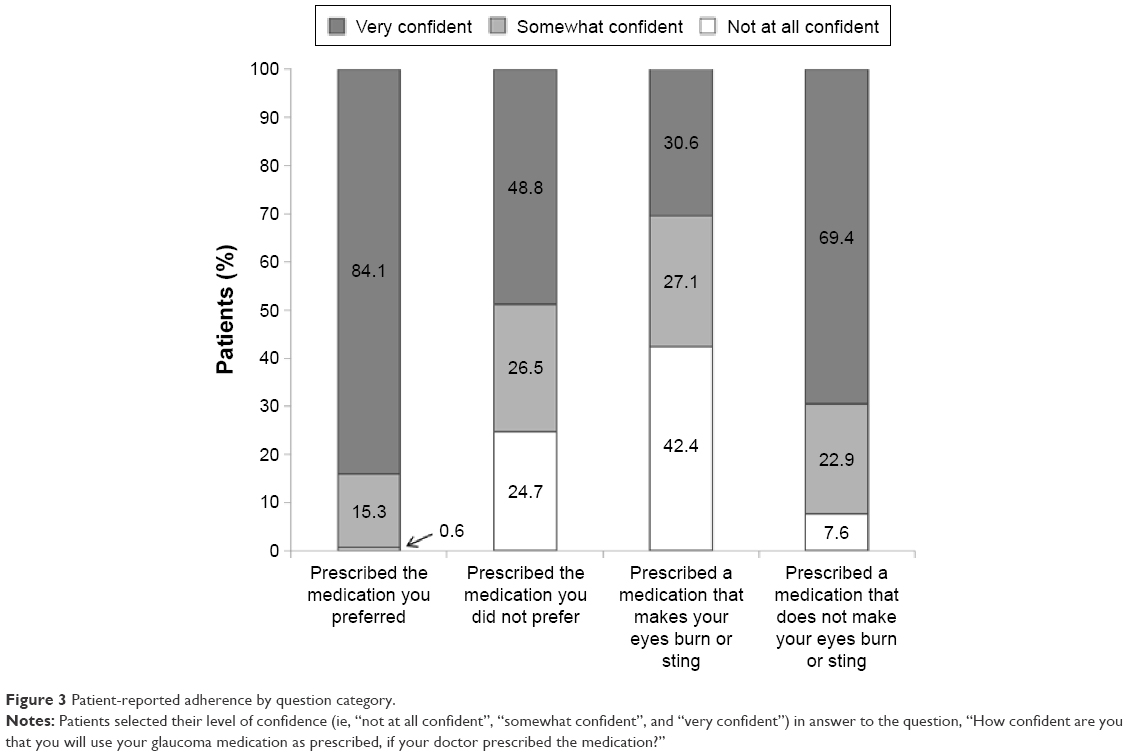 | Figure 3 Patient-reported adherence by question category. |
Ten patients discontinued BAK-free travoprost preserved with polyquaternium-1 because of 15 AEs (eye irritation, n=3; eye pruritus, n=2; and eye pain, photophobia, blurred vision, reduced visual acuity, conjunctivitis, eczema around the eye, foreign body sensation, headache, migraine, and dyspnea, n=1 each). Serious AEs were reported in four patients (upper gastrointestinal hemorrhage, n=1; cholelithiasis, n=1; and respiratory infection, n=2); all were considered unrelated to BAK-free travoprost. Throughout the study, 50 patients reported 73 treatment-emergent AEs, most of which were reported by <2% of patients (Table 2). Approximately, all of these were mild to moderate in severity (98.6%; n=72/73), and most were considered by the investigators to be unrelated to the study medication (58.9%; n=43/73). A majority of treatment-related AEs were eye disorders (86.7%; n=26/30).
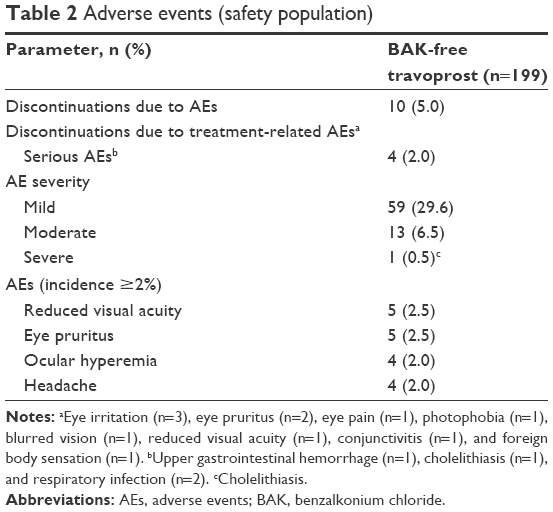 | Table 2 Adverse events (safety population) |
Discussion
AEs associated with few topical glaucoma medications may limit their use and necessitate switching to more tolerable medications.26–29 Switching from BAK-preserved latanoprost or bimatoprost to BAK-free, polyquaternium-1-preserved travoprost 0.004% provided additional IOP reductions after 6 weeks of treatment that were maintained for up to 12 weeks. The severity of ocular surface disease was reduced 12 weeks after the transition to BAK-free travoprost. At the end of the study, more patients preferred BAK-free travoprost when asked to select between BAK-free travoprost and BAK-containing latanoprost or bimatoprost. BAK-free travoprost was associated with mild-to-moderate AEs and was generally well tolerated.
Preservatives such as BAK that are commonly used in ophthalmic solutions are associated with burning, stinging, and dry eye and may increase the frequency of punctate keratitis.18–20,30–33 Furthermore, increased time of BAK exposure has been associated with a greater incidence of ocular surface disease,33 suggesting that patients with glaucoma or elevated IOP controlled with a BAK-preserved, IOP-lowering medication may require a therapy switch over time because of BAK-related tolerability concerns.
Persistence and adherence to topical IOP-lowering regimens are low,28 in part because of medication-related side effects;26,27,29 thus, improvements in ocular surface symptoms may have a beneficial effect on patients’ willingness to take their medication. Indeed, in the present study, more patients preferred BAK-free travoprost over their previous medication and felt very confident that they would adhere to their treatment if prescribed their preferred medication or a medication that did not elicit ocular symptoms.
Switching to polyquaternium-1-preserved travoprost was associated with IOP reductions from baseline of ~1 mmHg, indicating that it had IOP-lowering efficacy similar to that of the previous treatments of latanoprost or bimatoprost. However, the travoprost formulation maintained IOP reductions while removing the deleterious effects of BAK.
Interpretation of these results is limited by the open-label, single-group study design. Patients may have been more likely to report symptom improvement after transition to BAK-free travoprost preserved with polyquaternium-1 because they anticipated transition to a more tolerable medication. In addition, direct comparison between bimatoprost and latanoprost is not possible because of the forced switch aspect of the study. Finally, the 12-week duration of the study limits long-term efficacy or tolerability extrapolation.
Conclusion
European patients with open-angle glaucoma or ocular hypertension who were switched from BAK-preserved latanoprost or bimatoprost to BAK-free travoprost preserved with polyquaternium-1 because of tolerability concerns experienced additional reductions in IOP and improved ocular symptoms after the switch. Furthermore, when deciding between BAK-free travoprost or BAK-containing latanoprost or bimatoprost, a greater proportion of patients favored BAK-free travoprost preserved with polyquaternium-1.
Acknowledgments
This study was funded by Alcon Laboratories, Inc., and was presented in part at the European Glaucoma Society Annual Congress (June 7–11, 2014, Nice, France). The authors are grateful to all the investigators from the various study sites in Belgium, Spain, Italy, and Sweden. Medical writing support was provided by Jillian Gee, PhD, CMPP, and Heather D Starkey, PhD, of Complete Healthcare Communications, Inc. (Chadds Ford, PA, USA) and was funded by Alcon Laboratories, Inc.
Author contributions
All authors meet International Committee of Medical Journal Editors criteria for authorship of this article. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
JG-F has received honoraria and lecture fees from Alcon Laboratories, Inc., Merck, Sharp, & Dohme, Bausch & Lomb, and Novartis and grant support from Alcon Laboratories, Inc., Allergan, Inc., Sylentis, Pfizer, and Merck, Sharp, & Dohme. DAH is an Alcon Laboratories, Inc., employee. The authors report no other conflicts of interest in this work.
References
Casson RJ, Chidlow G, Wood JP, Crowston JG, Goldberg I. Definition of glaucoma: clinical and experimental concepts. Clin Experiment Ophthalmol. 2012;40:341–349. | ||
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. | ||
Collaborative Normal-Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Am J Ophthalmol. 1998;126:487–497. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–713. | ||
The Advanced Glaucoma Intervention Study (AGIS) 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130:429–440. | ||
European Glaucoma Society. Terminology and Guidelines for Glaucoma. 3rd ed. Savona, Italy: Dogma S.r.l.; 2008. | ||
Toris CB, Zhan G, Fan S, et al. Effects of travoprost on aqueous humor dynamics in patients with elevated intraocular pressure. J Glaucoma. 2007;16:189–195. | ||
Lin L, Zhao YJ, Chew PT, et al. Comparative efficacy and tolerability of topical prostaglandin analogues for primary open-angle glaucoma and ocular hypertension. Ann Pharmacother. 2014;48:1585–1593. | ||
Webers CA, Beckers HJ, Nuijts RM, Schouten JS. Pharmacological management of primary open-angle glaucoma: second-line options and beyond. Drugs Aging. 2008;25:729–759. | ||
Li N, Chen XM, Zhou Y, Wei ML, Yao X. Travoprost compared with other prostaglandin analogues or timolol in patients with open-angle glaucoma or ocular hypertension: meta-analysis of randomized controlled trials. Clin Experiment Ophthalmol. 2006;34:755–764. | ||
van der Valk R, Webers CA, Schouten JS, Zeegers MP, Hendrikse F, Prins MH. Intraocular pressure-lowering effects of all commonly used glaucoma drugs: a meta-analysis of randomized clinical trials. Ophthalmology. 2005;112:1177–1185. | ||
Zhang WY, Po AL, Dua HS, Azuara-Blanco A. Meta-analysis of randomised controlled trials comparing latanoprost with timolol in the treatment of patients with open angle glaucoma or ocular hypertension. Br J Ophthalmol. 2001;85:983–990. | ||
Whitcup SM, Cantor LB, VanDenburgh AM, Chen K. A randomised, double masked, multicentre clinical trial comparing bimatoprost and timolol for the treatment of glaucoma and ocular hypertension. Br J Ophthalmol. 2003;87:57–62. | ||
Parrish RK, Palmberg P, Sheu WP; Group XLTS. A comparison of latanoprost, bimatoprost, and travoprost in patients with elevated intraocular pressure: a 12-week, randomized, masked-evaluator multicenter study. Am J Ophthalmol. 2003;135:688–703. | ||
Dubiner HB, Noecker R. Sustained intraocular pressure reduction throughout the day with travoprost ophthalmic solution 0.004%. Clin Ophthalmol. 2012;6:525–531. | ||
Garcia-Feijoo J, Martinez-de-la-Casa JM, Castillo A, Mendez C, Fernandez-Vidal A, Garcia-Sanchez J. Circadian IOP-lowering efficacy of travoprost 0.004% ophthalmic solution compared to latanoprost 0.005%. Curr Med Res Opin. 2006;22:1689–1697. | ||
Aptel F, Cucherat M, Denis P. Efficacy and tolerability of prostaglandin analogs: a meta-analysis of randomized controlled clinical trials. J Glaucoma. 2008;17:667–673. | ||
Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17:341–349. | ||
Kuppens EV, de Jong CA, Stolwijk TR, de Keizer RJ, van Best JA. Effect of timolol with and without preservative on the basal tear turnover in glaucoma. Br J Ophthalmol. 1995;79:339–342. | ||
Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86:418–423. | ||
Ammar DA, Kahook MY. Effects of benzalkonium chloride- or polyquad-preserved fixed combination glaucoma medications on human trabecular meshwork cells. Mol Vis. 2011;17:1806–1813. | ||
Ammar DA, Noecker RJ, Kahook MY. Effects of benzalkonium chloride- and polyquad-preserved combination glaucoma medications on cultured human ocular surface cells. Adv Ther. 2011;28:501–510. | ||
Liang H, Brignole-Baudouin F, Pauly A, Riancho L, Baudouin C. Polyquad-preserved travoprost/timolol, benzalkonium chloride (BAK)-preserved travoprost/timolol, and latanoprost/timolol in fixed combinations: a rabbit ocular surface study. Adv Ther. 2011;28:311–325. | ||
Baudouin C, Labbe A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29:312–334. | ||
Lewis RA, Katz GJ, Weiss MJ, et al. Travoprost 0.004% with and without benzalkonium chloride: a comparison of safety and efficacy. J Glaucoma. 2007;16:98–103. | ||
Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the Glaucoma Adherence and Persistency Study. Ophthalmology. 2008;115:1320–1327. | ||
Kholdebarin R, Campbell RJ, Jin YP, Buys YM. Multicenter study of compliance and drop administration in glaucoma. Can J Ophthalmol. 2008;43:454–461. | ||
Reardon G, Kotak S, Schwartz GF. Objective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: a systematic review. Patient Prefer Adherence. 2011;5:441–463. | ||
Zimmerman TJ, Hahn SR, Gelb L, Tan H, Kim EE. The impact of ocular adverse effects in patients treated with topical prostaglandin analogs: changes in prescription patterns and patient persistence. J Ocul Pharmacol Ther. 2009;25:145–152. | ||
Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29:618–621. | ||
Ghosh S, O’Hare F, Lamoureux E, Vajpayee RB, Crowston JG. Prevalence of signs and symptoms of ocular surface disease in individuals treated and not treated with glaucoma medication. Clin Experiment Ophthalmol. 2012;40:675–681. | ||
Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17:350–355. | ||
Rossi GC, Pasinetti GM, Scudeller L, Bianchi PE. Ocular surface disease and glaucoma: how to evaluate impact on quality of life. J Ocul Pharmacol Ther. 2013;29:390–394. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.