")
Back to Journals » OncoTargets and Therapy » Volume 11
Efficacy and safety of weekly nab-paclitaxel plus cisplatin with concurrent intensity-modulated radiotherapy in patients with inoperable, locally advanced esophageal cancer: a pilot trial
Authors Wang D, Zhang W, Qian D, Guan Y, Chen X, Zhang H, Wang J, Pang Q
Received 15 March 2018
Accepted for publication 21 June 2018
Published 28 September 2018 Volume 2018:11 Pages 6333—6338
DOI https://doi.org/10.2147/OTT.S168275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Daquan Wang,* Wencheng Zhang,* Dong Qian, Yong Guan, Xi Chen, Hualei Zhang, Jun Wang, Qingsong Pang
Department of Radiation Oncology, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin 300060, China
*These authors contributed equally to this work
Background: Nab-paclitaxel is produced by the combination of paclitaxel particles with human serum albumin. Encouraging efficacy has been observed with nab-paclitaxel-based chemotherapy in a variety of solid tumors. The aim of the study reported here was to evaluate the efficacy and safety of weekly nab-paclitaxel plus cisplatin with concurrent intensity-modulated radiotherapy in patients with locally advanced esophageal cancer.
Methods: Seventeen patients with esophageal cancer were enrolled between July 2014 and December 2015.The treatment included radical radiotherapy (95% planning target volume 60Gy/30f) and concurrent chemotherapy comprising nab-paclitaxel 60mg/m2/week plus cisplatin 25mg/m2/week, administered on days 1, 8, 15, and 22 of each 28-day cycle. The end point of this study included objective response rate (ORR), local-recurrence free survival (LRFS), distant metastasis-free survival (DMFS), progression-free survival (PFS), and overall survival (OS).
Results: All the patients enrolled in the trial had squamous cell carcinoma. The median follow-up duration was 20.47 months. The ORR was 88.2%. LRFS, DMFS, PFS and OS at 3 years were 61%, 40%, 17% and 35%, respectively. The trial regimen was well tolerated, with grade 3–4 myelosupression, grade 3 radioactive esophagitis, and grade 3 radiation pneumonitis rates of 17.6%, 17.6%, and 11.8%, respectively.
Conclusion: Weekly nab-paclitaxel plus cisplatin with concurrent intensity-modulated radiotherapy is an effective and well-tolerated treatment option for inoperable, locally advanced squamous cancer of esophageal.
Keywords: nab-paclitaxel, esophageal cancer, squamous cell carcinoma
Introduction
Since the publication of long-term follow-up data from the landmark RTOG 8501 clinical trial, PF-based chemoradiotherapy has become established as the standard treatment for inoperable, locally advanced esophageal carcinoma.1 A number of recent studies have explored the application of taxane-based chemoradiotherapy in this indication, and have shown that platinum/paclitaxel combinations offer improved response rates and clinical efficacy vs PF-based regimens.2–4 However, traditional solvent-based paclitaxel is associated with adverse events such as hypersensitivity, neurotoxicity, and myelosuppression, necessitating prophylactic pretreatment with antihistamines or steroids. Nab-paclitaxel is a novel, albumin-bound, hypoallergenic paclitaxel formulation that, compared with traditional solvent-based paclitaxel, demonstrates reduced toxicity and improved tolerability.5 Animal xenograft studies indicate that nab-paclitaxel is more rapidly distributed to tumor tissue,6 and clinical trials in breast and non-small-cell lung cancer have demonstrated increased ORRs in patients treated with nab-paclitaxel/platinum vs solvent-based paclitaxel/platinum.7–10
A recent Phase II clinical trial in locally advanced esophageal cancer reported R0 resection, pathologic complete response, and pathologic downstaging rates of 100%, 13.3%, and 63.3%, respectively, with acceptable tolerability, in patients treated with concurrent nab-paclitaxel plus cisplatin chemotherapy followed by surgery.11 However, little is known about the efficacy of nab-paclitaxel-based chemoradiotherapy in this indication. The present clinical trial was therefore designed to evaluate the efficacy and safety of nab-paclitaxel plus cisplatin administered concurrently with radiotherapy in Chinese patients with inoperable, locally advanced esophageal cancer.
Materials and methods
Patients
Eligible patients were adults aged ≤75 years with: pathologically confirmed, inoperable, locally advanced esophageal cancer (T3N0M0–TxNxM1a) (American Joint Committee on Cancer staging, sixth edition) or cervical esophageal cancer; one or more measurable lesion; Eastern Cooperative Oncology Group performance status 0–1; white blood cell count ≥3,500 mm3; absolute neutrophil count ≥1,500 mm3; platelet count ≥100,000 mm3; hemoglobin concentration ≥90 g/L; serum bilirubin level <1.5 of the ULN for the institution; alanine aminotransferase and aspartate aminotransferase levels ≤2.5 ULN; serum albumin ≥30 g/L; serum creatinine ≤1.5 ULN; and normal cardiac function with no severe heart disease. Exclusion criteria included: history of esophagectomy; pregnancy or breast feeding; past history of other cancers except for cured non-melanoma skin cancer or cervical cancer; expected inability to complete the study or life expectancy <3 months; current participation in any other clinical trial in esophageal cancer; and any other conditions considered by the monitors or auditors to be abnormal.
All patients provided written informed consent. All procedures were conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines, and local regulatory requirements. The trial protocol was approved by the ethics committee of Tianjin Medical University Cancer Institute and Hospital (approval number E2014067).
Assessment
All the patients were evaluated before treatment by the following: physical examination, upper digestive endoscopy, endoscopic ultrasonography, cervical/abdominal ultrasound, upper gastrointestinal radiography, and chest/abdominal CT scan. Positron emission tomography–CT scan was not essential. Tumor response were assessed using chest/abdominal CT scan, upper gastrointestinal radiography, and cervical/abdominal ultrasound.
Treatments
Nab-paclitaxel 60 mg/m2/week and cisplatin 25 mg/m2/week with concurrent radiotherapy were administered on days 1, 8, 15, and 22 of a 28-day cycle. Two cycles of consolidate chemotherapy (nab-paclitaxel 175 mg/m2/d1 and cisplatin 75 mg/m2/d2 of each 21-day cycle) were administered 4 weeks after radiotherapy. Contrast-enhanced CT scans were used to improve the accuracy of radiotherapy dose distribution where possible; plain scans were carried out in patients who were sensitive to the contrast agent or had other complications. A head–neck–shoulder net or chest net was used to immobilize patients in the supine position for CT simulation. The scan range extended from the laryngeal prominence to the inferior margin of the first lumbar vertebra.
Radiotherapy was performed using a 6 MV linear accelerator. The PTV prescription dose (95% PTV) was 60 Gy/30 f, and the fractional dose was 2 Gy delivered once daily, 5 days per week. Maximal doses for normal organs were 45 Gy for the spinal cord and 18 Gy for bilateral lungs. The mean lung dose (bilateral) was ≤18 Gy. The volume of organ receiving n% dose of Gy (Vn) was: bilateral lung V20 <28% and V30 <20%; heart V30 <40% and V40 <30%.
GTV was determined based on the results of upper gastrointestinal radiography, esophageal endoscopy, and chest CT. If lymphatic metastasis was present in the mediastinum, supraclavicular region, or abdominal cavity, GTV in involved lymph nodes (GTVnd) was delineated. The CTV was delineated as GTV and GTVnd plus: 3–5 cm margins in the vertical direction, which covered the corresponding lymphatic drainage areas; and 0.6–0.8 cm margins in the anteroposterior and transverse directions, which did not exceed the anatomic boundary. PTV was defined as CTV plus 5 mm margins.
Trial end points
The primary trial end point was the ORR, LRFS, DMFS, and PFS. Secondary end points included OS and therapy-related adverse reactions. The ORR was based on Response Evaluation Criteria in Solid Tumors version 1.1.12 Acute adverse reactions were evaluated according to Common Terminology Criteria for Adverse Events version 3.0.13 LRFS was defined as the length of time from the start of treatment until disease recurrence of primary lesion(s) (in the mediastinal region and/or cervical lymphatic drainage area); DMFS was defined as the length of time from the start of treatment until tumor progression excluding local failure; PFS was defined as the length of time from the start of treatment until disease progression/recurrence, death from any cause, or the last follow-up visit; OS was defined as the length of time from the start of treatment until death from any cause, censoring, or the last follow-up visit.
Follow-up
The initial follow-up visit was scheduled 2–3 months after the end of treatment, with subsequent follow-up visits taking place every 3 months during the first year. Thereafter, if disease remained stable, patients were followed up once every 6 months for 3 years, and subsequently once every year. The follow-up schedule was designed to detect any delayed side effects, and to establish final treatment outcomes. Follow-up evaluations included an assessment of signs and symptoms, Karnofsky Performance Scale score, routine blood tests, tumor markers, and imaging examinations, such as abdominal ultrasound, upper gastrointestinal radiography, and chest CT.
Statistical methods
SPSS version 22.0 (IBM, Armonk, NY, USA) was used for statistical analysis. The LRFS, DMFS, PFS, and OS were estimated using Kaplan–Meier methodology.
Results
In total, 17 patients were enrolled in the trial between July 2014 and December 2015. Baseline demographics and clinical characteristics of the trial population are summarized in Table 1. Patients’ median age was 60 years (range 36–70 years), 16 of the 17 patients were male, all the patients had squamous cell carcinoma, and 12 patients (70.6%) had stage III disease. Physical parameters related to lesions of the patients are summarized in Table 2. All the patients finished the course of chemoradiotherapy. Fourteen patients finished two cycles of consolidative chemotherapy, while three patients did one. At the data cutoff point (January 28, 2018), the median length of follow-up was 20.47 months.
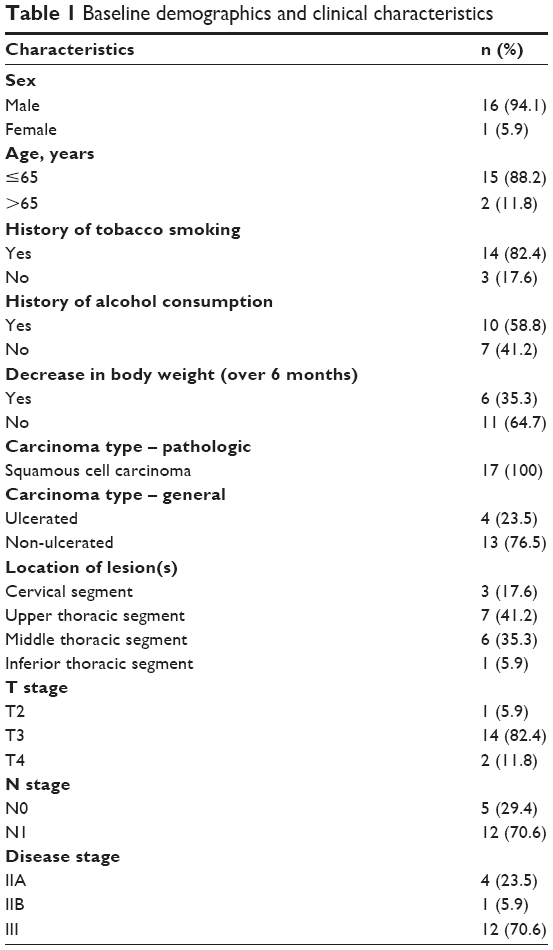 | Table 1 Baseline demographics and clinical characteristics |
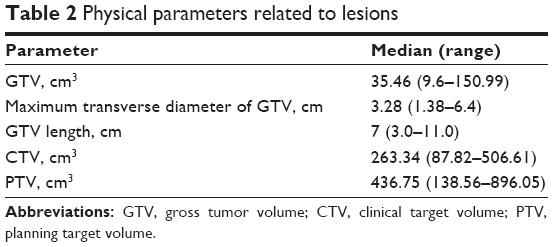 | Table 2 Physical parameters related to lesions |
The ORR 2–3 months after treatment initiation was 88.2% (15 patients), with complete response and partial response rates of 17.6% (three patients) and 70.6% (12 patients), respectively. OS at 1, 2, and 3 years was 71%, 47%, and 35%, respectively. PFS at 1, 2, and 3 years was 59%, 24%, and 17%, respectively. Median PFS and median OS were 13.5 months (95% CI 8.051–20.861) and 22.5 months (95% CI 18.176–32.864), respectively (Figure 1).
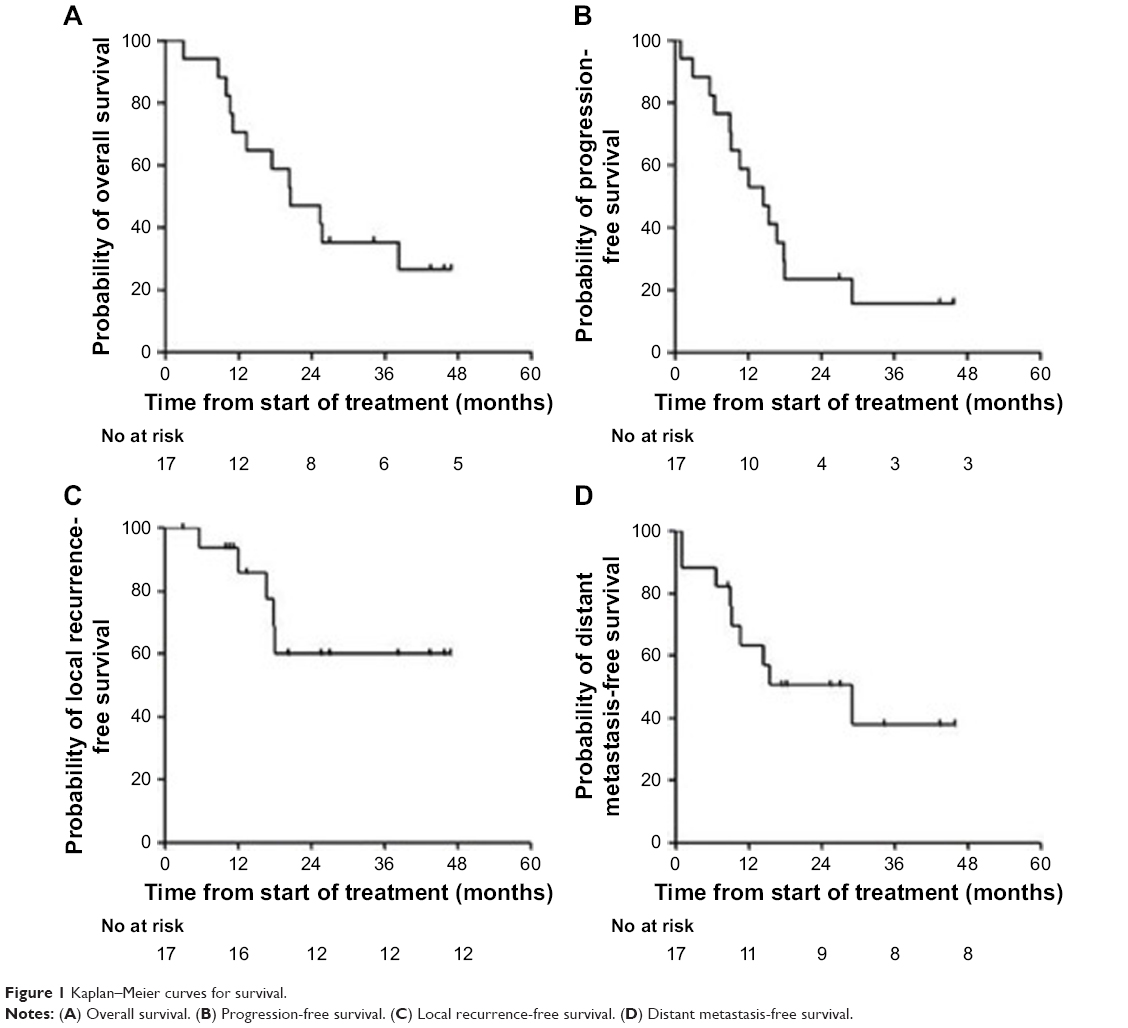 | Figure 1 Kaplan–Meier curves for survival. |
Of the 17 patients, 14 (82.4%) had disease recurrence, 5 (29.4%) had local recurrence, and 9 (52.9%) had distant metastasis. LRFS and DMFS at 1, 2, and 3 years were 94%, 61%, and 61% and 64%, 50%, and 40%, respectively (Figure 1).
Adverse reactions included mainly hematologic events, radiation esophagitis, and radiation pneumonitis (Table 3). One patient was hospitalized and isolated because of developing grade 4 leukopenia during treatment.
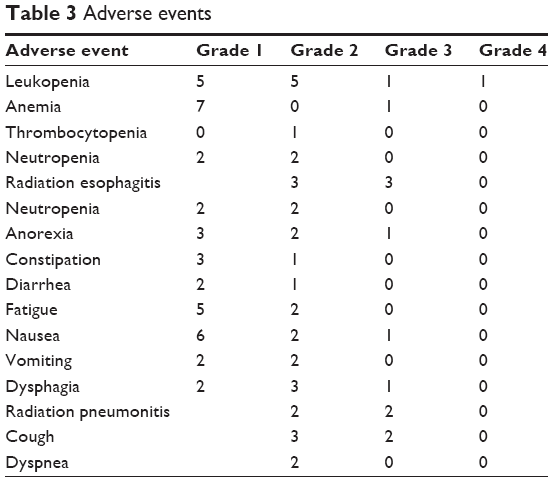 | Table 3 Adverse events |
Discussion
Nab-paclitaxel is produced by the combination of paclitaxel particles with human serum albumin. As nab-paclitaxel contains no polyoxyethylene castor oil or ethanol, allergic reactions and neurotoxicity are greatly reduced in comparison with solvent-based paclitaxel.5 Encouraging efficacy has been observed with nab-paclitaxel-based chemotherapy in a variety of solid tumors, including breast cancer, non-small-cell lung cancer, pancreatic cancer, and head and neck squamous cell carcinoma.5,7,9,14 Several studies have also explored the efficiency of the regimens in esophageal cancer. In a clinical trial reported by Fan et al, in which 77.1% of the population had stage III esophageal cancer, the ORR for all patients who received two cycles of nab-paclitaxel plus cisplatin chemotherapy was 65.7%.11 Similarly, in a study of 33 patients with recurrence or metastasis of advanced esophageal cancer, a radiographic response was observed in 60.6% of those who received two to six cycles of nab-paclitaxel plus cisplatin.15 Previous studies have also shown that paclitaxel-based chemoradiotherapy for esophageal cancer leads to ORRs of 50%–73%.16,17 Our trial indicated that nab-paclitaxel-based chemoradiotherapy leads to a superior ORR of 88.2%, which is encouraging.
The RTOG 8501 and RTOG 9405 clinical trials established PF-based chemoradiotherapy as the standard treatment for esophageal cancer.1,18 More recent trials have reported 2-year OS rates of 32%–46% in patients treated with PF-based chemoradiotherapy.18–21 In our trial, 2-year OS and median OS were 47% and 22.5 months, which are satisfying. A number of clinical trials indicated that docetaxel-based chemoradiotherapy may bring more toxicities than PF-based regimens. In a randomized trial by Zhao et al, grade 3–4 hematologic toxicities were observed in 35.6% in the docetaxel group.17 Notably, in our trial, only 17.6% (three of 17) of patients developed grade 3–4 hematologic toxicities, and no incidences of grade 4 radioactive esophagitis or pneumonitis were observed. Furthermore, although none of the patients received anti-allergic pretreatment prior to nab-paclitaxel administration, no allergic reactions occurred during treatment, demonstrating the favorable tolerability of this formulation.
FFCD 9102 trial included 130 patients with esophageal squamous cell carcinoma treated by chemoradiotherapy, and the local control rate was 57% at 2 years.20 We observed an LRFS of 61% at 2 years, which was similar to that in FFCD 9102 trial. However, it is a remarkable fact that patients in our trial were in a more advanced stage than those in FFCD 9102 trial (stage N1: 70.6% vs 40%). We applied relatively high dose of nab-paclitaxel (60 mg/m2) in the trial, which may have contributed to better local control.
Our trial provides the first evidence that nab-paclitaxel-based chemoradiotherapy is effective and safe for esophageal cancer. In consideration of nab-paclitaxel’s low toxicities, more patients might be able to finish the course of chemoradiotherapy. However, there are limitations that must be considered. First, only 17 patients were enrolled in the trial; hence, future study in larger populations is needed. Second, long-term efficiency was not observed because of short follow-up time. Of note, all the patients in our trial had squamous cell carcinoma; therefore, the conclusion is only applicable to esophageal squamous cell carcinoma.
In conclusion, our findings suggest that weekly nab-paclitaxel plus cisplatin concurrent with radiotherapy brings satisfied outcome among patients with inoperable, locally advanced esophageal squamous cell carcinoma. Future prospective studies are needed to confirm these results.
Abbreviations
CT, computed tomography; CTV, clinical target volume; DMFS, distant metastasis-free survival; GTV, gross tumor volume; LRFS, local recurrence-free survival; ORR, objective response rate; OS, overall survival; PF, cisplatin plus 5-fluorouracil; PFS, progression-free survival; PTV, planning target volume; ULN, upper limit of normal.
Acknowledgments
Editorial assistance in the preparation of this manuscript was provided by the Investigator Initiated Research Writing Group (an initiative from Ashfield Healthcare Communications, part of UDG Healthcare plc), and was funded by Celgene Corporation. No specific funding was received for this study, and Celgene Corporation only provided funding for editorial assistance in the preparation of this manuscript, not for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281(17):1623–1627. | ||
Song T, Zhang X, Fang M, Wu S. Concurrent chemoradiotherapy using paclitaxel plus cisplatin in the treatment of elderly patients with esophageal cancer. Onco Targets Ther. 2015;8:3087–3094. | ||
Honing J, Smit JK, Muijs CT, et al. A comparison of carboplatin and paclitaxel with cisplatinum and 5-fluorouracil in definitive chemoradiation in esophageal cancer patients. Ann Oncol. 2014;25(3):638–643. | ||
Zhao C, Lin L, Liu J, et al. A phase II study of concurrent chemoradiotherapy and erlotinib for inoperable esophageal squamous cell carcinoma. Oncotarget. 2016;7(35):57310–57316. | ||
Loong HH, Chan AC, Wong AC. Evolving Evidence of the Efficacy and Safety of nab-Paclitaxel in the Treatment of Cancers with Squamous Histologies. J Cancer. 2016;7(3):268–275. | ||
Desai N, Trieu V, Yao Z, et al. Increased antitumor activity, intratumor paclitaxel concentrations, and endothelial cell transport of cremophor-free, albumin-bound paclitaxel, ABI-007, compared with cremophor-based paclitaxel. Clin Cancer Res. 2006;12(4):1317–1324. | ||
Gradishar WJ, Tjulandin S, Davidson N, et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J Clin Oncol. 2005;23(31):7794–7803. | ||
Untch M, Jackisch C, Schneeweiss A, et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trial. Lancet Oncol. 2016;17(3):345–356. | ||
Socinski MA, Bondarenko I, Karaseva NA, et al. Weekly nab-paclitaxel in combination with carboplatin versus solvent-based paclitaxel plus carboplatin as first-line therapy in patients with advanced non-small-cell lung cancer: final results of a phase III trial. J Clin Oncol. 2012;30(17):2055–2062. | ||
Socinski MA, Okamoto I, Hon JK, et al. Safety and efficacy analysis by histology of weekly nab-paclitaxel in combination with carboplatin as first-line therapy in patients with advanced non-small-cell lung cancer. Ann Oncol. 2013;24(9):2390–2396. | ||
Fan Y, Jiang Y, Zhou X, et al. Phase II study of neoadjuvant therapy with nab-paclitaxel and cisplatin followed by surgery in patients with locally advanced esophageal squamous cell carcinoma. Oncotarget. 2016;7(31):50624–50634. | ||
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. | ||
Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol. 2003;13(3):176–181. | ||
von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. | ||
Shi Y, Qin R, Wang ZK, Dai GH. Nanoparticle albumin-bound paclitaxel combined with cisplatin as the first-line treatment for metastatic esophageal squamous cell carcinoma. Onco Targets Ther. 2013;6:585–591. | ||
Day FL, Leong T, Ngan S, et al. Phase I trial of docetaxel, cisplatin and concurrent radical radiotherapy in locally advanced oesophageal cancer. Br J Cancer. 2011;104(2):265–271. | ||
Zhao T, Chen H, Zhang T. Docetaxel and cisplatin concurrent with radiotherapy versus 5-fluorouracil and cisplatin concurrent with radiotherapy in treatment for locally advanced oesophageal squamous cell carcinoma: a randomized clinical study. Med Oncol. 2012;29(5):3017–3023. | ||
Minsky BD, Pajak TF, Ginsberg RJ, et al. INT 0123 (Radiation Therapy Oncology Group 94-05) phase III trial of combined-modality therapy for esophageal cancer: high-dose versus standard-dose radiation therapy. J Clin Oncol. 2002;20(5):1167–1174. | ||
Ishida K, Ando N, Yamamoto S, Ide H, Shinoda M. Phase II study of cisplatin and 5-fluorouracil with concurrent radiotherapy in advanced squamous cell carcinoma of the esophagus: a Japan Esophageal Oncology Group (JEOG)/Japan Clinical Oncology Group trial (JCOG9516). Jpn J Clin Oncol. 2004;34(10):615–619. | ||
Bedenne L, Michel P, Bouché O, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007;25(10):1160–1168. | ||
Nishimura Y, Hiraoka M, Koike R, et al. Long-term follow-up of a randomized Phase II study of cisplatin/5-FU concurrent chemoradiotherapy for esophageal cancer (KROSG0101/JROSG021). Jpn J Clin Oncol. 2012;42(9):807–812. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.