")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Efficacy and Safety of Rituximab Therapy for Lupus Nephritis Among SLE Female Patients; a Retrospective Hospital-Based Study
Authors Abdelkarim Aloub KO, Eltahirm NIA, Elagib EM, Adam Essa ME , Hussein MMA
Received 24 September 2022
Accepted for publication 6 December 2022
Published 13 December 2022 Volume 2022:14 Pages 301—308
DOI https://doi.org/10.2147/OARRR.S391091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Khansa Osama Abdelkarim Aloub,1 Noha Ibrahim Ahmed Eltahirm,1,2 Elnour Mohammed Elagib,1,2 Mohammed Elmujtba Adam Essa,3,4 Mustafa Mohammed Ali Hussein3,4
1Department of Internal Medicine and Rheumatology, Omdurman Military Hospital, Omdurman, Sudan; 2Department of Medicine, Faculty of Medicine, Karary University, Omdurman, Sudan; 3Department of Clinical Medicine, Medical and Cancer Research Institute, Nyala, Sudan; 4Faculty of Medicine, Al fashir University, Al Fashir, Sudan
Correspondence: Mohammed Elmujtba Adam Essa, Department of Clinical Medicine, Medical and Cancer Research Institute, Nyala, Sudan, Tel +24990700938, Email [email protected]
Background: Renal affection in systemic lupus erythematosus (SLE) is a high-risk manifestation in which novel treatment strategies are required, particularly in patients who show lower response to conventional therapy. Rituximab has been used as an off-label treatment for lupus nephritis (LN) for the last ten years. This study aims to assess the outcome of the use of rituximab to treat LN patients.
Methods: A retrospective cross-sectional study included 40 LN patients on Rituximab therapy who attended the Rheumatology clinic at Omdurman Military Hospital, Khartoum, Sudan. Between January to July 2020. Data were collected from the hospital records and included demographic, duration of disease and Rituximab doses. Renal biopsy, renal function parameters, albumin-creatinine ratio, hematological parameters and inflammatory markers. Assessment of the outcomes was conducted by the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI score). Data were analyzed by using Statistical Package for Social Studies Program (SPSS, V. 21.0. IBM; Chicago). Chi-square test was used as significance test, the P. value was considered as significant at level 0.05 and akk continues variables had a normal distribution with Kolmogorov–Smirnov test.
Results: Renal function test showed significant improvement after 6 months of treatment with Rituximab. In addition, the mean of the SLE Activity Index 2000 (SLEDAI 2K) was significantly decreased with remarkable improvement in the histological degree of LN. The histology of renal biopsy of the patients commonly was diffuse proliferative nephritis followed by minimal mesangial glomerulonephritis, mesangial proliferative LN then membranous nephritis respectively. Improvement was common among the patients aged 20– 39 years, those with disease duration less than 5 years, who received 4 doses and rituximab as the initial modality.
Conclusion: Rituximab therapy is effectively managing patients with lupus nephritis, after 6 months of follow-up, Patients showed remarkable clinical and laboratory improvement.
Keywords: rituximab, LN, SLE, conventional therapy
Introduction
SLE is a chronic multisystem autoimmune disease that is highly heterogeneous in its presentation. It causes various symptoms and signs, which makes it a challenging condition for clinical diagnosis and treatment, affecting both female-to-males with a ratio of 8–9:1.1,2 New insight into immunopathogenesis provides theories for developing potential clinical biomarkers and therapeutic targets of SLE.3 One of its most severe manifestations is lupus nephritis (LN) which is associated with increased morbidity and mortality.4
Different pathophysiological mechanisms have been involved in the development of LN in SLE patients.5 A combination of genetic, environmental and immunological factors mediates the processes that result in renal damage.6 Of special importance for the present review is the role of the B cells, which are hyperactive in SLE. The B cells mediate and regulate antibody production, interact with memory T cells and stimulate pro-inflammatory cytokine production, all of which make them essential components of the pathophysiology of LN.7 It is for these reasons that the use of rituximab is proposed. This monoclonal antibody is directed against CD20, an antigen expressed on the surface of mature and immature B cells. CD20 regulates the initiation of the cell cycle. The binding of the antibody to Fc receptor induces apoptosis and cytotoxicity, mediated by both complement and antibodies.8 LN is an immune complex glomerular nephritis that progresses as a result of recurrent complications of SLE.9 The pathophysiology of LN involves a variety of pathogenic mechanisms which are intrarenal and extrarenal pathogenic mechanisms.10 The extrarenal factors include complex combinations of genetic variants that are changed in each patient; this may clarify the variability of clinical manifestations.5
The use of biologic therapies as an adjunct to disease-modifying anti-rheumatic drugs (DMARDs) for the treatment of autoimmune and rheumatologic diseases is rapidly expanding, owing to the good efficacy and safety profiles of these drugs, and the better understanding of the initial targets of altered immune regulation and activity in various diseases.11 Although some of the biological therapies have been found to be useful in more than one disease, others are specific to a single disease. Research is ongoing to identify other molecular targets.12
The development of biological therapies has had an impact on the management of several medical conditions.13 Their use in systemic lupus erythematosus (SLE), however, remains very limited.14 The aim of the study is to assess the outcome of the use of rituximab to treat SLE patients with lupus nephritis.
Materials and Methods
Study Design
This is an analytical retrospective cross-sectional hospital-based study.
Study Area
The study was conducted at the department of rheumatology, Omdurman Military Hospital in Khartoum state, Sudan.
Study Population
SLE patients with LN attended the rheumatologic department of Omdurman Military Hospital and received Rituximab.
Sample Size Determination
Total coverage of all SLE patients with lupus Nephritis on Rituximab treatment during the study period is 40 patients who are treated at the department of rheumatology, Omdurman Military Hospital in Khartoum state, Sudan.
Data Collection Tools and Methods
Data collection is carried out by the principal investigator. After recruiting the study subjects, structured questionnaires will be used to collect data composed of; demographic, duration of the SLE and Rituximab doses (using Patients Hospital Records), and all the patients were treated according to the standard protocol treatment of SLE patients with LN (received 500 mg once/week for 1 month). Hematological parameters (hemoglobin, leucocyte and platelet counts) and inflammatory markers (ESR, CRP, C3 and C4) were compared at admission and after 6 months. Assessment of the outcomes was being measured through the parameters of renal function test (urea, creatinine, albumin-creatinine ratio) and urine dipstick (for proteinuria) in addition to the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI score). Screening for tuberculosis, hepatitis and HIV was performed on all the patients before treatment with rituximab as most of the patients were been treated by MMF or CNI but they have not shown any improvement, so we shifted to rituximab. Regarding the adverse side effect of rituximab no patients report any side effect during the follow up of the treatment.
Study Variables
Independent variables (Socio-demographic characteristics of participants, age, gender, duration of disease, number of Rituximab doses of Hematological parameters (hemoglobin, leucocyte and platelet counts), renal function (urea, creatinine, albumin-creatinine ratio) and proteinuria), inflammatory markers (ESR, CRP, C3 and C4), dependent variables (Rituximab outcome by SLEDAI-2K Score for SLE patients).
Data Analysis
Data were analyzed by using Statistical Package for Social Studies Program (SPSS, V. 21.0. IBM; Chicago). Chi-square test was used as significance test, P value was considered as significant at level 0.05 and akk continues variables had a normal distribution with Kolmogorov–Smirnov test.
Ethical Consideration
Ethical approval was obtained from Sudan medical specialization board (SMSB). Written informed consent was obtained from patients.
Results
The mean SLE Activity Index 2000 (SLEDAI 2K) was significantly decreased after 6 months of rituximab use (34.5±13.7 vs 12.3±16.1; P. value = 0.000) with mean difference = −22.2 (Figure 1). In addition to improvement (complete and partial) presented in 36 (90%) patients, deterioration in 2 (5%) and not responding in 2 (5%) patients. Improvement was common among the patients aged 20–39 years more than others (P. value = 0.000) and also higher among those with disease duration less than 5 years more than others (P. value = 0.01). The mean disease duration was found to be 5.8±4 years and one-half (n = 20; 50%) had a duration of fewer than 5 years (Table 1).
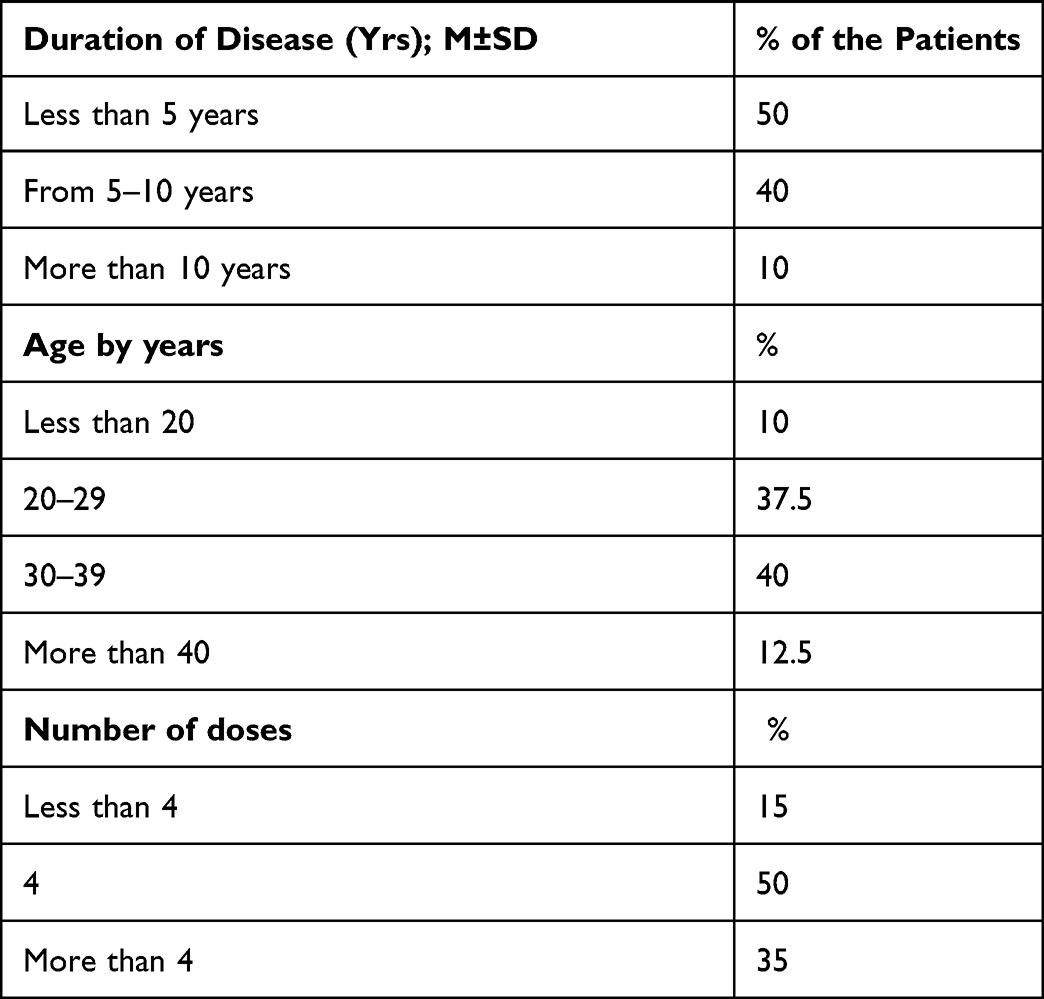 |
Table 1 Shows the Age Distributions, Number of Rituximab Doses and the Disease Duration of SLE Patients with Lupus Nephritis on Rituximab Treatment (N = 40) |
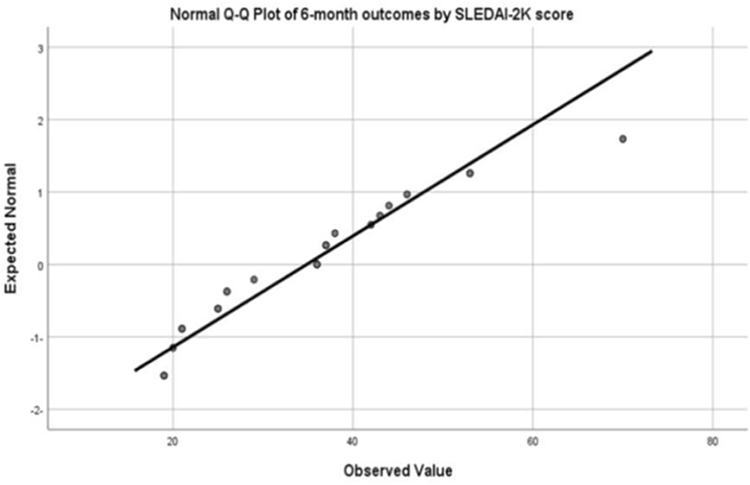 |
Figure 1 Shows the distribution Q-Q of 6 months outcome by SLEDAI-2K score. |
The patients who received 4 doses and rituximab as initial modality shows better response than others (P. value = 0.036) (Figure 2), the number of Rituximab doses was less than 4 doses in 6 (15%) patients, 4 doses in 20 (50%) and more than 4 doses in 14 (35%) patients (Table 1).
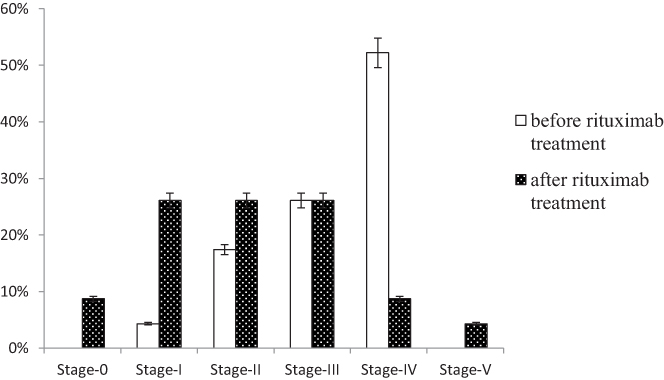 |
Figure 2 Shows the scores of SLE Disease Activity Index 2000 (SLEDAI 2K) before and after Rituximab treatment (N=40). |
In general, the study included a total of 40 female SLE patients with LN on Rituximab treatment, their mean age was 34.9±8 years and the majority of them 16 (40%) belonged to the age group from 30 to 39 years (Table 1). The hematological parameter of the study group showed that there was a significant rising in hemoglobin (9.9±2.7 vs; 11.4±1.6 P. value = 0.000) and platelets count (220.5±143.4220.5±143.4 vs 265±103; P. value = 0.001) after 6 months of Rituximab use.
In inflammatory investigations, CRP (13.4±7.5 vs 2.1±1.7; P. value = 0.000) and ESR (72.3±35 vs 39.3±4.5; P. value = 0.000) were significantly decreased after 6 months of Rituximab use. Also, the levels of C3 levels (40% vs 75%; P. value = 0.002) and C4 levels (74.5% vs 80%; P. value = 0.000) were significantly increased after 6 months of Rituximab use (Figure 1).
In the renal function test, there was significant improvement in urea levels (72.6±50.9 vs 49.4±29.8; P. value = 0.000), creatinine levels (3.4±2.5 vs 1.8±0.4; P. value = 0.000) and albumin creatinine ratio (477.5 vs 185; P. value = 0.000) after 6 months of Rituximab use. In addition, 3(7.5%) patients had proteinuria of 1+ or less before Rituximab use and 29 (72.5%) after Rituximab use (P. value = 0.000). Among the patients who underwent renal biopsy (n = 23). Only 4.3% of patients showed minimal mesangial glomerulonephritis before the use of rituximab and raise it to 34.8% after it was been used. Before the use of rituximab, only 17.4% of the patients’ renal biopsy showed mesangial proliferative LN, the percentage increased to 26.1% after 6 months receiving of rituximab, 26.1% of the patients showed focal proliferative nephritis before and after rituximab treatment, 52.2% of all the patients showed diffuse proliferative nephritis which decreased to 8.7% after 6 months treatment with rituximab and only 1% after treatment showed membranous nephritis. Non affordability was the main cause of not renal biopsy conduction in 10 out of 17 patients (58.8%), patient refusal in 6/17 (35.3%), and non-availability in 1/17 (5.9%) patients.
Discussion
The prognosis of SLE and LN patients has improved over the last half-century due to the use of steroids and other agents as well as the introduction of renal dialysis and transplant.15 Still, the damaging effect occurring by corticosteroid treatment increased the rate of morbidity among these patients.16 It is important to initiate induction treatment with the best possible clinical efficacy at a very early stage of LN. The principal goals of LN management are renal remission with minimal toxic effects.17 As a result, efforts and studies have been focused on alternatives that can induce and maintain disease remission and improve overall outcomes.18 Therefore, in this study, we are evaluating the outcome of Rituximab (RTX) to treat patients with LN among SLE Patients.
The mean age of our study participants is 34.9±8 years and the majority of them 40% belonged to the age group of 30–39 years. These findings were comparable to others where it concluded the mean age is 36.2 years,19 and other studies reported mean ages of 30 and 31 years.20
In regards to the renal function test, there was a significant improvement in urea levels (72.6±50.9 vs 49.4±29.8; P. value = 0.000), creatinine levels (3.4±2.5 vs 1.8±0.4. P. value = 0.000). These findings are in agreement with published studies where it found a significant reduction in creatinine levels after 6 months of administration of Rituximab.20,21 Regarding the hematological parameters, there was a significant improvement in hemoglobin (9.9±2.7 vs 11.4±1.6; P. value = 0.000) and platelet count (220.5±143.4220.5±143.4 vs 265±103; P. value = 0.001) after six months of Rituximab use. Similar findings were reported by some authors who studied the effects of RTX in refractory autoimmune hemolytic anemia.22
The albumin creatinine ratio in this study was statistically decreased after 6 months of Rituximab use, leading to reducing of the median urinary protein creatinine ratio from 446 to 190 mg/mmol. Other studies showed similar findings (80). The ultimate aim of LN management is to prevent nephron loss and, thus, chronic kidney diseases, particularly end-stage kidney disease (ESKD), so conventicle therapy such as immunosuppressants is used.23 However, many patients do not achieve short-term remission and experience CKD with these regimens as a result of a new treatment paradigm, by switching to a combination such as rituximab and anti-CD20 obinutuzumab showed very satisfying results.24,25 The levels of CRP, ESR, C3 and C4 levels were significantly increased after 6 months of Rituximab use. The same co-ordination was reported.26
Only 4.3% of patients showed minimal mesangial glomerulonephritis before the use of rituximab and raise it to 34.8% after it was been used. Before the use of rituximab, only 17.4% of the patients’ renal biopsy showed mesangial proliferative LN, the percentage increased to 26.1% after 6 months receiving of rituximab, 26.1% of the patients showed focal proliferative nephritis before and after rituximab treatment, 52.2% of all the patients showed diffuse proliferative nephritis which decreased to 8.7% after 6 months treatment with rituximab and only 1% after treatment showed membranous nephritis.
A remarkable improvement in the histological degree of lupus nephritis was detected by renal biopsy, as the frequency of stage-0 and stage-I (minimal mesangial glomerulonephritis) were 4.3% (n = 1) before Rituximab use and raise to 34.8% (n = 8) after Rituximab use. Stages II–V (mesangial proliferative LN, focal proliferative nephritis and diffuse proliferative nephritis) were found in 95.6% of patients before Rituximab use compared to 65.2% after follow-up (Figure 2). These results were consistent with a review that showed renal activity index (AI) was determined by morphologic alteration in renal biopsy, and the maximum score is 24 points. These trials mostly included patients with active LN despite treatment, WHO or International Society of Nephrology/Renal Pathology Association class III (eight patients), IV (33 patients), III–V (one patient), IV–V (seven patients).27 Twelve patients had class V LN. In all patients, there was a significant reduction in AI following RTX treatment (mean difference =−3.46; 95% CI: −4.43 to −2.50, P < 0.01).18,28
Treatment with rituximab has produced a variety of serologic and clinical side effects depending on the disease; in SLE some studies reported resistant clinical manifestations, such as renal, CNS, hematological features and vasculitic.29 Fortunately, none of these effects were been reported in our study patients during the duration of follow up.
Finally, our study showed that, improvement was common among patients aged from 20 to 29 years (P. value = 0.004), patients with diseases duration <5 years (P. value = 0.001), patients were taking 4 doses of Rituximab (P. value = 0.036) and patients were taking Rituximab as initial modality (P. value = 0.045).
Limitation of the study: all the patients were proposed to do renal biopsy; however, only 57.5% of them performed while the rest either refused to go through the procedure or were financially unoffered.
In conclusion, Rituximab treatment in patients with LN showed effective results based on SLEDAI 2K score. There was a significant rise in hemoglobin and platelet count in hematological parameters, reduce urea, creatinine, ACR as well as proteinuria in renal function parameters and reduce CRP, ESR and normalized C3/C4 in inflammatory markers, also it gave a transition into favourable degrees of lupus nephritis. Moreover, the improvement was significant in the patients aged 20–29 years.
Abbreviations
ACR, American College Of Rheumatology; ADCC, Antibody Dependent Cellular Cytotoxicity; AEs, Adverse Events; ANA, Antinuclear Antibodies; ANA, Antineutrophil Cytoplasmic Antibody; APC, Antigen-Presenting Cell; BCR, B Cell Receptor; BLyS, B-Lymphocyte Stimulator; CKD, Chronic Kidney Disease; CMC, Complement Mediated Cytotoxicity; CNS, Central Nervous System; CR, Complete Remission; CYC, Cyclophosphamide; DHEA, Dehydroepiandrosterone; DIL, Drug-Induced Lupus; DLE, Discoid Lupus Erythematosus; DMARDs, Disease-Modifying Anti-Rheumatic Drugs; EBV, Epstein–Barr Virus; ESRD, End Stage Renal Disease; EXPLORER, Randomised, Double-Blind, Placebo-Controlled Exploratory Phase II/III SLE Evaluation Of Rituximab; HACA, Human Antichimeric Antibodies; HCQ, Hydroxycholoroquines; IL, Interleukin; ISN/RPS, International Society Of Nephrology/Renal Pathology Society; LILRB4, Leukocyte Immunoglobulin Like Receptor B4; LN, Lupus Nephritis; LUNAR, Lupus Nephritis Assessment with Rituximab; MHC, Major Histocompatibility Complex; MMF, Mycophenolate Mofetil; MTX, Methotrexate; NET, Neutrophil Extracellular Traps; NLE, Neonatal Lupus Erythematosus; NSAID, Non-Steroid Anti-Inflammatory Drug; PR, Partial Remission; RA, Rheumatoid Arthritis; RANTES, Regulated Upon Activation, Normal T Cell Expressed And Presumably Secreted; SLEDAI, SLE Disease Activity Index; SRI, SLE Responder Index; TNF, Tumor Necrosis Factor; WHO, World Health Organization.
Data Sharing Statement
All the data used in the study are available from the first and corresponding author on reasonable request.
Ethics Approval for the Study
Obtained from federal Ministry of health Sudan and Sudan medical specializations board.
Consent for Publication
Obtained.
Acknowledgments
For their support to conduct this research, the authors wish to acknowledge rheumatology counsel at Sudan medical specialization board and Medical and Cancer Research Institute (MCRI), Sudan.
Author Contributions
All authors made a significant contribution to this work, whether that is in the study design, acquisition of data, conception, execution, data analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds have been received.
Disclosure
All authors declare that they have no conflict of interest and the study complies with the Declaration of Helsinki with no received fund.
References
1. Abdelgalil Ali Ahmed S, Adam Essa ME, Ahmed AF, et al. Incidence and clinical pattern of mixed connective tissue disease in Sudanese patients at Omdurman military hospital: hospital-based study. Open Access Rheumatol. 2021;13:333–341. doi:10.2147/OARRR.S335206
2. Ibn Idris Rodwan AA, Ahmed Elmansour OK, Ahmed AFE, et al. A rare association of thrombotic thrombocytopenic purpura with systemic lupus erythematosus in a Sudanese woman: case report. J Blood Med. 2021;12:945–949. doi:10.2147/JBM.S334689
3. Tsokos GC, Lo MS, Costa Reis P, Sullivan KE. New insights into the immunopathogenesis of systemic lupus erythematosus. Nat Rev Rheumatol. 2016;12(12):716–730. doi:10.1038/nrrheum.2016.186
4. Bhat P, Radhakrishnan J. B lymphocytes and lupus nephritis: new insights into pathogenesis and targeted therapies. Kidney Int. 2008;73(3):261–268. doi:10.1038/sj.ki.5002663
5. Bhargava R, Li H, Tsokos GC. Pathogenesis of lupus nephritis: the contribution of immune and kidney resident cells. Curr Opin Rheumatol. 2022. doi:10.1097/BOR.0000000000000887
6. Moulton VR, Suarez-Fueyo A, Meidan E, Li H, Mizui M, Tsokos GC. Pathogenesis of human systemic lupus erythematosus: a cellular perspective. Trends Mol Med. 2017;23(7):615–635. doi:10.1016/j.molmed.2017.05.006
7. Choi SC, Morel L. B cell contribution of the CD4(+) T cell inflammatory phenotypes in systemic lupus erythematosus. Autoimmunity. 2017;50(1):37–41. doi:10.1080/08916934.2017.1280028
8. Mossner E, Brunker P, Moser S, et al. Increasing the efficacy of CD20 antibody therapy through the engineering of a new type II anti-CD20 antibody with enhanced direct and immune effector cell-mediated B-cell cytotoxicity. Blood. 2010;115(22):4393–4402. doi:10.1182/blood-2009-06-225979
9. Yo JH, Barbour TD, Nicholls K. Management of refractory lupus nephritis: challenges and solutions. Open Access Rheumatol. 2019;11:179–188. doi:10.2147/OARRR.S166303
10. Sterner RM, Hartono SP, Grande JP. The pathogenesis of lupus nephritis. J Clin Cell Immunol. 2014;5(2):115.
11. Rosman Z, Shoenfeld Y, Zandman-Goddard G. Biologic therapy for autoimmune diseases: an update. BMC Med. 2013;11:88. doi:10.1186/1741-7015-11-88
12. Leone A, Sciascia S, Kamal A, Khamashta M. Biologicals for the treatment of systemic lupus erythematosus: current status and emerging therapies. Expert Rev Clin Immunol. 2015;11(1):109–116. doi:10.1586/1744666X.2015.994508
13. Sinicato NA, Postal M, Appenzeller S, Niewold TB. Defining biological subsets in systemic lupus erythematosus: progress toward personalized therapy. Pharmaceut Med. 2017;31(2):81–88. doi:10.1007/s40290-017-0178-6
14. Postal M, Costallat LT, Appenzeller S. Biological therapy in systemic lupus erythematosus. Int J Rheumatol. 2012;2012:578641. doi:10.1155/2012/578641
15. Leandro MJ, Edwards JC, Cambridge G, Ehrenstein MR, Isenberg DA. An open study of B lymphocyte depletion in systemic lupus erythematosus. Arthritis Rheum. 2002;46(10):2673–2677. doi:10.1002/art.10541
16. Mahieu MA, Strand V, Simon LS, Lipsky PE, Ramsey-Goldman R. A critical review of clinical trials in systemic lupus erythematosus. Lupus. 2016;25(10):1122–1140. doi:10.1177/0961203316652492
17. Zhou Y, Xiao L, Tang S. Annexin A2 and FTH1 are potential biomarkers for lupus nephritis. Exp Ther Med. 2018;16(5):3766–3776. doi:10.3892/etm.2018.6686
18. Alshaiki F, Obaid E, Almuallim A, Taha R, El-Haddad H, Almoallim H. Outcomes of rituximab therapy in refractory lupus: a meta-analysis. Eur J Rheumatol. 2018;5(2):118–126. doi:10.5152/eurjrheum.2018.17096
19. Machado RIL, Scheinberg MA, Queiroz MY, et al. Use of rituximab as a treatment for systemic lupus erythematosus: retrospective review. Einstein. 2014;12:36–41. doi:10.1590/S1679-45082014AO2706
20. Gunnarsson I, Sundelin B, Jonsdottir T, Jacobson SH, Henriksson EW, van Vollenhoven RF. Histopathologic and clinical outcome of rituximab treatment in patients with cyclophosphamide-resistant proliferative lupus nephritis. Arthritis Rheum. 2007;56(4):1263–1272. doi:10.1002/art.22505
21. Melander C, Sallee M, Trolliet P, et al. Rituximab in severe lupus nephritis: early B-cell depletion affects long-term renal outcome. CJASN. 2009;4(3):579–587. doi:10.2215/CJN.04030808
22. Abadie K, Hege KM. Severe refractory autoimmune hemolytic anemia with five-year complete hematologic response to third course of treatment with rituximab: a case report. J Med Case Rep. 2014;8:175. doi:10.1186/1752-1947-8-175
23. Austin HA, Klippel JH, Balow JE, et al. Therapy of lupus nephritis. Controlled trial of prednisone and cytotoxic drugs. N Engl J Med. 1986;314(10):614–619. doi:10.1056/NEJM198603063141004
24. Mejia-Vilet JM, Malvar A, Arazi A, Rovin BH. The lupus nephritis management renaissance. Kidney Int. 2022;101(2):242–255. doi:10.1016/j.kint.2021.09.012
25. Tamirou F, Houssiau FA. Management of lupus nephritis. J Clin Med. 2021;10(4):670. doi:10.3390/jcm10040670
26. Roccatello D, Sciascia S, Rossi D, et al. Intensive short-term treatment with rituximab, cyclophosphamide and methylprednisolone pulses induces remission in severe cases of SLE with nephritis and avoids further immunosuppressive maintenance therapy. Nephrol Dial Transplant. 2011;26(12):3987–3992. doi:10.1093/ndt/gfr109
27. Merrill JT, Neuwelt CM, Wallace DJ, et al. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2010;62(1):222–233. doi:10.1002/art.27233
28. Zhong Z, Li H, Zhong H, Zhou T. Clinical efficacy and safety of rituximab in lupus nephritis. Drug Des Devel Ther. 2019;13:845–856. doi:10.2147/DDDT.S195113
29. Garcia-Carrasco M, Jimenez-Hernandez M, Escarcega RO, et al. Use of rituximab in patients with systemic lupus erythematosus: an update. Autoimmun Rev. 2009;8(4):343–348. doi:10.1016/j.autrev.2008.11.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.