")
Back to Journals » OncoTargets and Therapy » Volume 16
Efficacy and Safety of Nanosomal Docetaxel Lipid Suspension (NDLS) versus Conventional Docetaxel as Neoadjuvant and Adjuvant Therapy for Primary Operable Breast Cancer
Authors Badiginchala R, Dattatreya PS, Suresh AVS, Nirni SS, Andra VV, Bunger D, Chaturvedi A
Received 8 December 2022
Accepted for publication 2 March 2023
Published 1 April 2023 Volume 2023:16 Pages 215—225
DOI https://doi.org/10.2147/OTT.S400824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Revathi Badiginchala,1 Palanki Satya Dattatreya,1 Attili Venkata Satya Suresh,1 Sharanabasappa Somanath Nirni,1 Vindhya Vasini Andra,1 Deepak Bunger,2 Alok Chaturvedi2
1Medical Oncology, Omega Hospitals, Hyderabad, Telangana, India; 2Medical Affairs, Intas Pharmaceuticals Limited, Ahmedabad, India
Correspondence: Revathi Badiginchala, Omega Hospitals, L/276A, Road Number 12, MLA Colony, Banjara Hills, Hyderabad, Telangana, 500034, India, Tel +8978698260, Email [email protected]
Objective: Nanosomal docetaxel lipid suspension (NDLS) is a novel formulation developed to overcome toxicity issues caused by excipients (polysorbate 80 and ethanol) present in commercially available docetaxel formulation. We conducted a prospective, observational study to compare the outcomes of nanosomal docetaxel lipid suspension (NDLS)-based versus conventional docetaxel-based chemotherapy in primary operable breast cancer.
Methods: Sixty adult women with newly diagnosed stage IIb-III breast cancer were included. Patients received NDLS-based (n=30) or docetaxel-based (n=30) chemotherapy. Patients received (1) four cycles of preoperative doxorubicin and cyclophosphamide (AC) followed by four cycles of NDLS or docetaxel (T) and surgery (neoadjuvant AC→NDLS [n=9], or neoadjuvant AC→T [n=10]), or (2) four cycles of preoperative AC followed by surgery and postoperative NDLS or T (neoadjuvant AC→adjuvant NDLS [n=14], or neoadjuvant AC→adjuvant T [n=15]), or (3) surgery followed by postoperative AC→NDLS or T (adjuvant AC→NDLS [n=7], or adjuvant AC→T [n=5]) regimens. The study outcomes were pathological complete response (pCR) rates, clinical overall response rates (ORR), disease-free survival (DFS), overall survival (OS), and adverse event (AE) profile.
Results: For neoadjuvant AC→T (n=10) vs neoadjuvant AC→NDLS (n=9), the pCR rates were 100% each, and the ORR were 100% vs 88.9% (p=1.0). All patients were alive at 6 months, and the median OS was not reached. Three patients had progressive disease (T: n=2, NDLS: n=1) with a DFS of 12 weeks in all three patients. Grade 3 infusion-related reactions were seen in five patients (16.7%) in T vs none in NDLS arms.
Conclusion: NDLS-based neo/adjuvant chemotherapy was efficacious in the treatment of primary operable breast cancer and showed comparable pCR, ORR, DFS and OS rates versus conventional docetaxel. NDLS was better tolerated than conventional docetaxel.
Keywords: NDLS, nanosomal docetaxel lipid suspension, docetaxel, breast cancer, operable
Introduction
Neoadjuvant chemotherapy (NACT) is considered the standard treatment option for early/locally advanced and primary operable breast cancer.1 Achieving pathological complete response (pCR) after NACT is associated with improved survival benefits and is considered as a surrogate endpoint for survival outcomes.2 The addition of taxanes to NACT has improved patient outcomes in clinical studies.3–5 In the National Surgical Adjuvant Breast and Bowel Project (NSABP) B27 study, the addition of docetaxel to neoadjuvant doxorubicin/cyclophosphamide therapy increased the pCR rate from 13.7% to 26.1%.6
Docetaxel is a hydrophobic molecule, and hence, polysorbate 80, a synthetic nonionic surfactant, along with ethanol as diluent is used in the conventional docetaxel formulation.7 Polysorbate 80 has been implicated in some adverse events (AEs) associated with drugs formulated with this vehicle.8,9 Studies have linked polysorbate 80 with acute hypersensitivity reactions and cumulative fluid retention, peripheral neuropathy, severe anaphylactoid reactions, and infusion-site reactions, among others.1,8,10–13 There are reports of alcohol intoxication in patients receiving conventional docetaxel.14,15
Lipid-based nanoformulations can effectively increase the drug’s water solubility, significantly improve drug membrane permeability and allow sustained drug release.16 Nanosomal (<100nm) particles of NDLS, developed using the “NanoAqualip” technology,13 may increase the systemic availability of docetaxel through enhanced permeability and retention in compromised tumor vasculature, and thus, overall improved therapeutic outcomes can be anticipated.12 Nanosomal docetaxel lipid suspension (NDLS) is a novel lipid-based, polysorbate 80- and ethanol-free formulation of docetaxel, which was developed13 to overcome the toxicity challenges generally associated with conventional docetaxel formulation. NDLS can obviate the need for premedication with corticosteroids because of its much lower risk of hypersensitivity compared with conventional docetaxel.12,13 NDLS has demonstrated better response rates and tolerability in locally advanced or metastatic breast cancer (MBC) versus conventional docetaxel.12 The safety and efficacy of NDLS as neoadjuvant and adjuvant therapy in locally advanced breast cancer has been reported in a real-world setting.17
There is a lack of head-to-head comparison of NDLS vs conventional docetaxel in neoadjuvant or adjuvant treatment of breast cancer. Hence, this study was conducted to compare the clinical outcomes of NDLS vs conventional docetaxel-based chemotherapy regimens when administered in a neoadjuvant or adjuvant setting in patients with locally advanced, primary operable breast cancer.
Patients and Methods
Study Design and Population
This prospective, observational study was conducted at Omega Hospitals, Hyderabad, Telangana, India, between September 2020 and August 2021. Patients aged above 18 years with newly diagnosed histologically confirmed stage IIb and IIIa breast cancer irrespective of subtypes (eg hormone receptor [HR] positive or negative, human epidermal growth factor receptor 2 [HER2] positive or negative and triple negative breast cancer [TNBC]), with an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, were included. Patients with dual malignancy and pregnant women and lactating mothers were excluded.
The exclusion criteria were as follows: (1) patients who received any type of treatment prior to neoadjuvant or adjuvant treatment, including chemotherapy, targeted therapy, radiotherapy, or endocrine therapy; (2) with previous or synchronous invasive or in situ breast cancer, male breast cancer, bilateral breast cancer, or inflammatory breast cancer; and (3) with acute and chronic inflammatory disease, autoimmune disease, mental disease, severe liver, kidney insufficiency, or serious complications. The cancer staging was done as per the eighth edition of American Joint Committee on Cancer (AJCC) guidelines.18 The study was conducted after approval from the Omega Hospital Institutional Ethical Committee. The study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and in accordance with the International Conference on Harmonization’s Good Clinical Practice (ICH-GCP) guidelines, relevant regulatory requirements, and in accordance with the protocol. All patients provided written informed consent.
Treatments
Patients were randomly allocated to NDLS or conventional docetaxel arms at the discretion of medical oncologist. Patients in NDLS group (n = 30) received (1) four cycles of preoperative doxorubicin and cyclophosphamide (AC) followed by four cycles of NDLS and then surgery (neoadjuvant AC→NDLS) or (2) four cycles of preoperative AC followed by surgery and postoperative NDLS (neoadjuvant AC→adjuvant NDLS), or (3) surgery followed by postoperative AC→NDLS (adjuvant AC→NDLS). Patients in docetaxel group (n = 30) received (1) four cycles of preoperative AC followed by four cycles of docetaxel (T) and then surgery (neoadjuvant AC→T) or (2) four cycles of preoperative AC followed by surgery and postoperative T (neoadjuvant AC→adjuvant T), or (3) surgery followed by postoperative AC→T (adjuvant AC→T).
The patients received either NDLS-based (75 mg/m2 IV over 60 min) or conventional docetaxel-based (75 mg/m2 IV over 60 min) chemotherapy with repeat cycles every 3 weeks for 4 cycles. All patients received four cycles of doxorubicin and cyclophosphamide at doses of 60 and 600 mg/m2, respectively, administered every 3 weeks.
Patients in both arms were pre-medicated with intravenous (IV) fosaprepitant 150 mg, IV palonosetron 0.25 mg, and IV dexamethasone 16 mg before all cycles. All patients received primary prophylaxis with subcutaneous (SC) pegfilgrastim 6 mg in all cycles. The HER2 positive patients received IV trastuzumab at 8 mg/kg on week 1 followed by 6 mg/kg every 3 weeks. The HR+ patients were treated as per the institutional practice. Patients were followed-up for 6 months following treatment completion.
NACT was delivered according to patients’ specific disease features following the guidelines of the National Comprehensive Cancer Network (NCCN). The physicians modified the treatment regimen doses and schedules according to tumor response and side effects. All patients underwent surgery 2–4 weeks after NACT. Pathological diagnosis was obtained via core needle biopsy before initiating NACT. Immunohistochemistry (IHC) was used to assess estrogen receptor (ER), progesterone receptor (PR), HER2 status, and Ki-67 level. ER- and PR-positive were defined as ≥1% positively stained tumor cells. HER2 status was evaluated using IHC and fluorescence in situ hybridization (FISH). HER2-negative was defined as an IHC scoring of 1+ or 2+ with FISH non-amplified, whereas HER2 positive was defined as 3+ on IHC based on the American Society of Clinical Oncology (ASCO) Guidelines.19 The cells with Ki-67 were counted and expressed as the percentage of cells with positive nuclear staining among the total tumor cells. The molecular subtypes of breast cancer were classified according to the St. Gallen Consensus.20
Study Outcomes
Baseline evaluation was performed within 1 week before NACT, and the post-treatment response assessments of NACT were evaluated before surgery by ultrasonography or magnetic resonance imaging (MRI). The pathology reports were reviewed by a pathologist to determine the pathological response category. pCR was defined as no pathologic evidence of a residual invasive carcinoma in the breast or axillary lymph nodes (ypT0/isN0 status) as per Miller-Payne grading system.21 Residual ductal carcinoma in situ was included under pCR. The clinical tumor response to NACT was measured following four cycles of AC→T, AC→NDLS and AC regimens in neoadjuvant settings using the RECIST 1.1.22 Complete response (CR) was defined as disappearance of all target lesions, partial response (PR) as a decline of ≥30% in tumor maximum diameter, and progressive disease (PD) as an increase of ≥20% from the baseline in the sum of all tumor diameter measurements. The disease was categorized as a stable disease (SD) when CR, PR, or PD were not noted.
Disease-free survival (DFS), overall survival (OS) and adverse events (AEs) were also evaluated. For DFS, OS and AEs, patients receiving NDLS-based or conventional docetaxel-based chemotherapy regimens in both neoadjuvant and adjuvant settings were considered. DFS was defined as the time from randomization to recurrence of tumor or death, and OS was defined as the time from the date of administration of first dose of chemotherapy till the last follow-up date for living patients and date of death for patients who died. AEs were graded as per the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.23 All patients were followed up every 3 months by telephone or outpatient interview for at least 6 months.
Statistical Analysis
Demographic and baseline characteristics were summarized using descriptive statistics. Categorical variables were summarized as frequency and percentage. Continuous variables were summarized as count, mean and standard deviation. Patients achieving pCR, ORR and experiencing AEs were presented as proportions. The median OS and DFS duration were determined. Quantitative variables were compared using unpaired t-test. Qualitative variables were correlated using Chi-square test/Fisher’s exact test. A p value of < 0.05 was considered statistically significant. The data analysis was performed using Graph Pad Prism version 9.
Results
Patient Population and Treatments
Between September 2020 and August 2021, a total of 60 patients with primary operable breast cancer were administered NDLS-based (n = 30) or conventional docetaxel-based (n = 30) chemotherapy for 4 cycles in a neoadjuvant or adjuvant setting. In the NDLS arm (n = 30), patients were administered neoadjuvant AC→NDLS (n = 9), neoadjuvant AC→ adjuvant NDLS (n = 14), or adjuvant AC→NDLS (n = 7) regimens. In the docetaxel arm, patients were administered neoadjuvant AC→T (n = 10), neoadjuvant AC→ adjuvant T (n = 15), or adjuvant AC→T (n = 5) regimens (Figure 1).
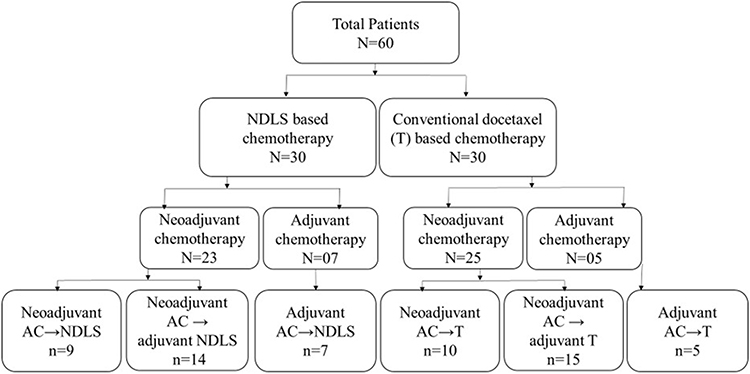 |
Figure 1 Patients’ disposition. In NDLS arm, patients were administered neoadjuvant AC followed by NDLS (AC→NDLS regimen; n=9), neoadjuvant AC regimen followed by adjuvant NDLS (n=14), or adjuvant AC followed by NDLS (AC→NDLS; n=7) regimens. In docetaxel arm, patients were administered neoadjuvant doxorubicin, cyclophosphamide (AC) followed by docetaxel (T) (AC→T regimen; n=10), neoadjuvant AC regimen followed by adjuvant T (n=15), or adjuvant AC followed by T (AC→T; n=5) regimens. In HER2+ patients in both the arms, trastuzumab was administered at 8 mg/kg IV on Week 1 followed by 6 mg/kg IV every 21 days. |
Baseline Demographics and Disease Characteristics
The baseline demographics and disease characteristics of the treatment arms were overall comparable (Table 1). Most patients in both NDLS and docetaxel treatment arms were post-menopausal females, and aged 50–59 years (60% vs 50%) followed by 40–49 years (33.3% vs 40%). All the study patients had invasive ductal carcinoma. The majority of patients in both arms had ECOG score 1–2, triple positive stage IIb breast cancer with cT2 tumor stage, cN1 nodal stage, tumor grade 2 and intermediate Ki-67 status (Table 1).
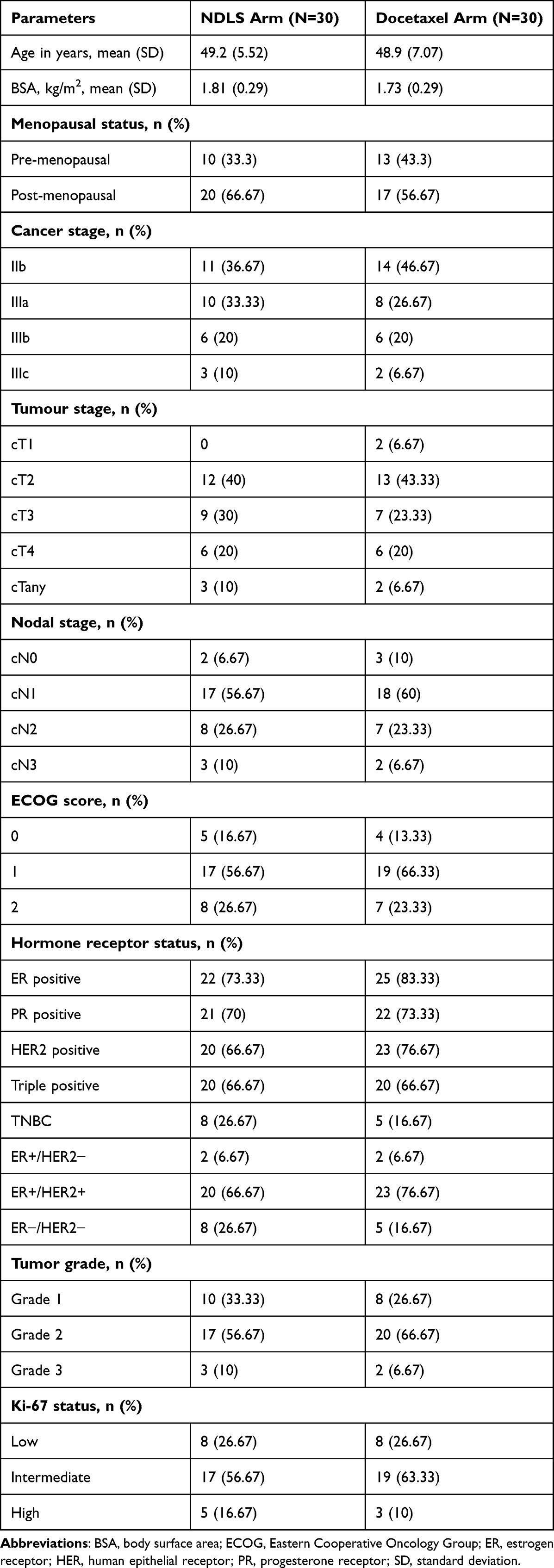 |
Table 1 Baseline Demographics and Disease Characteristics |
Pathological Response Rate
All patients who received neoadjuvant AC→NDLS and AC→T regimens achieved pCR (100% for both). The pCR rate for patients receiving neoadjuvant AC→adjuvant NDLS was 71.43% (n=10/14) and neoadjuvant AC→adjuvant T was 53.33% (n=8/15), and the difference was not statistically significant (Figure 2); the ypT0/isypN0/+ status was 28.57% (n=4/14) vs 40% (n=6/15) (p=0.5176), whereas one patient in the docetaxel arm had ypT+N+ status. The hormone receptor and HER2 positive status did not affect the pCR rates between the treatment arms (Table 2).
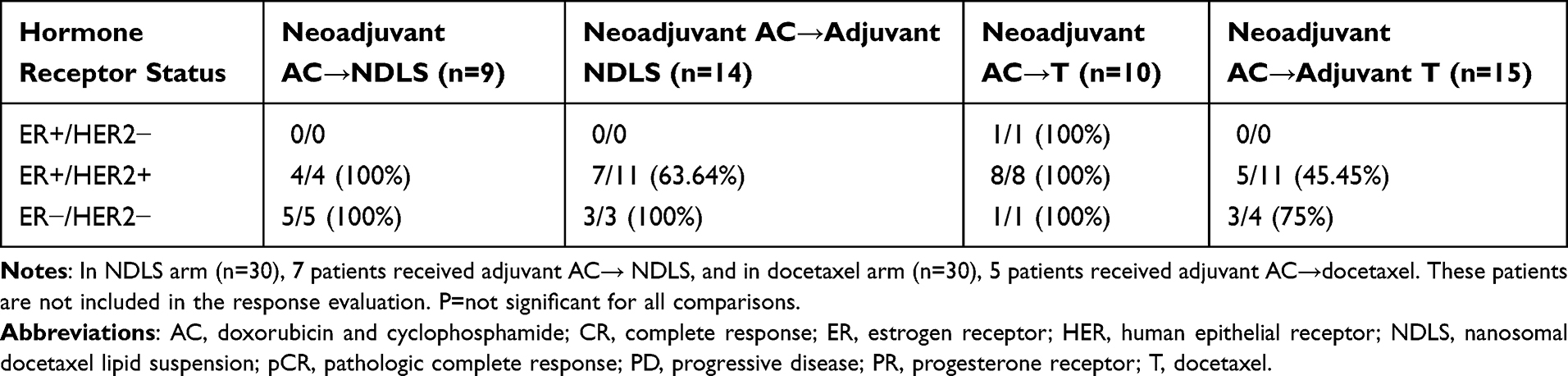 |
Table 2 Pathologic Complete Response Rates Based on Hormone and HER2 Receptor Status |
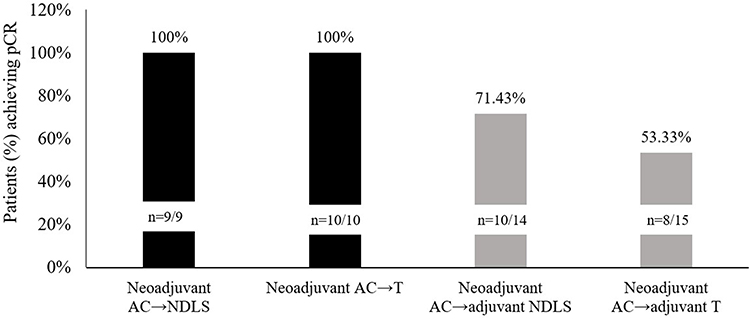 |
Figure 2 Pathologic complete response rates. Abbreviations: pCR, pathologic complete response rate; AC, doxorubicin and cyclophosphamide combination regimen; AC→NDLS, doxorubicin and cyclophosphamide combination regimen followed by sequential nanosomal docetaxel lipid suspension; AC→T, doxorubicin and cyclophosphamide combination regimen followed by sequential conventional docetaxel. |
Clinical Response Rates
There were no statistically significant (P>0.05) differences observed for clinical response between the NDLS-based vs conventional docetaxel-based NACT regimens (Figure 3). Similarly, the hormone and HER-2 receptor status did not affect the clinical response rates across the neoadjuvant treatment regimens (Table 3). The majority of patients underwent a modified radical mastectomy (MRM) [docetaxel: 25 (83.33%), NDLS: 27 (90%)], while the rest underwent breast conservation surgery (BCS). Both treatment arms were comparable with no statistically significant differences between them.
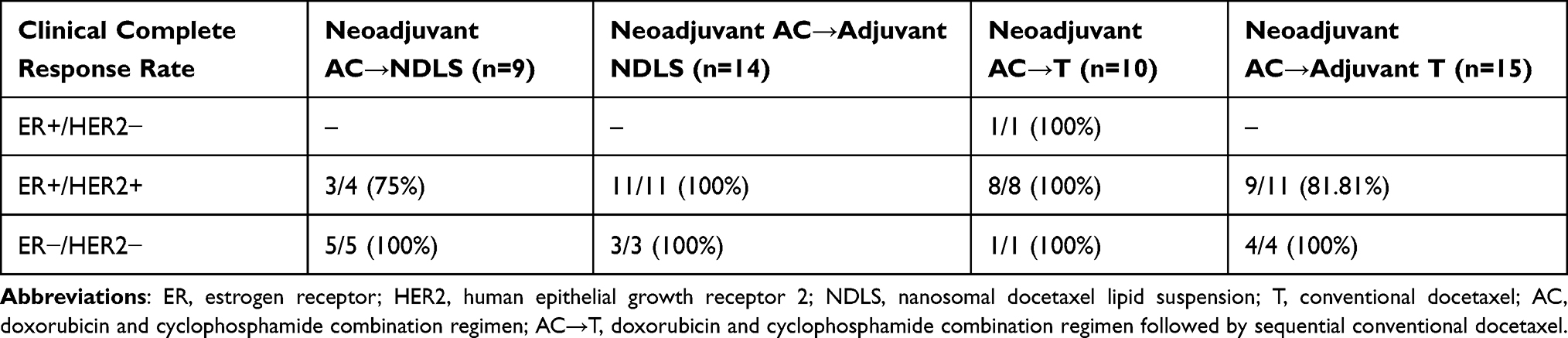 |
Table 3 Clinical Response Rates Based on Hormone Receptor Status |
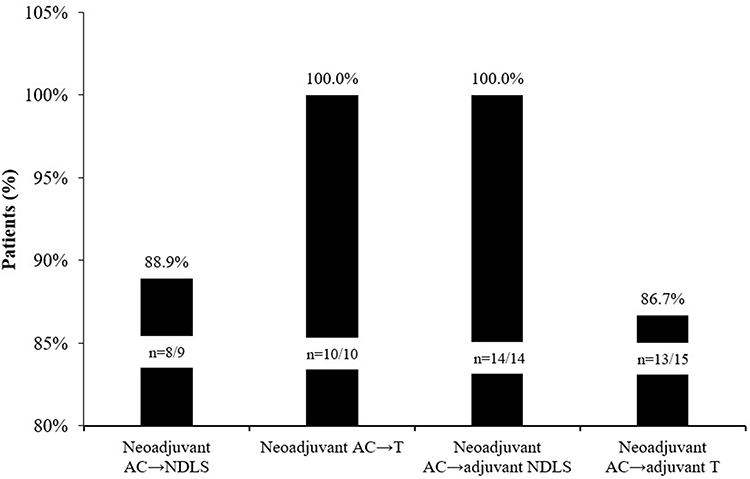 |
Figure 3 Clinical response rate. Abbreviations: AC, doxorubicin and cyclophosphamide combination regimen; AC→NDLS, doxorubicin and cyclophosphamide combination regimen followed by sequential nanosomal docetaxel lipid suspension; AC→T, doxorubicin and cyclophosphamide combination regimen followed by sequential conventional docetaxel; NDLS, nanosomal docetaxel lipid suspension; T, docetaxel. |
Disease Free Survival and Overall Survival
All the 60 patients were alive at 6 months follow-up; hence, the median OS was not evaluable in either of the treatment arms. After completion of four cycles, three patients had PD, two in the docetaxel arm and one in the NDLS arm. DFS was 12 weeks in all three patients.
Safety
In this study, none of the patients had febrile neutropenia or grade 3 thrombocytopenia in either arms. In the NDLS arm, no patient had grade 3 infusion-related (IRRs) or allergic reactions, while IRRs were observed in five patients (16.7%) in the docetaxel arm. Grade 3 AEs in terms of anaphylactic reactions, hyperglycemia, and peripheral neuropathy were noted in 3%, 27% and 10% patients in the docetaxel treatment arm only.
Discussion
The current prospective, observational study compared the clinical outcomes of NDLS-based versus conventional docetaxel-based neoadjuvant or adjuvant chemotherapy in primary operable breast cancer. The study demonstrated comparable response rates with a better safety profile for NDLS based regimens.
For NDLS, it has been hypothesized that an enhanced permeability and retention (EPR) effect may result in enhanced transport of NDLS to tumors and an improved tolerability profile of NDLS compared with that of docetaxel at equimolar doses, with no requirement of corticosteroid premedication.12,13 NDLS, a novel lipid-based polysorbate 80 and ethanol-free docetaxel formulation, has demonstrated better response rates and tolerability in advanced breast cancer patients in comparison to conventional docetaxel.12 In this study, conventional docetaxel and NDLS both given as IV infusion at a dose of 75 mg/m2 in locally advanced or MBC patients, who previously had failed chemotherapy, demonstrated a higher ORR for NDLS at 35.5% compared to 26.3% for conventional docetaxel.24 Head-to-head data comparison between NDLS and docetaxel is still lacking in a curative setting.
The sequential use of docetaxel in a neoadjuvant setting after completion of AC cycles has shown increased pCR rates as compared to neoadjuvant AC regimens alone in the National Surgical Adjuvant Breast and Bowel Project (NSABP)-2725 and the German Preoperative Adriamycin Docetaxel Study Group (GEPARDUO)26 studies.
In the Phase III NSABP-27 study, compared to preoperative AC alone, preoperative AC followed by docetaxel increased the pCR rate (13.7% vs 26.1%; p<0.001), clinical CR rate (40.1% vs 63.6%; p<0.001), and ORR (85.5% vs 90.7%; p<0.001).25 In the GEPARDUO trial, sequential doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2 (AC) every 21 days followed by docetaxel 100 mg/m2 every 21 days for four cycles each in a neoadjuvant setting showed a pCR rate of 22.4% and ORR of 85% in patients with early breast cancer (n=453).26 In a randomized Phase II study by Schneeweiss et al, AC→T (four cycles of doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2 q3w followed by four cycles of docetaxel 100 mg/m2 q3w) showed a pCR rate of 20.2% and ORR of 68.1%.24 In a study by the Dutch Breast Cancer Trialists’ Group (BOOG) patients (n=201) treated with 4 cycles of sequential doxorubicin/cyclophosphamide (60/600 mg/m2) followed by 4 cycles of docetaxel (100 mg/m2) showed a pCR rate of 28% in patients with large resectable or locally advanced breast cancer.27
In our study, the pCR rates for both neoadjuvant AC→T and neoadjuvant AC→NDLS were 100%. The hormone receptor and HER-2 positivity status had no significant influence on response rates for both the arms in our study. The pCR rate for neoadjuvant AC→adjuvant NDLS was 71.43% and neoadjuvant AC→adjuvant T was 53.33% in our study. The NSABP-27 reported a pCR rate of 14.5% in the neoadjuvant AC→ adjuvant docetaxel.25 The high pCR rates in our study could be attributed to a small sample size.
Breast-conserving surgery (BCS) is the primary surgical choice for breast cancer. In some patients, MRM is still carried out due to tumour size (relative to breast size), tumour multicentricity, inability to achieve negative surgical margins after multiple resections, prior radiation to the chest wall/breast or other contraindications to RT, unsuitability for oncoplastic breast conservation, and patient choice.28 However, in our study, as most of the patients reporting at the study center were from far-flung, rural areas and had logistic concerns in terms of frequent follow-ups after BCS, majority of them underwent MRM in both the docetaxel and NDLS treatment arms.
Adjuvant chemotherapy is a well-established strategy for lowering the risk of breast cancer recurrence and improving survival.29,30 Docetaxel is recommended as a combination therapy for treating breast cancer in an adjuvant setting by several guidelines.17,31,32 Docetaxel either in combination with anthracyclines (ie, the docetaxel, doxorubicin and cyclophosphamide [TAC] regimen) or sequentially (ie, four cycles of AC followed by four cycles of docetaxel [AC→T]) is commonly used as an adjuvant treatment of breast cancer.33 A meta-analysis of most effective adjuvant therapy regimens in early stage breast cancer by Fujii et al concluded that the sequential AC→T is the most effective adjuvant therapy regardless of hormone receptor status.34 In our study, 7 patients received AC→NDLS and 5 patients received AC→T regimens in the adjuvant setting. The median OS was not reached for both NDLS-based and conventional docetaxel-based chemotherapy arms in the current study. Similar results were reported in breast cancer patients in a multicentric real-world study by Subramaniam et al, in which the median OS was not reached for patients who were treated with NDLS-based chemotherapy either in a neoadjuvant or an adjuvant setting.17 All the study patients were alive at 6 months follow-up after the study completion, whereas in the study by Subramaniam et al, the proportion of patients who were alive was 91.7% in the neoadjuvant setting and 90.2% in the adjuvant setting at median follow-up durations of 21.1 months and 21.6 months, respectively.17 Several other studies have reported the effectiveness of AC→T regimen as adjuvant chemotherapy in early breast cancer patients.35,36
Docetaxel causes a variety of acute and long-term side effects. Important AEs associated with docetaxel include infusion reactions, febrile neutropenia, fatigue, fluid retention, pneumonitis, cutaneous and nail toxicity, epiphora and lacrimal duct stenosis, gastrointestinal complications, and neuropathies.37 Peripheral neuropathy is a long-term side effect of taxane chemotherapy that may be debilitating for patients well after completion of treatment.38 In our study, there were no events of febrile neutropenia or grade 3 thrombocytopenia in both the arms. In the docetaxel arm, grade 3 AEs such as neutropenia (3.3%), infusion-related reactions (16.7%), allergic reactions and anaphylaxis (3.3%), hyperglycemia (26.7%), and peripheral neuropathy (10%) were reported, whereas in the NDLS arm grade 3 events of only neutropenia (6.7%) were reported, suggesting a better safety profile of NDLS.
The safety profile of NDLS was evaluated in MBC patients in the study by Ahmad et al and showed all grade ≥3 treatment-related AEs in 77.55% vs 52.17% of patients receiving NDLS and conventional docetaxel, respectively.12 In the study by Subramanian et al, at least one AE was reported in 85.2% patients. Anemia, thrombocytopenia, lymphopenia and neutropenia were the most common haematological AEs, whereas hyperglycemia and alteration in liver function tests were the most common non-hematological AEs reported. AEs of interest with docetaxel such as hypersensitivity reactions, fluid retention, peripheral neuropathy and nail disorders were not reported with the use of NDLS.17
The study limitations include a single center and non-randomized study design with a small sample size and short follow-up duration. As a result, there may be a potential selection bias and statistical error. Second, it is a small cohort study, which may affect the effectiveness of the results. In the future, a study with larger sample size to verify the results is necessary. Finally, the follow-up of this study is relatively short; hence, studies with long-term follow-up are needed to elicit a more accurate result.
Conclusions
In summary, our real-world study demonstrated that NDLS was as effective as conventional docetaxel in neo/adjuvant setting for locally advanced primary operable breast cancer, irrespective of receptor status. Overall, NDLS was better tolerated as compared with conventional docetaxel. This study provides a valuable reference for the management of patients with primary operable breast cancer. More patients with early and locally advanced breast cancer are now being diagnosed globally because of efficient screening programs and neoadjuvant chemotherapy (NACT) is increasingly being used to treat such patients. NDLS can be a safe and effective option for these patients; however, studies with a larger sample size and longer follow-up would be required to prove the safety and efficacy of NDLS in a neoadjuvant setting.
Acknowledgment
The authors thank Mr. Shreekant Sharma (Intas Pharmaceuticals Limited, Ahmedabad, India) for manuscript writing and follow-up with journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval to the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
DB and AC are employees of Intas Pharmaceuticals Ltd. The authors report no other conflicts of interest in this work.
References
1. Sarid D, Ron IG, Sperber F, et al. Neoadjuvant treatment with paclitaxel and epirubicin in invasive breast cancer: a phase II study. Clin Drug Investig. 2006;26(12):691–702. doi:10.2165/00044011-200626120-00003
2. Pennisi A, Kieber-Emmons T, Makhoul I, Hutchins L. Relevance of pathological complete response after neoadjuvant therapy for breast cancer. Breast Cancer. 2016;10:103–106. doi:10.4137/BCBCR.S33163
3. Buzdar AU, Singletary SE, Theriault RL, et al. Prospective evaluation of paclitaxel versus combination chemotherapy with fluorouracil, doxorubicin, and cyclophosphamide as neoadjuvant therapy in patients with operable breast cancer. J Clin Oncol. 1999;17(11):3412–3417. doi:10.1200/JCO.1999.17.11.3412
4. Gradishar WJ. Docetaxel as neoadjuvant chemotherapy in patients with stage III breast cancer. Oncology. 1997;11(8 Suppl 8):15–18.
5. Miller KD, McCaskill-Stevens W, Sisk J, et al. Combination versus sequential doxorubicin and docetaxel as primary chemotherapy for breast cancer: a randomized pilot trial of the Hoosier Oncology Group. J Clin Oncol. 1999;17(10):3033–3037. doi:10.1200/JCO.1999.17.10.3033
6. Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of national surgical adjuvant breast and bowel project protocols B-18 and B-27. J Clin Oncol. 2008;26(5):778–785. doi:10.1200/JCO.2007.15.0235
7. Sánchez-Moreno P, Boulaiz H, Ortega-Vinuesa JL, Peula-García JM, Aránega A. Novel drug delivery system based on docetaxel-loaded nanocapsules as a therapeutic strategy against breast cancer cells. Int J Mol Sci. 2012;13(4):4906–4919. doi:10.3390/ijms13044906
8. ten Tije AJ, Verweij J, Loos WJ, Sparreboom A. Pharmacological effects of formulation vehicles: implications for cancer chemotherapy. Clin Pharmacokinet. 2003;42(7):665–685. doi:10.2165/00003088-200342070-00005
9. van Zuylen L, Verweij J, Sparreboom A. Role of formulation vehicles in taxane pharmacology. Invest New Drugs. 2001;19(2):125–141. doi:10.1023/A:1010618632738
10. Engels FK, Mathot RA, Verweij J. Alternative drug formulations of docetaxel: a review. Anticancer Drugs. 2007;18(2):95–103. doi:10.1097/CAD.0b013e3280113338
11. Taxotere®. Prescribing_information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020449s059lbl.pdf.
12. Ahmad A, Sheikh S, Taran R, et al. Therapeutic efficacy of a novel nanosomal docetaxel lipid suspension compared with taxotere in locally advanced or metastatic breast cancer patients. Clin Breast Cancer. 2014;14(3):177–181. doi:10.1016/j.clbc.2013.09.011
13. Ahmad A, Sheikh S, Ali S, Ahmad M, Paithankar M. Development of aqueous based formulation of docetaxel: safety and pharmacokinetics in patients with advanced solid tumors. J Nanomed Nanotechnol. 2015;6:295.
14. Mirza A, Mithal N. Alcohol intoxication with the new formulation of docetaxel. Clin Oncol. 2011;23(8):560–561. doi:10.1016/j.clon.2011.04.010
15. Estevez LG, Cuevas JM, Anton A, et al. Weekly docetaxel as neoadjuvant chemotherapy for stage II and III breast cancer: efficacy and correlation with biological markers in a Phase II, multicenter study. Clin Cancer Res. 2003;9(2):686–692.
16. McKeage K. Nanosomal docetaxel lipid suspension: a guide to its use in cancer. Clin Drug Investig. 2017;37(4):405–410. doi:10.1007/s40261-017-0510-7
17. Subramanian S, Prasanna R, Biswas G, et al. Nanosomal docetaxel lipid suspension-based chemotherapy in breast cancer: results from a multicenter retrospective study. Breast Cancer. 2020;12:77–85. doi:10.2147/BCTT.S236108
18. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
19. Wolff AC, Hammond MEH, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice guideline focused update. J Clin Oncol. 2018;36(20):2105–2122. doi:10.1200/JCO.2018.77.8738
20. Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn HJ. Strategies for subtypes--dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22(8):1736–1747. doi:10.1093/annonc/mdr304
21. Ogston KN, Miller ID, Payne S, et al. A new histological grading system to assess response of breast cancers to primary chemotherapy: prognostic significance and survival. Breast. 2003;12(5):320–327. doi:10.1016/S0960-9776(03)00106-1
22. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
23. National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf.
24. Schneeweiss A, Marmé F, Ruiz A, et al. A randomized phase II trial of doxorubicin plus pemetrexed followed by docetaxel versus doxorubicin plus cyclophosphamide followed by docetaxel as neoadjuvant treatment of early breast cancer. Ann Oncol. 2011;22(3):609–617. doi:10.1093/annonc/mdq400
25. Bear HD, Anderson S, Brown A, et al. The effect on tumor response of adding sequential preoperative docetaxel to preoperative doxorubicin and cyclophosphamide: preliminary results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2003;21(22):4165–4174. doi:10.1200/JCO.2003.12.005
26. von Minckwitz G, Raab G, Caputo A, et al. Doxorubicin with cyclophosphamide followed by docetaxel every 21 days compared with doxorubicin and docetaxel every 14 days as preoperative treatment in operable breast cancer: the GEPARDUO study of the German Breast Group. J Clin Oncol. 2005;23(12):2676–2685. doi:10.1200/JCO.2005.05.078
27. Vriens B, Van de Vijver K, Boetes C, et al. Abstract P1-11-10: sequential versus upfront intensified neoadjuvant chemotherapy in patients with large resectable or locally advanced breast cancer (INTENS), first results from a phase III study of the Dutch Breast Cancer Trialists’ Group (BOOG). Cancer Res. 2010;70(24):P1–11–10. doi:10.1158/0008-5472.SABCS10-P1-11-10
28. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(8):1194–1220. doi:10.1093/annonc/mdz173
29. Thiery-Vuillemin A, Llombart-Cussac A, Chaigneau L, et al. Sequential taxane and anthracycline-containing neoadjuvant regimens: the sequential order impact. Breast. 2011;20(1):46–49. doi:10.1016/j.breast.2010.07.001
30. Zaheed M, Wilcken N, Willson ML, O’Connell DL, Goodwin A. Sequencing of anthracyclines and taxanes in neoadjuvant and adjuvant therapy for early breast cancer. Cochrane Database Syst Rev. 2019;2(2):CD012873–CD012873. doi:10.1002/14651858.CD012873.pub2
31. Bear HD, Anderson S, Smith RE, et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: nationalSurgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2006;24(13):2019–2027. doi:10.1200/JCO.2005.04.1665
32. Cardoso F, Senkus E, Costa A, et al. 4th ESO-ESMO international consensus guidelines for Advanced Breast Cancer (ABC 4)†. Ann Oncol. 2018;29(8):1634–1657. doi:10.1093/annonc/mdy192
33. Martin M. Docetaxel, Doxorubicin and Cyclophosphamide (the TAC regimen): an effective adjuvant treatment for operable breast cancer. Womens Health. 2006;2(4):527–537. doi:10.2217/17455057.2.4.527
34. Fujii T, Le Du F, Xiao L, et al. Effectiveness of an adjuvant chemotherapy regimen for early-stage breast cancer: a systematic review and network meta-analysis. JAMA Oncol. 2015;1(9):1311–1318. doi:10.1001/jamaoncol.2015.3062
35. Eiermann W, Pienkowski T, Crown J, et al. Phase III study of doxorubicin/cyclophosphamide with concomitant versus sequential docetaxel as adjuvant treatment in patients with human epidermal growth factor receptor 2-normal, node-positive breast cancer: BCIRG-005 trial. J Clin Oncol. 2011;29(29):3877–3884. doi:10.1200/JCO.2010.28.5437
36. Livi L, Meattini I, de Luca Cardillo C, et al. Use of doxorubicin plus cyclophosphamide followed by docetaxel as adjuvant chemotherapy for breast cancer. J Chemother. 2011;23(1):36–39. doi:10.1179/joc.2011.23.1.36
37. Murali A, Gupta S, Pendharkar D. Efficacy and tolerability of nanoparticle docetaxel lipid suspension. J Clin Oncol. 2018;36(15_suppl):e14542–e14542. doi:10.1200/JCO.2018.36.15_suppl.e14542
38. Ho MY, Mackey JR. Presentation and management of docetaxel-related adverse effects in patients with breast cancer. Cancer Manag Res. 2014;6:253–259. doi:10.2147/CMAR.S40601
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.