")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 13
Efficacy and Safety of Evocalcet Evaluated by Dialysate Calcium Concentration in Patients with Secondary Hyperparathyroidism Undergoing Hemodialysis
Authors Shigematsu T , Asada S, Endo Y, Kawata T , Fukagawa M, Akizawa T
Received 21 December 2019
Accepted for publication 20 March 2020
Published 12 May 2020 Volume 2020:13 Pages 97—106
DOI https://doi.org/10.2147/IJNRD.S243210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Takashi Shigematsu,1 Shinji Asada,2 Yuichi Endo,3 Takehisa Kawata,2,3 Masafumi Fukagawa,4 Tadao Akizawa5
1Department of Nephrology, Wakayama Medical University, Wakayama, Japan; 2Medical Affairs Department, Kyowa Kirin Co., Ltd., Tokyo, Japan; 3R&D Division, Kyowa Kirin Co., Ltd., Tokyo, Japan; 4Division of Nephrology, Endocrinology, and Metabolism, Department of Internal Medicine, Tokai University School of Medicine, Kanagawa, Japan; 5Division of Nephrology, Department of Medicine, Showa University School of Medicine, Tokyo, Japan
Correspondence: Takashi Shigematsu
Department of Nephrology, Wakayama Medical University, 811-1 Kimiidera, Wakayama 641-8509, Japan
Tel +81-73-441-0638
Fax +81-73-441-0639
Email [email protected]
Purpose: Evocalcet is a novel oral calcimimetic drug that has demonstrated similar efficacy to cinacalcet in regulating serum parathyroid hormone (PTH), calcium, and phosphate levels, with fewer upper gastrointestinal tract-related adverse drug reactions (ADRs) in patients with secondary hyperparathyroidism undergoing hemodialysis in Japan. We investigated the efficacy and safety of once-daily oral evocalcet under different dialysate calcium concentrations.
Patients and Methods: A post hoc analysis by dialysate calcium concentration (2.5, 2.75, and 3.0 mEq/L) was performed using data from a previous Phase 3 study that included cinacalcet as an active control. Efficacy endpoints were the proportion of patients who achieved the target intact PTH levels of ≥ 60 and ≤ 240 pg/mL between Week 28 and Week 30; time-course changes in serum intact PTH; calcium and phosphorus levels, bone turnover markers, and fibroblast growth factor 23 (FGF23) over the 30-week study period. Safety endpoints were overall ADRs and hypocalcemia- and upper gastrointestinal tract-related ADRs.
Results: A total of 634 patients were included in the analysis. Levels of intact PTH, calcium, phosphate, bone turnover markers, and FGF23 showed improvement in all sub-groups, irrespective of dialysate calcium concentration. The incidence of upper gastrointestinal tract-related ADRs was significantly lower in the evocalcet group than the cinacalcet group with dialysate calcium concentrations of 2.75 and 3.0 mEq/L (p< 0.05 for both concentrations).
Conclusion: Evocalcet was effective and safe in regulating the levels of serum intact PTH, calcium, and phosphate in patients with secondary hyperparathyroidism undergoing hemodialysis, irrespective of dialysate calcium concentration.
Keywords: hypocalcemia, intact parathyroid hormone, oral calcimimetic, post hoc analysis, upper gastrointestinal tract
Introduction
Secondary hyperparathyroidism frequently develops in patients with severe chronic kidney disease (CKD) undergoing hemodialysis, and is characterized by the increased synthesis and secretion of parathyroid hormone (PTH)1–4 that can lead to mineral and bone disorders (MBDs), and the development of bone lesions and life-long effects through the calcification of soft tissues such as blood vessels.5 It is therefore clear that maintaining a balance in the levels of phosphate, calcium, and PTH is critical in patients with secondary hyperparathyroidism.6 The Japanese Society for Dialysis Therapy recommends target ranges for serum PTH, calcium, and phosphate levels in its clinical practice guideline for the management of CKD-MBDs, including secondary hyperparathyroidism.7
Calcium-sensing receptors detect extracellular calcium concentrations. Upon binding to these receptors, calcium-sensing receptor positive allosteric modulators suppress PTH secretion and are therefore widely used as therapeutic agents for secondary hyperparathyroidism. Cinacalcet, the first calcium-sensing receptor positive allosteric modulator, demonstrated a strong inhibitory effect on PTH secretion without elevating the serum calcium level and increased the proportion of patients achieving the target PTH, calcium, and phosphate concentrations.8
Similar to cinacalcet, the novel positive allosteric modulator evocalcet decreases serum PTH and calcium levels.9–14 Furthermore, a previous phase 3 study showed that the incidence of adverse drug reactions (ADRs) of upper gastrointestinal disorders was less frequent with evocalcet compared with cinacalcet.15 Therefore, evocalcet may be beneficial for patients receiving cinacalcet when the occurrence of gastrointestinal ADRs causes lower adherence and insufficient dosages.
Another factor to be considered in the regulation of serum calcium concentration is the dialysate calcium concentration used for maintenance dialysis. Dialysate calcium concentration at 3.5 mEq/L was associated with increased all-cause mortality and cardiovascular-related hospitalization in patients undergoing hemodialysis.16,17 Therefore, the Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group recommends a calcium concentration in dialysate of between 2.5 and 3.0 mEq/L.18 Although one dialysate calcium concentration of 2.75 mEq/L became available in 1993 in Japan,19 any dialysate calcium concentrations below 3.0 mEq/L were unlikely to have a clinically significant effect on patient prognosis.20 Unlike in other countries, where single-patient dialysis fluid delivery systems have been used based on each patient’s condition, a central dialysis fluid delivery system has been adopted for the past 45 years in Japan with the dialysate calcium concentration determined based on the policy of the medical facility.21 Because evocalcet and cinacalcet both lower the serum calcium concentration, their efficacy and safety may be affected by the concentration of dialysate calcium.
This study therefore investigated the efficacy and safety of treatment with once-daily oral evocalcet for 30 weeks in patients with secondary hyperparathyroidism receiving hemodialysis by stratifying the previous phase 3 results by dialysate calcium concentration.
Materials and Methods
Study Design
This study (ClinicalTrials.gov, NCT02549391 and JAPIC, JapicCTI-153013) was a post hoc analysis of the previous phase 3, randomized, double-blind, intra-subject dose-adjustment, parallel-group study of evocalcet with cinacalcet as an active control.15 In brief, the previous study consisted of a 28-week dose-adjustment period followed by a 2-week evaluation period. All patients received daily evocalcet (starting dose of 1 mg for patients with intact PTH <500 pg/mL or 2 mg for ≥500 pg/mL, up to 8 mg from Week 3 to Week 28, and a fixed dose until the end of the study period) or cinacalcet (starting dose of 25 mg, up to 100 mg from Week 3 to Week 28, and a fixed dose until the end of the study period) for 30 weeks to achieve an intact PTH level ≥60 and ≤240 pg/mL. Changes in prescribed dialysis conditions, including dialysate calcium concentration, dialyzer, dialysis time, and number of dialysis sessions per week, as well as initiation of or changes in preparation, dose, and dosing regimen of vitamin D receptor activator (VDRA) medications or derivatives were prohibited from 2 weeks prior to screening to the end of the study. Any changes in preparation, dose, and dosing regimen of phosphate binder and calcium preparation were prohibited from 2 weeks prior to screening until Week 0.
The dose was increased on the day of dialysis after the longest interval between dialysis sessions if all of the following dose increase criteria were met: current dose had been maintained for ≥3 weeks and intact PTH level >240 pg/mL at the last scheduled visit prior to a dose change. However, even where the intact PTH level was ≤240 pg/mL, the investigator determined the dose increase to ensure an intact PTH level of approximately 150 pg/mL; serum corrected calcium level at the last scheduled visit before the dose change was ≥8.4 mg/dL; and the investigator determined that a dose increase would not interfere with the safety of the patient. The dose was reduced if intact PTH level decreased to <60 pg/mL or the investigator determined that the dose should be reduced because of an adverse event. The dose of evocalcet was increased or reduced in 1-mg increments, while cinacalcet was increased in 25-mg and decreased in 25-mg or 12.5-mg increments.
Patient Population
Patients with secondary hyperparathyroidism who were receiving hemodialysis 3 times a week, were ≥20 years of age, and had a mean intact PTH >240 pg/mL and corrected serum calcium ≥9.0 mg/dL were included in the study. Major exclusion criteria included treatment with cinacalcet ≤2 weeks before screening; change in dose or dosing regimen of VDRA or its derivatives, phosphate binder or calcium preparation, or initiation of treatment with such drugs ≤2 weeks before screening; change in dialysate calcium concentration, dialyzer, dialysis time, or number of dialysis sessions per week ≤2 weeks before screening; treatment with bisphosphonates, denosumab, teriparatide, and parathyroidectomy and/or parathyroid intervention ≤24 weeks before screening.
Stratified Analysis
The previous phase 3 data were stratified by dialysate calcium concentration (2.5: <2.625 mEq/L, 2.75: ≥2.625 and <2.875 mEq/L, and 3.0: ≥2.875 mEq/L) in the evocalcet and cinacalcet treatment arms. Efficacy endpoints were mean intact PTH level over the study period and mean percent change in intact PTH level from baseline throughout the study period; number and percentage of patients with mean intact PTH level ≥60 and ≤240 pg/mL in Week 28 to Week 30 of the evaluation period; and change in the level of corrected serum calcium; serum phosphate; bone turnover markers as bone-specific alkaline phosphatase (BAP), tartrate-resistant acid phosphatase-5b (TRACP-5b), and procollagen type I N-terminal pro-peptide (PINP); intact fibroblast growth factor 23 (FGF23); mean daily dose for each study drug; and the conversion ratio between evocalcet and cinacalcet from baseline to the end of the study period. Safety was evaluated by ADRs, including hypocalcemia- and upper gastrointestinal tract-related ADRs.
Statistical Analysis
Efficacy was evaluated in the per protocol set, which included enrolled patients who received at least one dose of any study treatment and had at least one intact PTH measurement after the study began but excluded those who did not meet any of the inclusion criteria or fell under any exclusion criterion; had drug compliance <70% out of 28 weeks of dispensed drug; received prohibited concomitant medications or therapy such as cinacalcet, bisphosphonates, denosumab, teriparatide, parathyroidectomy, and/or parathyroid intervention or peritoneal dialysis; missed intact PTH measurement at ≥2 of 3 time points between Week 28 and Week 30; or had a protocol deviation that might have affected the efficacy evaluation. Safety was evaluated in the safety analysis set, which included patients who enrolled in the study and received at least one dose of any study treatment.
Unless otherwise specified, categorical data were summarized using frequencies and percentages, and continuous data were summarized using descriptive statistics consisting of the number of patients, mean, standard deviation, median, and interquartile range. For the categorical, the Chi-square test was used, and for continuous data, the Kruskal–Wallis test and analysis of variance were used based on the data distribution.
The proportion of patients who achieved the recommended mean intact PTH level of ≥60 and ≤240 pg/mL7 between Week 28 and Week 30 were calculated for each sub-group, and difference in achievement ratio and 95% confidence interval (CI) were analyzed by analysis of variance.
All ADRs that occurred after the start of study treatment were summarized according to the MedDRA version 19.0 and the incidence rate was calculated by sub-groups and treatment arms. For hypocalcemia-related ADRs, corrected calcium decreased, blood calcium decreased, and hypocalcemia by preferred term, as well as a combination of all three were summarized and incidence rates were obtained by sub-group and treatment arm. The same analysis was used for upper gastrointestinal tract-related ADRs that included nausea, vomiting, abdominal discomfort, abdominal distension, and decreased appetite.
Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC), and two-tailed p-values of <0.05 were considered statistically significant.
Results
The previous phase 3 study was conducted at 89 sites in Japan from October 2015 to November 2016. The present analysis included 519 patients in the per protocol set and 634 patients in the safety analysis set. A similar number of patients were included in each sub-group between the evocalcet and cinacalcet arms, there were no significant differences in baseline characteristics between the two arms, except in cinacalcet use prior to screening and VDRA use at baseline among the sub-groups in the cinacalcet arm (Table 1).
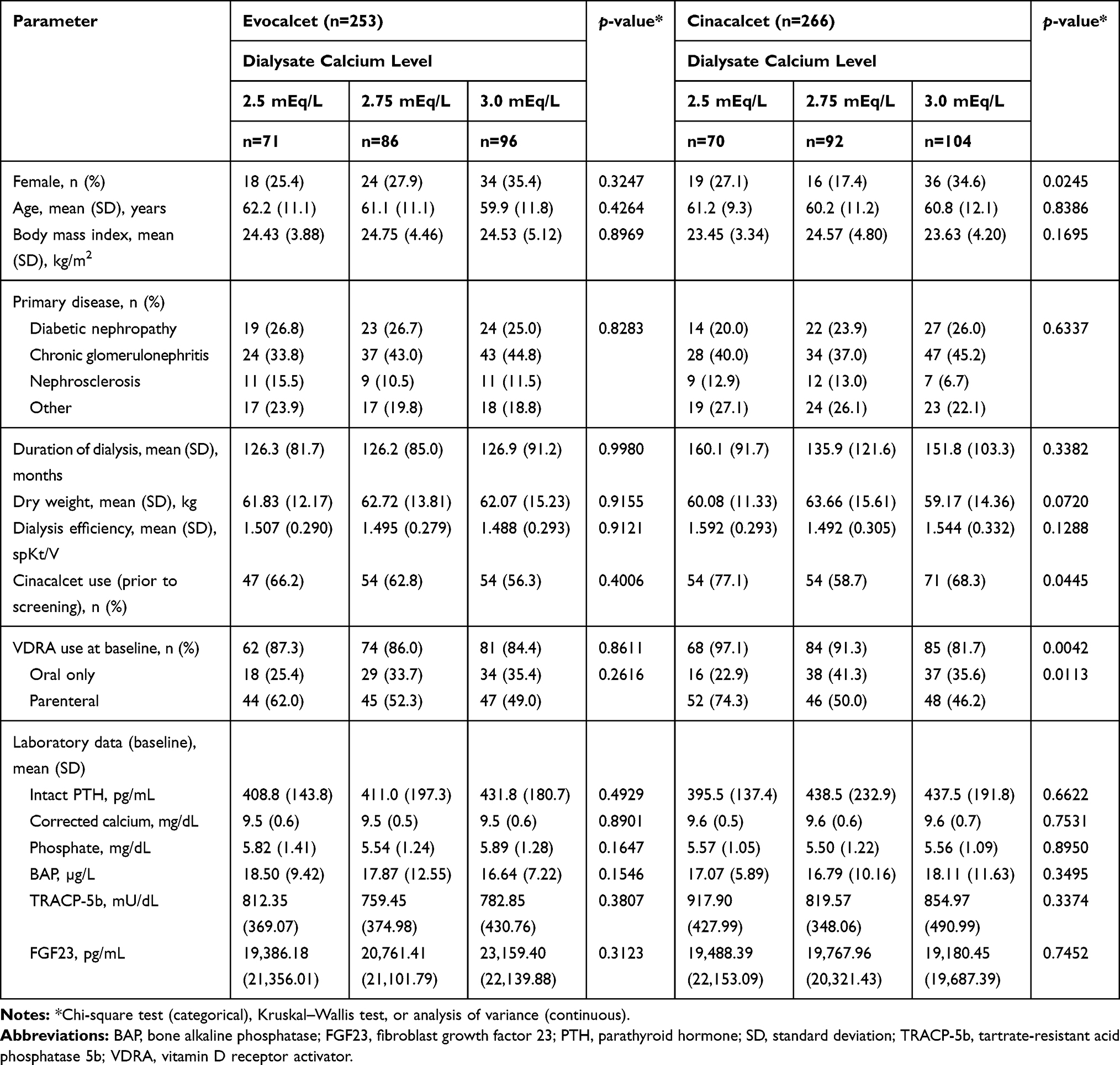 |
Table 1 Patient Baseline Characteristics by Dialysate Calcium Level |
Efficacy
Mean intact PTH levels gradually decreased over the 28-week dose-adjustment period and 2-week evaluation period in all sub-groups of both arms (Figure 1A). Similarly, the mean percent changes in the intact PTH levels from the baseline showed approximately a 50% reduction by the evaluation period (Figure 1B).
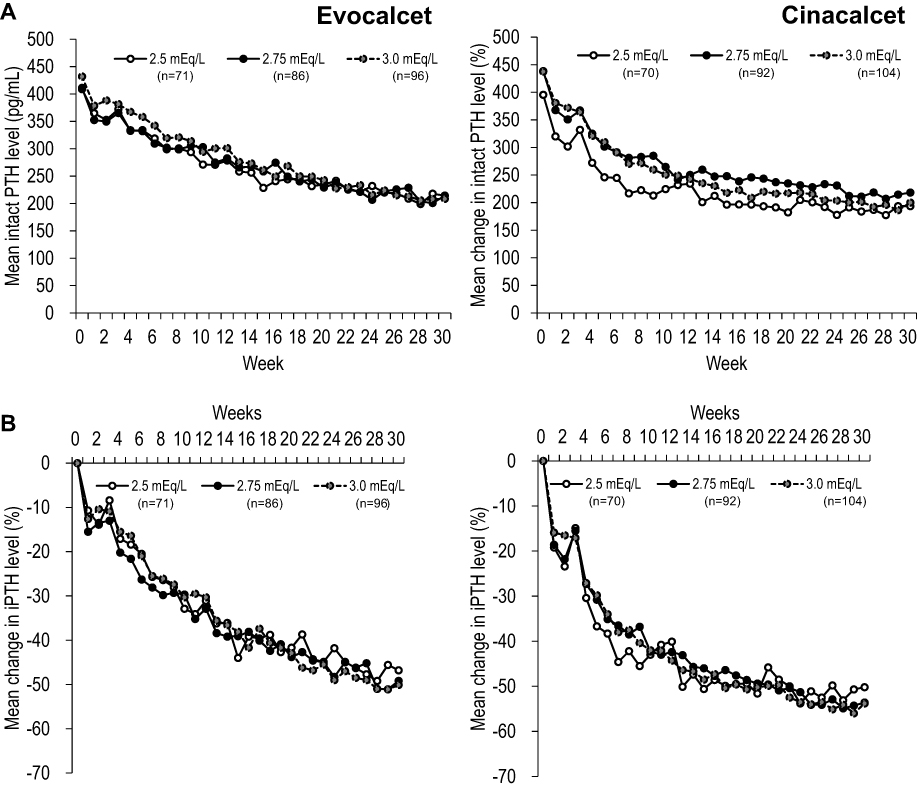 |
Figure 1 Trends in mean intact PTH level (A) and mean percent change in intact PTH level (B) by dialysate calcium concentration in patients treated with evocalcet and cinacalcet.Abbreviation: PTH, parathyroid hormone. |
During the evaluation period, no significant difference was found among the sub-groups of both treatment arms in the number and percentage of patients who achieved the mean intact PTH level of ≥60 pg/mL and ≤240 pg/mL (71.8% to 79.3%), irrespective of dialysate calcium concentration (Supplementary Table S1).
The daily doses of evocalcet and cinacalcet started to increase from Week 3. Although the daily evocalcet dose continued to increase until Week 20, the daily cinacalcet dose stabilized by Week 12. The ratio subsequently decreased, approaching an equal conversion dose of 12.5 by Week 20 (Supplementary Figure S1).
The mean level of corrected serum calcium decreased to a similar extent in the 3 sub-groups of each arm (Figure 2A). In the cinacalcet arm, the level increased slightly up to Week 30. The mean level of serum phosphorus decreased slightly over the 30 weeks in all sub-groups of both arms (Figure 2B).
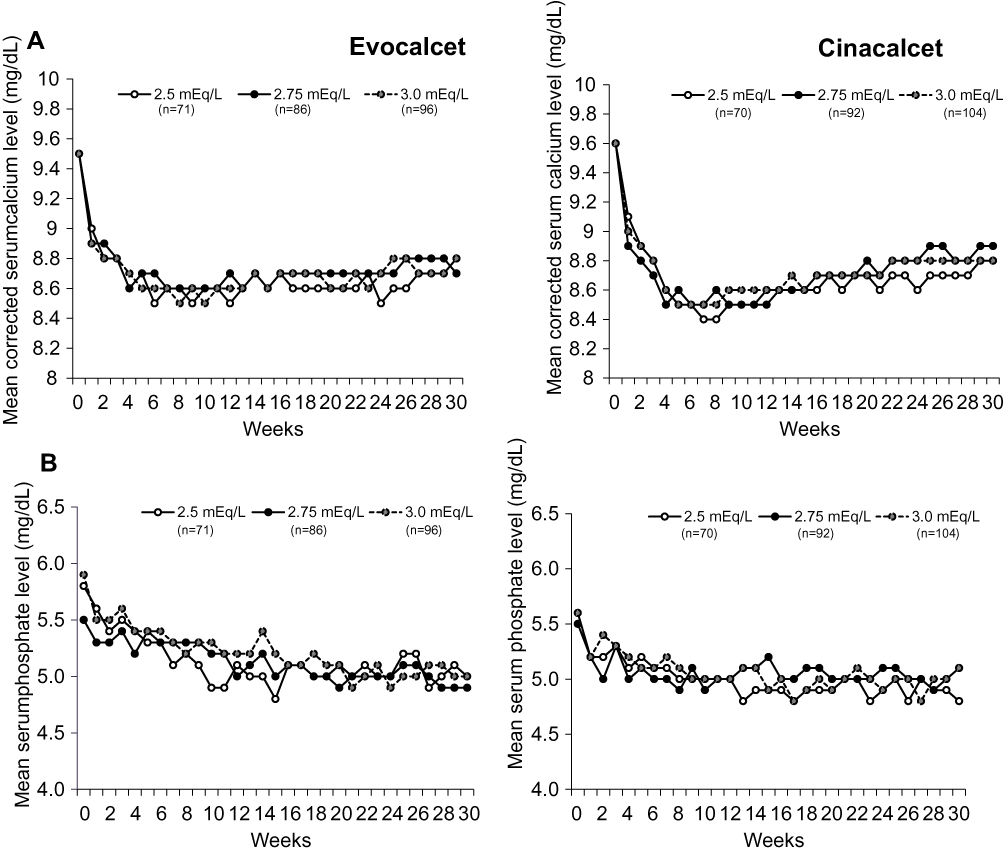 |
Figure 2 Trends in mean serum corrected calcium (A) and phosphate (B) level by dialysate calcium concentration in patients treated with evocalcet and cinacalcet. |
The levels of bone metabolic markers showed similar trends in both arms irrespective of dialysate calcium concentration. The mean BAP level increased slightly after the start of the treatment, subsequently decreased, and returned to the baseline level by Week 30 in all sub-groups of both arms (Supplementary Figure S2A and Supplementary Table S2). The mean TRACP-5b and PINP levels in all sub-groups of both arms were similarly decreased throughout the study period after the initiation of treatment (Supplementary Figure S2B and Supplementary Table S2).
The median level of intact FGF23 decreased over the study period with some variability among the sub-groups of both treatment arms although the differences were not significant (Supplementary Figure S2C and Supplementary Table S2).
Safety
The incidence of ADRs in the sub-groups of the evocalcet arm was slightly lower than that in the cinacalcet arm (Supplementary Table S3), but was similar among the sub-groups in each arm. Hypocalcemia-related ADRs such as corrected calcium decreased and blood calcium decreased were marginally less frequent in the evocalcet arm than in the cinacalcet arm, but no clear difference was observed among the sub-groups within each arm (Figure 3A). The upper gastrointestinal tract-related ADRs occurred at similar frequencies among the sub-groups in each arm, irrespective of dialysate calcium concentration. However, a significantly lower incidence rate was observed in the evocalcet arm compared with the cinacalcet arm under dialysate calcium concentrations of 2.75 mEq/L (p=0.0053) and 3.0 mEq/L (p=0.0429) (Figure 3B).
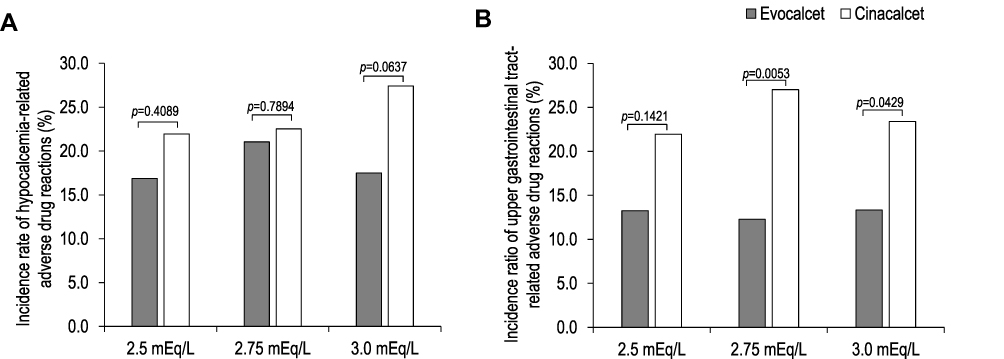 |
Figure 3 Incidence of hypocalcemia- (A) and upper gastrointestinal tract-related (B) adverse drug reactions by dialysate calcium concentration in patients treated with evocalcet and cinacalcet. Chi-square test. |
Discussion
Dialysate calcium concentration is a contributing factor to the levels of serum PTH, calcium, and phosphate in patients undergoing hemodialysis.22,23 Despite concerns that dialysate calcium concentration can affect the efficacy of calcimimetics, the present results showed that evocalcet and cinacalcet are effective and safe, irrespective of dialysate calcium concentration.
The efficacy and safety of treatment with once-daily oral evocalcet for 30 weeks15 and 52 weeks24 were investigated in the previous phase 3 studies in patients with secondary hyperparathyroidism receiving hemodialysis. The results of those studies demonstrated the noninferiority of evocalcet to cinacalcet in suppressing intact PTH levels, with a lower incidence of gastrointestinal tract-related ADRs. The results of the present post hoc analysis are consistent with those of the previous results, indicating that similar efficacy and safety can be expected for evocalcet with dialysate calcium concentrations ranging from 2.5 to 3.0 mEq/L for up to 30 weeks.
A potential negative impact of dialysate calcium concentration on disease control has been addressed in a previous study, in which a decrease in dialysate calcium concentration from 3.0 mEq/L to 2.5 mEq/L had a negative impact on MBD parameters and increased PTH concentration.25 In contrast, our present results showed that evocalcet and cinacalcet were effective in achieving the target intact PTH levels in 70% of patients for all dialysate calcium concentrations, suggesting that although serum calcium concentration can affect the PTH level, dialysate calcium concentrations in the range of 2.5 to 3.0 mEq/L are unlikely to affect the efficacy of evocalcet or cinacalcet.
In this study, the level of BAP increased transiently but returned to the baseline level by Week 30, while the level of TRACP-5b gradually decreased over the 30-week study period. These findings are consistent with those observed following treatment with other calcimimetics.26,27 Although further studies are needed, evocalcet and cinacalcet appear to improve bone metabolism with dialysate calcium concentrations of 2.5 to 3.0 mEq/L.
The present results showed that the FGF23 level decreased to approximately 50% in all sub-groups of each arm, which is consistent with the EVOLVE study of cinacalcet.28 However, the FGF23 levels were somewhat variable, which is consistent with previous studies,24,26,27 indicating that other factors, likely uncontrolled for in the present analysis and in previous studies, may be involved in the regulation of serum intact FGF23 level. Given the accumulating evidence to suggest a significant association between elevated FGF23 and cardiovascular disease,28–30 the decreasing trend in FGF23 level observed after treatment with evocalcet and cinacalcet may be a beneficial effect.
Given the known association between secondary hyperparathyroidism in patients receiving hemodialysis and MBDs, all of which contribute to cardiovascular disease and mortality, calcimimetics, especially evocalcet, which exerts its efficacy at lower doses than cinacalcet with a lower incidence of developing upper digestive tract-related ADRs, may confer a clinical benefit as well as optimal control of mineral and bone metabolism.
A limitation of this study is that the efficacy and safety of evocalcet and cinacalcet by dialysate calcium concentration were assessed only for 30 weeks. Given that patients with severe CKD undergo hemodialysis for longer than 30 weeks, and that their prognosis with respect to cardiovascular disease and MBDs is dependent on the calcium balance,6 further studies are required to understand how different dialysate calcium concentrations affect the outcome of long-term treatment with evocalcet and cinacalcet. Another limitation of this study is the inclusion of a specific patient population in Japan. Because evocalcet was developed and first approved in Japan, the present analysis may represent the first validation of the efficacy and safety of evocalcet irrespective of dialysate calcium concentration. However, it should be noted that the PTH level in Japan is controlled at a lower range than that recommended by the KDIGO guidelines18 and, therefore, the PTH levels in patients in Japan are controlled lower than those in other regions.31
A further limitation is that patient characteristics were not controlled among the sub-groups. In addition, because of the small sample size in each sub-group of both arms, the study might have insufficient power to compare efficacy or safety among the sub-groups. However, since the present results were consistent with those of the previous phase 3 study, evocalcet and cinacalcet appear to be effective and safe when used alongside all dialysate calcium concentrations evaluated in this study.
Finally, patients in this study were not permitted to change the dialysate calcium concentration and dose or dosing regimen of any VDRA or its derivative during the evaluation period. However, changes in the administration of calcium-based/non-calcium-based phosphate binders were allowed; therefore, any effects related to these medications cannot be ruled out.
Conclusion
In summary, evocalcet and cinacalcet were effective in controlling the levels of serum intact PTH, corrected calcium and phosphate, irrespective of dialysate calcium concentration. Overall, no important safety concerns were raised, and the incidence of upper gastrointestinal tract-related ADRs was lower in the evocalcet arm compared with the cinacalcet arm. These findings demonstrate that evocalcet and cinacalcet are effective and safe when used alongside dialysate calcium concentrations of 2.5 to 3.0 mEq/L in patients with secondary hyperparathyroidism undergoing hemodialysis.
Abbreviations
ADR, adverse drug reaction; BAP, bone-specific alkaline phosphatase; CI, confidence interval; CKD, chronic kidney disease; FGF23, fibroblast growth factor 23; KDIGO, Kidney Disease: Improving Global Outcomes; MBD, mineral bone disorder; PINP, procollagen type I N-terminal pro-peptide; PTH, parathyroid hormone; TRACP-5b, tartrate-resistant acid phosphatase-5b; VDRA, vitamin D receptor activator.
Data Sharing Statement
Data sharing is not available as all the relevant data are included in the manuscript and its Supplementary materials.
Ethics and Consent Statements
The study was approved by the ethics committee at each study site, and was carried out in accordance with the principles of the Declaration of Helsinki and in compliance with the Pharmaceuticals, Medical Devices, and Other Therapeutic Products Act, Good Clinical Practice (Ministry of Health and Welfare Ordinance No. 28 dated March 27, 1997), and the partial revision of the Ordinance. Signed informed consent was obtained from all patients before the study.
Acknowledgments
The authors thank all the collaborators for their participation in the study (see Supplementary List of collaborators), Ms. Shiori Yasui, Mr. Taichi Mizogui and Dr. Shinjo Yada of A2 Healthcare Corporation for statistical analysis, and ASCA Corporation for medical writing assistance.
Author Contributions
TS was responsible for writing the manuscript and contributed to the research and data analysis. SA, YE, and TK contributed to the study design, data analysis, and manuscript preparation. MF and TA had overall responsibility for the study, and contributed to the study design, research, analysis, and manuscript preparation. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by Kyowa Kirin Co., Ltd. (KKC).
Disclosure
TS received consulting fees from KKC, Ono Pharmaceutical, Taisho Toyama Pharmaceutical, Fuji Pharma, and FUSO pharmaceutical industries, and lecture fees from KKC, Chugai Pharmaceutical, Bayer, Kissei Pharmaceutical, Torii Pharmaceutical, Ono Pharmaceutical, and FUSO pharmaceutical industries. SA, YE, and TK are employees of KKC. MF received consulting fees from KKC and Ono Pharmaceutical; lecture fees from KKC, Bayer, Torii Pharmaceutical, and Ono Pharmaceutical; and grants from KKC and Bayer. TA received consulting fees from KKC, Astellas Pharma, Bayer, Fuso Pharmaceutical, Japan Tobacco, Ono Pharmaceutical, Sanwa Chemical, Otsuka, GSK, and NIPRO, and lecture fees from KKC, Chugai Pharmaceutical, Bayer, Kissei Pharmaceutical, Torii Pharmaceutical, and Ono Pharmaceutical. The authors report no other conflicts of interest in this work.
References
1. Cunningham J, Locatelli F, Rodriguez M. Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options. Clin J Am Soc Nephrol. 2011;6:913–921. doi:10.2215/CJN.06040710
2. Komaba H, Kakuta T, Fukagawa M. Diseases of the parathyroid gland in chronic kidney disease. Clin Exp Nephrol. 2011;15:797–809. doi:10.1007/s10157-011-0502-5
3. Ketteler M, Block GA, Evenepoel P, et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD) guideline update: what’s changed and why it matters. Kidney Int. 2017;92:26–36. doi:10.1016/j.kint.2017.04.006
4. Rodelo-Haad C, Rodríguez-Ortiz ME, Martin-Malo A, et al. Phosphate control in reducing FGF23 levels in hemodialysis patients. PLoS One. 2018;13:e0201537. doi:10.1371/journal.pone.0201537
5. Moe S, Drüeke T, Cunningham J, et al. Definition, evaluation, and classification of renal osteodystrophy: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006;69:1945–1953. doi:10.1038/sj.ki.5000414
6. van der Sande FM, Ter Meulen KJA, Kotanko P, Kooman JP. Dialysate calcium levels: do they matter? Blood Purif. 2019;47:230–235. doi:10.1159/000494584
7. Fukagawa M, Yokoyama K, Koiwa F, et al. Clinical practice guideline for the management of chronic kidney disease-mineral and bone disorder. Ther Apher Dial. 2013;17:247–288.
8. Pereira L, Meng C, Marques D, Frazão JM. Old and new calcimimetics for treatment of secondary hyperparathyroidism: impact on biochemical and relevant clinical outcomes. Clin Kidney J. 2018;11:80–88. doi:10.1093/ckj/sfx125
9. Akizawa T, Shimazaki R, Shiramoto M, Fukagawa M; Evocalcet Study Group. Pharmacokinetics, pharmacodynamics, and safety of the novel calcimimetic agent evocalcet in healthy Japanese subjects: first-in-human Phase I study. Clin Drug Investig. 2018;38:945–954. doi:10.1007/s40261-018-0687-4
10. Akizawa T, Ikejiri K, Kondo Y, Endo Y, Fukagawa M. Evocalcet, a new oral calcimimetic for dialysis patients with secondary hyperparathyroidism. Ther Apher Dial. 2019. doi:10.1111/1744-9987.13434
11. Shigematsu T, Shimazaki R, Fukagawa M, Akizawa T. Pharmacokinetics of evocalcet in secondary hyperparathyroidism patients receiving hemodialysis: first-in-patient clinical trial in Japan. Clin Pharmacol. 2018;10:101–111. doi:10.2147/CPAA.S171044
12. Shigematsu T, Shimazaki R, Fukagawa M, Akizawa T; Evocalcet Study Group. Pharmacodynamics of evocalcet for secondary hyperparathyroidism in Japanese hemodialysis patients. Clin Exp Nephrol. 2019;23:258–267. doi:10.1007/s10157-018-1635-6
13. Tsuruya K, Shimazaki R, Fukagawa M, Akizawa T; Evocalcet Study Group. Efficacy and safety of evocalcet in Japanese peritoneal dialysis patients. Clin Exp Nephrol. 2019;23:739–748. doi:10.1007/s10157-019-01692-y
14. Kawata T, Tokunaga S, Murai M, et al. A novel calcimimetic agent, evocalcet (MT-4580/KHK7580), suppresses the parathyroid cell function with little effect on the gastrointestinal tract or CYP isozymes in vivo and in vitro. PLoS One. 2018;13:e0195316. doi:10.1371/journal.pone.0195316
15. Fukagawa M, Shimazaki R, Akizawa T; Evocalcet study group. Head-to-head comparison of the new calcimimetic agent evocalcet with cinacalcet in Japanese hemodialysis patients with secondary hyperparathyroidism. Kidney Int. 2018;94:818–825. doi:10.1016/j.kint.2018.05.013
16. Young EW, Albert JM, Satayathum S, et al. Predictors and consequences of altered mineral metabolism: the dialysis outcomes and practice patterns study. Kidney Int. 2005;67:1179–1187. doi:10.1111/j.1523-1755.2005.00185.x
17. Kim HW, Kim SH, Kim YO, et al. Impact of dialysate calcium concentration on clinical outcomes in incident hemodialysis patients. Medicine (Baltimore). 2015;94:e1694. doi:10.1097/MD.0000000000001694
18. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int. 2009;76(Suppl 113):S1–130.
19. Sakai Y, Otsuka T, Ohno D, Murasawa T, Sakai S, Tsuruoka S. Clinical benefit of the change of dialysate calcium concentration from 3.0 to 2.75 mEq/L. Ther Apher Dial. 2014;18:181–184. doi:10.1111/1744-9987.12099
20. Iseki K, Henn LL, Nomura T, et al. Dialysate calcium concentration below 3.0 mEq/L is not associated with improved outcomes in the Japanese Dialysis Outcomes and Practice Patterns Study. Nephron. 2018;140:240–248. doi:10.1159/000493470
21. Kawanishi H, Moriishi M, Takahashi N, Tsuchiya S. The central dialysis fluid delivery system (CDDS): is it specialty in Japan? Ren Replace Ther. 2016;2:1. doi:10.1186/s41100-016-0016-4
22. Matsuura A, Inaguma D, Itawaki D, et al. The change of the dialysate calcium concentration from 3.0 to 2.75 mEq/L did not affect the serum PTH level in hemodialysis patients. J Jpn Soc Dial Ther. 2012;45:873–880. doi:10.4009/jsdt.45.873.
23. Shinkai N, Yanase M, Kyoda Y, et al. Effects of dialysate calcium concentration on calcium-phosphorus metabolism in hemodialysis patients. J Jpn Soc Dial Ther. 2010;43:933–938. doi:10.4009/jsdt.43.933.
24. Yokoyama K, Shimazaki R, Fukagawa M, Akizawa T; Evocalcet Study Group. Long-term efficacy and safety of evocalcet in Japanese patients with secondary hyperparathyroidism receiving hemodialysis. Sci Rep. 2019;9:6410. doi:10.1038/s41598-019-42017-z
25. Yokoyama K, Kagami S, Ohkido I, et al. The negative Ca(2+) balance is involved in the stimulation of PTH secretion. Nephron. 2002;92:86–90. doi:10.1159/000064484
26. Susantitaphong P, Vadcharavivad S, Susomboon T, et al. The effectiveness of cinacalcet: a randomized, open label study in chronic hemodialysis patients with severe secondary hyperparathyroidism. Ren Fail. 2019;41:326–333. doi:10.1080/0886022X.2018.1562356
27. Shigematsu T, Fukagawa M, Yokoyama K, et al. Effects of the intravenous calcimimetic etelcalcetide on bone turnover and serum fibroblast growth factor 23: post hoc analysis of an open-label study. Clin Ther. 2018;40:2099–2111. doi:10.1016/j.clinthera.2018.10.016
28. Moe SM, Chertow GM, Parfrey PS, et al. Cinacalcet, fibroblast growth factor-23, and cardiovascular disease in hemodialysis: the Evaluation of Cinacalcet HCl Therapy to Lower Cardiovascular Events (EVOLVE) trial. Circulation. 2015;132:27–39. doi:10.1161/CIRCULATIONAHA.114.013876
29. Gutiérrez OM, Mannstadt M, Isakova T, et al. Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N Engl J Med. 2008;359:584–592. doi:10.1056/NEJMoa0706130
30. Martin A. Bone and heart health in chronic kidney disease: role of dentin matrix protein 1. Curr Opin Nephrol Hypertens. 2019;28:297–303. doi:10.1097/MNH.0000000000000512
31. Tentori F, Wang M, Bieber BA, et al. Recent changes in therapeutic approaches and association with outcomes among patients with secondary hyperparathyroidism on chronic hemodialysis: the DOPPS study. Clin J Am Soc Nephrol. 2015;10:98–109. doi:10.2215/CJN.12941213
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.