")
Back to Journals » Cancer Management and Research » Volume 12
Efficacy and Safety of Cyclin-Dependent Kinases 4 and 6 Inhibitors in HR+/HER2− Advanced Breast Cancer
Authors Xie N, Qin T, Ren W, Yao H, Yu Y, Hong H
Received 18 March 2020
Accepted for publication 30 April 2020
Published 4 June 2020 Volume 2020:12 Pages 4241—4250
DOI https://doi.org/10.2147/CMAR.S254365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Ning Xie,1,* Tao Qin,1,* Wei Ren,1 Herui Yao,1,2 Yunfang Yu,1 Huangming Hong1
1Department of Medical Oncology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Guangzhou, People’s Republic of China; 2Breast Tumor Center, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunfang Yu; Huangming Hong Tel +86-20-34071337
Fax +86-20-81332833
Email [email protected]; [email protected]
Purpose: To assess the efficacy and safety of cyclin-dependent kinases 4 and 6 inhibitors (CDKi) combined with endocrine therapy (ET) in women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer (ABC) and compare the efficacy of different CDKi (palbociclib, ribociclib, or abemaciclib).
Materials and Methods: This study based on randomized Phase 2 or 3 trials of CDKi plus ET compared with placebo plus ET for women with HR+/HER2−ABC and identify relevant randomized clinical trials (RCTs) published prior to February 2020. The primary endpoint was progression-free survival (PFS), the secondary endpoints included overall survival (OS), objective response rate (ORR), clinical benefit response (CBR) and safety. The PROSPERO registry number is 42018081105.
Results: The results from eight trials including 4580 participants were pooled. Evidence indicated that the PFS of CDKi group was significantly prolonged (hazard ratio [HR] 0.55, 95% confidence interval [CI] 0.50– 0.60, P < 0.01) compared with placebo group. The ORR and CBR were better (risk ratio [RR] 1.47, 95% CI 1.30– 1.67, P < 0.01; 1.24, 95% CI 1.15– 1.35, P < 0.01) in the CDKi group. The OS of CDKi group (HR 0.75, 95% CI 0.67– 0.85, P < 0.01) was significantly longer than ET alone. Subgroup analyses confirmed that the benefit was consistent across most subgroups. Subgroup analyses showed no statistically significant difference of PFS among three CDKi: palbociclib vs ribociclib (HR 0.55, 95% CI 0.49– 0.60, P = 0.34), palbociclib vs abemaciclib (HR 0.53, 95% CI, 0.47– 0.59, P = 0.61), and ribociclib vs abemaciclib (HR 0.56, 95% CI, 0.51– 0.62, P = 0.72). Treatment-related grade 3 or 4 hematologic adverse events (AEs) were more frequently in CDKi group.
Conclusion: CDKi combined with ET can significantly prolong PFS and improve the ORR, CBR and OS in patients with HR+/HER2− ABC. However, the advantage of different CDKi has not been established.
Keywords: CDK4/6 inhibitor, HR-positive, HER2-negative, advanced breast cancer
Introduction
Approximately two-thirds of breast cancer patients are hormone receptor (HR)-positive and human epidermal growth factor receptor 2 (HER2)-negative, representing the largest subtype of the disease.1,2 Endocrine therapy (ET) is an important treatment for this subtype; however, ET resistance and disease progression occur in a large subset of these cancers, necessitating the discovery of new approaches.3 The dysregulation of the cell cycle is one of the defined hallmarks of breast cancer.4 Cyclin-dependent kinases (CDKs) play an important role in regulating cell cycle progression,5 and their interaction with cyclin D facilitates the hyperphosphorylation of the retinoblastoma (Rb) gene product, which in turn leads to progression through the G1 checkpoint to the S phase of the cell cycle. This phenomenon has been described in a number of malignant conditions and is associated with endocrine resistance in breast cancer.6
Studies have shown that the direct inhibition of cyclin-dependent kinases 4 and 6 (CDK 4/6) disrupts this pathway and can diminish HR-positive breast cancer cell growth, act synergistically with antiestrogens, and reverse endocrine resistance.7,8 Compared with ET alone, the inhibition of CDK4/6 alongside ET has significantly improved progression-free survival (PFS) in patients with HR-positive, HER2-negative, advanced breast cancer (ABC).9–11 However, there are still some unsolved questions. So far, all three CDK4/6 inhibitors (CDKi) (palbociclib, ribociclib, or abemaciclib) followed parallel developmental strategies, and the absence of head-to-head comparative trials made it difficult to make decisions between the different options. The specific patient populations who can benefit from CDKi and whether CDKi are equally effective in different populations remain unclear. In addition, the adverse events (AEs) of CDKi need to be recognized more systematically. To address these concerns, our meta-analysis attempted to collect comprehensive, high-quality evaluations of the most recent randomized clinical trials (RCTs) to provide the available evidence for the efficacy and safety of CDKi in combination with ET in patients with HR-positive, HER2-negative ABC.
Materials and Methods
Search Strategy
A systematic literature search in PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Web of Science databases was performed to identify relevant RCTs published prior to February 2020. The population, intervention, comparison, and outcome (PICO) strategy was used with the following search terms: CDK4/6 inhibitors, HR-positive, HER2-negative, advanced breast cancer, and randomized clinical trials. No restrictions were imposed regarding sample size, population, language, publication year.
Eligibility and Exclusion Criteria
The Phase II or III RCTs divided patients into CDKi group and placebo group in accordance with the eligibility criteria; original full-text articles that reported one or more of the following outcomes: progression-free survival (PFS), overall survival (OS), objective response rate (ORR), clinical benefit response (CBR), and safety. Further eligibility criteria were that the patients with HR-positive/HER2-negative ABC should have data on menstrual status. The exclusion criteria were as follows: patients who had received previous treatment with a CDKi; inflammatory breast cancer; central nervous system metastases; symptomatic visceral disease or any disease burden; clinically significant cardiac arrhythmias and/or uncontrolled heart disease.
Data Extraction and Quality Assessment
The following baseline characteristics and outcomes were extracted: trial name (including first author, year of publication, and registry numbers for clinical trials), trial phase, number of participants, inclusion criteria, study design, median PFS, and primary and secondary endpoints. In original full-text articles that reported one or more of the following outcomes: PFS, OS, ORR, CBR, and safety, the primary outcome was PFS. The secondary outcomes included ORR (complete response + partial response), CBR (complete response + partial response + stable disease for ≥24 weeks), OS and safety. Measurable disease was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1.
Statistical Analysis
All efficacy endpoints were subjected to intention-to-treat (ITT) analysis when possible. Statistical heterogeneity was evaluated with I2 statistic, and the Mantel Haenszel effects model was applied. A random-effects model was used regardless of whether the heterogeneity was low or high. Dichotomous data were analyzed according to the relative risk (RR). For time-to-event data, estimated hazard ratios (HRs) were pooled using the inverse-variance method. The 95% confidence interval (CI) was reported for all estimates. P < 0.05 was considered statistically significant. We used Review Manager 5.3 to assess the risk of bias in individual studies. Subgroup analyses were then performed to detect the influence of stratification factors and other baseline characteristics. All statistical values are reported with the two-sided P-value. Statistical analyses were performed using R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). To ensure the reliability and accuracy of the results, two authors independently uploaded the data. Any differences of opinion were discussed between the two authors and as needed, a third party was involved until a consensus was reached.
Results
Search Results and Study Characteristics
We qualitatively examined each article according to the eligibility and exclusion criteria and selected eight RCTs with 4580 patients for inclusion in our meta-analysis. The eight RCTs were published between 2015 and 2019.8,10–16 Of the included trials, five trials examined the combination of CDKi and a nonsteroidal aromatase inhibitor (NSAI),8,10–13 three trials examined the combination of CDKi and fulvestrant.14–16 Three trials examined the combination of palbociclib and ET,12–14 three trials examined the combination of ribociclib and ET,8,11,16 and two trials examined the combination of abemaciclib and ET.10,15 The main characteristics of these included studies are listed in Table 1. We applied uniform criteria recommended by the Cochrane Collaboration to evaluate the risk of bias of the RCTs (Figure 1).
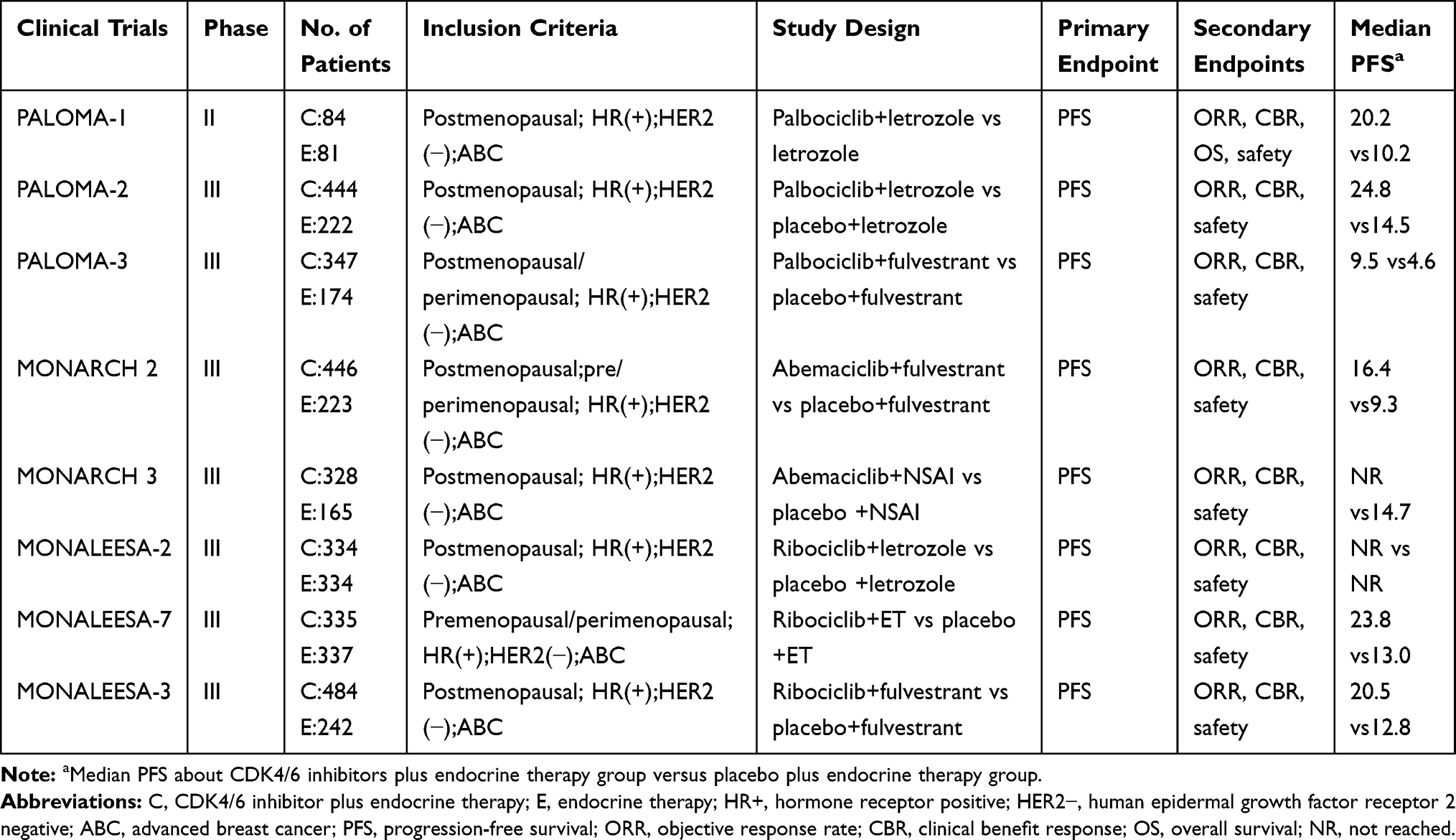 |
Table 1 Baseline Characteristics of the Included Studies |
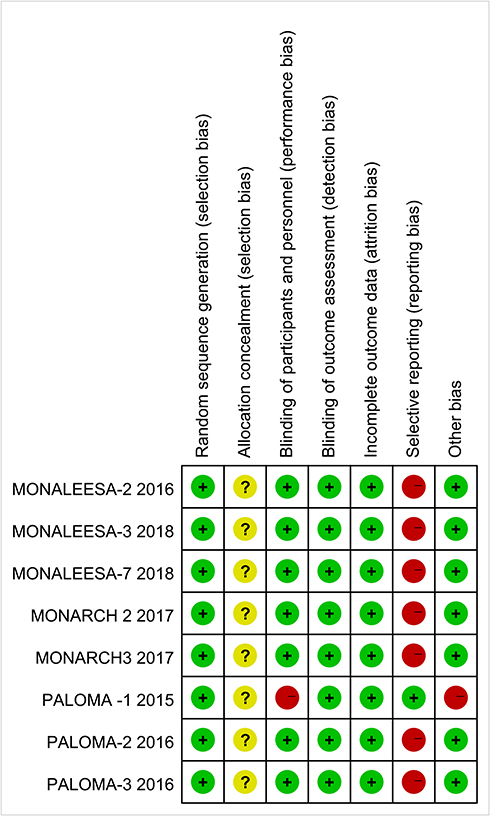 |
Figure 1 Risk of bias summary. |
Primary Endpoint Analysis
The pooled data of our meta-analysis provide evidence that CDKi combined with ET lead to a significantly longer PFS than placebo plus ET (HR 0.55, 95% CI 0.50–0.60, P < 0.01; Figure 2A). In the subgroup analysis for PFS, across all demographic subgroups and patient baseline prognostic factors, a consistent conclusion that CDKi plus ET could decrease the incidence of disease progression or death, except for race. Although White and Asian had a significant decrease in the incidence of disease progression or death with the CDKi plus ET (HR 0.61, 95% CI 0.54–0.68; HR 0.47, 95% CI 0.34–0.64), there was no significant statistical difference in other race category (HR 0.44, 95% CI 0.16–1.20). All subgroup analyses of PFS confirmed that CDKi plus nonsteroidal aromatase inhibitor (NSAIs) group could decrease the incidence of disease progression or death. However, for Asian and other race category, there was no significant decrease in the incidence of disease progression or death with the treatment of CDKi plus fulvestrant (Table 2).
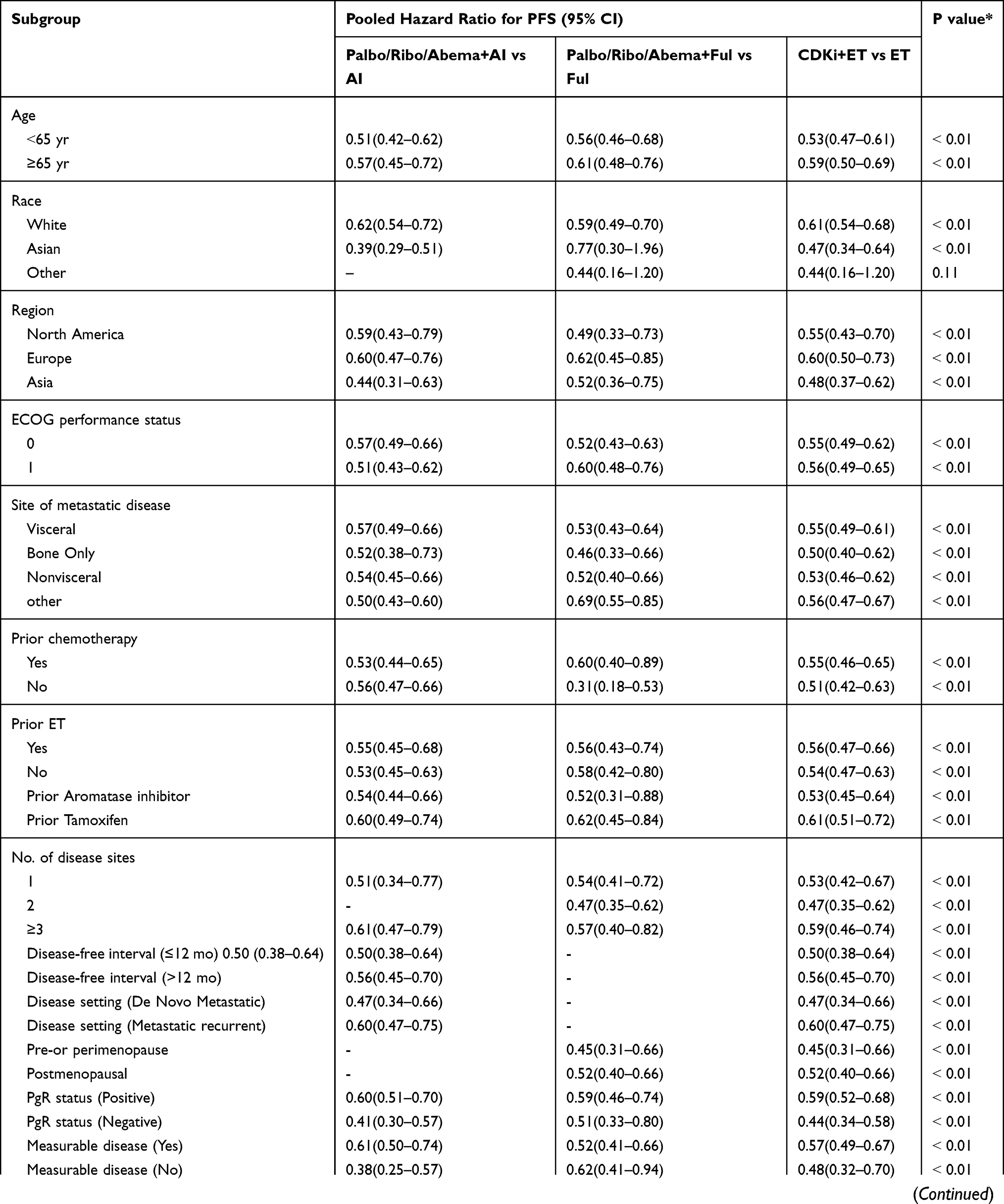 |
Table 2 Subgroup Analysis of Progression-Free Survival |
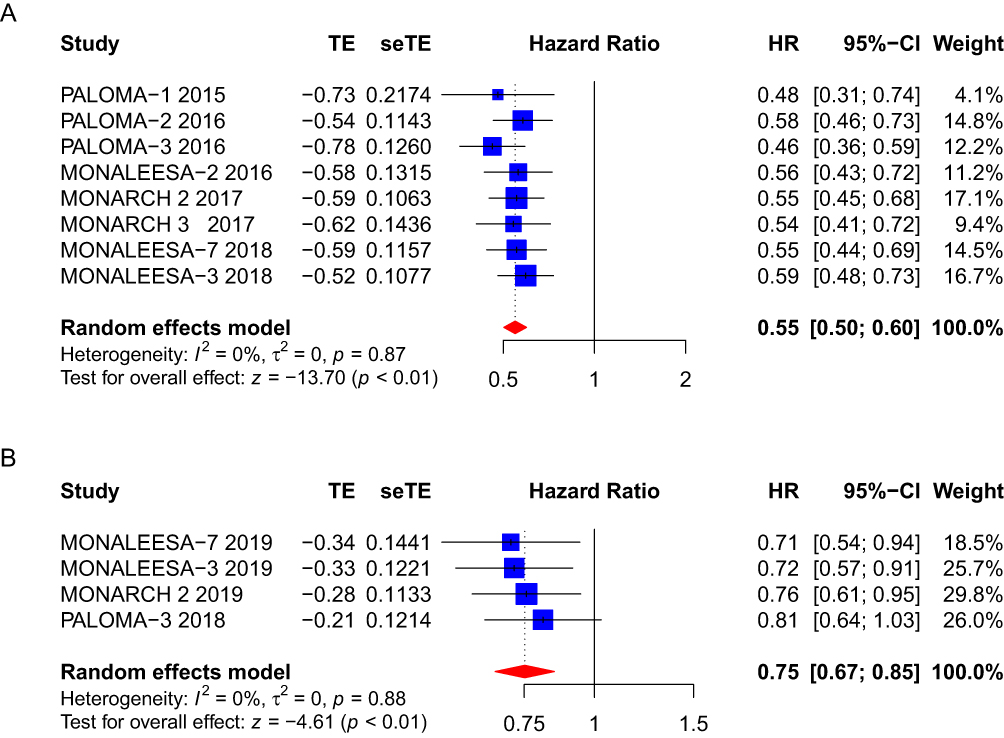 |
Figure 2 Forest plot of comparison: (A) progression-free survival; (B) overall survival. |
Secondary Endpoint Analysis
The ORR of the patients who had been randomly assigned to the CDKi group was higher than that of the placebo group (RR 1.48, 95% CI 1.30–1.68, P < 0.01). In patients with measurable disease, the CDKi group had a higher ORR than the placebo group (RR 1.47, 95% CI 1.30–1.67, P<0.01). Patients in the CDKi group had a greater CBR to treatment than patients in the placebo group, both in the ITT population (RR 1.21, 95% CI, 1.12–1.30, P<0.01) and in the population with measurable disease (RR 1.24, 95% CI 1.15–1.35, P<0.01) (Table 3). The OS benefit of CDKi plus ET has been compared in MONALEESA-7, MONALEESA-3, MONARCH-2, and PALOMA-3 trials. CDKi plus ET showed significantly longer OS than ET alone (HR for death 0.75, 95% CI 0.67–0.85, P<0.01; Figure 2B).
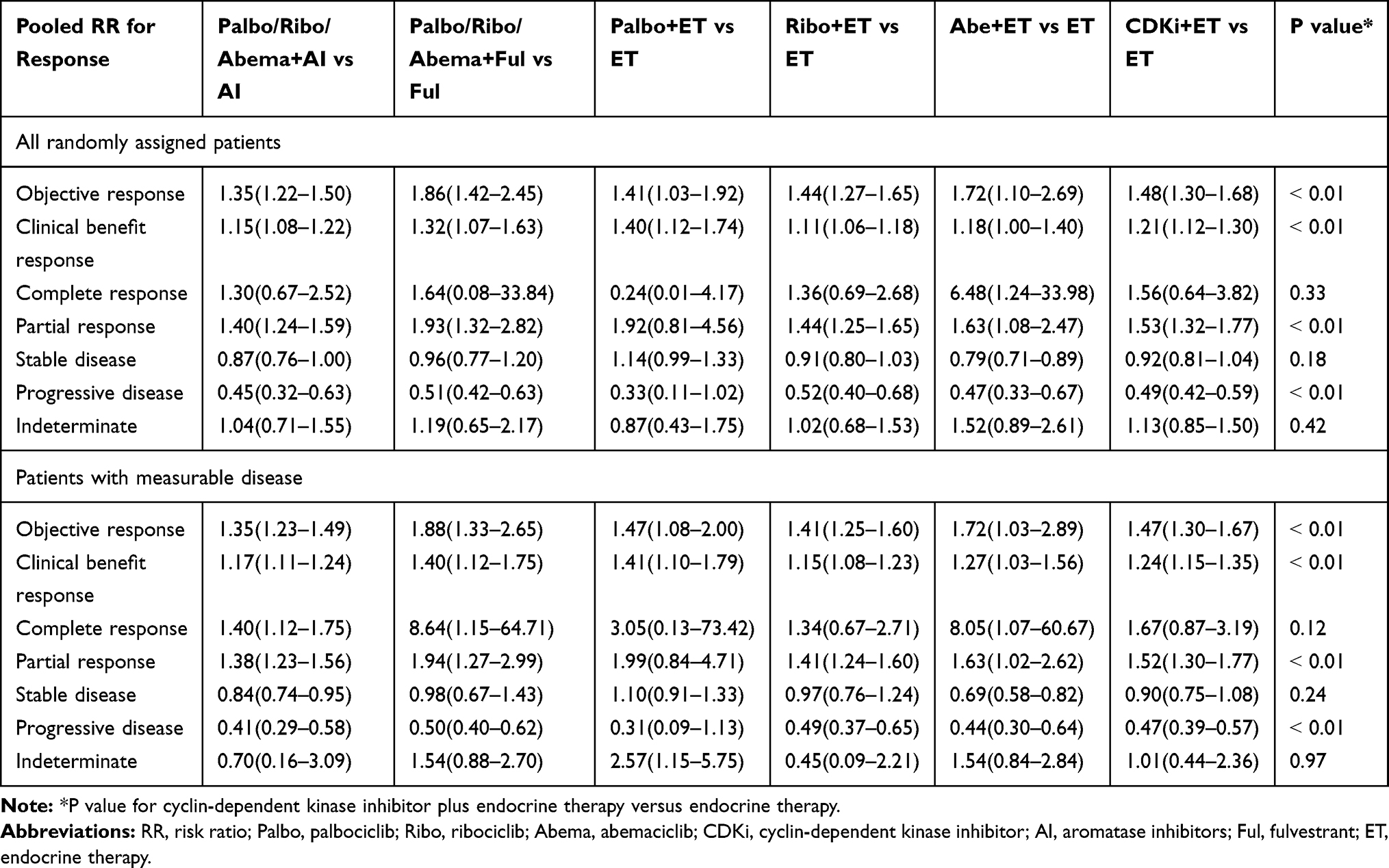 |
Table 3 Pooled Risk Ratio for Overall Response |
Subgroup Analysis and Sensitivity Analysis
Subgroup analysis for three CDKi showed no statistically significant difference of PFS existed among these three CDKi plus NSAI regimens as first-line therapy: palbociclib vs ribociclib (HR 0.55, 95% CI 0.49–0.60, P = 0.34; Figure S1A), palbociclib vs abemaciclib (HR 0.53, 95% CI, 0.47–0.59, P = 0.61; Figure S1B), and ribociclib vs abemaciclib (HR 0.56, 95% CI 0.51–0.62, P = 0.72; Figure S1C). According to stratification factors and other baseline characteristics, confirmed that the therapeutic effect of CDKi was not weakened (Supplementary Table S1). Sensitivity analysis was used to detect the stability of the consolidated results except the only Phase-II clinical trial (PALOMA-1). The result showed that all the outcomes were stable (HR 0.55, 95% CI 0.50–0.60, P<0.01; Supplementary Figure S2).
Safety
For grade 3 or 4 hematologic AEs, the results indicated that the CDKi group had a significantly increased risk of neutropenia (RR 33.52, 95% CI 17.27–65.05, P < 0.01), leukopenia (RR 22.08, 95% CI 12.12–40.21, P < 0.01), thrombocytopenia (RR 7.08, 95% CI 1.95–25.73, P < 0.01), and anemia (RR 2.25, 95% CI 1.39–3.64, P < 0.01). It is noteworthy that the CDKi group had a significantly increased risk of aspartate aminotransferase elevated (RR 3.48, 95% CI 1.89–6.43, P < 0.01) and alanine aminotransferase elevated (RR 6.08, 95% CI 3.16 −11.71, P < 0.01). As for pain in extremity, the dangers of it were minimized in the CDKi group, compared with the placebo group (RR 0.27, 95% CI 0.08–0.87, P = 0.03). Furthermore, fatigue, decreased appetite and asthenia were also more common in the CDKi group. However, for other serious AEs, there were no significant differences between groups with respect to vomiting (RR 1.33, 95% CI 0.60–2.94, P = 0.49), rash (RR 3.02, 95% CI 0.95–9.54, P = 0.06) and electrocardiogram QT prolonged (RR 4.01, 95% CI 0.89–18.05, P = 0.07). For three different CDKi, abemaciclib significantly increased the risk of grade 3 to 4 diarrhea (Table 4).
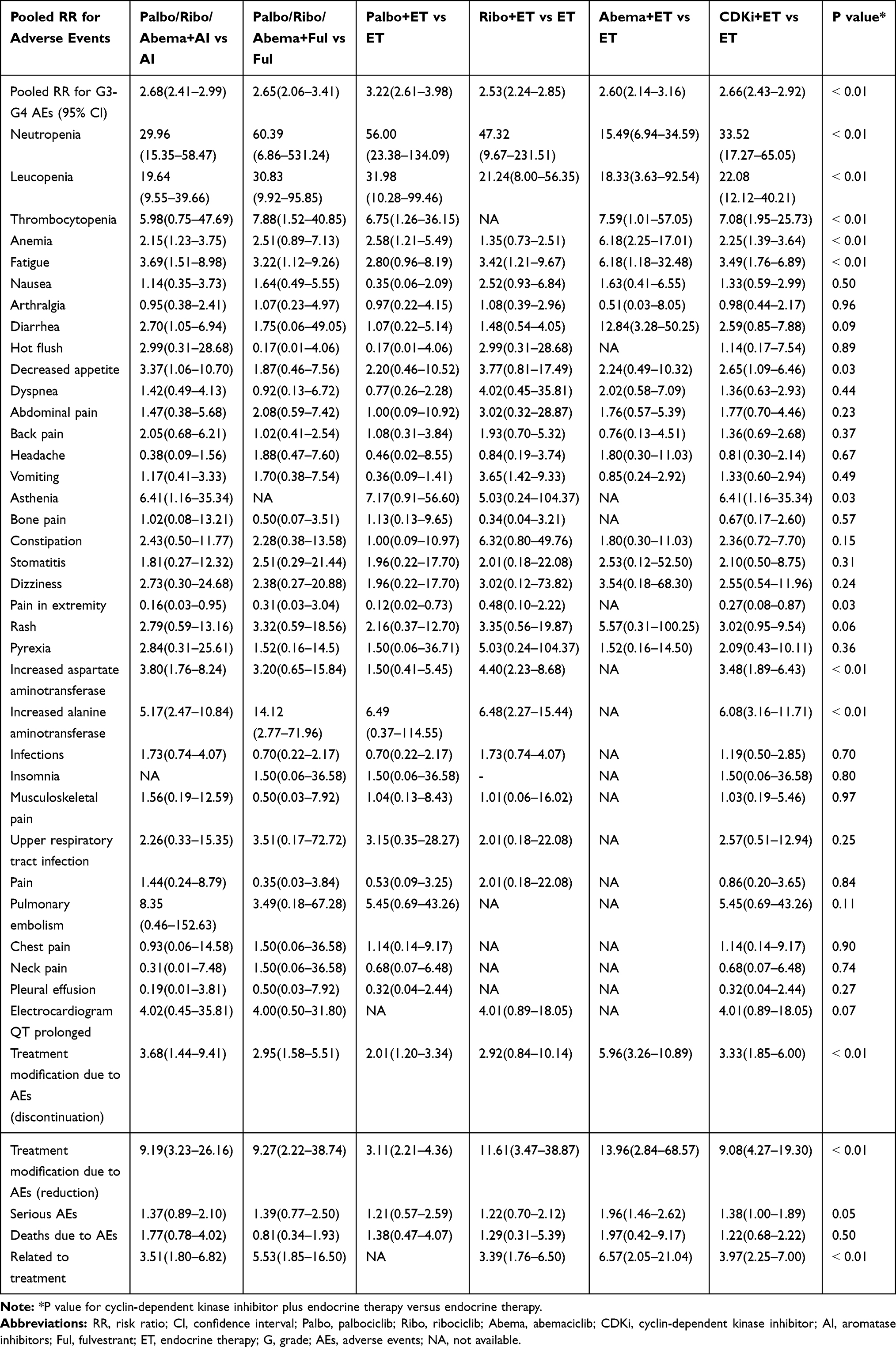 |
Table 4 Subgroup Analysis of Common Grade 3 and 4 Adverse Events |
Discussion
This study constitutes a comprehensive and systematic evaluation of the efficacy and safety of CDKi combined with ET for patients with HR-positive, HER2-negative ABC. Overall, PFS (P < 0.01) was significantly longer in the CDKi group than in the placebo group, and the ORR and CBR were better in the CDKi group. In addition, CDKi plus ET showed a significant OS benefit over ET alone. The results of the safety analyses showed that the CDKi group was well tolerated. The most common grade 3 or 4 AEs in the CDKi combination group were hematologic AEs. Furthermore, these treatment effects were consistent across most prespecified subgroups, such as age, Eastern Cooperative Oncology Group (ECOG) performance status, ET resistance, and the kind of CDKi. These data provide additional confirmation for the use of CDKi and ET combinations as effective first-line treatment for women with HR-positive/HER2-negative ABC.
Hormone-directed drugs have been the mainstay of treatment for advanced HR-positive breast cancer for more than four decades. To improve clinical outcomes, many drugs targeting HRs or ligand pathways have emerged, including tamoxifen, steroidal and NSAIs, and fulvestrant.17 However, most drugs that target other pathways, including the Her1 and Her2 pathways, angiogenesis, and IGFR, have been less than satisfactory and might play a role in the development of resistance to hormone drugs.18–20 The development of CDKi for the treatment of HR-positive ABC was based on the findings of preclinical studies that identified a dependence of HR-positive breast cancer on CDK4 and CDK6 signaling and a synergistic effect from targeting the HR, cyclin D CDK4/6 Rb pathway.21 Early preclinical data suggest that relative amounts of pRb in various breast cancer subtypes may be predictive, although pRb loss is uncommon in HR-positive, HER2-negative breast cancers.21 PALOMA-1 indicated that the increase in cyclin D1, loss of p16, or both may be a potential predictor, but further studies are needed.12 The large genome expression analysis report of the PALOMA-3 study showed that although palbociclib plus fulvestrant was effective for all patients with biomarker grouping,14 the high expression of CCNE1 mRNA was associated with relative resistance to palbociclib, and the expression level of CCNE1 mRNA might be a predictive indicator of the efficacy of palbociclib plus fulvestrant.22 More biomarkers and biomarkers of resistance will also be assessed in ongoing and future molecular studies.23,24
Palbociclib, ribociclib and abemaciclib are orally administered, potent, and selective small-molecule inhibitors of CDK 4 and 6.25,26 Previous studies have demonstrated that palbociclib, ribociclib and abemaciclib have the ability to inhibit pRb phosphorylation as well and suppress the proliferation of breast cancer cells, in particular for the HR-positive subtype of breast cancer.21,27 Relevant clinical data showed that CDKi could inhibit the growth of tumors, which would not only be a great benefit to patients with ABC but also to patients with early breast cancer.28 In addition, related preclinical studies have shown that HER2+ breast cancer cell lines remain sensitive to CDKi, indicating that HER2+ breast cancer patients may also benefit from the treatment of CDKi.29 However, preclinical research revealed that there was no relevant effect of CDKi on the triple-negative subtype of breast cancer.21 Although the OS benefit of CDKi combined with ET has reported in multiple trials,30–34 how to combine CDKi with chemotherapy and targeted drugs is still an important clinical problem to be solved. Nevertheless, further studies are needed to determine whether CDKi have the ability to antagonize the antitumor effects of cytotoxic chemotherapy or targeted therapy, which has the function of killing cancer cells in the cell cycle.35 In addition, more RCTs are needed to determine which groups are more suitable for treatment with CDKi.
A high incidence of hematologic AEs has consistently been observed in combination treatment with CDKi. The most common hematologic grade 3 or 4 AEs were neutropenia, leucopenia, anemia and thrombocytopenia. Although the incidence of neutropenia of any grade in the CDKi group was 66.08% in the current meta-analysis, the incidence of febrile neutropenia was 1.13%. Although hematologic AEs were the most common all-grade and grade 3 or 4 AEs, they were not accompanied with serious clinical outcomes and are likely the result of an on-target effect of CDKi on marrow progenitor cells.36 The absence of serious complications resulting from CDKi-associated hematologic AEs probably reflects a cytostatic rather than cytotoxic effect of the drug on bone marrow progenitor cells, different from what is seen with typical cytotoxic drugs. Our meta-analysis provides useful data for the safety profile of the combination of CDKi and ET, suggesting that AEs are manageable and treatable. AEs were generally manageable with CDKi dose adjustments. There was a low proportion of patients who discontinued study treatment owing to AEs.
Our study has some limitations. Firstly, there is no head-to-head trial compared different CDKi, and we have no individual patient data to make a further comparison, mainly because of the limited data available in the real-world study. Secondly, there are no data of biomarkers to predict efficacy. Finally, further follow-up of OS is still needed to determine the effect of CDKi on long-term survival.
Conclusion
In conclusion, the data from these RCTs provide proof for the efficacy and safety of CDKi in advanced, HR-positive, HER2-negative ABC. The improvement in PFS is substantial in this population. Although the AEs of CDKi are higher, it is generally acceptable and manageable. These data clearly warrant further investigation of the efficacy and safety of CDKi in combination with hormonal blockade, both in patients with this subtype of breast cancer and in other cancer settings.
Acknowledgments
We are grateful to professor Herui Yao from the Breast Tumor Centre of Sun Yat-sen Memorial Hospital for his guidance on this study. This study was supported by grants from the National Science and Technology Major Project (2020ZX09201021), the Sun Yat-Sen University Clinical Research 5010 Program (2018007), the China Postdoctoral Science Foundation (2019M663288), the Sun Yat-Sen Clinical Research Cultivating Program (SYS-Q-202007), and Natural Science Foundation of Guangdong Province (2017A030313489).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5). doi:10.1093/jnci/dju055.
2. Rugo HS, Rumble RB, Macrae E, et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: american society of clinical oncology guideline. J clin oncol. 2016;34(25):3069–3103. doi:10.1200/JCO.2016.67.1487
3. Milani A. Overcoming endocrine resistance in metastatic breast cancer: current evidence and future directions. World J Clin Oncol. 2014;5(5):990–1001. doi:10.5306/wjco.v5.i5.990
4. Ciriello G, Gatza ML, Beck AH, et al. Comprehensive molecular portraits of invasive lobular breast cancer. Cell. 2015;163(2):506–519. doi:10.1016/j.cell.2015.09.033
5. Choi YJ, Anders L. Signaling through cyclin D-dependent kinases. Oncogene. 2014;33(15):1890–1903. doi:10.1038/onc.2013.137
6. Finn RS, Aleshin A, Slamon DJ. Targeting the cyclin-dependent kinases (CDK) 4/6 in estrogen receptor-positive breast cancers. Breast Cancer Res. 2016;18(1):17. doi:10.1186/s13058-015-0661-5
7. Gelbert LM, Cai S, Lin X, et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: in-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Invest New Drugs. 2014;32(5):825–837. doi:10.1007/s10637-014-0120-7
8. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748. doi:10.1056/NEJMoa1609709
9. Malorni L, Curigliano G, Minisini AM, et al. A phase II trial of the CDK4/6 inhibitor palbociclib (P) as single agent or in combination with the same endocrine therapy (ET) received prior to disease progression, in patients (pts) with hormone receptor positive (HR+) HER2 negative (HER2-) metastatic breast cancer (mBC) (TREnd trial). J Clin Oncol. 2017;35.
10. Goetz MP, Toi M, Campone M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J clin oncol. 2017;35(32):3638–3646. doi:10.1200/JCO.2017.75.6155
11. Tripathy D, Im SA, Colleoni M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised Phase 3 trial. Lancet Oncol. 2018;19(7):904–915. doi:10.1016/S1470-2045(18)30292-4
12. Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16(1):25–35. doi:10.1016/S1470-2045(14)71159-3
13. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. doi:10.1056/NEJMoa1607303
14. Cristofanilli M, Turner NC, Bondarenko I, et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016;17(4):425–439. doi:10.1016/S1470-2045(15)00613-0
15. Sledge GW
16. Slamon DJ, Neven P, Chia S, et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J clin oncol. 2018;36(24):2465–2472. doi:10.1200/JCO.2018.78.9909
17. Chlebowski RT. Changing concepts of hormone receptor-positive advanced breast cancer therapy. Clin Breast Cancer. 2013;13(3):159–166. doi:10.1016/j.clbc.2012.11.002
18. Robertson JF, Ferrero JM, Bourgeois H, et al. Ganitumab with either exemestane or fulvestrant for postmenopausal women with advanced, hormone-receptor-positive breast cancer: a randomised, controlled, double-blind, phase 2 trial. Lancet Oncol. 2013;14(3):228–235. doi:10.1016/S1470-2045(13)70026-3
19. Martin M, Loibl S, von Minckwitz G, et al. Phase III trial evaluating the addition of bevacizumab to endocrine therapy as first-line treatment for advanced breast cancer: the letrozole/fulvestrant and avastin (LEA) study. J clin oncol. 2015;33(9):1045–1052. doi:10.1200/JCO.2014.57.2388
20. Finn RS, Press MF, Dering J, et al. Quantitative ER and PgR assessment as predictors of benefit from lapatinib in postmenopausal women with hormone receptor-positive, HER2-negative metastatic breast cancer. Clin Cancer Res. 2014;20(3):736–743. doi:10.1158/1078-0432.CCR-13-1260
21. Finn RS, Dering J, Conklin D, et al. PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro. Breast Cancer Res. 2009;11(5):R77. doi:10.1186/bcr2419
22. Turner NC, Liu Y, Zhu Z, et al. Cyclin E1 expression and palbociclib efficacy in previously treated hormone receptor-positive metastatic breast cancer. J clin oncol. 2019; 37(14);Jco1800925.
23. Herrera-Abreu MT, Palafox M, Asghar U, et al. Early adaptation and acquired resistance to CDK4/6 inhibition in estrogen receptor-positive breast cancer. Cancer Res. 2016;76(8):2301–2313. doi:10.1158/0008-5472.CAN-15-0728
24. Yang C, Li Z, Bhatt T, et al. Acquired CDK6 amplification promotes breast cancer resistance to CDK4/6 inhibitors and loss of ER signaling and dependence. Oncogene. 2017;36(16):2255–2264. doi:10.1038/onc.2016.379
25. Tripathy D, Bardia A, Sellers WR. Ribociclib (LEE011): mechanism of action and clinical impact of this selective cyclin-dependent kinase 4/6 inhibitor in various solid tumors. Clin Cancer Res. 2017;23(13):3251–3262. doi:10.1158/1078-0432.CCR-16-3157
26. Torres-Guzman R, Calsina B, Hermoso A, et al. Preclinical characterization of abemaciclib in hormone receptor positive breast cancer. Oncotarget. 2017;8(41):69493–69507. doi:10.18632/oncotarget.17778
27. Tolaney SM, Rosen LS, Beeram M, et al. Clinical activity of abemaciclib, an oral cell cycle inhibitor, in metastatic breast cancer. Cancer Res. 2015;75.
28. Curigliano G, Gomez Pardo P, Meric-Bernstam F, et al. Ribociclib plus letrozole in early breast cancer: a presurgical, window-of-opportunity study. Breast. 2016;28:191–198. doi:10.1016/j.breast.2016.06.008
29. Goel S, Wang Q, Watt AC, et al. Overcoming therapeutic resistance in HER2-positive breast cancers with CDK4/6 inhibitors. Cancer Cell. 2016;29(3):255–269. doi:10.1016/j.ccell.2016.02.006
30. Pal SK, Miller MJ, Agarwal N, et al. Clinical cancer advances 2019: annual report on progress against cancer from the american society of clinical oncology. J clin oncol. 2019;37(10):834–849. doi:10.1200/JCO.18.02037
31. Im SA, Lu YS, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381(4):307–316. doi:10.1056/NEJMoa1903765
32. Slamon DJ, Neven P, Chia S, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N Engl J Med. 2020;382(6):514–524. doi:10.1056/NEJMoa1911149
33. Sledge GW
34. Turner NC, Slamon DJ, Ro J, et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N Engl J Med. 2018;379(20):1926–1936. doi:10.1056/NEJMoa1810527
35. Xu H, Yu S, Liu Q, et al. Recent advances of highly selective CDK4/6 inhibitors in breast cancer. J Hematol Oncol. 2017;10(1):97. doi:10.1186/s13045-017-0467-2
36. Roberts PJ, Bisi JE, Strum JC, et al. Multiple roles of cyclin-dependent kinase 4/6 inhibitors in cancer therapy. J Natl Cancer Inst. 2012;104(6):476–487. doi:10.1093/jnci/djs002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.