")
Back to Journals » Clinical Ophthalmology » Volume 13
Efficacy and safety of bromfenac 0.09% and sodium hyaluronate 0.4% combination therapy, versus placebo in patients with pterygium I–III for clinical signs on ocular inflammation
Authors Chávez-Mondragón E , Palacio C , Soto-Gómez A , Villanueva-Nájera M , De Wit-Carter G, Suárez-Velasco R, Baiza-Duran L, Olvera-Montaño O , Muñoz-Villegas P
Received 31 January 2019
Accepted for publication 27 March 2019
Published 2 May 2019 Volume 2019:13 Pages 781—787
DOI https://doi.org/10.2147/OPTH.S203648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eduardo Chávez-Mondragón,1 Claudia Palacio,2 Abraham Soto-Gómez,3 Miguel Villanueva-Nájera,4 Guillermo De Wit-Carter,5 Ruben Suárez-Velasco,6 Leopoldo Baiza-Duran,7 Oscar Olvera-Montaño,7 Patricia Muñoz-Villegas7
1Fundación de Asistencia Privada Conde de Valenciana, IAP, CDMX, Mexico; 2Fundación Hospital Nuestra Señora de la Luz, IAP, CDMX, Mexico; 3Catarata y Glaucoma de Occidente, SA de CV, Guadalajara, Jalisco, Mexico; 4Private Office, CDMX, Mexico; 5Asociación para Evitar la Ceguera en Mexico IAP, CDMX, Mexico; 6Novam y Vita, Guadalajara, Jalisco, Mexico; 7Clinical Research Department, Laboratorios Sophia, SA de CV, Zapopan, Jalisco, Mexico
Purpose: This study evaluated the clinical efficacy and safety of bromfenac 0.09%, sodium hyaluronate 0.4% (SH) combination therapy, versus placebo and SH in a clinical model of pterygium I–III.
Methods: A total of 166 eyes (99 patients) with pterygium grade I–III were randomized to bromfenac 0.09% ophthalmic solution+SH 0.4% or placebo+SH 0.4%. This was a Phase IV, prospective, parallel, double-masked, multicenter clinical trial. One drop of bromfenac or placebo was instilled two times a day (BID) for 20 days, both groups accompanied treatments with one drop of SH three times a day (TID). The primary efficacy endpoints were the conjunctival hyperemia and the Ocular Surface Disease Index (OSDI) score. Other results measured included burning, foreign body sensation, and photophobia. The safety was assessed by the tear break-up time (TBUT), visual acuity (VA), IOP, lissamine green, fluorescein stains, and the incidence of adverse events (AEs).
Results: Compared with baseline, there was a significant reduction in the conjunctival hyperemia (p=0.0001) and OSDI score in both groups (p=0.0001). There was a significant improvement in ocular symptomatology for both, placebo/SH and bromfenac/SH groups (p=0.0001), the decrement in the ocular burning was 41.1% vs 24.6%, the foreign body sensation was 31.5% vs 36.2% and, for photophobia was 23.3% vs 30.5%, respectively. A statistically significant difference was observed in TBUT for bromfenac/SH (p=0.045), at day 20. There were no significant alterations in IOP (p=0.068) or VA (p=0.632). Similar improvements were observed in the fluorescein and green lissamine staining. Finally, the incidence of AE was similar between groups.
Conclusion: The treatment with bromfenac 0.09% ophthalmic solution and SH 0.4% combination therapy for 3 weeks reduced clinical signs, in patients with pterygium I–III. The results suggest that bromfenac 0.09% can improve the symptomatology, reduce the presentation of clinical signs associated with superficial ocular inflammation.
Keywords: nonsteroidal anti-inflammatory drug, Ocular Surface Disease Index, conjunctival hyperemia, ocular lubricant
Introduction
Bromfenac is a topical, NSAID. Its chemical structure lengthens the absorption into the ocular tissues and enhances the duration of anti-inflammatory activity.1 It is the first and only topical ophthalmic NSAID with a once-daily dosing regimen approved by the Food and Drugs Administration for the treatment of post-operative pain and inflammation following cataract surgery.2
The manipulation of ocular structures like surgery, infections, ocular trauma, among others, can produce an inflammatory process. After lysis, multiple chemical mediators induce the expression of cyclooxygenase (COX), an important group of enzymes active in the inflammatory process. Prostaglandins (PGs) are products of COX-2 and have several effects in the tissue. COX-2, which is inducible, is upregulated in states of inflammation, and converts the arachidonic acid into several PGs.1–3 NSAIDs block the PGs response through inhibiting COX enzymes.4–6 Furthermore, NSAIDs can decrease pain and photophobia after refractive surgery and alleviate itching associated with allergic conjunctivitis.5
Pterygium is a type of benign uncontrolled growth of the conjunctive tissue that lays over the cornea. Pterygium is an inflammatory active, invasive, and chronic disease. However, its pathogenesis remains incompletely understood. Clinically, the condition involves invasive centripetal growth with associated inflammation and neovascularization.3 Inflammation induces angiogenic pathways, resulting in neovascularization contributing to pterygia development and growth. COX-2 is expressed in both primary pterygia and recurrent pterygia.4
Many patients show foreign body sensation, tearing, chronic ocular discomfort, itching, and redness, and are commonly treated with lubricants, vasoconstrictors, or corticosteroids.7Redness can be taken as sign of inflammation which may suggest the progression and severity of a specific disease like pterygium.8,9 This fibrovascular tissue is characterized by its wedge-shaped and vascular growth that originate in the eye corneal limbus.9,10
The effectiveness and safety of bromfenac 0.09% ophthalmic solution (Zebesten®, Laboratorios Sophia, SA de CV, Zapopan, Jalisco, Mexico) in the treatment of ocular inflammatory signs and in the reduction of cystoid macular edema after phacoemulsification has been shown previously in Mexican population.6
Finally, sodium hyaluronate (SH) has been used as a lubricant. Lubricants have a rheological profile, they are viscous under static conditions on the eye, while this viscosity decreases during blinking; this behavior can be reproduced by hyaluronic acid (sodium salt) eye drops.11 Many studies have demonstrated the safety and efficacy of SH as eye drops.12–15 It was also proposed that SH might have a direct role in the control of ocular surface inflammation. The use of hypotonic SH eye drops has been shown increased tear osmolarity that could play a part in the pathogenesis of the ocular surface damage.16 Several clinical symptoms related to pterygium are commonly treated with lubricants.
The purpose of this study was to evaluate the clinical efficacy and safety of bromfenac 0.09% and SH 0.4% ophthalmic solutions in a combination therapy, versus placebo and SH 0.4%, in the presence of clinical signs and ocular inflammation on a clinical model of pterygium I–III.
Material and methods
Study design
This was a Phase IV, prospective, parallel, double-masked, multicenter clinical trial (registered at ClinicalTrials.gov as NCT03521791). It was conducted in six centers in Mexico. An ethics committee in each center reviewed and approved the study (see Ethics approval section). The research was conducted in compliance with the Declaration of Helsinki and in accordance with Good Clinical Practices Standards. All patients that participated in this study provided written and signed informed consent. Patients were recruited between January and August 2018.
Participants
Inclusion criteria included either men or women (aged >18 years) with a diagnosis of pterygium I–III (temporal and/or nasal) according to the Johnston Classification (Table 1).17 In the cases where subjects presented bilateral pterygium, both eyes were eligible. Double-headed pterygium cases were eligible too. Exclusion criteria included use of topical ocular drops and systemic medication that may affect the study’s results (eg, NSAID, antihistaminic, artificial tears with BAK, etc.), patients with autoimmune disease, corneal dystrophy, diagnosis of pterygium IV, corneal dellen, ocular surface inflammatory, proliferative or neoplastic diseases, any type of corneal ulcers, history of penetrating keratoplasty, ocular surgery within 3 months before baseline, pregnant or breastfeeding patients and patients at risk of pregnancy without birth control treatment.
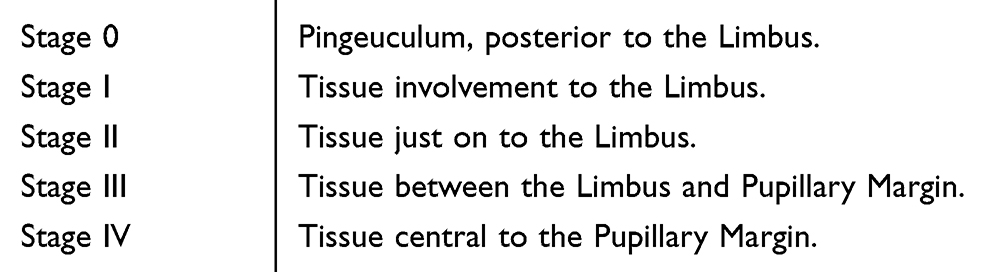 | Table 1 Pterygium classification |
Treatment and evaluations
A total of 166 eyes (99 patients) were randomized 1:1 to bromfenac 0.09% ophthalmic solution (PRO-155)+SH 0.4% (Lagricel® Ofteno, Laboratorios Sophia, SA de CV, Zapopan, Jalisco, Mexico) (n=47 subjects) or placebo+SH 0.4% (n=52 subjects), using a random numbers software. Patients instilled one drop of study drug in the inferior conjunctival sac (PRO-155 or placebo) BID and one drop TID of SH 0.4% for 20 days. Treatment assignment was masked throughout the study for all the researchers, patients, and other sponsoring team members. Follow-up visits were on days 7, 15, and 21 after randomization. A safety call was carried out 2 weeks after the final visit (36th day). The study drug was discontinued if either the principal investigator or patient judged that it was not in the latter’s best interest to continue.
At each follow-up visit, tear break-up time (TBUT), Ocular Surface Disease Index (OSDI), slit-lamp examination, visual acuity, and fluorescein and green lissamine dyes were examined.
Subjective symptoms were graded on a numerical scale of 0–4 using the OSDI questionnaire.18 The sum of the scores was used in the analysis. The TBUT was recorded as the number of seconds that elapsed between the last blink and the appearance of the first dry spot in the tear film. The ocular surface was evaluated with a slit-lamp aided by fluorescein staining, and for conjunctival staining, green lissamine was instilled in the eye. Surface dye staining was classified in a scale from 0 to V in accordance with the percentage of the affected area (Oxford scale). The visual acuity was determined with a Snellen chart and expressed in LogMAR values. The IOP was measured using a calibrated Goldmann applanation tonometer during the baseline and final visits.
The primary efficacy endpoints were the conjunctival hyperemia and the OSDI score. The tolerability was assessed by the burning, foreign body sensation, and photophobia. The safety was measured by the TBUT, visual acuity, IOP, lissamine green and fluorescein ocular surface stains, and the incidence of adverse events (AEs).
Statistical analysis
Statistical analysis was carried out using SPSS 19.0 software (SPSS Inc., Chicago, IL, USA). Efficacy evaluations were made only in per-protocol population (PP), established as a randomized patient with no major deviation from the protocol after performing a bivariate analysis. Sample size calculation was performed to test the improvement of conjunctival hyperemia after pterygium surgery of 2.9 grades of severity.19 With an alpha of 0.05, a power of 80%, and standard deviation of 0.4, a sample size of 69 cases (eyes) was found to be necessary. It was therefore planned to include 83 eyes per group in this study, allowing as much as 20% of cases to be excluded from the PP population as a result of major protocol deviations. Comparisons of treatment group categorical variables were done using the Mann–Whitney U test or Fisher’s exact test. The continuous variables were analyzed using Student's t-test and Chi-square test. The ordinal variables were analyzed using 2×2 contingency tables (McNemar’s test). The Wilcoxon signed rank test was used to compare within-group categorical variable changes from the baseline value. A two-side test with p≤0.05 was considered to indicate statistical significance.
Results
Characteristics of the participants
Ninety-nine patients were enrolled. Of the 99 patients, 42 (80.8%) patients in group 1 (placebo/SH), and 41 (87.2%) patients in group 2 (PRO-155/SH) completed the entire protocol without deviations. Between 19.2% and 12.8% of the patients discontinued their participation secondary to: presentation of AE (1 patient, group 1), patient’s decision unrelated to AE (2 patients, group 1), lost of follow-up (4 patients, group 2), and protocol deviations (7 and 2 patients, respectively). Demographic and baseline characteristic were similar between the two treatment groups without significant differences, see Table 2. Mean age±SD was 55.5±13.4 years (range 27–87); 72.3% of patients were female. Clinical signs and symptoms were similar between groups.
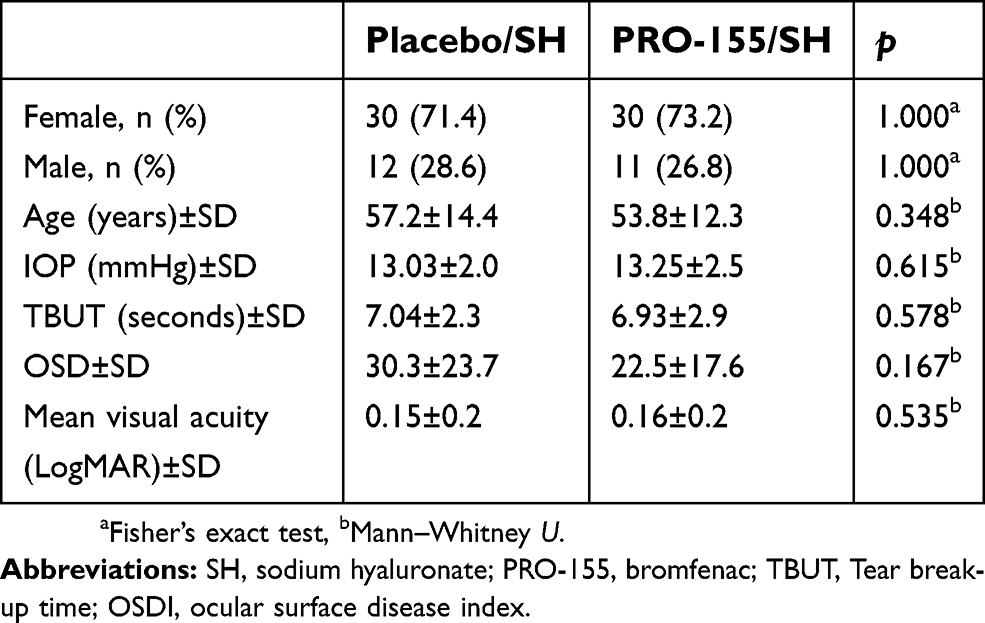 | Table 2 Demographic and baseline characteristics (n=83 completed patients) |
Efficacy
Conjunctival hyperemia
In the PP population, after 3 weeks of treatment, compared with the baseline there was a significant reduction in the conjunctival hyperemia in both groups (p=0.0001). The patients treated with placebo/SH resulted in a reduction of the severity on Efron scale a 29% (slight severity). This improvement was higher in the PRO-155/SH group, when a significant reduction on the severity was found in the final visit over the 52% of the patients. On the day 7 (visit 1), and on day 15 (visit 2) the improvement on the PRO-155/SH was statistically significant when compared to Placebo/SH (p=0.049 and p=0.021, respectively), see Figure 1.
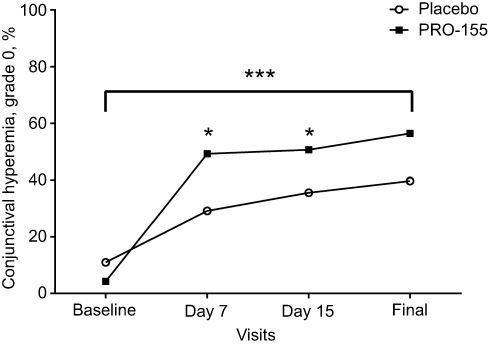 | Figure 1 Conjunctival hyperemia. Frequency of conjunctival hyperemia, grade 0 (normal). At each experimental visit for placebo/SH (black circle) and PRO-155/SH (white square). ***p=0.0001 for final visit>baseline (McNemar’s test), *p<0.05 for PRO-155/SH>placebo/SH at days 7 and 15 (X2 test). |
Ocular Surface Disease Index (OSDI)
Baseline OSDI was similar between groups (placebo/SH: 30.31±23.7 and PRO-155/SH: 22.51±17.6, p=0.167). There was a statistically significant reduction in the OSDI score in both groups during their final visit (12.35±16.8 vs 6.25±8.2, respectively) compared with the baseline (p=0.0001). No difference was observed between the two groups (p=0.086), see Table 4.
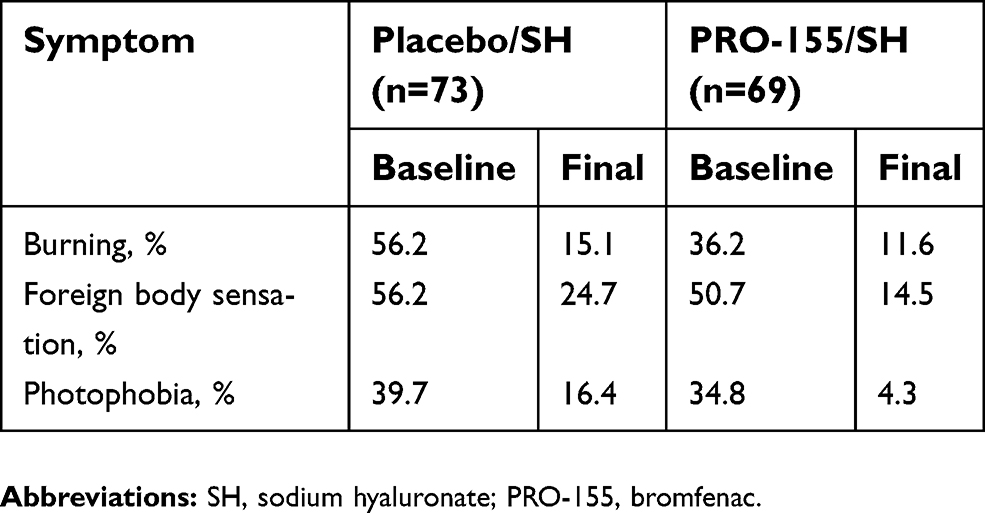 | Table 3 Ocular symptomatology (presence) |
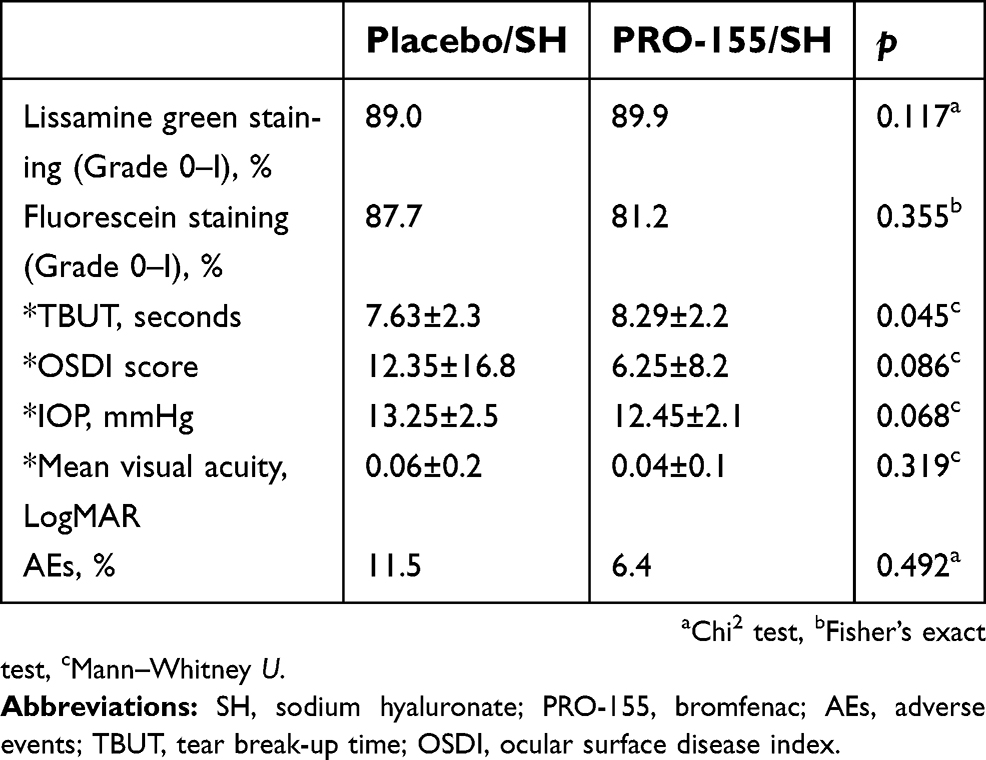 | Table 4 Clinical signs and safety |
Tolerability
Ocular symptomatology
Burning, foreign body sensation, and photophobia were considered the parameters of ocular symptomatology. All subjects showed a significant improvement of ocular symptomatology over the duration of the study. As shown in Table 3, there was a significant decrease of burning, foreign body sensation, and photophobia from the baseline to final visit (p=0.0001) in both groups. At the end of the study, the improvement in ocular burning for the placebo/SH group was 41.1%, for foreign body sensation it was 31.5% and, for photophobia it was 23.3%. The improvement in the ocular symptomatology for the PRO-155/SH group was 24.6%, 36.2%, and 30.5%, respectively. The improvement in photophobia was higher in the PRO-155/SH group (p=0.027).
Safety
Tear break-up time (TBUT)
After the intervention, the TBUT increased in both groups compared with baseline (p=0.0001), with a significant difference between treatments in the final visit (7.63±2.3 vs 8.29±2.2), when PRO-155/SH was higher (p=0.045), see Figure 2.
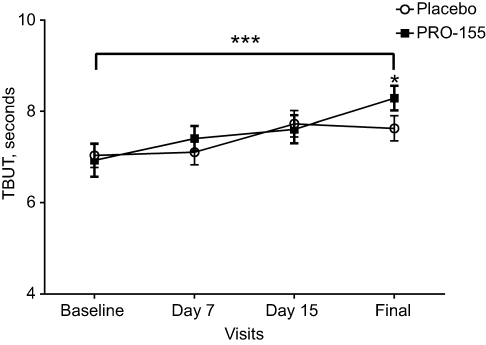 | Figure 2 Tear break-up time. Tear break-up time±S.E.M. At each experimental visit for placebo/SH (black circle) and PRO-155/SH (white square). ***p=0.0001 for final visit>baseline (Wilcoxon test), *p=0.045 for PRO-155/SH>placebo/SH at final visit (Mann–Whitney U test). |
Visual acuity (LogMAR)
The visual acuity did not decrease from baseline (0.15±0.2 vs 0.16±0.2) to final visit (0.14±0.2 vs 0.13±0.2) in placebo/SH and PRO-155/SH, respectively (p=0.101), see Table 4.
IOP
After the intervention period, the IOP did not increase from baseline (13.03±2.1 vs 13.25±2.5) to final visit (13.08±1.8 vs 12.45±2.1) for placebo/SH and PRO-155/SH groups, respectively (p=0.068), see Table 4.
Fluorescein and green lissamine staining
There was a statistically significant improvement for the fluorescein staining score in both groups (p=0.0001). The fluorescein staining score change from baseline for the placebo/SH group was 27.1% at day 7, 37% at day 15, and 31.5% at the final visit. Meanwhile, the improvement from baseline for PRO-155/SH was 17.4%, 26.1%, and 16%, respectively. No difference was observed between the two groups. Similar findings in the green lissamine staining were observed. There was a statistically significant improvement in both groups (p=0.0001). The green lissamine staining score for the placebo/SH group was 19% at day 7, 23.3% at day 15, and 19.1% at the final visit. Meanwhile, the improvement for PRO-155/SH was 10.1%, 20.3%, and 20.3%, respectively. No significant between-group differences were observed, see Table 4.
Adverse events (AEs)
Data on safety was analyzed for the to-be-treated population (ITT). A total of 20 AE were reported by 9.1% (9/99) of the randomized patients during the protocol. There were no significant differences for the incidence of AE between treatments (X2(1)=0.794, p=0.492). A total of 17 AE were reported for placebo/SH (14 ocular-EA and 3 non-ocular), and 3 for PRO-155/SH (1 ocular-EA and 2 non-ocular), there were no significant differences for the ocular or non-ocular AE between treatments (X2(1)=3.268, p=0.140. The most commonly reported non-ocular AE was headache (5%), while the most frequent ocular AE were ocular pain (15%) and foreign body sensation (15%). Serious AE did not occur during the study.
Discussion
Pterygium is an inflammatory, active, invasive, and chronic disease of unclear pathogenesis. Inflammation is the manifestation of vascular and cellular response of the tissue to injury.1,3 Bromfenac is a topical, NSAID, its chemical structure lengthens the absorption into the ocular tissues and enhances the duration of anti-inflammatory activity.1 Previous studies have been conducted to evaluate the safety and efficacy of bromfenac 0.09% for the treatment of signs associated to ocular inflammation and for the reduction of presentation of cystoid macular edema after phacoemulsification.6 Several clinical symptoms related to pterygium are commonly treated with lubricants. SH has been used as a lubricant, its use could play an important part in the pathogenesis of the ocular surface damage. SH increase precorneal tear film stability, reduce the tear evaporation rate, and the use of hypotonic hyaluronate should be encouraged for the treatment of diseases of ocular surface.7,16
In this study, we compared the efficacy and safety of bromfenac 0.09% and SH 0.4% combination therapy, versus placebo in a clinical model of pterygium I–III. We demonstrated that the combination of bromfenac and SH effectively reduces the presence of clinical signs of ocular inflammation. Fibrovascular redness is an important clinical sign, characterized by its wedge-shaped, angular and vascular growth. Also, redness can be taken as a sign of inflammation.9,10 After 3 weeks of treatment, there was a significant decrease in the conjunctival hyperemia in both groups. As much as 29% of patients in group 1 (placebo/SH) improved the severity of their clinical presentation. The results indicate that SH has a beneficial effect on the treatment of conjunctival hyperemia, in agreement with other studies conducted with SH eye drops.14,16 Meanwhile, 52% of group 2 (PRO-155/SH) showed a decrease in the severity of their conjunctival hyperemia, patients in group 2 reported a significantly greater improvement in conjunctival hyperemia compared with placebo group at day 7; this result is consistent with previous studies.6
The OSDI is a valid and trustworthy instrument for measuring of the symptoms of ocular irritation related to dry eye disease and their impact on vision-related function. It possesses necessary psychometric properties to be used as an end point in clinical trials.18 In this study, subjective symptoms were graded using the OSDI questionnaire. Both groups demonstrated a reduction of OSDI scores which reached normal values by the final visit.
Likewise, many patients with pterygium show foreign body sensation, tearing, chronic ocular discomfort, itching, and redness.7 In our study, clinical symptoms like burning, foreign body sensation, and photophobia were significantly decreased by the final visit in both groups. The improvement in photophobia was higher in the PRO-155/SH versus placebo/SH at the end of the study, consistently with previous studies with NSAIDs.5
TBUT, visual acuity, IOP and fluorescein, and green lissamine staining were performed to evaluate the safety of bromfenac. Mean TBUT was increased in both groups, with significant differences in PRO-155/SH by the end of the study. For visual acuity and IOP, there were no differences between treatments.
Topical ophthalmic NSAIDs are commonly used as the treatment of post-operative inflammation in several surgical procedures. Local irritation signs and symptoms include conjunctival hyperemia, burning, stinging, and corneal anesthesia. A more serious complication involves corneal ulceration and full-thickness corneal melts.20 In our study, regardless of literature reports of AE due to the use of NSAIDs, no differences were shown between treatments for lissamine green and fluorescein staining. Ocular staining scores were lower (Oxford scale) in both groups compared with their baseline, similarly to other authors’ findings on regards to the use of bromfenac.6 Similarly, the presence of AEs in both groups showed no statistically significant differences. Only one patient in placebo/SH group discontinued the study due to a non-serious AE. Non-serious AEs occurred during the study.
Many studies have demonstrated the safety and efficacy of SH as a lubricant.12–15 SH might have a direct role in the control of ocular surface inflammation in patients with dry eye. Meanwhile, bromfenac blocks the PGs response through inhibiting COX enzymes.4–6 In the present study, the combination bromfenac 0.09% and SH 0.4% was effective in reducing the presence of clinical signs and ocular inflammation on a clinical model of pterygium I–III.
Further studies are necessary to understand the effect of SH in the treatment of clinical signs and ocular inflammation, and trials with a prolonged follow-up are needed to conclusively determine the efficacy of this combination therapy.
Conclusion
The treatment with the combination of bromfenac 0.09% and SH 0.4% for 3 weeks reduces clinical signs (conjunctival hyperemia, photophobia, OSDI, burning, and foreign body sensation) in patients with pterygium I–III. Furthermore, 0.09% bromfenac/SH 0.4% are more effective than SH 0.4% eye drops alone in improving conjunctival hyperemia, TBUT, and photophobia in pterygium I–III. These results suggest that bromfenac 0.09% can improve the presentation of clinical signs on ocular inflammation.
Abbreviation list
OSDI, Ocular Surface Disease Index; PGs, prostaglandins; PRO-155, bromfenac 0.09%; SH, sodium hyaluronate; TBUT, tear break-up time.
Data sharing
The database generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval
The study was approved by Comité de Ética en Investigación Instituto Jalisciense de Investigación Clínica SA de CV, Comité de Ética en Investigación Asociación Para Evitar la Ceguera en México, IAP, Comité de Investigación Instituto de Oftalmología Fundación de Asistencia Privada Conde de Valenciana IAP, Comité de Investigación de Medica Sur, SAB de CV and Comité de Investigación de Accelerium S de RLCV.
Acknowledgments
We thank the participants in the study. The authors thank Alejandra Sánchez-Rios (Laboratorios Sophia, SA de CV) for her editorial assistance in the preparation of this article.
Author contributions
All Authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
This study was sponsored by Laboratorios Sophia, SA de CV. Leopoldo Baiza-Durán, Oscar Olvera-Montaño, and Patricia Muñoz-Villegas are employees of Laboratorios Sophia. The authors declare that they have no other competing interests in this work.
References
1. Ahuja M, Dhake AS, Sharma SK, Majumdar DK. Topical ocular delivery of NSAIDs. Aaps J. 2008;10(2):229–241. doi:10.1208/s12248-008-9024-9
2. Cable M. Comparison of bromfenac 0.09% QD to nepafenac 0.1% TID after cataract surgery: pilot evaluation of visual acuity, macular volume, and retinal thickness at single site. Clin Ophthalmol. 2012;6:997–1004. doi:10.2147/OPTH.S32179
3. Bradley JC, Yang W, Bradley RH, Reid TW, Schwab IR. The science of pterygia. Br J Ophthalmol. 2010;94:815–820. doi:10.1136/bjo.2008.151852
4. Karahan N, Baspinar S, Ciris M, Baydar CL, Kapucuoglu N. Cyclooxygenase-2 expression in primary and recurrent pterygium. Indian J Ophthalmol. 2008;56(4):279–283.
5. Kim AJ, Flach AJ, Jampol LM. Nonsteroidal anti-inflammatory drugs in ophthalmology. Major review. Surv Ophthalmol. 2010;55:108–133. doi:10.1016/j.survophthal.2009.07.005
6. Palacio C, Fernández de OL, Bustos FR, et al. Bromfenac 0.09% bioavailability in aqueous humor, prophylactic effect on cystoid macular edema, and clinical signs of ocular inflammation after phacoemulsification in a Mexican population. Clin Ophthalmol. 2016;10:233–237. doi:10.2147/OPTH.S93530
7. Coroneo MT, Di Girolamo N, Wakefield D. The pathogenesis of pterygia. Curr Opin Ophthalmol. 1999;10:282–288.
8. Che Azemin MZ, Mohd Tamrin MI, Hilmi MT, et al. Inter-grader reliability of supervised pterygium redness grading system. Adv Sci Lett. 2016;22(10):2885–2888. doi:10.1166/asl.2016.7125
9. Che Azemin MZ, Hilmi MR, Mohd Tamrin MI, et al. Fibrovascular redness grading using Gaussian process regression with radial basis function kernel.
10. Hilmi MR, Che Azemin MZ, Mohd Kamal K, et al. Prediction of changes in visual acuity and contrast sensitivity function by tissue redness after pterygium surgery. Current Eye Res. 2017;42:852–856. doi:10.1080/02713683.2016.1250277
11. Fallacara A, Vertuani S, Panozzo G, Pecorelli A, Valacchi G, Manfredini S. Novel artificial tears containing cross-linked hyaluronic acid: an invitro re-epithelization study. Molecules. 2017;22(12):2104. doi:10.3390/molecules22122104
12. You IC, Li Y, Jin R, Ahn M, Choi W, Yoon KC. Comparison of 0.1%, 0.18%, and 0.3% hyaluronic acid eye drops in the treatment of experimental dry eye. J Ocul Pharm Ther. 2018;34(8):557–564. doi:10.1089/jop.2018.0032
13. Park Y, Song JS, Choi CY, Yoon KC, Lee HK, Kim HS. A randomized multicenter study comparing 0.1%, 0.15%, and 0.3% sodium hyaluronate with 0.05% cyclosporine in the treatment of dry eye. J Ocul Pharm Ther. 2017;33(2):66–72. doi:10.1089/jop.2016.0086
14. Robert P-Y, Cochener B, Amrane M, et al. Efficacy and safety of cationic emulsion in the treatment of moderate to severe dry eye disease: a randomized controlled study. Eur J Ophthalmol. 2016;26(6):546–555. doi:10.5301/ejo.5000830
15. Hwang HS, Sung Y-M, Lee WS, Kim EC. Additive effect of preservative-free sodium hyaluronate 0.1% in treatment of dry eye syndrome with diquafosol 3% eye drops. Cornea. 2014;33(9):935–941. doi:10.1097/ICO.0000000000000213
16. Aragona P, Stefano G, Ferreri F, Spinella R, Stilo A. Sodium hyaluronate eye drops off different osmolarity for the treatment of dry eye in Sjögren‘s syndrome patients. Br J Ophthalmol. 2002;86:879–884.
17. Johnston SC, Williams PB, Sheppard JD. A comprehensive system for pterygium classification. IOVS. 2004;45:2940.
18. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118:615–621.
19. Ozgurhan EB, Kara N, Bozkurt E, et al. Effect of fluoremethalone/tetrahydrozoline fixed combination on conjuctival autograft morphology after primary pterygium excision. Biomed Res Int. 2013;2013(481843):8. doi:10.1155/2013/481843
20. Gaynes BI, Fiscella R. Topical nonsteroidal anti-inflammatory drugs for ophthalmic use. Drug Saf. 2002;25(4):233–250. doi:10.2165/00002018-200225040-00002
 © 2019 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2019 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.