")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Effects of Trial Population Selection on Quality of Life and Healthcare Decision-Making: A Systematic Review and Example in the Treatment of Hepatocellular Carcinoma with Radioembolization
Authors Pollock RF , Colaone F , Shergill S , Brennan VK, Agirrezabal I
Received 12 May 2021
Accepted for publication 2 September 2021
Published 22 September 2021 Volume 2021:13 Pages 835—841
DOI https://doi.org/10.2147/CEOR.S319857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Richard F Pollock,1 Fabien Colaone,2 Suki Shergill,2 Victoria K Brennan,2 Ion Agirrezabal2
1Health Economics and Outcomes Research, Covalence Research Ltd, London, UK; 2Global Health Economics, Pricing, Reimbursement & Market Access, Sirtex Medical United Kingdom Ltd, London, UK
Correspondence: Richard F Pollock
Covalence Research Ltd, 51 Hayes Grove, London, SE22 8DF, UK
Tel +44 20 8638 6525
Email [email protected]
Background and Aims: Quality of life is among the most important considerations in the treatment of hepatocellular carcinoma (HCC), arguably second only to overall survival. Measuring and modeling patient quality of life is also crucial in the evaluation of the cost-effectiveness of health interventions. In the present study, we aimed to identify cost-utility analyses comparing selective internal radiation therapy (SIRT) with systemic therapy in patients with unresectable HCC and to compare the modeled incremental quality of life differences between the two therapies.
Methods: A systematic literature review was conducted. PubMed, EMBASE, the Cochrane Library, and health technology assessment agency websites were searched to identify cost–utility studies of SIRT versus systemic therapies in the treatment of HCC. Key characteristics of the studies, modeled populations and incremental quality of life outcomes were extracted from the included studies.
Results: The systematic literature review retrieved 1140 studies, of which four were ultimately included. Hand searches then identified two distinct analyses, and an updated version of one of the four studies identified initially. From these seven studies, 18 analyses were included. Analyses using data from the overall trial populations reported incremental quality-of-life estimates spanning − 0.09 to +0.28 quality-adjusted life years (QALYs), with that range expanding to − 0.09 to +0.60 QALYs when also considering post hoc sub-group analyses.
Conclusion: The wide range of incremental QALYs, with substantial differences between overall trial populations and subgroups, illustrates the impact that the choice of target population may have on the relative quality of life outcomes of the compared interventions, which may in turn affect clinical decision-making. The small differences also highlight both the importance of reporting measures of dispersion around the findings, and the limitations of the incremental cost-effectiveness ratio (ICER) for assessing the relative cost-effectiveness of interventions that are predicted to result in similar quality-of-life outcomes.
Keywords: hepatocellular carcinoma, quality of life, brachytherapy
Background and Aims
Quality of life is among the most important considerations in palliative care settings where the prospect of a cure is uncertain, arguably second to overall survival.1 Accurately measuring and modeling health-related quality of life (HRQoL) is therefore crucial for healthcare decision-making.
The HRQoL outcomes of treatments are often compared and valued using quality-adjusted life years (QALYs), an outcome combining measures of both the length and quality of life. When small differences in overall survival exist between two treatment options, the instruments used to value quality of life, the selection of underlying trial population (and associated survival analysis), and the choice of modeling technique can drastically affect the outcome and interpretation of health economic analyses. This is particularly apparent when considering the incremental cost-effectiveness ratio (ICER) as the key outcome measure, where changes in the directionality of the QALY outcomes may determine whether an intervention is, for example, more costly and more effective (and therefore potentially also cost-effective) or more costly and less effective (ie, dominated).2
Unresectable hepatocellular carcinoma (HCC) is a condition associated with a poor survival prognosis, and advances in therapy able to prolong the life expectancy of patients have been notably difficult to achieve in HCC.3 The challenges arising from the comparison of technologies between which no significant overall survival difference has been established have recently been illustrated in two health technology assessments (HTA) in unresectable HCC from the National Institute for Health and Care Excellence (NICE) and the French Haute Autorité de Santé (HAS). NICE recently conducted a multiple technology appraisal (MTA) that included an evaluation of the cost-utility of selective internal radiation therapy (SIRT) versus sorafenib in the treatment of patients with unresectable HCC.4 The cost-utility analysis showed that SIRT would result in a reduction of 0.076 QALYs versus sorafenib, contradicting a 2018 analysis by HAS, which concluded that SIRT using SIR-Spheres Y-90 resin microspheres was associated with an improvement of 0.023 QALYs versus sorafenib based on models using data from the same two Phase III randomized controlled trials (RCTs).5–7 This raises questions about the influence of the selection of clinical data, survival modeling techniques, and quality of life modeling on healthcare decision-making.
In the present study, we aimed to identify cost-utility analyses comparing SIRT using SIR-Spheres Y-90 resin microspheres versus systemic therapy in patients with unresectable HCC and to compare the modeled incremental QALY outcomes between the two therapies. The comparison of SIRT and systemic therapies for unresectable HCC was selected because a recent systematic literature review (SLR) and network meta-analysis confirmed that only two RCTs have been conducted comparing these interventions (specifically SIR-Spheres Y-90 resin microspheres and sorafenib). This limited availability of RCT data restricts the drivers of differences in modeled QALYs to the selection of the trial population, HRQoL measures, and the modeling approaches employed, rather than different underlying clinical data.8
Methods
An SLR was conducted to identify cost–utility studies of SIRT using SIR-Spheres Y-90 resin microspheres versus systemic therapies in the treatment of unresectable HCC. Search terms were designed using a combination of free-text and Medical Subject Heading (MeSH) terms aligned with those employed by NICE in the SLR conducted as part of the HCC MTA.4,9 PubMed, EMBASE, and the Cochrane Collaboration databases were searched on 3 March 2020 for studies published between 2017 and the search date, with results being collated and de-duplicated using Sourcerer (Covalence Research Ltd, London, UK).10 The database searches were identical to those conducted as part of the SLR registered in PROSPERO under ID CRD42020179826.11 Results from the searches were combined with the economic studies identified during the NICE SLR conducted for the MTA of SIRT in the treatment of HCC, which covered the period from 2000 to January 2019. The overlap between the NICE searches and the new searches conducted for the present study (covering the period 2017 and 2018) allowed the agreement between the search strategies and study retrieval to be validated, with the new search then also extending the coverage of the NICE search by 14 months. Hand searches of prominent HTA agency websites were also conducted, covering NICE in the UK, HAS in France, Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG) in Germany, Agenzia Italiana del Farmaco (AIFA) in Italy, Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) in Spain, Medical Services Advisory Committee (MSAC) in Australia, and Canadian Agency for Drugs and Technologies in Health (CADTH).
The titles and abstracts of the unique studies retrieved from the searches were screened by two independent reviewers against a pre-specified set of inclusion/exclusion criteria. Full-text versions of the remaining included studies were retrieved and screened against the same inclusion/exclusion criteria to determine the final inclusion status. Any discrepancies between reviewers were resolved by discussion. Incremental QALY outcomes were extracted from the included studies, and the magnitudes of incremental QALYs were ranked in descending order to illustrate the range and distribution of values.
Results
The SLR retrieved 1140 studies across PubMed, EMBASE, and Cochrane Collaboration databases, of which 84 were duplicates, leaving 1056 studies for screening. After title and abstract screening, 15 studies were left that potentially met the inclusion criteria, with further full-text screening leaving four studies included.12–15 Two of the studies retrieved as congress abstracts were also published as a full manuscript after the search dates.16,17 In one of the manuscripts, by Marqueen et al, results differed substantially from those presented in the abstract and outcomes from both studies were therefore ultimately extracted to facilitate a comparison of the results.16 The additional two cost-utility analyses from NICE and HAS were identified through hand searches, giving a total of seven studies evaluating the cost-utility of SIR-Spheres Y-90 resin microspheres versus sorafenib in the treatment of HCC (Figure 1). Six of the seven included studies used clinical data obtained exclusively from the SARAH and SIRveNIB RCTs comparing SIR-Spheres Y-90 resin microspheres with sorafenib.6,7 The only study not based on SARAH or SIRveNIB assumed equal efficacy of sorafenib and SIR-Spheres Y-90 resin microspheres and modeled a QALY difference based on the incidence of adverse events from the SHARP trial of sorafenib and the ENRY study of SIR-Spheres Y-90 resin microspheres.14,18,19 Eighteen analyses from the seven studies were ultimately included for presentation in the present study, of which 14 were based on the overall trial populations, one assumed equal efficacy, and three were of subgroups of either patients with low tumor burden (LTB) and albumin-bilirubin (ALBI) grade 1, or patients receiving a tumor absorbed radiation dose of ≥100 Gy (referred to as an “optimized dosimetry” subgroup).
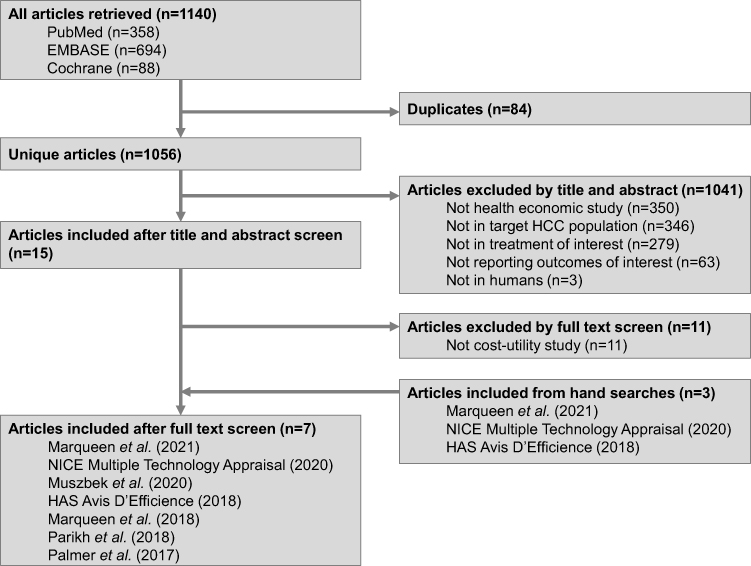 |
Figure 1 Systematic literature review flow diagram for the identification of cost–utility studies of selective internal radiation therapy versus systemic therapy in patients with hepatocellular carcinoma. Abbreviations: HAS, Haute Autorité de Santé; HCC, hepatocellular carcinoma; NICE, National Institute for Health and Care Excellence. |
Across the 14 analyses of the overall trial populations, the incremental quality of life estimates ranged from −0.09 to +0.28 QALYs (equivalent to spending between 4.7 fewer weeks and 14.6 more weeks in full health), with the negative end of the range favoring sorafenib over SIR-Spheres Y-90 resin microspheres, and the positive end favoring SIR-Spheres Y-90 resin microspheres over sorafenib (Figure 2). Notably, the 2019 Parikh et al study reported analyses at both ends of the range, with the −0.09 QALY difference driven by data from the SARAH intention-to-treat (ITT) population, and the +0.28 QALY difference driven by data from the SIRveNIB per protocol (PP) populations.12 The single analysis assuming equal efficacy reported a QALY difference of 0.0079 QALYs in favor of SIR-Spheres Y-90 resin microspheres, as it accounted for the favorable adverse event profile of SIR-Spheres Y-90 resin microspheres compared with sorafenib.
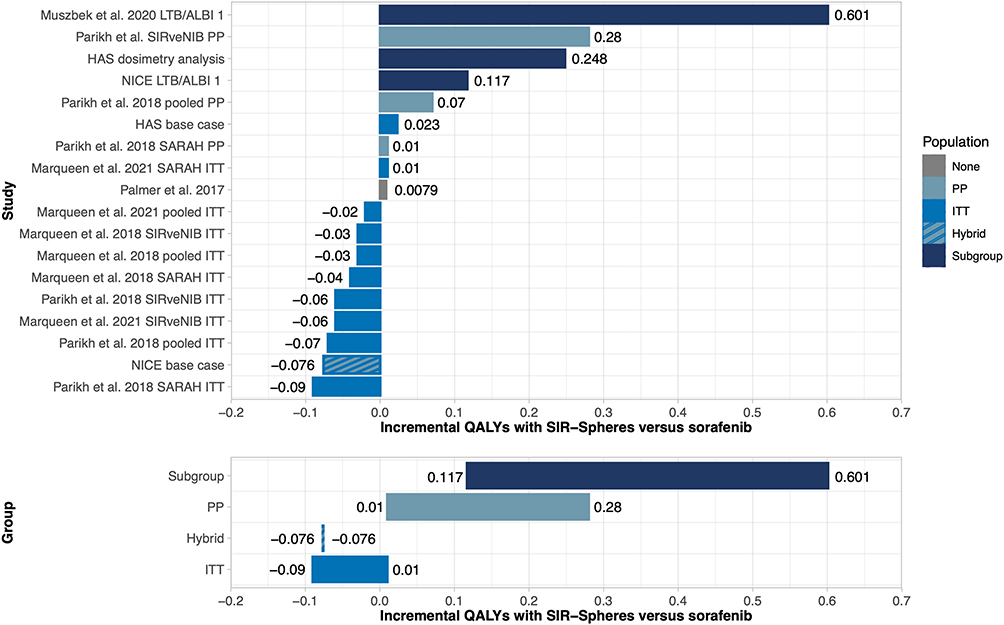 |
Figure 2 Incremental quality-adjusted life years gained with SIR-Spheres Y-90 resin microspheres versus sorafenib in the treatment of patients with hepatocellular carcinoma. Abbreviations: ALBI, albumin-bilirubin grade; HAS, Haute Autorité de Santé; ITT, intention-to-treat; LTB, low tumor burden; NICE, National Institute for Health and Care Excellence; PP, per protocol. Notes: In the case of the NICE base case analysis, “hybrid” reflects the use of data from the ITT population in the sorafenib arm of the analysis, in concert with data from the PP population in the SIR-Spheres Y-90 resin microsphere arm of the analysis. |
When including the three subgroup analyses, the upper end of the range (favoring SIR-Spheres Y-90 resin microspheres) increased to +0.601 QALYs in a subgroup analysis in patients with LTB ALBI grade 1.20 Only seven of the eighteen analyses reported confidence intervals around the ICER.13,14,16
Discussion
The SLR identified seven studies evaluating the cost-utility of SIR-Spheres Y-90 resin microspheres versus sorafenib in the treatment of unresectable HCC, six of which were based on data from SARAH and SIRveNIB RCTs. Across the 15 analyses included in the present synthesis not based on specific subgroups, incremental QALYs ranged from −0.09 to +0.28 with SIR-Spheres Y-90 resin microspheres versus sorafenib. Both bounds of the range arose from different analyses in the same modeling study, with the difference between the two extremes being driven exclusively by the choice of the trial analysis population. When including analyses based on either LTB/ALBI grade 1 or optimized dosimetry sub-groups, the range widened on the positive end to +0.601 QALYs in favor of SIR-Spheres Y-90 resin microspheres versus sorafenib. A key strength of the present study was the systematic identification of incremental QALY outcomes across seven studies comparing SIR-Spheres Y-90 resin microspheres with sorafenib, interventions for which head-to-head data were only available from two RCTs. This limited the available data on which health economic comparisons could be based, and thereby focused on differences beyond trial selection; however, this could also be considered a weakness of the study in that the scope of the review was relatively narrow given the recent growth of the HCC armamentarium to include lenvatinib and atezolizumab-bevacizumab.
The recent NICE appraisal of SIR-Spheres Y-90 resin microspheres versus sorafenib reported a reduction of 0.076 QALYs with SIR-Spheres Y-90 resin microspheres relative to sorafenib, ranking as the 13th least favorable of the 14 analyses based on the overall trial populations (ie, not sub-groups). In the discussion of previous health economic evidence comparing SIRT with sorafenib, the NICE appraisal report noted that “results may be very sensitive to different assumptions around survival or HRQoL”. Given that this sensitivity was known ahead of time, the efforts to characterize uncertainty around the analysis conducted by the Assessment Group on behalf of NICE were not extensive, likely falling short of health economic reporting guidelines codified in the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist (specifically item 20b on the characterization of uncertainty).21 No confidence or credible intervals were reported around any of the base case or scenario analyses conducted by NICE, and scatterplots from probabilistic sensitivity analyses were not presented, thereby frustrating efforts to understand the modeled distributions of incremental QALY outcomes. Regarding the overall assessment of cost-effectiveness, the final appraisal determination noted that the NICE committee “took this uncertainty into consideration in its decision-making”, but based on the minimal extent to which measures of uncertainty were presented, the committee must either have been restricted to a qualitative rather than quantitative assessment of the uncertainty or had access to uncertainty measures that are not in the public domain.22
Further to these methodological and reporting considerations, the present review highlights that the comparison of interventions with distinct modalities (a molecular-targeted agent versus a locoregional transarterial intervention) can have additional implications for economic modeling. In this instance, high proportions of patients in the ITT populations of the SARAH and SIRveNIB trials did not ultimately go on to receive SIRT (22.4% and 28.6% respectively), much higher than the proportions not ultimately receiving sorafenib (2.8% and 9.0% respectively). In most cases, this was because patients enrolled into and randomized within these trials were ultimately deemed ineligible for SIRT after an initial work-up phase performed after randomization. Patient selection for these trials may therefore not reflect the current clinical practice of SIRT, in which approximately 10% of patients are considered ineligible after their work-up.23 In this context, economic models including per protocol analyses (in which all patients received their allocated treatment) or post hoc subgroup analyses focused on patients most likely to receive and benefit from the intervention are most appropriate to ensure the external validity of their outcomes. This aspect of patient selection is particularly pertinent for the present example comparing SIR-Spheres Y-90 resin microspheres versus sorafenib, as all the models resulting in a negative QALY outcome were based at least in part on unselected populations, such as the full ITT population of the SARAH and/or SIRveNIB trials. Analyses conducted exclusively in PP or subgroup analyses resulted in QALY gains for SIR-Spheres Y-90 resin microspheres. Methodological approaches and selection of specific trial populations and utility values may legitimately differ between different healthcare systems (or even different treatment centers within the same system), but should always be justified, and ideally validated with local clinical input.
Further to considerations around the ITT and PP populations, patients randomly assigned to the SIR-Spheres Y-90 resin microsphere arm who went on to receive the treatment, waited a median time of 21 and 29 days after randomization before receiving treatment, compared with a median time of 3 and 7 days to receive sorafenib in SIRveNIB and SARAH, respectively.24 Importantly for the present analysis, these treatment initiation delays of approximately three weeks were not captured or adjusted for in either the ITT or PP analyses of the trials. Given the NICE finding of a difference of 3.76 quality-adjusted weeks of life between the two treatments, for example, a 3-week delay in initiation of one treatment should not be discounted when interpreting the findings. This consideration is particularly important because clinical practice of SIRT with SIR-Spheres Y-90 resin microspheres has recently been evolving to allow patients to be treated during the same hospital admission as their work-up, whether in an inpatient or outpatient setting.25
The wide range of incremental quality of life estimates spanning parity raises further considerations on the reporting of health economic analyses. The present study found that only two of the included studies (detailing seven of the included analyses) reported confidence intervals around the ICERs. Given the underlying clinical data and the precedent for directionally opposite findings from the same clinical trials illustrated by Parikh et al in 2018, the importance of characterizing uncertainty around the findings cannot be overstated. Given the diverse array of drivers of QALY outcomes, all possible sources of uncertainty should be explored, including population-level heterogeneity, first-order uncertainty, second-order parameter uncertainty, and structural uncertainty in the model.26
In conclusion, there are numerous factors that can contribute to differences in modeled incremental QALY outcomes. Across the studies included in the present analysis, incremental QALY outcomes ranged from −0.09 to +0.28 QALYs in analyses based on the ITT or PP populations. Analyses based on patient subgroups yielded substantially higher QALY outcomes for SIR-Spheres Y-90 resin microspheres compared to sorafenib, ranging from +0.117 to +0.601 QALYs. These outcomes demonstrate that appropriate patient selection can translate into meaningful improvements in the quality-adjusted life expectancy of patients with unresectable HCC in real-world clinical practice. In addition, the wide variations in QALY outcomes underline the importance of analyzing and presenting all of the factors driving QALY differences in line with best practice guidelines on the reporting of economic evaluations, such as those outlined in the CHEERS statement and checklist, especially in analyses in which the QALY difference is close to zero.
Acknowledgments
The abstract of this paper was presented at Virtual ISPOR 2021 (May 17–20, 2021) as poster presentation PCN133. The abstract was subsequently published in Value in Health, Volume 24, Issue 5, S1 (May 2021).
Funding
This manuscript was supported by consultancy fees from Sirtex Medical United Kingdom Ltd.
Disclosure
Mr Richard F Pollock is the sole director of Covalence Research Ltd, which received consultancy fees from Sirtex Medical United Kingdom Ltd (the manufacturer of SIR-Spheres Y-90 resin microspheres) to conduct the literature review, extract the data, and prepare the figures and manuscript. Mr Fabien Colaone, Dr Victoria K Brennan, and Dr Ion Agirrezabal are full-time employees of Sirtex Medical United Kingdom Ltd. Ms Suki Shergill is a director and full-time employee of Sirtex Medical United Kingdom Ltd. The authors report no other conflicts of interest in this work.
References
1. Collins M, Latimer N. NICE’s end of life criteria: who gains, who loses? BMJ. 2013;346(mar21 1):f1363. doi:10.1136/bmj.f1363
2. Paulden M. Calculating and interpreting ICERs and net benefit. Pharmacoeconomics. 2020;38(8):785–807. doi:10.1007/s40273-020-00914-6
3. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
4. National Institute for Health and Care Excellence. Selective internal radiation therapies for treating hepatocellular carcinoma [TA688]. Available from: https://www.nice.org.uk/guidance/ta688/.
5. Haute Autorité de Santé. SIR-Spheres® (Y-90 resin microspheres) Traitement du carcinome hépatocellulaire inoperable. Available from: https://www.has-sante.fr/upload/docs/application/pdf/2019-03/sir-spheres_11122018_avis_efficience.pdf.
6. Vilgrain V, Pereira H, Assenat E, et al.; SARAH Trial Group. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled Phase 3 trial. Lancet Oncol. 2017;18(12):1624–1636. doi:10.1016/S1470-2045(17)30683-6
7. Chow PKH, Gandhi M, Tan SB, et al.; Asia-Pacific Hepatocellular Carcinoma Trials Group. SIRveNIB: selective internal radiation therapy versus sorafenib in Asia-Pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36(19):1913–1921. doi:10.1200/JCO.2017.76.0892
8. Pollock RF, Brennan VK, Shergill S, Colaone F. A systematic literature review and network meta-analysis of first-line treatments for unresectable hepatocellular carcinoma based on data from randomized controlled trials. Expert Rev Anticancer Ther. 2021;21(3):341–9. doi:10.1080/14737140.2021.1842204
9. Wade R, Sharif-Hurst S, Harden M, et al. Methods for selecting the best evidence to inform a NICE technology appraisal on selective internal radiation therapies for hepatocellular carcinoma. Syst Rev. 2020;9(1):184. doi:10.1186/s13643-020-01447-x
10. Covalence Research Ltd. Sourcerer. London, UK; 2021. Available from: https://sourcerer.pro.
11. Pollock RF. A systematic review and network meta-analysis of selective internal radiation therapy in the treatment of unresectable hepatocellular carcinoma based on randomized controlled trials. PROSPERO 2020 CRD42020179826. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020179826.
12. Parikh ND, Singal AG, Kulik LM, Hutton D. PS4-15 cost-effectiveness of sorafenib versus selective internal radiation therapy for patients with advanced hepatocellular carcinoma. Med Decis Making. 2019;39(1):E188–9.
13. Marqueen KE, Ang C, Mazumdar M, Buckstein M, Ferket BS. Cost-effectiveness analysis of selective internal radiation therapy with yttrium-90 resin microspheres versus sorafenib in advanced hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2018;102(3):e402. doi:10.1016/j.ijrobp.2018.07.1185
14. Palmer D, Ross P, Shah T, et al. Cost effectiveness of selective internal radiation therapy (SIRT) with Y- 90 resin microspheres versus sorafenib in Barcelona Clinic Liver Cancer (BCLC) stage C hepatocellular carcinoma patients in the UK. Ann Oncol. 2017;28(Suppl. 5):239–240. doi:10.1093/annonc/mdx369.087
15. Muszbek N, Remak E, Evans R, Brennan V, Colaone F, Shergill S. Cost-utility analyis (sic) of selective internal radiation therapy (SIRT) with Y-90 resin microspheres in hepatocellular carcinoma (HCC). Value Health. 2019;22(3):S452. doi:10.1016/j.jval.2019.09.280
16. Marqueen KE, Kim E, Ang C, Mazumdar M, Buckstein M, Ferket BS. Cost-effectiveness analysis of selective internal radiotherapy with yttrium-90 versus sorafenib in locally advanced hepatocellular carcinoma. JCO Oncol Pract. 2021;17(2):e266–e277. doi:10.1200/OP.20.00443
17. Muszbek N, Remak E, Evans R, et al. Cost-utility analysis of selective internal radiation therapy with Y-90 resin microspheres in hepatocellular carcinoma. Future Oncol. 2021;17(9):1055–1068. doi:10.2217/fon-2020-1004
18. Golfieri R, Bilbao JI, Carpanese L, et al.; European Network on Radioembolization with Yttrium-90 Microspheres (ENRY) study collaborators. Comparison of the survival and tolerability of radioembolization in elderly vs. younger patients with unresectable hepatocellular carcinoma. J Hepatol. 2013;59(4):753–761. doi:10.1016/j.jhep.2013.05.025
19. Llovet JM, Ricci S, Mazzaferro V, et al.; SHARP Investigators Study Group. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
20. Palmer DH, Hawkins NS, Vilgrain V, Pereira H, Chatellier G, Ross PJ. Tumor burden and liver function in HCC patient selection for selective internal radiation therapy: SARAH post-hoc study. Future Oncol. 2020;16(1):4315–4325. doi:10.2217/fon-2019-0658
21. Husereau D, Drummond M, Petrou S, et al.; CHEERS Task Force. Consolidated health economic evaluation reporting standards (CHEERS) statement. Value Health. 2013;16(2):e1–5. doi:10.1016/j.jval.2013.02.010
22. National Institute for Health and Care Excellence. Selective internal radiation therapies for treating hepatocellular carcinoma [TA688]. Final appraisal determination. Available from: https://www.nice.org.uk/guidance/ta688/documents/final-appraisal-determination-document.
23. Sancho L, Rodriguez-Fraile M, Bilbao JI, et al. Is a technetium-99m macroaggregated albumin scan essential in the workup for selective internal radiation therapy with yttrium-90? an analysis of 532 patients. J Vasc Interv Radiol. 2017;28(11):1536–1542. doi:10.1016/j.jvir.2017.07.019
24. Sposito C, Mazzaferro V. The SIRveNIB and SARAH trials, radioembolization vs. sorafenib in advanced HCC patients: reasons for a failure, and perspectives for the future. Hepatobiliary Surg Nutr. 2018;7(6):487–489. doi:10.21037/hbsn.2018.10.06
25. Li MD, Chu KF, DePietro A, et al. Same-day yttrium-90 radioembolization: feasibility with resin microspheres. J Vasc Interv Radiol. 2019;30(3):314–319. doi:10.1016/j.jvir.2018.10.016
26. Briggs AH, Weinstein MC, Fenwick EA, Karnon J, Sculpher MJ, Paltiel AD; ISPOR-SMDM Modeling Good Research Practices Task Force. Model parameter estimation and uncertainty analysis: a report of the ISPOR-SMDM modeling good research practices task force working group-6. Med Decis Making. 2012;32(5):722–732. doi:10.1177/0272989X12458348
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.