")
Back to Journals » Open Access Journal of Sports Medicine » Volume 8
Effects of prophylactic ankle and knee braces on leg stiffness during hopping
Authors Hobara H, Hashizume S, Kobayashi Y
Received 12 January 2017
Accepted for publication 2 February 2017
Published 26 April 2017 Volume 2017:8 Pages 107—112
DOI https://doi.org/10.2147/OAJSM.S132275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff

Hiroaki Hobara, Satoru Hashizume, Yoshiyuki Kobayashi
Human Informatics Research Institute, National Institute of Advanced Industrial Science and Technology, Tokyo, Japan
Abstract: During human movement, the leg can be represented as a mechanical spring, with its stiffness potentially contributing to sports performance and injury prevention. Although many individuals perform athletic activities with joint stabilizers, little is known about the effects of prophylactic lower extremity braces on leg stiffness. The objective of this study was to investigate the effect of ankle and/or knee braces on leg stiffness measured during one-legged hopping at a range of frequencies. Thirteen male participants performed one-legged hopping with their dominant leg at frequencies of 2.2, 2.6, and 3.0 Hz. All participants were randomly tested under the following four brace conditions: 1) no brace (control), 2) prophylactic ankle brace, 3) prophylactic knee brace, and 4) prophylactic ankle and knee braces. Based on a spring–mass model, leg stiffness was calculated using data from an accelerometer. It was found that leg stiffness increased with increasing hopping frequency for each brace condition. However, there were no significant differences in leg stiffness among the four brace conditions at the three hopping frequencies. Since some level of leg stiffness is needed for optimal athletic performance and training, these results suggest that ankle and knee braces do not significantly interfere with dynamic hopping activities.
Keywords: spring–mass model, injury prevention, compensatory strategy
Introduction
Since many individuals perform athletic activities with joint stabilizers, prophylactic ankle and knee braces are required to prevent lower extremity injury without interfering athletic performance in sport activities. Previous studies have reported that semirigid or soft ankle braces do not significantly affect a person’s jumping performance.1,2 Furthermore, several studies have demonstrated that prophylactic knee braces do not significantly inhibit athletic performance during a stop–jump task,3 cross-over hop, or one-legged vertical jump.4,5 However, little is known about the effects of prophylactic lower extremity braces on one-legged hopping, which involves typical spring-like behavior of the legs.
During hopping and jumping activities, the legs of a human exhibit characteristics similar to those of a spring. The leg spring is compressed during the first half of the stance phase and rebounds during the second half. Leg stiffness (Kleg), which is defined as the ratio of the peak ground reaction force to the maximum center of mass vertical displacement at the middle of the stance phase,6 has been shown to increase with increasing hopping height.7–9 Kleg is also correlated to agility and speed during sprint running.10–14 Previous studies have suggested that endurance training enhances Kleg,15,16 but that plyometrics training has a greater influence on Kleg than endurance training.17–20 Therefore, a better understanding of Kleg regulation would provide us with a basis for better evaluation of the changes in stiffness that accompany training regimes and would allow for the development of more effective training methods.
A previous study has shown that neither prophylactic ankle taping nor bracing affects Kleg during hopping at frequencies of 2.3–3.0 Hz.1 However, in that study, the authors only investigated the effects of an ankle stabilizer on Kleg during hopping. Therefore, it remains unclear whether Kleg during hopping is affected by knee braces or by a combination of ankle and knee braces during hopping. The objective of this study was to investigate the effect of ankle and/or knee braces on leg stiffness measured during one-legged hopping at a range of frequencies. We hypothesized that Kleg would not vary during hopping with ankle and/or knee bracing over a wide range of hopping frequencies.
Methods
Participants
Thirteen healthy male subjects with no known neuromuscular disorders or lower-limb functional limitations participated in this study. The physical characteristics of the participants were as follows: age, 26.5±5.2 years; height, 1.75±0.06 m; and body mass, 66.08±8.43 kg (mean ± standard deviation). We only included subjects on whose legs currently available prophylactic joint braces fitted. All participants were either sedentary or mildly active; none had been involved in any type of regular exercise or training for at least 1 year prior to the test. All participants provided written informed consent prior to the study, which had in turn received institutional ethical approval (Environment and Safety Headquarters, Safety Management Division, AIST).
Ankle and knee braces
In our study, commercially available ankle braces (Ankle Guard-Soft; ALCARE, Tokyo, Japan) and knee braces (Knee Guard-Ligament 3; ALCARE) were used to stabilize the ankle and knee joints, respectively (Figure 1). The Ankle Guard-Soft provides medial support of the ankle via a half figure-eight lift, horseshoe, and stirrup straps that encompass the ankle to prevent inversion and joint laxity. The Knee Guard-Ligament 3 provides anterior support to the knee joint via interconnected anchor straps on the thigh and shank with medial plastic stays, which constrain anterior perturbation and joint laxity. To minimize within-subject and between-subject variations, the ankle and knee braces were fitted and checked by a single tester.
 | Figure 1 Ankle brace and knee brace used in this study. Notes: (A) Lateral view ankle brace, (B) medial view ankle brace, and (C) anterolateral view knee brace. |
Task and procedure
Prior to the experiment, limb dominance was determined by asking the participants which leg they preferred to use when kicking a ball, and the limb reported by the participant was identified as the dominant leg.21,22 After being fitted with the braces, the participants immediately moved to the experiment area. Each participant completed the testing by performing one-legged hopping under the following four brace conditions: 1) no braces (NBR), 2) prophylactic ankle brace (ANK), 3) prophylactic knee brace (KNE), and 4) prophylactic ankle and knee braces (A&K). The brace conditions and hopping frequencies were randomized.
The participants were instructed to perform one-legged hopping in place on their dominant leg with their arms akimbo. During each trial, a hopping frequency of 2.2, 2.6, or 3.0 Hz was maintained using a digital metronome. We chose these frequencies because a range of 2.2–3.0 Hz was the broadest possible metronome beat frequency range that the subjects could follow and because we considered a spring–mass model to be appropriate for modeling the activity in this range.8 Because different contact time instructions can affect stiffness regulation during hopping at a given hopping frequency,7,9 the participants were asked to hop for as short a contact time as possible. Before data were collected, all participants were instructed to practice for as long as necessary until they felt comfortable with the task. All participants practiced for 3–4 min and reported that the practice session had sufficiently prepared them.
Data collection and analysis
Data collected during 10 consecutive hops per brace condition were used in the analyses. According to a previous study,6 Kleg can be calculated using a spring–mass model (Figure 2). We used an accelerometer (Myotest®; Myotest SA, Sion, Switzerland) to estimate Kleg during hopping for each subject and brace condition. The Myotest device (dimensions: 5.4×10.2×11.1 cm; weight: 58 g) contains a three-dimensional inertial accelerometer (68 g) that allows vertical acceleration to be recorded at a sampling frequency of 500 Hz. The acceleration data obtained were used to estimate the contact and flight times. The Kleg during hopping can be indirectly calculated by an estimation equation.23 In the equation, Kleg was calculated by modeling the ground reaction force as a sine wave as it is expected from oscillation of pure spring–mass model. Therefore, Kleg during hopping was calculated as follows:
|
|
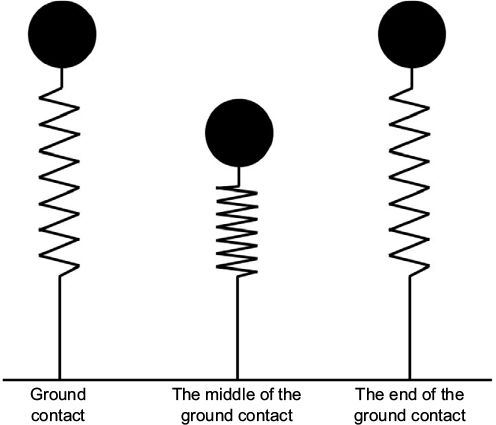 | Figure 2 Spring–mass model for hopping. Notes: This model consists of a body mass and a massless linear spring that supports the body mass. The mass is equivalent to the body mass. The model is shown at the beginning of the ground contact phase (left), the middle of the ground contact phase (middle), and the end of the ground contact phase (right). |
where m is the total body mass, tc is the ground contact time, and tf is the flight time.23 The device was attached so that it was perpendicular to a large (8.5 cm) Velcro elastic belt. The device was fixed at the hip level on the left side of the body, as recommended by the manufacturer.24 The reliability and validity of the device were examined in previous studies.24–26
Statistics
A two-way (frequency × braces) repeated-measures analysis of variance (ANOVA) was performed to compare Kleg for the four brace conditions. To assess the validity of the assumptions inherent in the ANOVA, Mauchly’s test of sphericity was performed using all of the ANOVA results. The Greenhouse–Geisser correction was used to adjust the number of degrees of freedom if an assumption was violated, and Bonferroni’s post hoc test for multiple comparisons was used if a significant main effect was observed. Statistical significance was set at P<0.05. We calculated the effect sizes (ES) for each ANOVA. SPSS for Windows, version 19 (SPSS Inc., Chicago, IL, USA) was used for all of the statistical analyses.
Results
The statistical analyses revealed the existence of a significant main effect of the hopping frequency on Kleg (F(1.17, 14.01)=55.03, P<0.01, ES=0.82). Kleg was greatest at a frequency of 3.0 Hz, followed by 2.6 and 2.0 Hz (P<0.01 for all frequencies; Figure 3). However, there was no significant main effect of the brace condition on Kleg (F(3.00, 36.00)=0.23, P=0.87, ES=0.02), nor was there a significant interaction effect between the hopping frequency and the brace condition (F(6.00, 72.00)=0.49, P=0.82, ES=0.04).
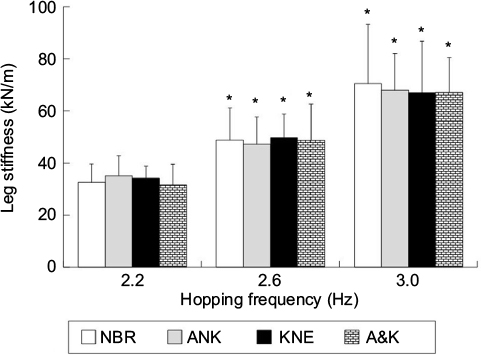 | Figure 3 Comparison of leg stiffness among the four brace conditions at three hopping frequencies. Note: The symbol “*”denotes significant differences between adjacent frequencies for each brace condition (P<0.01). Abbreviations: NBR, no braces; ANK, prophylactic ankle brace; KNE, prophylactic knee brace; A&K, prophylactic ankle and knee braces. |
Discussion
The objective of this study was to investigate the effect of ankle and/or knee braces on leg stiffness measured during one-legged hopping at a range of frequencies. We found that Kleg increased with increasing hopping frequency for each brace condition, but there were no significant differences in Kleg among the different brace conditions (Figure 3). The results support our initial hypothesis, which was that for a wide range of hopping frequencies, Kleg would be invariant when ankle and/or knee braces were worn. Given that prophylactic braces are used extensively for prevention and treatment of soft tissue injuries of the lower extremities, it is interesting to discover that wearing prophylactic lower-extremity braces does not impede Kleg during dynamic tasks.
One possible explanation for the invariance of Kleg when prophylactic braces are worn is the intralimb compensation strategy. A previous study compared Kleg between low-cost (relatively higher stiffness) and high-cost (relatively lower stiffness) footwear.27 The authors found no significant differences in Kleg between the two types of footwear during hopping at a frequency of 2.2 Hz. This suggests that the lower extremity adapts to maintain a comfortable level of stiffness. Previous studies have also shown that Kleg remains invariant during hopping while wearing different types of spring-loaded ankle–foot orthoses.21,28 The results of these studies suggest that humans maintain invariant Kleg by employing various intralimb compensation strategies that are specific to the nature of the joint loading. Williams and Riemann1 found that prophylactic ankle taping and bracing did not affect the participants’ Kleg or spring–mass characteristics during hopping, which suggests that the participants maintained similar spring–mass characteristics by compensating with increased knee and hip range of motions (ROMs). Hence, it is reasonable to assume that invariant Kleg observed during wearing of ankle and/or knee braces is attributable to intralimb compensatory strategies involving the proximal knee and hip joints. The mechanisms that humans employ to maintain invariant Kleg while wearing braces should be examined in future research.
A second possible explanation for invariant Kleg with ankle and/or knee braces is that the braces used in this study did not restrict hopping movement in the sagittal plane. According to a previous study, the biomechanical characteristics of a hopping movement can be described in the sagittal plane.29 However, the ankle (Ankle Guard-Soft) and knee braces (Knee Guard-Ligament 3) used in this study provide medial support to the ankle and anterior support to the knee joint. Hence, the results of this study could be attributable to the fact that the braces we used did not influence the joint motion in the sagittal plane.
A third possible explanation for the invariant Kleg is that the performance deterioration caused by wearing braces was offset within each joint. Several studies have demonstrated that braces can have detrimental effects on vertical jump performance.30–32 Conversely, previous studies have suggested that ankle supports not only provide mechanical stabilization of the ankle joint but may also improve proprioceptive input by stimulation of the cutaneous mechanoreceptors around the ankle.33–35 Previous studies have also shown that prophylactic knee braces enhance proprioception, coordination, maximal force, and balance.36–38 Consequently, the possible negative effects of the braces may be offset within each joint.
There are certain limitations of this study that must be taken into account when interpreting the results. First, the detailed mechanisms of how subjects maintained constant Kleg during hopping under the four brace conditions at the three hopping frequencies could not be determined in this study. Although we found Kleg to be invariant with respect to the brace conditions and hopping frequencies considered in this study, Kleg, that is, the stiffness of a multijointed system, also depends on the combination of torsional stiffnesses of the joints.39,40 Joint stiffness is also influenced by changes in the touchdown joint angle, pre-activity (muscle activity before ground contact), and muscle activity, including the short-latency stretch reflex response in the leg extensors upon landing.29,40 Additional biomechanical monitoring, such as joint kinetics/kinematics measurements, electromyography, and ultrasonography, is needed to address these limitations. Second, our participants moved immediately into the experiment area after being fitted for each brace condition to perform one-legged hopping. Although no participants reported any loose braces around the ankle and knee joints, it is difficult to know with certainty whether the braces were fully snugly fitted to each participant for each of the brace conditions. The ankle and/or knee braces may have become loose during movement to an extent that motion within the normal ankle or knee sagittal-plane ROM occurred during the hopping, allowing normal Kleg response. In future research, examining the effects of several ankle and knee braces on Kleg during hopping, this possibility should be accounted for by double checking the fit of the braces. Finally, the current results and interpretations in this study are based on the chosen braces (Ankle Guard-Soft and Knee Guard-Ligament 3). Thus, caution should be exercised in interpretation and generalization of these findings to other braces. Further research is required on whether and how Kleg changes with other prophylactic ankle and knee braces.
Conclusion
In summary, our results suggest that during a one-legged hopping task, neither prophylactic ankle nor knee bracing affects Kleg over a range of hopping frequencies. Evidently, additional research is necessary to determine the mechanisms responsible for the invariance of Kleg when ankle, knee braces, and combination of both ankle and knee braces are worn.
Acknowledgment
This study was partly supported by a priority project in National Institute of Advanced Industrial Science and Technology and JSPS KAKENHI Grant Number 26702027.
Disclosure
The authors report no conflicts of interest in this work.
References
Williams S, Riemann BL. Vertical leg stiffness following ankle taping and bracing. Int J Sports Med. 2009;30(5):383–386. | ||
Rosenbaum D, Kamps N, Bosch K, Thorwesten L, Völker K, Eils E. The influence of external ankle braces on subjective and objective parameters of performance in a sports-related agility course. Knee Surg Sports Traumatol Arthrosc. 2005;13(5):419–425. | ||
Yu B, Herman D, Preston J, Lu W, Kirkendall DT, Garrett WE. Immediate effects of a knee brace with a constraint to knee extension on knee kinematics and ground reaction forces in a stop-jump task. Am J Sports Med. 2004;32(5):1136–1143. | ||
Mortaza N, Abu Osman NA, Jamshidi AA, Razjouyan J. Influence of functional knee bracing on the isokinetic and functional tests of anterior cruciate ligament deficient patients. PLoS One. 2013;8(5):e64308. | ||
Mortaza N, Ebrahimi I, Jamshidi AA, et al. The effects of a prophylactic knee brace and two neoprene knee sleeves on the performance of healthy athletes: a crossover randomized controlled trial. PLoS One. 2012;7(11):e50110. | ||
Blickhan R. The spring-mass model for running and hopping. J Biomech. 1989;22(11–22):1217–1227. | ||
Arampatzis A, Schade F, Walsh M, Brüggemann GP. Influence of leg stiffness and its effect on myodynamic jumping performance. J Electromyogr Kinesiol. 2001;11(5):355–364. | ||
Farley CT, Blickhan R, Sato J, Taylor CR. Hopping frequency in humans: a test of how springs set stride frequency in bouncing gaits. J Appl Physiol (1985). 1991;71(6):2127–2132. | ||
Hobara H, Kanosue K, Suzuki S. Changes in muscle activity with increase in leg stiffness during hopping. Neurosci Lett. 2007;418(1):55–59. | ||
Bret C, Rahmani A, Dufour AB, Messonnier L, Lacour JR. Leg strength and stiffness as ability factors in 100 m sprint running. J Sports Med Phys Fitness. 2002;42(3):274–281. | ||
Chelly SM, Denis C. Leg power and hopping stiffness: relationship with sprint running performance. Med Sci Sports Exerc. 2001;33(2):326–333. | ||
Durand S, Ripamonti M, Beaune B, Rahmani A. Leg ability factors in tennis players. Int J Sports Med. 2010;31(12):882–886. | ||
Young W, Farrow D. A review of agility: practical applications for strength and conditioning. J Strength Cond Res. 2006;28(5):24–29. | ||
Hobara H, Tominaga S, Umezawa S, et al. Leg stiffness and sprint ability in amputee sprinters. Prosth Orth Int. 2012;36(3):312–317. | ||
Girard O, Millet G, Slawinski J, Racinais S, Micallef JP. Changes in leg-spring behavior during a 5000 m self-paced run in differently trained athletes. Sci Sports. 2010;25(2):99–102. | ||
Hobara H, Kimura K, Omuro K, et al. Differences in lower extremity stiffness between endurance trained athletes and untrained subjects. J Sci Med Sport. 2010;13(1):106–111. | ||
Harrison AJ, Keane SP, Coglan J. Force-velocity relationship and stretch-shortening cycle function in sprint and endurance athletes. J Strength Cond Res. 2004;18(3):473–479. | ||
Hobara H, Kimura K, Omuro K, et al. Determinants of difference in leg stiffness between endurance- and power-trained athletes. J Biomech. 2008;41(3):506–514. | ||
Laffaye G, Bardy BG, Durey A. Leg stiffness and expertise in men jumping. Med Sci Sports Exerc. 2005;37(4):536–543. | ||
Rabita G, Couturier A, Lambertz D. Influence of training background on the relationships between plantarflexor intrinsic stiffness and overall musculoskeletal stiffness during hopping. Eur J Appl Physiol. 2008;103(2):163–171. | ||
Chang YH, Roiz RA, Auyang AG. Intralimb compensation strategy depends on the nature of joint perturbation in human hopping. J Biomech. 2008;41(9):1832–1839. | ||
Hobara H, Inoue K, Kanosue K. Effect of hopping frequency on bilateral differences in leg stiffness. J Appl Biomech. 2013;29(1):55–60. | ||
Dalleau G, Belli A, Viale F, Lacour JR, Bourdin M. A simple method for field measurements of leg stiffness in hopping. Int J Sports Med. 2004;25(3):170–176. | ||
Casartelli N, Müller R, Maffiuletti NA. Validity and reliability of the Myotest accelerometric system for the assessment of vertical jump height. J Strength Cond Res. 2010;24(11):3186–3193. | ||
Choukou MA, Laffaye G, Taiar R. Reliability and validity of an accelerometric system for assessing vertical jumping performance. Biol Sport. 2014;31(1):55–62. | ||
Ruggiero L, Dewhurst S, Bampouras TM. Validity and reliability of two field-based leg stiffness devices: implications for practical use. J Appl Biomech. 2016;32(4):415–419. | ||
Bishop M, Fiolkowski P, Conrad B, Brunt D, Horodyski M. Athletic footwear, leg stiffness, and running kinematics. J Athl Train. 2006;41(4):387–392. | ||
Ferris DP, Bohra ZA, Lukos JR, Kinnaird CR. Neuromechanical adaptation to hopping with an elastic ankle-foot orthosis. J Appl Physiol. 2006;100(1):163–170. | ||
Hobara H, Inoue K, Muraoka T, Omuro K, Sakamoto M, Kanosue K. Leg stiffness adjustment for a range of hopping frequencies in humans. J Biomech. 2010;43(3):506–511. | ||
Burks RT, Bean BG, Marcus R, Barker HB. Analysis of athletic performance with prophylactic ankle devices. Am J Sports Med. 1991;19(2):104–106. | ||
Paris DL. The effects of the Swede-O, New Cross, and McDavid ankle braces and adhesive ankle taping on speed, balance, agility, and vertical jump. J Athl Train. 1991;27(3):253–256. | ||
MacKean LC, Bell G, Burnham RS. Prophylactic ankle bracing vs. taping: effects on functional performance in female basketball players. J Orth Sports Phys Ther. 1995;22(2):77–81. | ||
Feuerbach JW, Grabiner MD, Koh TJ, Weiker GG. Effect of an ankle orthosis and ankle ligament anesthesia on ankle joint proprioception. Am J Sports Med. 1994;22(2):223–229. | ||
Heit EJ, Lephart SM, Rozzi SL. The effect of ankle bracing and taping on joint position sense in the stable ankle. J Sport Rehab. 1996;5(3):206–213. | ||
Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surg Sports Traumatol Arthrosc. 1995;3(1):39–46. | ||
Baltaci G, Aktas G, Camci E, Oksuz S, Yildiz S, Kalaycioglu T. The effect of prophylactic knee bracing on performance: balance, proprioception, coordination, and muscular power. Knee Surg Sports Traumatol Arthrosc. 2011;19(10):1722–1728. | ||
Ramsey DK, Wretenberg PF, Lamontagne M, Nemeth G. Electromyographic and biomechanic analysis of anterior cruciate ligament deficiency and functional knee bracing. Clin Biomech. 2003;18(1):28–34. | ||
Theoret D, Lamontagne M. Study on three-dimensional kinematics and electromyography of ACL deficient knee participants wearing a functional knee brace during running. Knee Surg Sports Traumatol Arthrosc. 2006;14(6):555–563. | ||
Butler RJ, Crowell HP, Davis IM. Lower extremity stiffness: implication for performance and injury. Clin Biomech. 2003;18(6):511–517. | ||
Farley CT, Houdijk HHP, Strien CV, Louie M. Mechanism of leg stiffness adjustment for hopping on surfaces of different stiffnesses. J Appl Physiol. 1998;85(3):1044–1055. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.