")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Effects of Patients’ Perceptions of Physician–Patient Relational Empathy on an Inflammation Marker in Patients with Crohn’s Disease: The Intermediary Roles of Anxiety, Self-Efficacy, and Sleep Quality
Authors Xu X, Zhang Y, Wang W, Zhang Y, Yang N
Received 1 July 2019
Accepted for publication 11 February 2020
Published 29 April 2020 Volume 2020:13 Pages 363—371
DOI https://doi.org/10.2147/PRBM.S221435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xianlin Xu,1,* Yan Zhang,2,* Wei Wang,3 Yin Zhang,1 Ningxi Yang2
1Department of Gastroenterology, Huiyang Sanhe Hospital, Huizhou, Guangdong, People’s Republic of China; 2College of Humanities and Social Sciences, Harbin Engineering University, Harbin, Heilongjiang, People’s Republic of China; 3School of Health Sciences, Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ningxi Yang 145 Nantong Road, Harbin, Heilongjiang, People’s Republic of China
Tel +86045182569608
Email [email protected]
Yin Zhang 3 Kanghe Road, Huizhou, Guangdong, People’s Republic of China
Tel +8607523800260
Email [email protected]
Background: Physician–patient empathy is inextricably linked with outcomes of patients. The purpose of this study was to test whether anxiety, self-efficacy, and sleep quality played intermediary roles in relationships between patients’ perceptions of physician–patient relational empathy and an inflammation marker in Crohn’s disease patients.
Methods: The study included 187 patients. At admission (T1) and 3 months after admission (T2), anxiety, self-efficacy, sleep, and the inflammatory marker IL6 of patients were tested and compared. Patients’ perceptions of physician–patient relational empathy (CARE scale) was measured at T2. Correlations among patients’ anxiety, self-efficacy, sleep quality, IL6, and CARE scores were explored by Pearson’s correlation analysis and a structural equation model.
Results: Compared with T1, patients showed higher self-efficacy and sleep quality and lower anxiety and IL6 at T2. Patients’ perceptions of physician–patient relational empathy were negatively related to anxiety and IL6 and connected to self-efficacy and sleep quality positively. Patients’ anxiety, self-efficacy, and sleep quality played intermediary roles incorrelations between empathy and IL6.
Conclusion: In correlations of patients’ perceptions of physician–patient relational empathy and IL6 in patients with Crohn’s disease, patients’ anxiety, self-efficacy, and sleep quality acted as intermediary effects. Therefore, medical staff should empathize with patients.
Keywords: empathy, Crohn’s disease, physician–patient communication, mental health
Introduction
Crohn’s disease (CD) is an intestinal inflammatory disease that may occur in any part of the gastrointestinal tract. Clinical manifestations are abdominal pain, diarrhea, and intestinal obstruction, which can be accompanied by fever, anemia, nutritional disorders, and parenteral damage, such as to joints, skin, eyes, oral mucosa, and the liver. This disease recurs repeatedly and cannot be cured completely.1 At the same time, the disease brings a lot of psychological pressure to patients, and patient-therapy efficacy is tightly associated with their psychological well-being.2 Therefore, it is very important to improve the mental health of patients.
Concern for patients’ mental health and emotional support are not only confined to professional psychological intervention but also reflected in daily communication, such as full empathy with patients. Empathy means understanding and coping with others’ situations from their standpoint in interpersonal communication.3 When facing the disease, patients experience both physical pain and psychological distress, as well as limitations in social adaptability. Therefore, they require more psychosocial support. When showing empathy to the patients, medical staff can understand specific situations of patients. On this basis, physicians can provide more targeted and humanistic treatment and care for patients. As such, both physicians and patients benefit.4 In addition, empathy embodies the humanistic care ability of physicians.5
Previous studies have paid attention to the impact of empathy of medical staff on patient-therapy effects. The good effect of physicians who have strong empathy with patients has been proved by former research. For instance, the inventor of the Jefferson Scale of Empathy, Hojat et al, found that patients with diabetes showed few acute metabolic complications, and low hemoglobin A1c and LDL-C if their physicians had strong empathy.6,7 Differently from those studies, which explored the impact of physician empathy on patient indicators, our research analyzed the influence of patient perceptions of physician–patient relational empathy on their psychological and physiological indicators and mechanisms.
IL6 has a significant function in the health evaluation of patients with inflammatory diseases.8 The relationships between IL6 and mental health have been confirmed.9 Therefore, this study focused on the effects of patient perceptions of physician–patient relational empathy on anxiety, self-efficacy, sleep, and IL6, and tested whether patient anxiety, self-efficacy, and sleep quality played intermediary roles in the relationship between patient perceptions of physician–patient relational empathy and IL6. We made two hypotheses: patient IL6 is affected by their perceptions of physician–patient relational empathy directly, and patient IL6 is affected by their perceptions of physician–patient relational empathy through the mediation of self-efficacy, anxiety, and sleep quality.
Methods
Participants
From July 2017 to June 2019, all patients with CD in several hospitals in the south of China were selected to participate in the research. Inclusion criteria were diagnosed with CD and hospitalized for 7 or more days because of CD, knew what disease they had and signed informed consent, prescription of mercaptopurine/azathioprine and/or mesalamine, and not on ongoing psychotropic medication. Exclusion criteria were other diseases that may act on emotion, sleep, and inflammatory markers, such as psychiatric disorders, Parkinson’s disease, malignant tumors, and acute infective diseases.
Procedures
Firstly, at admission (T1) and 3 months after admission (T2), data on patients’ anxiety, self-efficacy, sleep, disease activity, and IL6 were collected and compared. Patients recalled their hospitalization experience and completed the CARE scale at T2. Secondly, the influence of patients’ demographic characteristics and disease condition on IL6 were tested at T2. Thirdly, we used Pearson's correlation analysis and a structural equation model to test whether patients’ perceptions of physician–patient relational empathy scores affected their IL6 and explore the relationships among anxiety, self-efficacy, sleep quality, IL6, and patients’ perceptions of physician–patient relational empathy scores at T2.
Measures
Patients’ Essential Information
Patient demographic information comprised sex, age, marital status, education, residence, monthly income, and medical insurance. Disease- and treatment-related information was also collected: hospitalization days, hormone use, change of prescription, course of disease, and disease activity. Disease activity was evaluated based on the simple endoscopic score for CD, which is the sum of the scores of a number of segments. Patients with a score ≤3 were classed as in remission, while ≥4 meant their disease was active.10
Anxiety
We used the Hospital Anxiety and Depression Scale (HADS) to measure patients’ anxiety. The HADS is a self-evaluation scale that contains 14 questions. There are seven questions measuring anxiety (HADS-A) and seven questions measuring depression . Each question is scored 0–3, each subscale is scored 0–21, and the total score of both scales is 0–42. Higher scores indicatesseverer anxiety or depression.11 For each subscale, a score of ≥8 shows anxiety/depression.12 Patients reply to questions based on their past month. In our study, HADS-A was chosen to measure the anxiety of patients. At present, the HADS is extensively applied to measure patient anxiety and depression. The reliability and validity of the scale is good.
Self-Efficacy
We used the General Self-Efficacy Scale was applied to test the self-efficacy of the patients. The Chinese version has good reliability and validity. On ten questions, each response scores 1–4, so for a total of 10–40. The final score is the total divided by 10. The higher the score, the higher the self-efficacy.13
Sleep Quality
Sleep monitoring was performed with polysomnography overnight (≥7 hrs). Based on international methodological standards, we chose surface disk electrodes to record electroencephalography signals of six positions synchronously (F3-A2, F4-A1, C3-A2, 01-A2, 02-A1). We used two surface electrodes to record the electromyography of patients’ chins. In order to test eye movements of both eyes, we put an electrode at 1 cm above and below the lateral canthus. Sleep efficiency,meaning ratio of total sleep time to hours in bed, was chose to assess sleep quality.
IL6
ELISA was chosen to measure IL6 levels in serum. We used SM802 enzyme labeling for measurement. Wuhan physician De Bioengineering produced the kits, and Shanghai Yongchuang Medical Devices produced the microplate reader. The measurement unit used was pg/mL.
Patient Perceptions of Physician–Patient Relational Empathy Scores
We chose the Consultation and Relational Empathy (CARE) measure to test patients’ perceptions of physician–patient relational empathyafter they had received treatment. There are ten questions in the scale, and each is scored 1–5, giving an aggregate score of 10–50. Higher scores mean patients perceive more empathy from the physician.14
Statistical Analyses
We used EpiData 3.1 to enter the data and SAS 9.4 for analysis thereof. We show data as means ± SD. Paired t-tests andχ2 were applied when comparing indicators at the two time points. Multiple linear regression was applied to measure the influence of population, social factors, and disease related indices on IL6. We use Pearson's correlation analysis and a structural equation model to study relationship between patient perceptions of physician empathy and anxiety, self-efficacy, sleep quality, and IL6. Tests were two-tailed, and α=0.05.
Results
Sample
A total of 220 patients received the invitation, 187 participated in the study, and the data were valid. The participation rate was 85%. Patients' average age was 32.03±6.17 years. Average hospitalization was 8.14±0.62 days. Demographics, disease, and treatment are shown in Table 1.
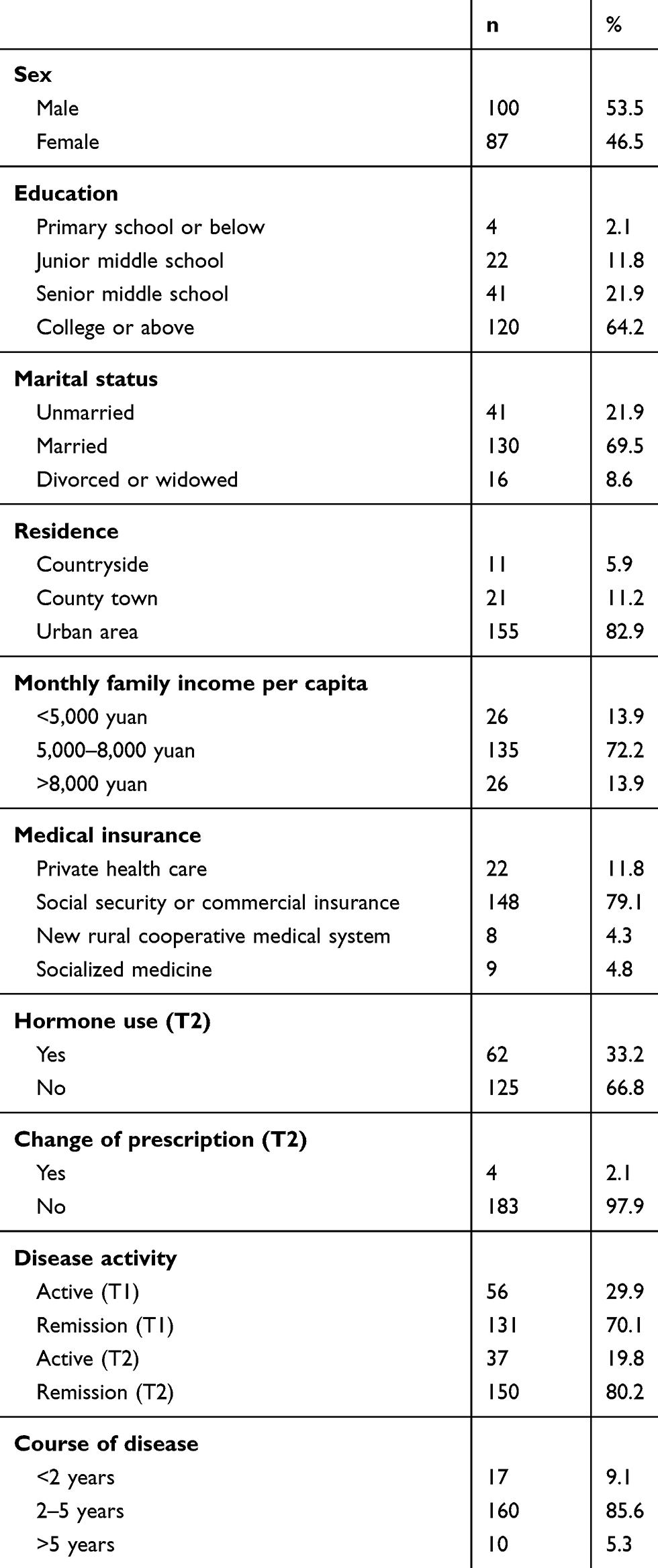 |
Table 1 Patient Demography and Disease |
Comparison of Patient Indices at Admission (T1) and 3 Months after Admission (T2)
Table 2 presents comparisons of patient indices at admission and 3 months after admission. At the two points of time, there were significant differences (P<0.01) inanxiety, self-efficacy, sleep, and IL6.
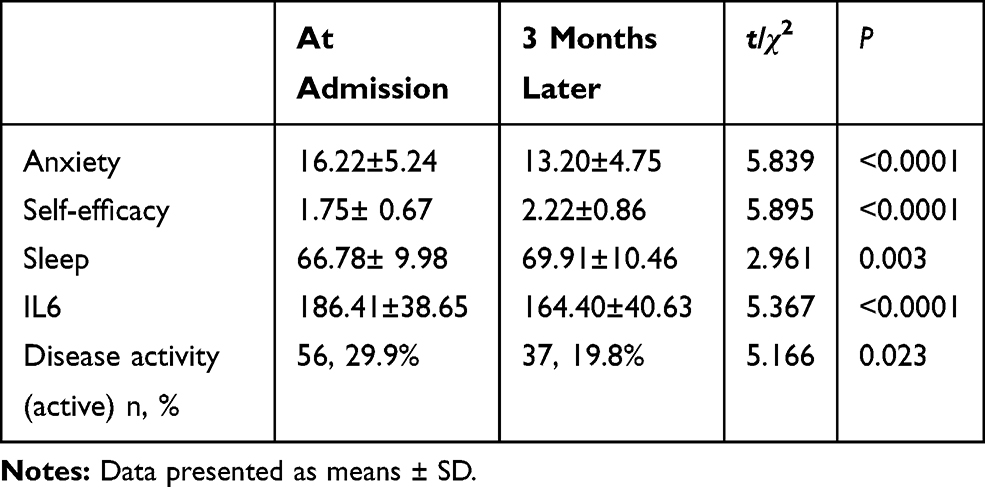 |
Table 2 Comparison of Patient Indices at Admission (T1) and 3 Months Later (T2) |
Influence of Population, Social Factors, and Disease-Related Indices on Patient IL6 at T2
The results of influence of population and social factors and disease related indexes on IL6 of patients at T2 are shown in Table 3. Results shows disease activity and course of disease were the influence factors of IL6.
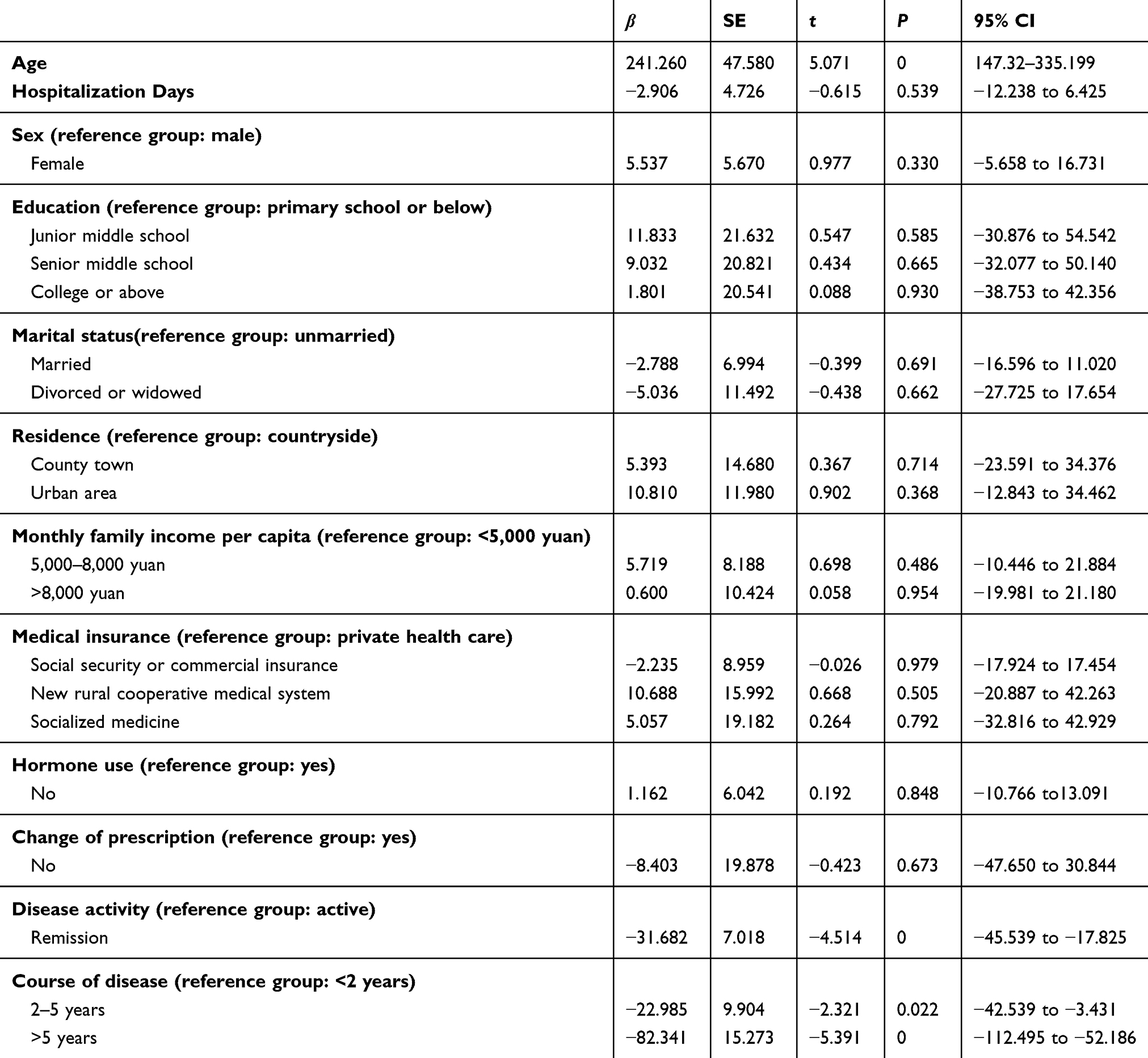 |
Table 3 Effects of Demographics and disease-Related Indices on Patient IL6 at T2 |
Correlations Between Patient Perceptions of Physician–Patient Relational Empathy and Anxiety, Self-Efficacy, Sleep Quality, and IL6 at T2
We applied Pearson’s correlation analysis to explore correlations between physician–patientrelational empathy and anxiety, self-efficacy, sleep, and IL6. The results revealed that patient perceptions of physician–patient relational empathy were negatively correlated with anxiety (r=−0.449, P<0.01) and IL6 (r=−0.378, P<0.01) and positivelycorrelated with self-efficacy (r=0.441, P<0.01) and sleep (r=0.416, P<0.01) . In addition, anxiety, self-efficacy, sleep, and IL6 showed significant correlations (Table 4).
 |
Table 4 Correlations Among Patient Perceptions of Doctor–Patient Relational Empathy and Patient Self-Efficacy, Anxiety, Sleep Quality, and IL6 |
Multiple Mediating Effects among Patients’ Perceptions of Physician–Patient Relational Empathy, Anxiety, Self-Efficacy, Sleep, and IL6 of Patients at T2
To explore the relationships among these variables further, we used path analysis to set up multiple intermediary models. Then, in order to confirm the hypothesis models described before, we used AMOS software. The fit of the structural equation was good: GFI 0.997, CFI 0.998, TLI 0.985, IFI 0.999, NFI 0.996, AGFI 0.950, RMSEA 0.054, and χ2/df 1.550). Figure 1 presents the model.
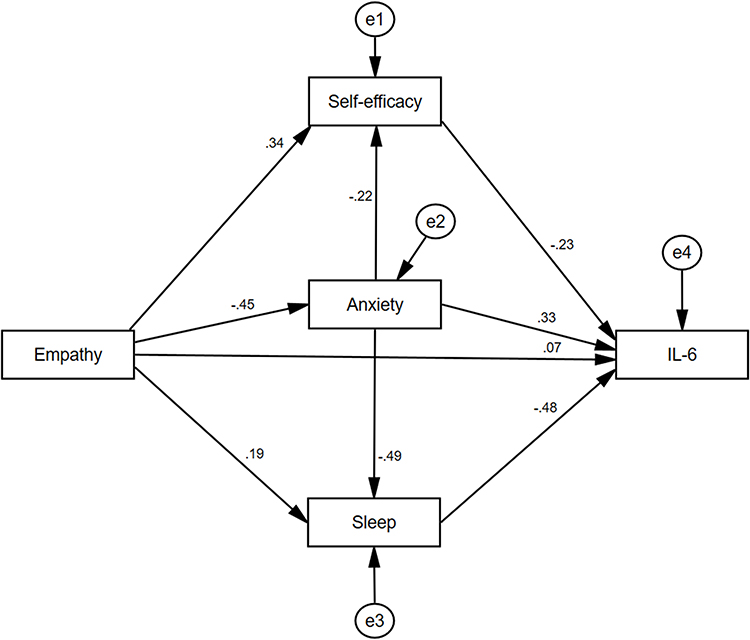 |
Figure 1 The model of relationships among patients’ perceptions of doctor-patent relational empathy and patents’ self-efficacy, anxiety, sleep quality, and IL6, with standardized β-weights. Note: e1–e4, residual error. |
Table 5 shows normalized path coefficients. Patient perceptions of physician–patient relational empathy significantly affected anxiety negatively (β=−0.449, P<0.05) and self-efficacy positively (β=0.340, P<0.05). Anxiety significantly affected self-efficacy negatively (β=−0.225, P<0.05) and sleep negatively (β=−0.493, P<0.05). Patient perceptions of physician–patient relational empathy significantly affected sleep positively (β=0.194, P<0.05). Self-efficacy significantly affected IL6 negatively (β=−0.226, P<0.05). Anxiety significantly affected IL6 positively (β=0.326, P<0.05). Sleep significantly affected IL6 negatively (β=−0.484, P<0.05). There was no significant effect of patient perceptions of physician–patient relational empathy on IL6 (β=0.067, P>0.05). Therefore, hypothesis 1 was refuted.
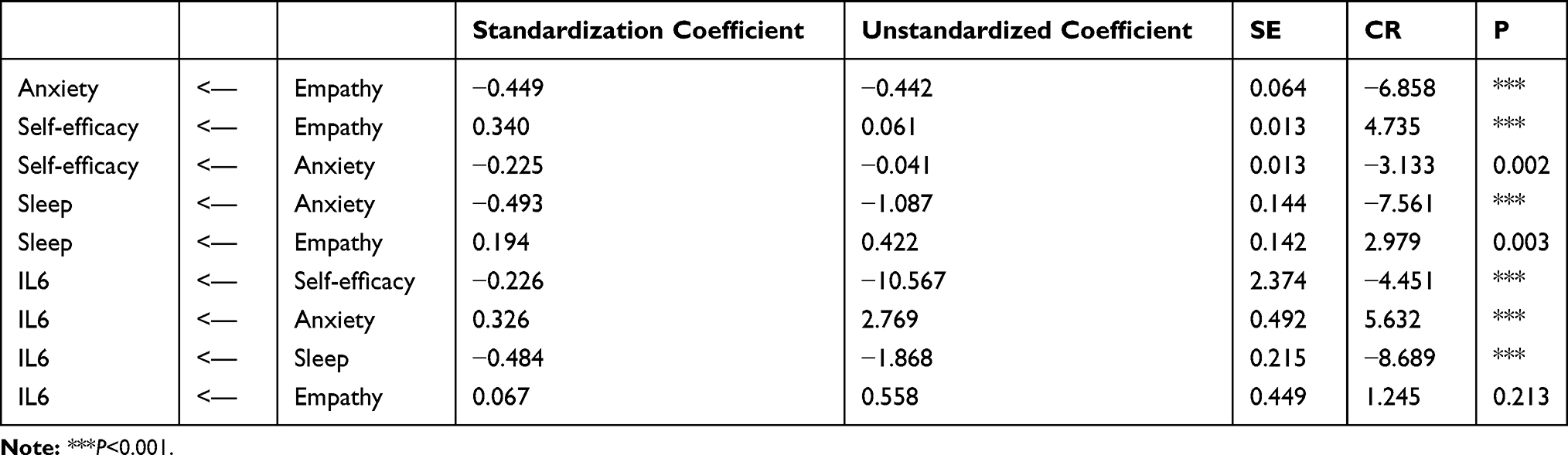 |
Table 5 Normalized Path Coefficients |
AMOS 21.0 was applied to measure the intermediary effect. We set IL6 as the dependent variable, patient perceptions of physician–patient relational empathy as argument, and anxiety, self-efficacy, and sleep as intervening variables. When the bootstrap was set at 5,000, in order to test the significance of specific intermediary effects, we applied the nonparametric percentile bootstrap method with deviation correction. Results indicated that the intermediary effect was significant when 0 was not included in the confidence interval. Five intermediary paths existed in the study. In the relationship between patient perceptions of physician–patient relational empathy and IL6, patients’ anxiety, self-efficacy, and sleep worked in intermediary roles:−0.146 (95% CI −1.873 to −0.653), −0.077 (95% CI–1.196 to –0.312), and −0.094 (95% CI −1.373 to −0.295). In the path of patient perceptions of physician–patient relational empathyanxiety → self-efficacy → IL6, when 0 was not contained in the CI, the effect was −0.023 (95% CI −0.410 to −0.070). This indicated that in the corrections between patient perceptions of physician–patient relational empathy and IL6, anxiety and self-efficacy had a significant chain intermediary effect (β=−0.023, P<0.05). In the path of patient perceptions of physician–patient relational → empathy → anxiety → sleep → IL6, when 0 was not contained in the CI, the effect was −0.107 (95% CI −1.362 to −0.570). This indicated that in corrections between patients’ perceptions of physician–patient relational empathy and IL6, anxiety and sleep played a significant chain-intermediary effect (β=−0.107, P<0.05). The results are shown in Table 6.
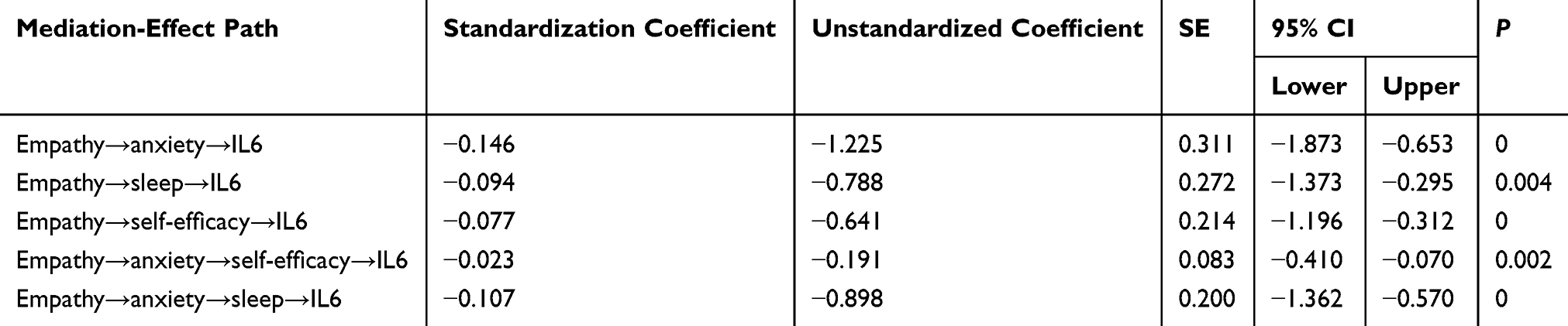 |
Table 6 Bootstrap Indirect-Effect Analysis |
Discussion
When indices at admission and 3 months later were compared, we found that changes in patients’ anxiety, sleep, self-efficacy, disease activity, and IL6 were statistically significant. This indicated that through hospitalization, the physical and emotional condition of patients had improved. At T2, after analyzing the influence of population and social factors, disease-, and treatment-related indexes on the IL6 of patients, we found disease activity and course of disease were influential factors for IL6 levels. When patients’ disease was in the active stage, their IL6 was high, because it is a factor related to inflammation reactions, and patients with active disease often have more inflammatory reactions.15 Those whose course of disease was shorter showed higher IL6, maybe because they felt more anxiety because of the uncertainty in illness.16 Also, negative mood may have improved IL6 levels of patients.
Then, the two hypotheses on correlations among anxiety, self-efficacy, sleep quality, IL6, and patient perceptions of physician–patient relational empathy were tested by path analysis. On the one hand, the hypothesis that patient perceptions of physician–patient relational empathy affected patients’ IL6 directly was rejected. This indicated that patients’ IL6 cannot be influenced by empathy directly. On the other hand, the hypothesis that patient perceptions of physician–patient relational empathy affect their IL6 through the intermediary roles of anxiety, self-efficacy and sleep was accepted.
Our results confirmed that the positive significance of the empathy between physician and patient was beneficial for patient outcomes in CD samples. In former research, it has been proved that empathy between medical staff and patients was beneficila to patients’ health. For instance, Pedersen et al found that physician-reported empathy was associated with gut feeling positively in cancer diagnosis.17 Weiss et al confirmed that when negative mood was expressed by the patients, if physicians responded empathically, patients would feel less anxiety.18 In our past research, we have found that empathy between patients and medical professionals had a positive effect on cancer patients and ulcerative colitis patients.19––21 These results reveal that empathy training should be included in medical education.
Clinical empathy is a hot topic nowadays. The mechanism of how empathy between medical staff and patients affects patient outcomes and needs to be deeply explored. This research focused on the impact of patient perception of physician empathy on their outcomes, because patients’ feelings may affect themdirectly, and analyzed its mechanism. For hypothesis 2, which was proved, the mechanism can be explained as follows.
First, empathy that patients feel they have received may have a positive impact on their anxiety, self-efficacy, and sleep. For one thing, when sharing the stories of patients and empathizing with them, physicians and nurses play multiple roles, including thosee of treatment, witness, and companion.22 Patients can talk about their pain, which reduces negative affectivity. Additionally, after receiving empathy from doctors, patients might improve their compliance. This made them feel more respected and mobilized their initiative, leading to a strong belief in recovery. Consequently, patient experienced less anxiety, higher self-efficacy, and betther sleep quality. Empathy between patients and physicians helps physicians to have better understanding of the patients according to their narratives. Therefore, health education and support for patients from physicians is targeted to patients’ personal conditions. This may help patients achieve a better mental state.23
Second, patients’ anxiety, self-efficacy, and sleep quality affected their IL6.Mental health indices and sleep affected IL6, which is a proinflammation marker. Anxiety leads to a change of inflammation markers because when patients face stress, the adrenal gland is provoked by the hypothalamic–pituitary–adrenal axis so that it produces cortisol. Cortisol can stimulate immunocytes to secrete more proinflammatory cytokines.24 Conversely, as self-efficacy is a healthy feeling, it can help reduce proinflammation markers. Moreover, if patients have high self-efficacy, they may manage their disease and health well, which contributes to disease control, thus reducing proinflammation factors. When it comes to sleep quality, it has been proved that sleep can affect inflammation markers and IL6 concentration can be improved by lack of sleep.25
In addition, patients’ self-efficacy and sleep were affected by anxiety directly. If a patient feels anxiety, he may reduce positive behavior and feel less self-efficacy.26 Patients’ sleep quality can be affected by anxiety. The reason for this is negative moods make cortisol increase, melatonin synthesis decrease, and cortisol-secretion rhythm early.27,28 Patients with these problems may have sleep disorders, such as waking up early and trouble falling asleep. Some relationships were inverse. For instance, less anxious patients might feel that the staff empathize more with them.29 Similarly, less inflammation improves sleep quality.30 Therefore, it is important to pay attention to patients' physiological as well as psychological indicators such that it promotes a virtuous cycle.
Our findings reveal that physicians should improve their empathy abilities and establish empathy with their patients. When treating patients, medical staff should listen to patient stories carefully and respond to them. In this process, show faith, love, and give them hope. Therefore, we advise a humanistic concept of “narrative medicine” be applied in clinical practice. Narrative medicine means story-telling by patients, and emphasizes that physicians should absorb and respond to patients’ stories so that they may empathize with patients deeply and take care of them better.31 In addition, future research is expected also to evaluate the role of alexithymia, which is an emerging clinical factor affecting patients with CD.32
There were some limitations in this study. First, patients’ inflammation may be affected by numerous potential nuisance variables, including sport and personal physique. Although we strictly controlled the criteria for membership, it was hard for us to take allfactors into account. In addition, clinically relevant anxiety of patients was not measured, and this should be studied in future research.
Conclusion
Our research shows that empathy between physicians and patients may affect patients’ mental health and the inflammation marker IL6. Anxiety, self-efficacy, and sleep quality of patients may play intermediary roles in correlations between patient perceptions of physician–patient relational empathy and inflammation markers in patients with CD. Accordingly, physicians should improve empathy with their patients. Anxiety, self-efficacy, and sleep should be included in the treatment focus of patients with CD, which may help to reduce levels of proinflammation markers.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. All patients signed the consent form. The Wuhan University School of Medicine Ethics Committee ratified the research (20161101).
Acknowledgment
We thank all the patients and physicians who took part in the study.
Funding
This research was supported by the Fundamental Research Funds for the Central Universities (HEUCF20181312).
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Shanahan F. Crohn’s disease. Lancet. 2002;359(9300):62–69. doi:10.1016/S0140-6736(02)07284-7
2. Boye B, Lundin KE, Jantschek G, et al. INSPIRE study: does stress management improve the course of inflammatory bowel disease and disease-specific quality of life in distressed patients with ulcerative colitis or Crohn’s disease? A randomized controlled trial. Inflamm Bowel Dis. 2011;17:1863–1873. doi:10.1002/ibd.21575
3. Richmond S. Being in others: empathy from a psychoanalytical perspective. Eur J Philos. 2004;12(2):244–264. doi:10.1111/j.0966-8373.2004.00209.x
4. Han JL, Pappas TN. A review of empathy, its importance, and its teaching in surgical training. J Surg Educ. 2018;75:88–94. doi:10.1016/j.jsurg.2017.06.035
5. Larso EB, Yao X. Clinical empathy as emotional labor in the patient-physician relationship. JAMA. 2005;293:1100–1106. doi:10.1001/jama.293.9.1100
6. Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physicians’ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86:359–364. doi:10.1097/ACM.0b013e3182086fe1
7. Del Canale S, Louis DZ, Maio V, et al. The relationship between physician empathy and disease complications: an empirical study of primary care physicians and their diabetic patients in Parma, Italy. Acad Med. 2012;87:1243–1249. doi:10.1097/ACM.0b013e3182628fbf
8. Rincon M, Irvin CG. Role of IL-6 in asthma and other inflammatory pulmonary diseases. Int J Biol Sci. 2012;8(9):1281–1290. doi:10.7150/ijbs.4874
9. Glaus J, Vandeleur CL, von Känel R, et al. Associations between mood, anxiety or substance use disorders and inflammatory markers after adjustment for multiple covariates in a population-based study. J Psychiatr Res. 2014;58:36–45. doi:10.1016/j.jpsychires.2014.07.012
10. Daperno M, D’Haens G, Van Assche G, et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: the SES-CD. Gastrointest Endosc. 2004;60(4):505–512. doi:10.1016/S0016-5107(04)01878-4
11. Zigmond AS, Snaith RD. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
12. Bjelland I, Hahl AA, Hauq TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An undated literature review. J Psychosom Res. 2002;52:69–77. doi:10.1016/S0022-3999(01)00296-3
13. Zhang JX, Schwarzer R. Measuring optimistic self-beliefs: A Chinese adaptation of the general self-efficacy scale. Psychologia. 1995;38:174–181.
14. Mercer SW, Maxwell M, Heaney D, Watt GC. The consultation and relational empathy (CARE) measure: development and preliminary validation and reliability of an empathy-based consultation process measure. Fam Pract. 2004;21:699–705. doi:10.1093/fampra/cmh621
15. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
16. Parker PA, Davis JW, Latini DM, et al. Relationship between illness uncertainty, anxiety, fear of progression and quality of life in men with favourable-risk prostate cancer undergoing active surveillance. BJU Int. 2016;117(3):469–477. doi:10.1111/bju.13099
17. Pedersen AF, Andersen CM, Ingeman ML, et al. Patient–physician relationship and use of gut feeling in cancer diagnosis in primary care: a cross-sectional survey of patients and their general practitioners. BMJ Open. 2019;9:e027288. doi:10.1136/bmjopen-2018-027288
18. Weiss R, Vittinghoff E, Fang MC, et al. Associations of physician empathy with patient anxiety and ratings of communication in hospital admission encounters. J Hosp Med. 2017;12:805–810. doi:10.12788/jhm.2828
19. Yang NX, Xiao H, Cao YN, et al. Influence of oncology nurses’ empathy on lung cancer patients’ cellular immunity. Psychol Res Behav Manag. 2018;11:279–287. doi:10.2147/PRBM.S168649
20. Yang NX, Xiao H, Wang W, et al. Effects of physicians’ empathy abilities on the cellular immunity of patients with advanced prostate cancer treated by orchiectomy: the mediating role of patients’ stigma and self-efficacy. Patient Prefer Adher. 2018;12:1305–1314. doi:10.2147/PPA.S166460
21. Chen XF, Zhang Y, Xu XL, et al. The mediating effects of anxiety, self efficacy and sleep quality on the relationship between physician-patient’s empathy and inflammatory marker in patients with ulcerative colitis. Med Sci Monit. 2019;25:7889–7897. doi:10.12659/MSM.917552
22. De Moor K. The physician’s role of witness and companion: medical and literary ethics of care in AIDS physicians’ memoirs. Lit Med. 2003;22:208–229. doi:10.1353/lm.2003.0020
23. Jubraj B, Barnett NL, Grimes L, Varia S, Chater A, Auyeung V. Why we should understand the patient experience: clinical empathy and medicines optimisation. Int J Pharm Pract. 2016;24:367–370. doi:10.1111/ijpp.2016.24.issue-5
24. Vanuytsel T, van Wanrooy S, Vanheel H, et al. Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut. 2014;63:1293–1299. doi:10.1136/gutjnl-2013-305690
25. Abedelmalek S, Chtourou H, Aloui A, Aouichaoui C, Souissi N, Tabka Z. Effect of time of day and partial sleep deprivation on plasma concentrations of IL-6 during a short-term maximal performance. Eur J Appl Physiol. 2013;113:241–248. doi:10.1007/s00421-012-2432-7
26. Bandura A, Adams NE. Analysis of self-efficacy theory of behavior change. Cognitive Therapy Res. 1977;1:287–310. doi:10.1007/BF01663995
27. van Santen A, Vreeburg SA, Van der Does AJ, Spinhoven P, Zitman FG, Penninx BW. Psychological traits and the cortisol awakening response: results from the Netherlands Study of Depression and Anxiety. Psychoneuroendocrinology. 2011;36:240–248. doi:10.1016/j.psyneuen.2010.07.014
28. Cardinali DP, Srinivasan V, Brzezinski A, Brown GM. Melatonin and its analogs in insomnia and depression. J Pineal Res. 2012;52:365–375. doi:10.1111/j.1600-079X.2011.00962.x
29. Sambo CF, Howard M, Kopelman M, Williams S, Fotopoulou A. Knowing you care: effects of perceived empathy and attachment style on pain perception. Pain. 2010;151(3):687–693. doi:10.1016/j.pain.2010.08.035
30. Straub RH, Detert J, Dziurla R, et al. Inflammation is an important covariate for the crosstalk of sleep and the HPA axis in Rheumatoid Arthritis. Neuroimmunomodulation. 2017;24(1):11–20. doi:10.1159/000475714
31. Charon R. Narrative medicine: A model for empathy, reflection, profession, and trust. JAMA. 2001;286:1897–1902. doi:10.1001/jama.286.15.1897
32. Carrozzino D, Porcelli P. Alexithymia in gastroenterology and hepatology: a systematic review. Front Psycho. 2018;9:470. doi:10.3389/fpsyg.2018.00470
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.