")
Back to Journals » International Journal of General Medicine » Volume 15
Effects of Nutritional Status on Neurodevelopment of Children Aged Under Five Years in East Gojjam, Northwest Ethiopia, 2021: A Community-Based Study
Authors Wondemagegn AT , Mulu A
Received 22 April 2022
Accepted for publication 27 May 2022
Published 8 June 2022 Volume 2022:15 Pages 5533—5545
DOI https://doi.org/10.2147/IJGM.S369408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amsalu Taye Wondemagegn,1 Abay Mulu2
1Department of Biomedical Sciences, School of Medicine, Debre Markos University, Debre Markos, Ethiopia; 2Department of Anatomy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Amsalu Taye Wondemagegn, Department of Biomedical Sciences, School of Medicine, Debre Markos University, P.O. Box: 269, Debre Markos, Amhara Regional State, Ethiopia, Tel +251 921815441, Email [email protected]
Introduction: Scientific evidence regarding relationships between developmental status and nutritional status of children aged under five years old is scarce, particularly in Africa. Thus, the objective of the present study is to evaluate the relationships between nutritional status and developmental status among children aged under five in Gojjam, Ethiopia.
Methods: A cross-sectional study was conducted on 390 child–mother pairs from December 1– 30 2021. Developmental status, nutritional status and related data were collected using age and stage questionnaire 3rd edition (ASQ-3) and measurements of body dimensions and other physical characteristics. Body dimensions data was obtained by measurement of height and weight of children aged under five years. Logistic regression analysis was executed to identify factors related with poor child developmental status. Adjusted odds ratio (AOR) and 95% CI was estimated to reveal the strength of association and statistical significance were declared at p-value less than 5%.
Results: The overall prevalence of developmental delay in the current study among under five years children was 22.6%. Moreover, in this study the prevalence of stunting, wasting and being underweight was 36.3%, 14.2% and 20.3%, respectively. Developmental delay among under-five children was significantly associated with experiencing repeated diseases during pregnancy (AOR: 2.43; 95% CI:1.38, 4.28), short birth interval (AOR: 2.78; 95% CI :1.52, 5.09), stunting (AOR: 2.61;95% CI: 1.41, 4.84), wasting (AOR: 3.68;95% CI: 1.61, 8.37) and being underweight (COR: 3.28;95% CI: 1.91, 5.63).
Conclusion: The overall developmental delay prevalence among under-five children in the present study was 22.6%. The prevalence of stunting, wasting and being underweight was 36.3%, 14.2% and 20.3%, respectively. Maternal diseases, birth interval and nutritional status of children aged under five years were among the factors which revealed statistically significant associations with developmental delay of under-five children. We recommend the concerned body to work on improving maternal health status during pregnancy, to enable mothers to adequately space subsequent births, and to work on improving the nutritional status of women and children in the current study area in order to improve the developmental status of children aged under five.
Keywords: child neurodevelopment, child developmental status, nutritional status, under-five children, Ethiopia
Introduction
Early postnatal years, especially the period of infancy, is the most crucial period in the human development process, in which the architecture of the brain is determined mainly due to the continuous interaction of genetically inherited factors and the environment in which the child lives.1 For healthy development of children, it is better to know their peculiar features and environmental factors favorable to their development.2 It is known that the child’s development is highly affected by the environment in which it grows.
Child development is a dynamic and exceptional process for every child, and is characterized by the continuousness and alterations in motor, cognitive, psychosocial and language skills, with the attainments of progressively multifaceted functions in their daily life and practice in their social role.3
Early years of life development is fundamental in that it is in this stage of human development that the nervous system structures grow, mature and become more sensitive to increased environmental exposure. Environmental factors such as nutrition, care and breastfeeding affect directly the previously determined genetic factors in the brain mainly during the premature years of life.4 For example, when the newborn child receives appropriate care, it will have better performance in school and out of school activities. On the other hand, it has been reported that poor nutrition among children resulted in poor developmental status as characterized by their retarded status in the awareness of their environment and being retarded in performing activities at the required speed.5 It is also reported that poor nutrition leads to retarded development due to its effect on neuron integration activities.5
It is known that in low-income countries like Ethiopia, diseases and poor nutrition are common especially in children under five years of age, where the brain development take place at increased speed.
It is reported6 that diseases and harmful practices like poor nutrition practices, harassment, violence and ignorance badly harm the development of neuron pathways and thus interfere with normal brain development.
It has been approximated7 that almost 219 million children aged under five years in low-income countries are living with double burden of malnutrition and poverty, which will seriously affect their development potential.
In Ethiopia malnutrition is the major public health concern, even though the country has made tremendous effort in averting the problem. According to EDHS 2016,8 38%, 24% and 10% of Ethiopian children aged under five years, respectively, were stunted, underweight and wasted. In spite of large magnitude of the problem among under-five children of the country, its association with child development is poorly understood.
Scientific evidence regarding magnitude of developmental problems as well as relationships between developmental status and nutritional status of children aged under five years, particularly in the African countries, is scarce. A study conducted in Nigeria9 and another study in southern parts of Ethiopia10 reported significant correlation between selected domains of child development and nutritional status.
According to the researchers’ knowledge there has been no previous attempt to study the extent of developmental problems among under-five children in the study area and no previous study tried to reveal the association between nutritional status and developmental status among such children.
Having such scientific evidence, this study may serve as baseline data on which further study will be carried out. In addition, such scientific evidence may serve as an input for policy makers and health care program planners so as to design strategies on how to support such disadvantaged population groups. At last, such screening types of study will give a rapid picture of children’s developmental state and general health in the community and will show whether further assessment is required to diagnose potential problems that may require intervention or distinct education services.11 Hence, the main objective of this study is to quantify the prevalence of neurodevelopmental problems and mainly to reveal the association between neurodevelopmental problems and nutritional status among children aged under five years in East Gojjam, Northwest Ethiopia.
Methods and Materials
Study Design, Setting and Population
A cross-sectional study with a community-based approach was conducted in East Gojjam, Amhara region from December 1–30 2021. East Gojjam administrative zone has 18 woredas; Debre Markos town is the capital of the zone, which is 299 kilometers from the capital, Addis Ababa, and 256 kilometers from the regional state capital, Bahir Dar. All children aged under five years and their respective primary caregivers living in the selected kebeles during the study period were our study population. Children and their primary caregivers who had been seriously sick (like having mental illnesses, having diagnosed chronic illnesses such as diabetes mellitus or hypertension) and/or hospitalized for diseases were excluded from the study. Moreover, children and their primary caregivers having body deformity like deformity of extremities or deformity of both anterior and posterior chest that make measurements difficult were not included in this study.
Sample Size Determination and Sampling Procedures
Single population proportion determination formula was used to calculate sample size. By considering a 19% prevalence of developmental problems among children aged under five years from a previous local study10 and by considering a 95% confidence interval and a margin of error of 5%, design effect of 1.5 and adding 10% for non-response rate, the final sample size is 390. Multi-stage sampling was used to select representative samples by using simple and systematic random sampling methods. First, from the zone 25% of the woredas were selected by lottery, namely: Debre Markos town, Dejen District, Bichena District, Enarji Enawga District and Machakel. Then, the representative administrative kebeles (AKs) in each selected woreda were selected by lottery. In the selected AKs of the districts’ households having children aged under five years were selected by systematic random sampling.
Data Collection Tools and Procedures
The required data were collected using body dimension measurements and a pretested structured questionnaire. The questionnaire was initially prepared in English and then translated into the local language, Amharic, and again it was translated back into English to check its consistency.
Body Dimension Measurement Procedures
Body dimension data were gained by measuring weight and height of children. Weight of under-five children was measured using recommended UNICEF weighing scale without any footwear and with minimal clothing to the nearest 0.1 kg. Standing height for those who are 24 months and older was measured without any footwear to the nearest 0.1 cm using a standard calibrated bar. While measurement of standing height is performed, the bar was placed on flat surface fixed to wall for stability and the participating children were standing without assistance and measured from the bottom of the foot to the highest point of the head. The height was compared with the new WHO child growth standards, 2006 reference data12 for that specific age and sex to get height for age. Children below 24 months of age (below 85 cm) were measured in a recumbent position (crown to heel length) by using a length board with a headpiece to the nearest 0.1 cm. Measurement of recumbent length was performed on study participants being in supine position with their head resting against the headboard. Next, we held and extended their knees and brought the footboard to the heel of the studied children. The nutritional status indices height-for-age (HFA), weight-for-height (WFH), and weight-for-age (WFA) were stated as z-scores using World Health Organization Child Growth Standards.12 Z-scores below minus two standard deviations (–2 SD) from the median of the reference population in terms of HFA, WFA and WFH were considered as stunted (chronically malnourished), underweight (both chronically and acutely malnourished) and wasted (acutely malnourished), respectively. Those whose z-score was between –2SD and –3 SD from the median reference in terms of HFA, WFA and WFH were considered moderately stunted, moderately underweight and moderately wasted, respectively. Those with z-scores below minus three standard deviations (–3 SD) from the median of the reference population in terms of HFA, WFA and WFH were considered severely stunted, severely underweight, and severely wasted, respectively. The right age of a child was prompted from the child’s vaccination card and mother’s recall. Recall of mothers was helped by referring to local events, happening around the time they gave birth to their children.
Measurement of Child’s Developmental Status
The domains of child development were assessed with the use of age and stage questionnaire third edition (ASQ-3) as a screening tool.13 Age and stage questionnaire is a consistent parent completed tool so as to screen for developmental delays among children under five years using 21 age-appropriate developmental questionnaires starting at 2 months and ending at 60 months of age.13 The ASQ-3 is fast and easy to use, which takes about 10–15 minutes for caregivers to complete and 2–3 minutes for experts to score. The ASQ-3 effectively screens five key developmental areas: communication, gross motor, fine motor, problem solving, and personal-social; each domain contains six questions that can be answered with a yes (10 points), sometimes (5 points) or not yet (0 points). Scores obtained from each domain are compared with cut-off scores at one and two standard deviations that are used to identify children at risk of developmental delay. Cutoff scores considered are obtained through empirical research.13 Based on the relative score in each of the domains the child was classified into three developmental states or areas. Scores falling in the white developmental area indicate the child is developing typically. Scores falling in the gray area mean the child should be monitored and another screening may be desirable in a few months (1−2 SD below the mean). Scores falling in the black area mean the child may be at risk for developmental delays and should be referred for further assessment (2 SD below mean). It has been reported14 that ASQ has a strong testing potential for detecting developmental delay among under-five children in low resource settings like Ethiopia.
Data Quality Assurance
Quality of data was maintained by (1) using educated data collectors and supervisors who had previous experience of data collection and supervision; (2) providing three days of intensive training to data collectors and supervisors focusing on the aim of the study, administration of the structured questionnaire, survey instruments, body dimensions measurements and ethical considerations; (3) conducting pre-test of questionnaires before the actual data collection work, considering 5% of the sample size of those individuals who were not included in the actual study to check the accuracy of responses and estimate time needed (some modifications were made on the basis of these results); and (4) regularly calibrating weighing scales with known weight object.
Data Processing and Analysis
Data were coded and entered in to Epi Data version 3.1 statistical package software and then exported to Statistical Package for Social Sciences (SPSS) software version 20.0 for analysis. Characteristics of the sample, like developmental status of children, nutritional status of children, demographic and socioeconomic factors, child factors and maternal factors, were presented in terms of frequencies and percentages through the use of text and tables. Bivariable and multivariable logistic regression analysis was executed to identify factors related with poor child developmental status. All the variables with p-value ≤0.2 at the bivariable logistic regression analysis were entered into the multivariable logistic regression model. Adjusted odds ratio (AOR) with 95% CI was estimated to reveal the strength of association and statistical significance was declared at p-value <5%. Collected weight and height data with their corresponding age and sex data were entered and analyzed using WHO Anthro version 2 software.15
Ethical Considerations
Ethical approval was obtained from Ethical Review Committee of Debre Markos University, School of Medicine. Permission was also obtained from the concerned bodies of East Gojjam and the responsible administrative bodies of the selected woredas and administrative kebeles. Study participants were informed regarding the aims of the study. Study participants provided informed verbal consent. We have also received informed verbal consent for children participating in the study from their primary caregivers. The main reason for not providing written consent was that, after they read through the document that explains the research or having them listen to an explanation of the research, the participants told us that they were happy to participate in our study but that they were uncomfortable with signing the form. The main reason may be due to low level of education of the study participants. In fact, the oral consent adheres to our Ethical Review Committee which approved the proposal for oral consent at these study sites. In conclusion, our study complies with the Declaration of Helsinki.
Results
Sociodemographic Characteristics of the Study Participants
Out of 390 planned study participants, 380 participated in the study, making a response rate of 97.4%. The median age of the children studied was 24 months, with an interquartile range of 23, and the mean age of the mothers/primary caregivers participating in this study was 27.57 years, with a standard deviation of 5.5 years. Majority of the primary caregivers in this study were urban residents, illiterate, married, had 5 or fewer children, had a husband-headed household, and were orthodox religion followers (Table 1). Majority of children in this study were male, aged 24 months or less, born less than 2 years apart, experienced health problems within 2 weeks preceding the survey, not practiced feeding pre-lacteals, practiced immediate breastfeeding following birth, and initiated complementary feeding in between 4 and 6 months (Table 2).
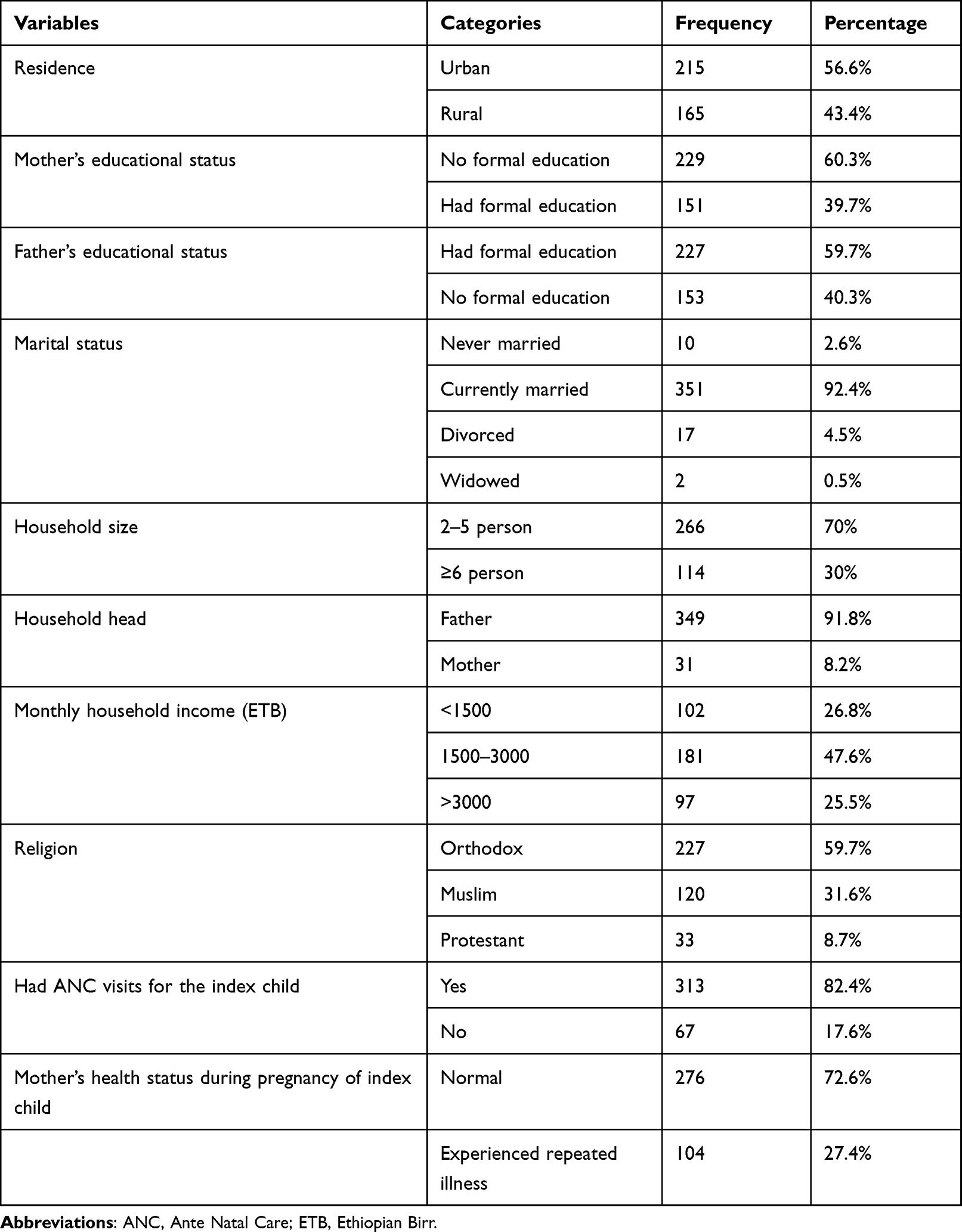 |
Table 1 Background Characteristics of Mothers/Primary Caregivers of Children Under Five Years in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
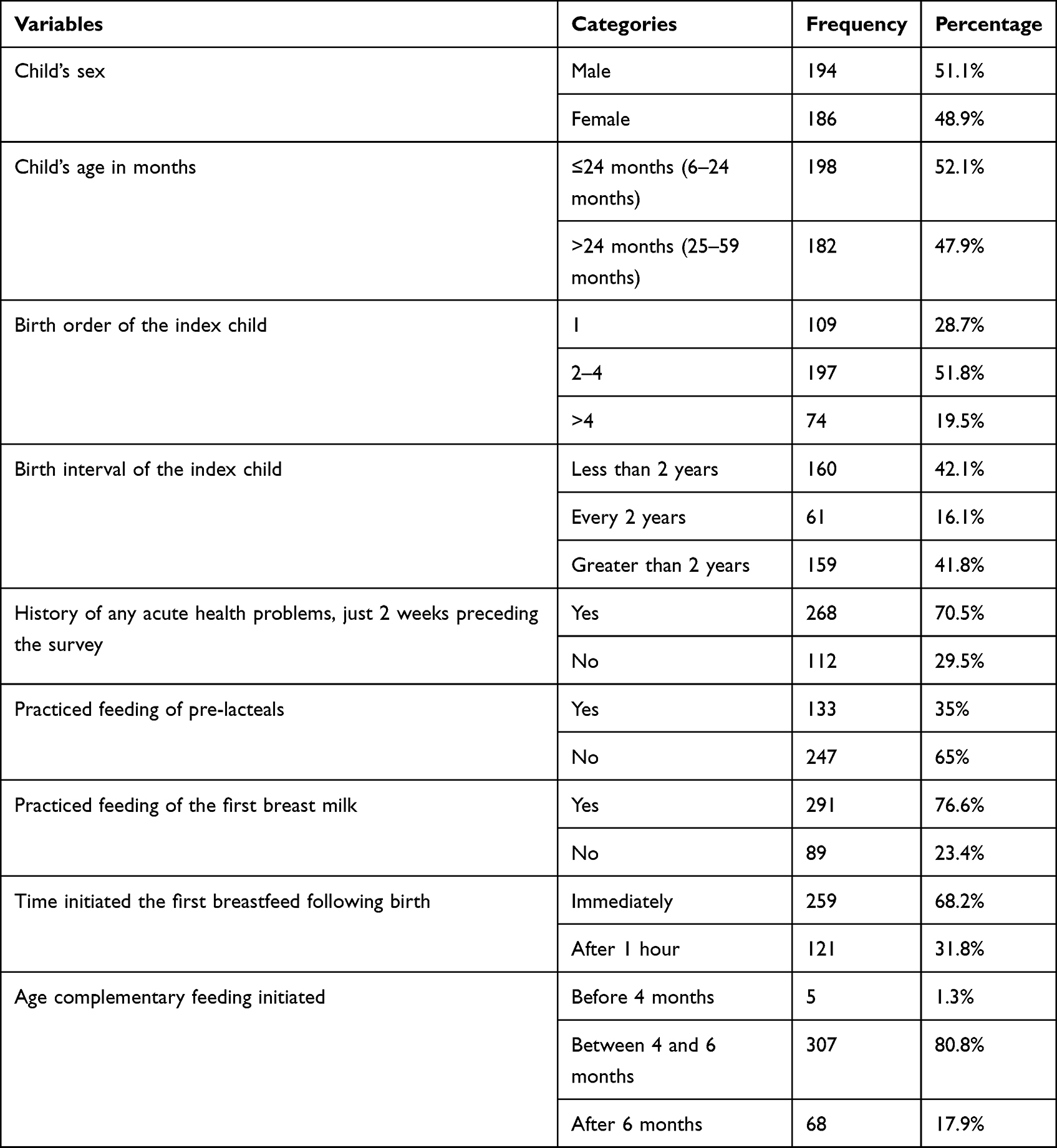 |
Table 2 Sociodemographic Characteristics and Selected Child Feeding Practices of Under-FiveChildren in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
Nutritional Status of Under-Five Children in the Current Study Area
The present study found that the prevalence of stunting, wasting and being underweight was 36.3%, 14.2% and 20.3%, respectively (Table 3). The study also found that the prevalence of severe stunting, severe wasting and being severely underweight was 11.8%, 3.4% and 5%, respectively. More importantly, the proportions of stunting, wasting and being underweight among developmentally delayed children aged under five years were 52.3%, 24.4% and 37.2%, respectively (Table 4).
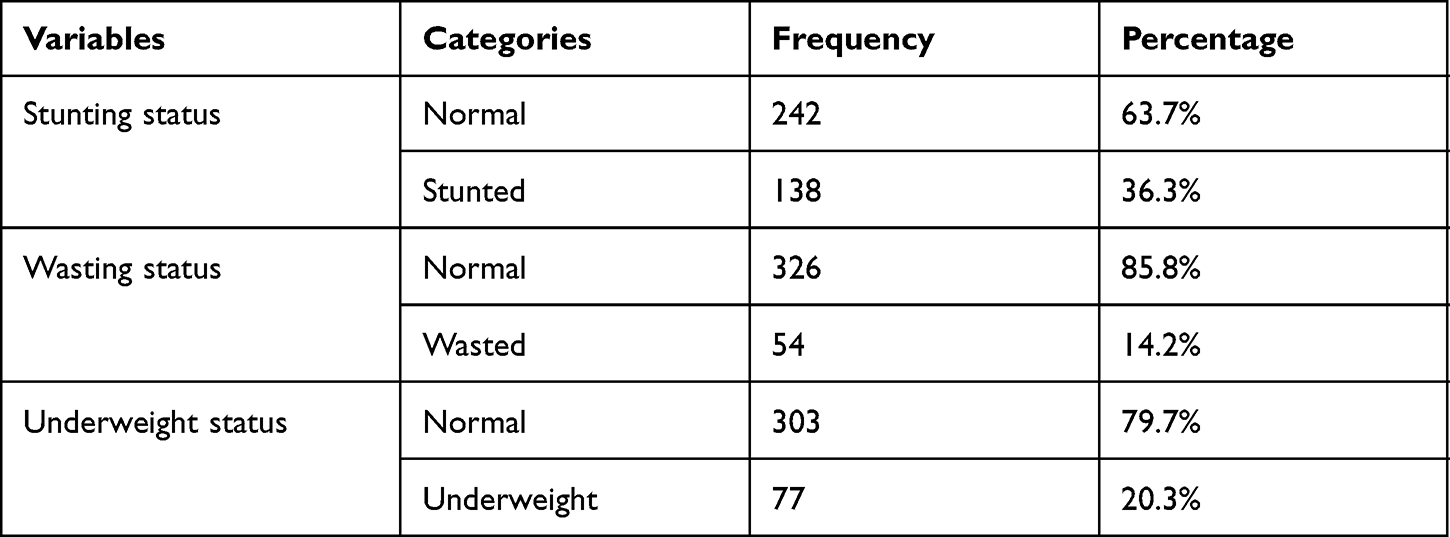 |
Table 3 Nutritional Status Indices of Under-Five Children in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
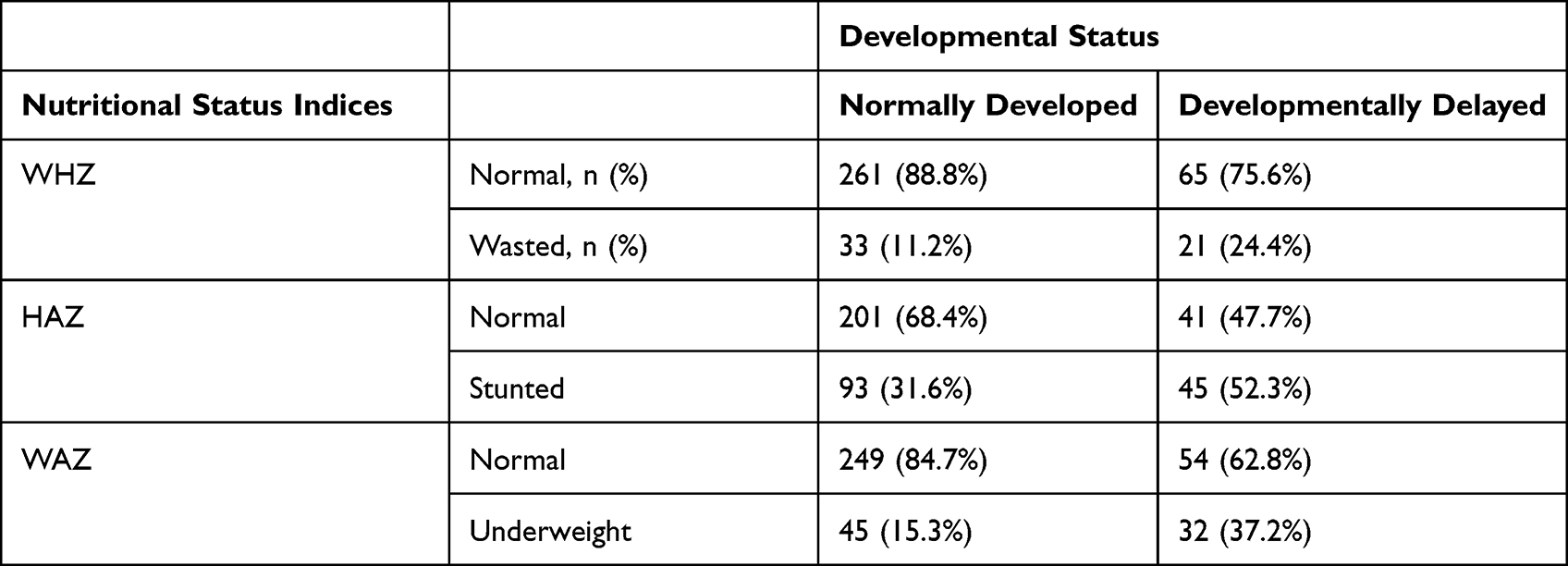 |
Table 4 Proportion of Nutritional Status Indices on Developmentally Delayed Under-Five Children in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
Child Developmental Status in the Current Study Area
The overall prevalence of developmental delay in the current study area among under-five year children was 22.6%. Based on specific development domains, 4.7% of the children under five years had a communication problem; 3.9% gross motor problem; 4.2% fine motor problem; 6.6% problem-solving skill difficulty; and 7.9% had problem of personal social interaction skill (Table 5).
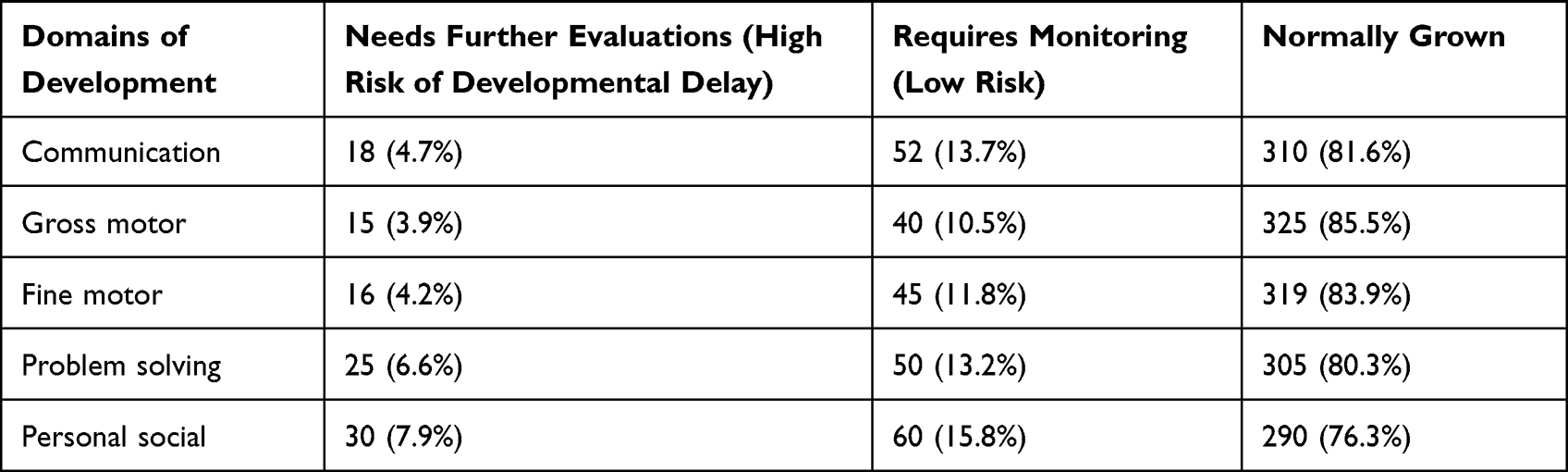 |
Table 5 Developmental Status by Domains of Neurodevelopment Among Children Aged Under Five Years Old in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
Association Between Developmental Status of Under-Five Children and Nutritional Status and Other Selected Variables
The binary logistic analysis result revealed that, among the variables, maternal health status during pregnancy of the index child, birth interval and nutritional status of under-five children were significantly associated with their developmental status. Those studied children whose mothers have experienced repeated diseases during their pregnancy had 2.4 times increased risk (AOR: 2.43; 95% CI:1.38, 4.28) for developmental delay compared to those children whose mothers were normal during their pregnancy. Children in this study who had been born less than 2 years apart were 2.8 times more at risk (AOR: 2.78; 95% CI: 1.52, 5.09) for developmental delay compared to those born at greater than 2 years interval. The risk of developmental delay among stunted children was 2.6 times higher (AOR: 2.61;95% CI: 1.41, 4.84) compared to non-stunted children. Wasted children were 3.7 times more at risk for developmental delay (AOR: 3.68; 95% CI: 1.61, 8.37) compared to non-wasted children. Those children in this study who were underweight were about 3 times more at risk (COR: 3.28;95% CI: 1.91, 5.63) for developmental delay compared to non-underweight children (Table 6).
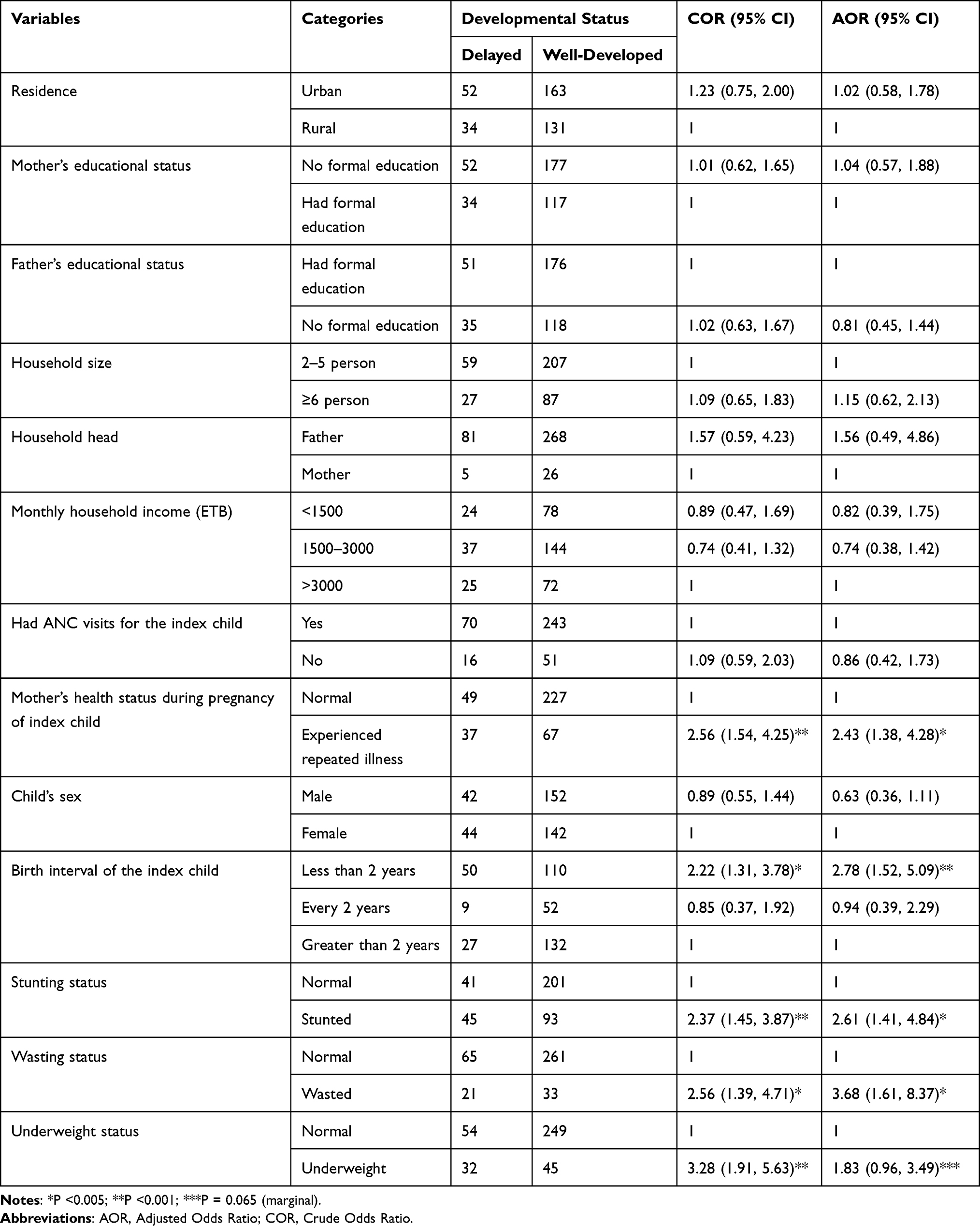 |
Table 6 Binary Logistic Regression Analysis Result Showing the Association Between Developmental Status of Under-Five Children and Their Nutritional Status Indices and Other Selected Variables in East Gojjam Zone, Northwest Ethiopia, 2021 (N=380) |
In addition to regression analysis, we performed correlational analysis to reveal also the relationships between developmental status and nutritional status indices among under-five children. The analysis results revealed a positive association between developmental status of under-five children and wasting status (Pearson coefficient, 0.16 with p <0.005), stunting status (Pearson coefficient, 0.18 with p <0.001), and underweight status (Pearson coefficient, 0.23 with p <0.001).
Discussion
The overall prevalence of developmental delay among under-five children in this study was found to be 22.6%. This study finding is lower than a study conducted in Nigeria,9 which was found to be 35.4%, and Malaysia,16 which was 31.7%. On the other hand, the present study finding is relatively higher than a previous local study10 conducted in the southern parts of Ethiopia, which reported a 19% overall prevalence. Similarly, the finding of present study is higher than previous studies by Agarwal et al, 201817 (12.2%), Shatla and Goweda, 202018 (16.4%), Sharma et al, 201919 (16.2%) and Gunardi et al, 201920 (10%). The variability of findings may be attributed to differences in sample size, socioeconomic status, nutritional status, health conditions and the methods implemented. For example, an extremely high magnitude (61.1%) of developmental delay was found among children with severe acute malnutrition in a study conducted elsewhere21 and 50% of developmental delay was observed among children under five with chronic under-nutrition.20 Moreover, higher prevalence of developmental delay was reported in underweight, wasted and stunted under-five children elsewhere.17
The most pronounced developmental defects in the present study were in relation to communication problems, problem-solving difficulties and personal social skill problems, which account for 4.7%, 6.6% and 7.9%, respectively. Relatively higher communication skill problems (5.6%), lower personal social skill problems (4.6%) and almost approaching problem-solving difficulties (5.5%) findings were reported by a previous study elsewhere.18 In fact, a higher magnitude of communication skill problems (24.5%) was reported by a previous study conducted in the eastern provinces of Saudi Arabia.22 On the other hand, relatively higher fine motor difficulties and much lower personal social and communication domain delay were reported by a study in Iran.23 An institution-based study conducted in Iraq24 found the magnitude of developmental delay in communication, fine motor, gross motor, problem solving and personal social domains of development among under-five children were 20.2%, 19.3%, 17.5%, 8.8% and 16.7%, respectively. This higher difference may be attributed to variability in the study setting and the tools used.
In the present study the prevalence of stunting, wasting and being underweight were 36%, 14% and 20%, respectively. Our findings in relation to stunting are comparable with those of the 2016 EDHS national report (38% prevalence)8 but lower than the 2016 EDHS regional report (46% prevalence). The present study found a relatively higher prevalence of wasting compared to the 2016 EDHS national and regional reports, which was 10%, and relatively lower underweight prevalence compared to 2016 EDHS national and regional reports. The variability may be because of variations in sample size, sampling area and study period.
In the current study, having experienced repeated diseases while pregnant was significantly associated with delayed development among under-five children. We found the risk of developmental delay among those children born from mothers who experienced diseases was 2 times higher compared to those born to normal mothers. Similarly, studies have reported that if the mother is depressed while pregnant, the child has three times increased risk of developing attention deficit25 and about 2 times increased risk of developing behavioral and emotional problems.26 In addition, other studies conducted elsewhere27,28 are in agreement with our finding, which reported significant association between maternal diseases and developmental delay in their children. Several possible justifications may be there for these findings but, as revealed by various studies, different diseases experienced during pregnancy such as depression, epilepsy, anxiety, anemia, bronchial asthma and metabolic disorders, like hypertension and diabetes, are responsible for changes in growth and fetal development, which in turn will have an impact on childhood and adulthood development. For example, mothers who faced psychiatric disorders of various types during pregnancy may have an impact on development and morphology of growing fetal brain. As reported from a study29 children born from mothers suffering from anxiety and depression have less developed areas of brain peculiar for controlling cognitive functions, especially the prefrontal cortex, which regulates reasoning, working memory, attention and the aspects of communication.
The present study found short birth interval significantly increased the risk of developmental delay among under-five children, which is in agreement with a previous study.30 Among the many explanations, one is that, as revealed by previous studies, longer intervals between children result in better health and nutritional status for children and their mothers.31,32 On the other hand, several studies have reported that short birth intervals increase the risk of under-nutrition,31,33–35 especially stunting and being underweight among under-five children, which in turn has an impact on their developmental state. Moreover, inadequate birth intervals may lead to mothers being affected by various maternal diseases like hemorrhage, anemia, nutritional deficiencies, and other maternal morbidities.36,37 But appropriate birth intervals enable mothers to fully recover from loss of previous pregnancies and lactation and enable them to have psychological as well as physical readiness for the next pregnancy.38
The current study found that under-nutritional status, that is, stunting, wasting and being underweight, among under-five children was significantly associated with their developmental delay. In the same way, several previous studies9,10,39–41 found a significant correlation between poor nutritional status and various domains of developmental problems of under-five children.
It has been reported that under-nutrition in the early years of life significantly affects brain development, cognitive development and behavioral development.42 This may be due to the fact that poor nutrition indices may be associated with deficiency of important nutrients necessary for brain development like folic acid, iron, iodine and others. For example, it has been shown that iodine deficiency has been associated with damage in brain development,43 which takes place mainly in the early years of life. Another study conducted elsewhere39 showed a statistically significant developmental delay among those children who received less iron compared to those who received appropriate iron.
In the current study there was no significant association between child’s sex and developmental delay, which is in line with previous studies.44–47 On the contrary, other previous studies18,22,27 found significant association between child’s sex and developmental delay among under-five children. In the current study, maternal educational status has no significant association with childhood developmental delay, in agreement with a previous study.48 In contrast, other previous studies18,20,49 found significant association between maternal educational status and developmental delay among under-five children. Lastly, the present study found insignificant association between paternal educational status and developmental delay of under-five children in line with a previous study.18 In contrast, another study23 found a significant association between paternal educational status and child developmental delay. Since this study’s findings are based upon a cross-sectional design, it did not enable us to conclude about the casual relationship. But, being a community-based study and using both urban and rural populations for analysis were the major strengths of this study.
Conclusion
In the current study, the overall prevalence of developmental delay was 22.6%. The prevalence of chronic under-nutrition, acute under-nutrition and being underweight was 36.3%, 14.2% and 20.3%, respectively. Maternal diseases, birth interval and nutritional status of under-five children were among the factors which revealed statistically significant association with developmental delay of children aged under five years. We recommend the concerned body to work on improving maternal health status during pregnancy, to adequately space subsequent births through the use of family planning and to work on improving the nutritional status of women and children aged under five years in the current study area in order to improve the development of such children.
Abbreviations
AK, Administrative Kebeles; ANC, Ante Natal Care; ASQ-3, Age and Stage Questionnaire 3rd edition; AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Crude Odds Ratio; EDHS, Ethiopian Demographic Health Survey; HFA, height-for-age; SD, Standard Deviation; SPSS, Statistical Package for Social Sciences; UNICEF, United Nations International Children’s Emergency Fund; WFA, weight-for-age; WFH, weight-for-height; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon request to corresponding author.
Acknowledgments
The authors would like to acknowledge Debre Markos University for providing ethical approval. Moreover, they would like also to acknowledge the study participants for their willingness to participate in the study; without their participation the study would not be finalized based on the stated objectives. Finally, the authors extend their appreciation to East Gojjam Zone Administration and the respective woreda and kebele administrative bodies.
Author Contributions
Amsalu Taye Wondemagegn was principal investigator involved in conception and design of the study, collection, entry, analysis, and interpretation of the data and preparation of the manuscript. Abay Mulu was involved in design of the study, entry, analysis, writing and interpretation of data as well as revision of the manuscript. Both authors contributed equally to this work; made a significant contribution to the work reported, took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for this research.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Fraser Mustard J. Early Human Development - Equity from the Start - Latin America. Revista Latinoamericana de Ciencias Sociales. 2009;7:639–680.
2. de Mello DF, Henrique NC, Pancieri L, Veríssimo Mde L, Tonete VL, Malone M. Child safety from the perspective of essential needs. Rev Lat Am Enfermagem. 2014;22(4):604–610. doi:10.1590/0104-1169.3651.2458
3. Souza JM, Veríssimo M. Child development: analysis of a new concept. Rev Lat Am Enfermagem. 2015;23(6):1097–1104. doi:10.1590/0104-1169.0462.2654
4. Young ME. From Early Child Development to Human Development: Investing in Our Children’s Future. World Bank Publications; 2002.
5. Prado EL, Dewey KG. Nutrition and brain development in early life. Nutr Rev. 2014;72(4):267–284. doi:10.1111/nure.12102
6. Spinazzola J, Ford J, Zucker M, et al. National survey of complex trauma exposure, outcome and intervention for children and adolescents. Psychiatr Ann. 2005;35(5):433–439. doi:10.3928/00485713-20050501-09
7. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B; International Child Development Steering G. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007;369(9555):60–70. doi:10.1016/S0140-6736(07)60032-4
8. Central Statistical Agency CSAE, Icf. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
9. Jimoh AO, Anyiam JO, Yakubu AM. Relationship between child development and nutritional status of under-five Nigerian children. South Af J Clin Nutrition. 2018;31(3):50–54. doi:10.1080/16070658.2017.1387434
10. Workie SB, Mekonen T, Mekonen TC, Fekadu W. Child development and nutritional status in 12–59 months of age in resource limited setting of Ethiopia. J Health Popul Nutr. 2020;39(1):1–9. doi:10.1186/s41043-020-00214-x
11. Moodie S, Daneri P, Goldhagen S, Halle T, Green K, LaMonte L. Early Childhood Developmental Screening: a Compendium of Measures for Children Ages Birth to Five. OPRE Report 2014-11. US Dep Health Human Services. 2014;4:58.
12. World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. World Health Organization; 2006.
13. Squires J, Bricker DD, Twombly E. Ages & Stages Questionnaires. Baltimore, MD, USA: Paul H. Brookes; 2009.
14. Juneja M, Mohanty M, Jain R, Ramji S. Ages and Stages Questionnaire as a screening tool for developmental delay in Indian children. Indian Pediatr. 2012;49(6):457–461. doi:10.1007/s13312-012-0074-9
15. World Health Organization. WHO Anthro for Personal Computers, Version 2. Software for Assessing Growth and Development of the World’s Children. Geneva: World Health Organization; 2007.
16. Bahtiar BA, Yusof HM, Kamarudin KS. Child Development and Nutritional Status of Children Under Five: a Cross-Sectional Study of a Fishermen Community in Terengganu, Malaysia. Jurnal Gizi Dan Pangan. 2021;16(2):91–100. doi:10.25182/jgp.2021.16.2.91-100
17. Agarwal D, Chaudhary SS, Sachdeva S, Misra SK, Agarwal P. Prevalence of developmental delay and factors affecting the development status among under 5 children in an urban slum of Agra city. National J Commun Med. 2018;9(7):474–479.
18. Shatla MM, Goweda RA. Prevalence and Factors Associated with Developmental Delays among Preschool Children in Saudi Arabia. J High Ins Public Health. 2020;50(1):10–17. doi:10.21608/jhiph.2020.79318
19. Sharma N, Masood J, Singh SN, et al. Assessment of risk factors for developmental delays among children in a rural community of North India: a cross-sectional study. J Educ Health Promot. 2019;8. doi:10.4103/jehp.jehp_189_18
20. Gunardi H, Nugraheni RP, Yulman AR, et al. Growth and developmental delay risk factors among under-five children in an inner-city slum area. Paediatr Indones. 2019;59(5):276–283. doi:10.14238/pi59.5.2019.276-83
21. Saleem J, Zakar R, Bukhari GMJ, Fatima A, Fischer F. Developmental delay and its predictors among children under five years of age with uncomplicated severe acute malnutrition: a cross-sectional study in rural Pakistan. BMC Public Health. 2021;21(1):1–10. doi:10.1186/s12889-021-11445-w
22. Al-Fadhli KY, Al-Bunaian NA. Prevalence and social influences of delayed language development in preschool-age Saudi children. Int J Sci Res. 2017;6(8):1712–1720.
23. Yaghini O, Kelishadi R, Keikha M, et al. Prevalence of developmental delay in apparently normal preschool children in Isfahan, Central Iran. Iranian j Child Neurol. 2015;9(3):17.
24. Dorre F, Fattahi Bayat G. Evaluation of children’s development (4-60mo) with history of NICU admission based on ASQ in Amir kabir Hospital, Arak. J Ardabil Univ Med Sci. 2011;11(2):143–150.
25. Luoma I, Tamminen T, Kaukonen P, et al. Longitudinal study of maternal depressive symptoms and child well-being. J Am Acad Child Adolesc Psychiatry. 2001;40(12):1367–1374. doi:10.1097/00004583-200112000-00006
26. O’Connor TG, Heron J, Golding J, Glover V, Team ALSS. Maternal antenatal anxiety and behavioural/emotional problems in children: a test of a programming hypothesis. J Child Psychol Psychiatry. 2003;44(7):1025–1036. doi:10.1111/1469-7610.00187
27. Torabi F, Akbari SAA, Amiri S, Soleimani F, Majd HA. Correlation between high-risk pregnancy and developmental delay in children aged 4–60 months. Lib J Med. 2012;7(1):879. doi:10.3402/ljm.v7i0.18811
28. Sajedi F, Alizad V. The incidence of motor developmental delay in high risk infants and effective risk factors in developing of it. 2004.
29. Plagemann A. Perinatal programming and functional teratogenesis: impact on body weight regulation and obesity. Physiol Behav. 2005;86(5):661–668. doi:10.1016/j.physbeh.2005.08.065
30. Cheslack-Postava K, Liu K, Bearman PS. Closely spaced pregnancies are associated with increased odds of autism in California sibling births. Pediatrics. 2011;127(2):246–253. doi:10.1542/peds.2010-2371
31. Chungkham HS, Sahoo H, Marbaniang SP. Birth interval and childhood undernutrition: evidence from a large scale survey in India. Clin Epidemiol Global Health. 2020;8(4):1189–1194. doi:10.1016/j.cegh.2020.04.012
32. Gebrehiwot SW, Abera G, Tesfay K, Tilahun W. Short birth interval and associated factors among women of child bearing age in northern Ethiopia, 2016. BMC Women’s Health. 2019;19(1):1–9. doi:10.1186/s12905-019-0776-4
33. Das T, Roy TB. While inadequate birth interval becomes detrimental to health & nutritional outcome in infant and under-five year children; a systematic review through BLR and CPH model. Clin Epidemiol Global Health. 2021;11:100714. doi:10.1016/j.cegh.2021.100714
34. Conde‐Agudelo A, Rosas‐Bermudez A, Castaño F, Norton MH. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms. Stud Fam Plann. 2012;43(2):93–114. doi:10.1111/j.1728-4465.2012.00308.x
35. Wendt A, Gibbs CM, Peters S, Hogue CJ. Impact of increasing inter‐pregnancy interval on maternal and infant health. Paediatr Perinat Epidemiol. 2012;26:239–258. doi:10.1111/j.1365-3016.2012.01285.x
36. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects of birth spacing on maternal health: a systematic review. Am J Obstet Gynecol. 2007;196(4):297–308. doi:10.1016/j.ajog.2006.05.055
37. Norton M. New Evidence on Birth Spacing: Promising Findings for Improving Newborn, Infant, Child, and Maternal Health. Vol. 89. Wiley Online Library; 2005:S1–S6.
38. Pimentel J, Ansari U, Omer K, et al. Factors associated with short birth interval in low-and middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2020;20(1):1–17. doi:10.1186/s12884-020-2852-z
39. Huiracocha-Tutiven L, Orellana-Paucar A, Abril-Ulloa V, Huiracocha-Tutiven M, Palacios-Santana G, Blume S. Child development and nutritional status in Ecuador. Global Pediatric Health. 2019;6:2333794X18821946.
40. Vazir S, Naidu AN, Vidyasagar P. Nutritional status, psychosocial development and the home environment of Indian rural children. Indian Pediatr. 1998;35:959–966.
41. Hamadani JD, Fuchs GJ, Osendarp SJM, Khatun F, Huda SN, Grantham-McGregor SM. Randomized controlled trial of the effect of zinc supplementation on the mental development of Bangladeshi infants. Am J Clin Nutr. 2001;74(3):381–386. doi:10.1093/ajcn/74.3.381
42. Chattopadhyay N, Saumitra M. Developmental outcome in children with malnutrition. J Nepal Paediatric Soc. 2016;36(2):170–177. doi:10.3126/jnps.v36i2.14619
43. World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers. World Health Organization; 2007.
44. Sajedi F, Vameghi R, Kraskian Mujembari A. Prevalence of undetected developmental delays in Iranian children. Child Care Health Dev. 2014;40(3):379–388. doi:10.1111/cch.12042
45. Bello AI, Quartey JNA, Appiah LA. Screening for developmental delay among children attending a rural community welfare clinic in Ghana. BMC Pediatr. 2013;13(1):119. doi:10.1186/1471-2431-13-119
46. Kapci EG, Kucuker S, Uslu RI. How applicable are Ages and Stages Questionnaires for use with Turkish children? Topics Early Child Spec Educ. 2010;30(3):176–188. doi:10.1177/0271121410373149
47. Kaur S, Sidhu NS, Randhawa RK. Biological Risk Factors and Early Developmental Delay Assessment in Infants Using Ages and Stages Questionnaire, Version 3 (ASQ-3). Int J Res Rev. 2021;8(7):272–277. doi:10.52403/ijrr.20210738
48. Valla L, Wentzel-Larsen T, Hofoss D, Slinning K. Prevalence of suspected developmental delays in early infancy: results from a regional population-based longitudinal study. BMC Pediatr. 2015;15(1):1–8. doi:10.1186/s12887-015-0528-z
49. Handal AJ, Lozoff B, Breilh J, Harlow SD. Sociodemographic and nutritional correlates of neurobehavioral development: a study of young children in a rural region of Ecuador. Revista Panamericana de Salud Pública. 2007;21:292–300. doi:10.1590/S1020-49892007000400004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.