")
Back to Journals » Journal of Blood Medicine » Volume 11
Effects of –3.7α Deletion and Sickle-Cell Trait on Ventilatory and Hemodynamic Responses to Maximum Exercise in Young Saudi Females
Authors Al Asoom LI , Al Makhaita MM, Rafique N , Al Afandi DT , Al Otaibi WM , Alsuwat HS, Alaithan MA , AbdulAzeez S , Borgio JF
Received 20 July 2020
Accepted for publication 5 September 2020
Published 20 October 2020 Volume 2020:11 Pages 371—378
DOI https://doi.org/10.2147/JBM.S272905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Lubna Ibrahim Al Asoom,1 Marwah Mansour Al Makhaita,1 Nazish Rafique,1 Dina Tariq Al Afandi,2 Waad Mohammed Al Otaibi,3 Hind Saleh Alsuwat,3 Mousa A Alaithan,3 Sayed AbdulAzeez,3 J Francis Borgio3
1Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Depatment of Pediatrics, College of Medicine, King Fahd Hospital of the University, Dammam, Saudi Arabia; 3Department of Genetic Research, Institute for Research and Medical Consultation (IRMC), Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Lubna Ibrahim Al Asoom
Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Email [email protected]
Introduction: Hemoglobinopathies are common disorders in Saudi Arabia and have an impact on the general health of the affected individuals. The current study aimed to find out the effects of the presence of α 3.7 kb rightward deletion or sickle-cell trait (SCT) on ventilatory and hemodynamic parameters of maximum exercise testing in young Saudi women.
Methods: In a cross-sectional study, 75 randomly selected female students from different colleges were tested for VO2max using a COSMED system for maximum exercise testing. Blood parameters and globin genotyping were determined.
Results: Hemoglobin genetic studies revealed 28 of the students had 3.7 α-globin deletion only (− 3.7α2/α1α2), five had SCT, and 42 had normal α-globin (α1α2/α1α2 and no HbS) and were considered the control group. Subjects with − 3.7α2/α1α2 showed significantly lower VO2max and higher resting systolic blood pressure, while SCT carriers showed no difference in regard to ventilatory parameters, but had higher post-exercise systolic blood pressure than controls.
Conclusion: It is concluded that individuals with 3.7 α-globin deletion might have lower fitness capacity, as demonstrated by lower VO2max, which might explain the general lower VO2max in the young women of this population. Furthermore, increments in resting systolic and posteexercise systolic blood pressure in 3.7 α-globin deletion and SCT, respectively, might indicate a future risk of cardiovascular diseases and require attention and extensive studies.
Keywords: cardiopulmonary exercise testing, exercise test, α-globin, sickle-cell trait, blood pressure, Saudi Arabia
Introduction
Hemoglobinopathies are common disorders in Saudi Arabia. These are genetic conditions characterized by an abnormal hemoglobin structure, due to various forms of mutations. The major types of hemoglobinopathies encountered in Saudi Arabia are sickle-cell disease and the two forms of thalassemia, ie, α and β.1 In a recent study, the overall prevalence (per 1,000 inhabitants) of sickle-cell disease was found to be 49.6, with the rate of carrier state 45.8 per 1,000 and diseased 3.8 per 1,000. On the other hand, the overall prevalence of β-thalassemia was 13.6 per 1,000 population, with 12.9 carriers and 0.7 diseased.2,3 The eastern and southern provinces of Saudi Arabia demonstrate the highest rate of both sickle-cell disease and β-thalassemia.4 Sickle-cell anemia and β-thalassemia manifest with severe anemia, failure to thrive, and multiorgan damage, and need frequent follow-up, hospitalization, lifelong medication, and blood transfusion.5 Sickle cell trait (SCT) is the carrier state of sickle-cell disease that results from inheriting one copy of a specific mutation in the β-globin gene. Two copies of this mutated gene encode the abnormal hemoglobin of sickle-cell anemia known as HbS. SCT is commonly known as a benign disorder, and those who carry it usually have a normal life.6 However, many incidents of sudden death have been reported with SCT carriers while performing physical activity under extreme conditions, such as at high altitude and high temperature.7 Properties of HbS in SCT carriers, such as low affinity to carry oxygen and abnormal rheology, are expected to develop into a condition of exertional sickling to SCT carriers.8
α-Thalassemia is also highly prevalent in the same regions of Saudi Arabia. Its rate reaches 45% of the population in the highest incident areas.9 Saudi research has revealed a mild reduction in the incidence of sickle-cell anemia and β-thalassemia owing to governmental preventive and screening programs; however, the rate of α-thalassemia remains constant, due to lack of screening tests for α carriers.4 α-Thalassemia ranges from a silent, mild condition of microcytic hypochromic anemia to a major lethal form.10 The presentation of α-thalassemia depends on the type of mutation in the α gene. It varies, with possible deletion, substitution, or complete absence of the gene. The 3.7α rightward deletion is one of the most prevalent deletions in the Saudi population. Deletion of one α-globin gene (−3.7α2/α1α2) among the four genes is designated α-thalassemia silent, and individuals born with this mutation live normal lives.11
Since oxygen-carrying capacity is an important factor in normal physical activity, we planned to study effects of the high prevalence of carrier states of an abnormal hemoglobin, in particular 3.7α rightward deletion and SCT, in the eastern province in extreme conditions of maximum exercise. Maximum oxygen consumption (VO2max) is the main component in cardiopulmonary exercise testing (CPET) and the gold standard for the assessment of physical fitness.12 In this study, we planned to perform CPET in SCT carriers, α-thalassemia–silent, and control subjects, and all ventilatory and hemodynamic parameters would be compared among the groups. We hypothesized that SCT-carrier females and those with the −3.7α2/α1α2 genotype would have lower ventilatory and abnormal hemodynamic responses in comparison with non-SCT carriers and non-α-thalassemia–silent females during CPET.
Methods
This was a cross-sectional study conducted from March 2017 to March 2018. A total of 75 Saudi female college students aged 19–25 years were randomly selected from different health colleges (Medicine, Dentistry, Nursing, Applied Medical Science and Clinical Pharmacy) of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. A list of all female students was requested from the administration. Students were numbered and arranged in ascending order. A random sample was selected based on numbers, and students were interviewed and assessed for eligibility. The sample size was calculated to assess VO2max using G*power 3.1 statistical power–analysis software13 based on the calculation of effect size to give the study power of 95%. An effect size of 0.21 was calculated using the mean VO2max value of the null hypothesis: H0 = 33.7 and SD = 10.97. Mean VO2max and SD values were taken from a local study.14 The mean VO2max value of the alternative hypothesis was H1 = 36. Sudents were grouped as −3.7α2/α1α2 (n=28), SCT (n=5), and without 3.7α rightward deletion or SCT (n=42). The last group was considered the control group.
Criteria for inclusion in the study were being apparently healthy, with normal body BMI of 18.50–24.99 kg/m2),15 and sedentary according to the definition of the International Physical Activity Questionnaire.16 Participants with any contraindication of exercise stress testing, known chronic illness, had undergone major surgery, or taking any medication apart from nonsteroidal anti-inflammatory drugs were excluded from the study. Additionally, pregnancy, breastfeeding, smoking, and using ergogenic aids were also considered exclusion criteria. All participants signed a written informed consent for participation in the study, including all the required procedures. The design of the study and all procedures performed complied with the Declaration of Helsinki and university ethical committee guidelines. Approval was awarded by the Institutional Review Board of the University of Imam Abdulrahman Bin Faisal (approval IRB –PGS-2017-01-219).
Cardiopulmonary Exercise Testing
Equipment and Setup
The exercise was carried out in the Exercise Research Center of the College of Applied Medical Sciences. All tests were performed from 10:00 am to 1:00 pm using COSMED system for CPET (Quark CPET; COSMED, Rome, Italy). This is composed of a gas analyzer (breath by breath analyzer) for continuous gas-exchange measurements made by open-circuit spirometry, electronically braked cycle ergometry (Ergoline), an electrocardiogram (ECG) monitor (wireless 12-lead stress PC ECG), arterial blood pressure cuff (mercury sphygmomanometer, diplomat-presameter sphygmomanometer, [Riester, Jungingen, Germany] and Spot Vital Signs device [Welch Allyn, Skaneateles Falls, NY, USA]), a pulse oximeter, and computer and online-analysis software for final reports. The system was calibrated in accordance with the manufacturer’s instructions.
Procedure
All subjects performed a maximal-exercise test on a stationary bicycle ergometer using 1-minute increments. Selection of the work-rate increase needed for the students was calculated by a formula previously published for cycle ergometry and sedentary females:17
- VO2 unloaded in mL/min = 150 + (6 × weight [kg]).
- Peak VO2 in mL/min = (height [cm] – age [years]) ×20 for sedentary men and ×14 for sedentary women.
- Work-rate increment per minute in watts = (peak VO2 in mL/min – VO2 unloaded in mL/min)/100.
Age-predicted maximal heart rate was obtained from the formula 220 – age).17 Subjects had measurement of resting arterial blood pressure (BP) taken in sitting position from the right arm. Three measurements of resting arterial blood pressure were recorded at three intervals, first after 5 minutes of rest then two after 3 minutes. The three readings were averaged.
After a period of rest, the incremental protocol allowed the subject initially to cycle for 3 minutes of unloaded pedaling as a warm-up. Then, power output started at 20 W and increased by 15 W every minute by computer control until the subject was limited by debilitating symptoms despite verbal encouragement. Cycling frequency was maintained at 50 rpm throughout the exercise with the assistance of the digital display on the bike to maintain the required cycling pace. Finally, subjects were asked to continue cycling for 3 minutes without resistance in the recovery period. Time till exhaustion was recorded. Subjects were asked about the reason for stopping the exercise test. The duration of the exercise was 6–12 minutes. Heart rate, oxygen saturation (SpO2%), arterial blood pressure, and ECG were monitored at resting baseline, during the exercise test, and 3 minutes postexercise. Maximum heart rate and blood pressure of the last achieved stage were determined.
Based on breath-gas analysis, VO2max, mL/min and mL/kg.min), carbon dioxide production (VCO2, mL/min), minute ventilation (L/min), respiratory rate (breaths/min), tidal volume (L), respiratory exchange ratio, ventilatory anerobic threshold (mL/min and mL/kg.min) were measured. VO2 values were considered maximal when two of four criteria were achieved: plateau of VO2 despite an increase in workload, respiratory exchange ratio 1:1 or higher, heart rate within 15 beats of the age-predicted maximum, and/or rating of perceived exertion ≥17. American College of Sport Medicine guidelines of indications for terminating exercise testing were followed.17
Hematologic Tests and Globin Genotypes
Blood samples were collected in EDTA vacutainers and analyzed for complete blood count (Hb g/dL, red blood cell [RBC] count, hematocrit, mean cell volume [MCV], mean corpuscular hemoglobin [MCH], MCH concentration, red cell–distribution width), iron concentration, serum ferritin, total iron-binding capacity, fetal hemoglobin percentage, HbS percentage, and HbA2 percentage. Genomic DNA from the blood samples was isolated and genotypes of α- and β-globin genes analyzed using Sanger sequencing with a BigDye Terminator kit (3500 genetic analyzer; Applied Biosystems, Foster City, CA, USA). Electropherograms were analyzed using DNA sequencing–analysis software version 5.4 (Applied Biosystems).
Statistical Analysis
SPSS 22 was used to perform statistical analyses. All data are expressed as means ± SD (interquartile range). Independent-sample Student’s t-tests were used to compare ventilatory and hemodynamic parameters between SCT carriers and controls and α-thalassemia silent vs controls. P<0.05 was considered significant.
Results
We evaluated 75 women aged 19–25 years (mean 20.29±0.99 years). These Saudi subjects were assigned to three groups: SCT (n=5), 3.7α rightward deletion (−3.7α2/α1α2, n=28), and controls who had been confirmed to have neither SCT nor 3.7α rightward deletion (α1α2/α1α2, n=42). Body indices and hematologic, ventilatory, and cardiovascular (hemodynamic) parameters of the three groups are presented in Table 1. On independent-sample Student’s t-tests comparing SCT carriers and controls, MCH and MCV were significantly lower in SCT carriers (P=0.004 and 0.045, respectively), while students with −3.7α2/α1α2 demonstrated significantly lower hemoglobin (P=0.02), MCH (P=0.005), MCV (P=0.00005), and VO2max than controls (P=0.004). Additionally, 3.7α deletion showed borderline- significance for higher resting systolic blood pressure (P=0.049) and SCT carriers significantly higher post-exercise systolic blood pressure (P=0.037).
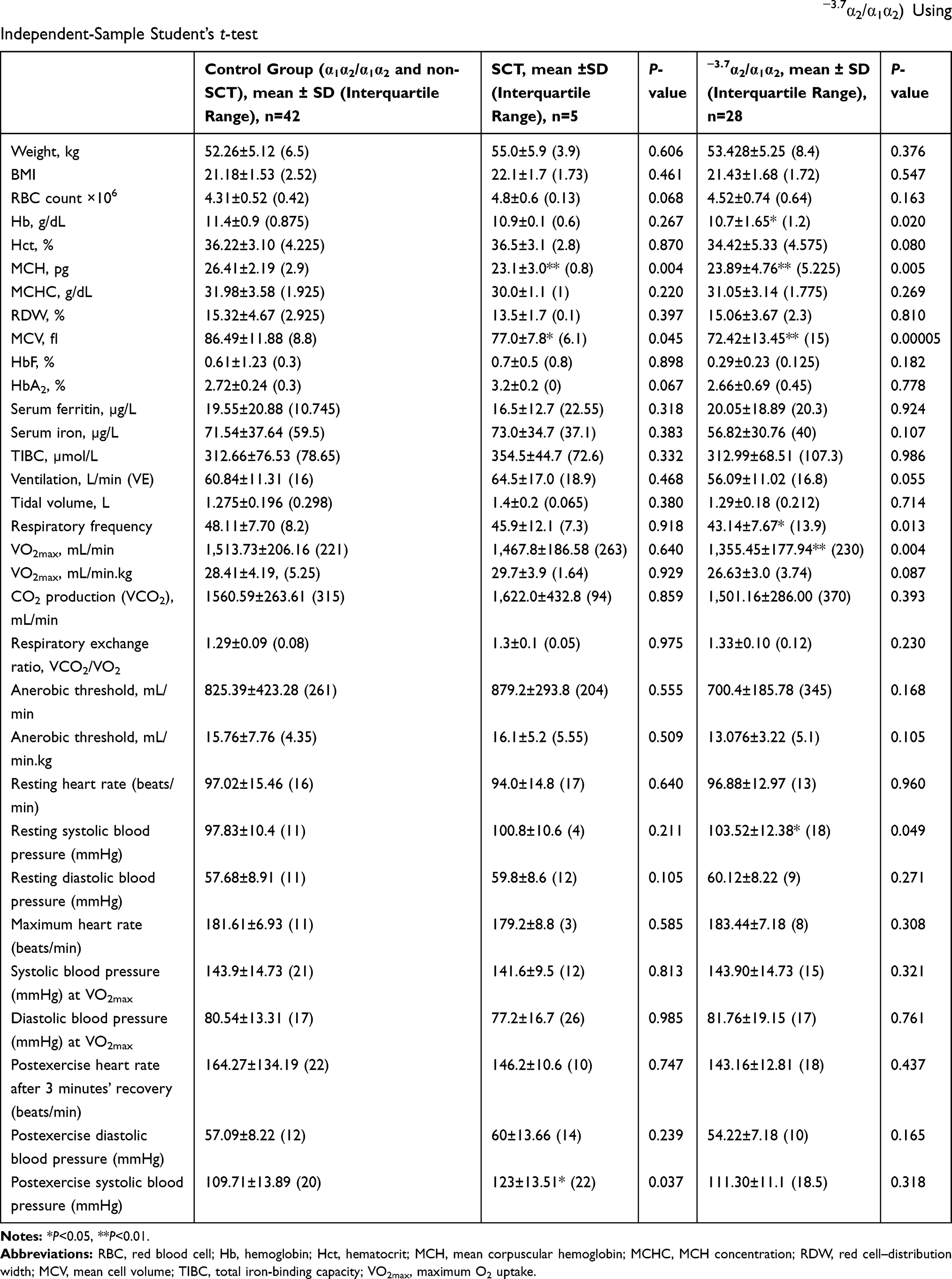 |
Table 1 Comparison of Body Indices and Hematological, Ventilatory, and Hemodynamic Parameters Between the Control Group and Sickle-Cell Trait (SCT) Subjects, and Between the Control Group and Subjects with 3.7 Rightward Deletion (−3.7α2/α1α2) Using Independent-Sample Student’s t-test |
All participants were subjected to genotyping analysis, ie, functional exonic (β0 or β+), intronic, and α-globin DNA variations (Table 2). The groups were compared in terms of β (HBB) mutations and α-globin–deletion mutations (Table 2). As shown in β0 or β+ mutations, the presence of hetero HBB:c20A>T on direct HBB sequencing was confirmed in all members of the SCT group. There were three exonic types in the control group, with highest appearance of hetero HBB:c435G>A (n=3). The −3.7α2/α1α2 group showed two exonic mutations only: hetero HBB:c431T>A (n=1) and hetero HBB:c93–21G>A (n=1). As the number of β-thalassemia carriers is very small, separate analysis was not done. Regarding the intronic mutations, hetero c315+74T>G had the highest appearance in the whole sample (n=26) and specifically in the control group (n=14). The second–most frequently occurring was homo c315+16G>C (n=21), but it appeared in the SCT group (n=3) and −3.7α2/α1α2 (n=18) only. Homo c315+74T>G (n=20) was found to be high in healthy control females (n=10) and −3.7α2/α1α2 (n=10). Furthermore, the α-globin genotype revealed a total of 28 with –3.7α2/α1α2 and 42 with α1α2/α1α2, while in SCT carriers two α-globin genotypes –3.7α2/α1α2 (n=2), two α1α2/α1α2 (n=2), and –4.2α1/α1α2 (n=1) were found (Table 2).
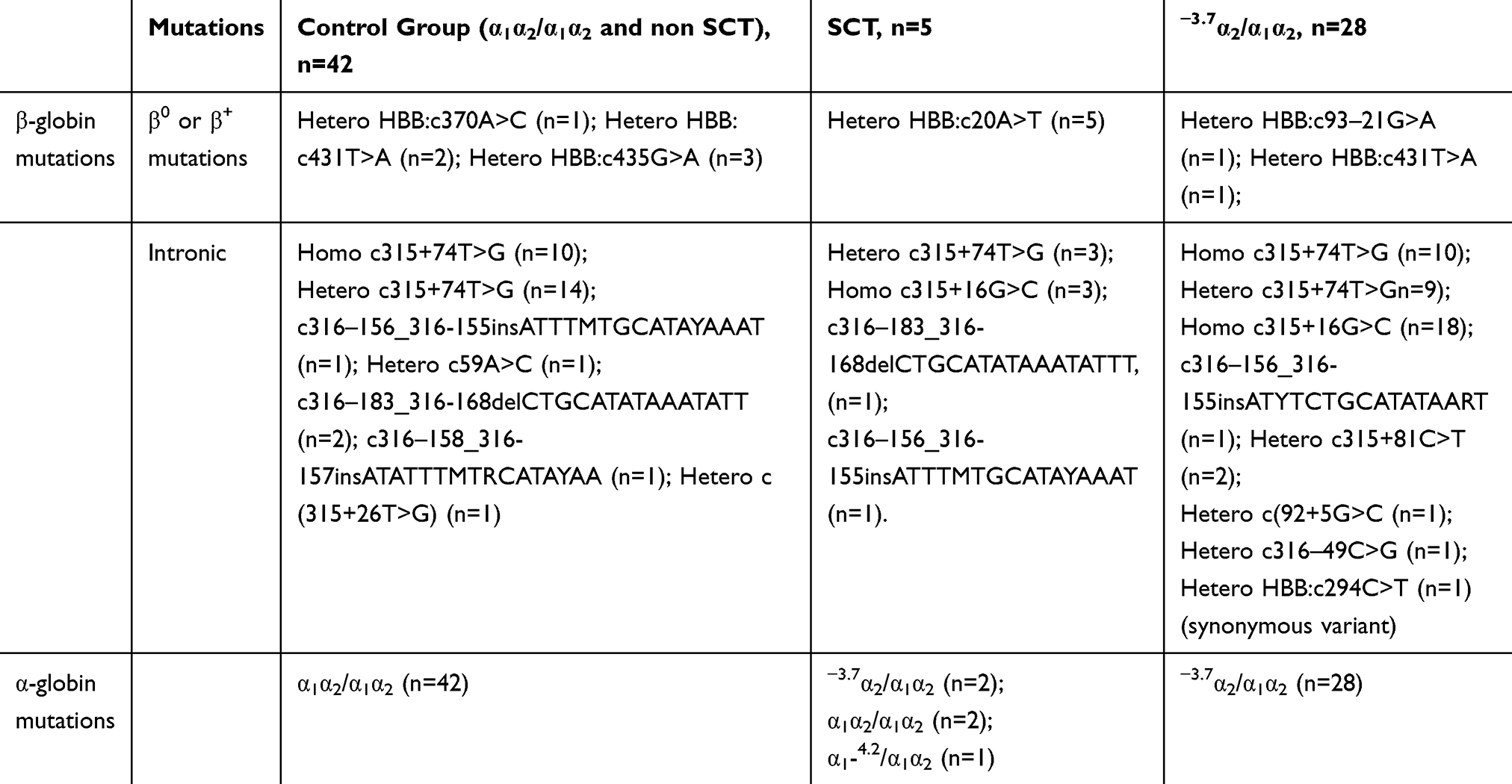 |
Table 2 β-globin Gene Variations in the Study Subjects |
Discussion
The 3.7α rightward deletion and sickle-cell mutation are the most prevalent globin-gene variations in the Saudi Arabian population, particularly in the eastern and southern regions.3,11 Despite active epidemiological studies and national screening programs for genetic blood diseases in Saudi Arabia, some carriers remain hidden and undiagnosed.18 Physical fitness assessment represented by VO2max in young, apparently healthy Saudi females in the eastern province revealed low values compared to international values, and the mechanism behind this remains uncertain.14,19,20 A recent attempt to explore such mechanisms studied functional exonic variations of low-VO2max Saudi females and revealed the association of genes involved in heart rate, body weight, breath tests, proteolysis, and cardiac muscle–fiber development.21 However, that study did not involve the most common hematologic abnormalities present in the area, ie, SCT and 3.7α rightward deletion. As such, the present study focused on the possible association of the presence of 3.7α rightward deletion and SCT among Saudi women with varying ventilatory and hemodynamic parameters associated with maximum exercise capacity. The present study revealed that 3.7α deletion is associated with low VO2max, due to hidden or clinically undiagnosed defective O2-carriage capacity. This is the first of its kind in observing the association of the 3.7α rightward deletion (−3.7α2/α1α2) with low VO2max among young women. The current diminished VO2max was further reflected by the microcytosis (MCV), and low MCH of 3.7α2/α1α2 females compared to normal subjects. Mehdi et al aimed to compare hematologic indices of inherited α- and β-thalassemia in Saudi Arabia. He found that low MCV and MCH with were the most important parameters in the diagnosis of α-thalassemia minor.4
Our subjects with 3.7α rightward deletion (−3.7α2/α1α2) demonstrated a borderline increase in resting systolic blood pressure. Based on experimental animal studies, it is believed that lack of α-hemoglobin culminates in a reduction in arterial blood pressure, because α-hemoglobin is expressed not only in RBCs but also in the endothelial cells of the vessels. α-Hemoglobin forms a complex structure with the enzymes regulating the metabolism of nitric oxide (NO). Lack of the α subunit culminates in an overbioavailability of NO and leads to relaxation of smooth-muscle cells of the arterioles and hence a reduction in arterial blood pressure.22,23 However, results collected from human subjects reveals conflicting data regarding the effect of α-thalassemia on arterial blood pressure. Some investigators have shown an elevated blood pressure and higher incidence of hypertension in α-thalassemic carriers.24 The increase in arterial blood pressure in α-thalassemic subjects was explained by the presence of high level of HbH in these carriers. HbH has higher affinity for NO than HbA. When HbH is infused into rats, it raises arterial blood pressure.25 Using 24-hour ambulatory arterial blood-pressure monitoring, Etyang et al showed normal arterial blood pressure in Kenyan adolescents with α-thalassemia.26 Therefore, it can be postulated that changes in arterial blood pressure in α-thalassemic carriers might be the result of the interaction between the two previously mentioned mechanisms, ie, the effect of deficiency in the α subunit in the endothelium and the increase in HbH. The current finding of low VO2max and relatively high resting systolic blood pressure in 3.7α rightward deletion is a very important one, and should raise the alert toward possible increased cardiovascular risk in this carrier group.
On the other hand, SCT carriers showed no difference in VO2max compared to controls. Although the sample in our study was small, particularly in regard to SCT (n=5), previous studies support our finding. In a longitudinal study estimating cardiovascular risk in healthy and SCT subjects, there were no differences between the two groups in regard to baseline fitness, duration of maximum exercise, heart rate, or metabolic equivalent of predetermined tasks.27 Similarly, several studies using incremental maximum exercise demonstrated no difference between SCT carriers and normal controls in regard to VO2max, ventilatory threshold, or hemodynamic parameters.28–31 Despite such experimental evidence for normal fitness levels of SCT carriers, some authors believe that SCT carriers might be hindered from highly competitive sports. Le Gallais et al observed no SCT carriers among Abidjan half-marathoners.32 Thiriet et al33 found that SCT candidates showed lower performance times that non-SCT ones during the Mount Cameroon Ascent Race.The pathophysiology behind these observations is not clear; however it was suggested that strenuous exercise might expose SCT carriers to dehydration that might affect the rheology of RBCs, leading to deformity of these cells, increasing blood viscosity, precipitating vaso-occlusive events, as well as triggering massive proinflammatory responses.34,35
Our SCT group showed also significantly higher postexercise systolic blood pressure than controls. SCT carriers are prone to ischemic heart attacks, stroke, and renal disease.27 Several investigations have been performed to find out the role of changes in blood pressure in cardiovascular and ischemic complications of SCT. However, most studies demonstrated no difference in resting arterial blood pressure between SCT carriers and controls.27,36 Even using ambulatory 24 hour blood-pressure monitoring, Etyang et al found no difference between the young SCT adolescents and their controls.37 However, in this study the significantly higher postexercise systolic blood pressure reflected another aspect of the control and regulation of arterial blood pressure: it demonstrates the recovery response of systolic blood pressure after maximum exercise.38 It most probably reflects a delay in the restoration of the resting sympathovagal balance in SCT carriers compared to normal controls. Furthermore, this is also an important finding that should draw attention toward the cardiovascular risk of SCT carriers, which was elucidated by maximum exercise.
Conclusion
The current study demonstrated for the first time that female students with the −3.7α2/α1α2 genotype exhibited lower VO2max than female students with the α1α2/α1α2 genotype. The −3.7α2/α1α2 group showed also lower MCH and MCV and a borderline increase in resting systolic blood pressure, while the SCT group exhibited normal ventilatory responses to maximum incremental exercise testing, with lower MCH and MCV. Furthermore, the SCT group showed higher postexercise systolic blood pressure than normal controls, which might indicate a delay in recovery of the sympathovagal balance during the postexercise period.
Acknowledgments
The authors thank the dean of the Institute for Research and Medical Consultations (IRMC), Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia for her continuous support and encouragement. This study was supported by the Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University (To Dr LIA, grant 2015292). We also appreciate the technical assistance from Mr Ranilo M Tumbaga, Mr Horace T Pacifico, and Ms Jee E Aquino.
Disclosure
The authors declare no competing interests for this work.
References
1. Al-Shahrani M. Steps toward the prevention of hemoglobinopathies in the kingdom of Saudi Arabia. Hemoglobin. 2009;33(Suppl sup1):S21–S24. doi:10.3109/03630260903346437
2. Alsaeed ES, Farhat GN, Assiri AM, et al. Distribution of hemoglobinopathy disorders in Saudi Arabia based on data from the premarital screening and genetic counseling program, 2011–2015. J Epidemiol Glob Health. 2017;7(Suppl S1):S41–S7. doi:10.1016/j.jegh.2017.12.001
3. Alaithan MA, AbdulAzeez S, Borgio JF. A comprehensive review of the prevalence of beta globin gene variations and the co-inheritance of related gene variants in Saudi Arabians with beta-thalassemia. Saudi Med J. 2018;39(4):329–335. doi:10.15537/smj.2018.4.21360
4. Mehdi SR, Al Dahmash BA. A comparative study of hematological parameters of α and β thalassemias in a high prevalence zone: saudi Arabia. Indian Journal of Human Genetics. 2011;17(3):207–211. doi:10.4103/0971-6866.92106
5. Alotaibi MM. Sickle cell disease in Saudi Arabia: A challenge or not. J Epidemiol Glob Health. 2017;7(2):99–101. doi:10.1016/j.jegh.2016.12.006
6. Al-Ali AK, Alsulaiman A, Alzahrani AJ, et al. Prevalence and Diversity of Haplotypes of Sickle Cell Disease in the Eastern Province of Saudi Arabia. Hemoglobin. 2020;44(2):78–81. doi:10.1080/03630269.2020.1739068
7. Xu Z, Zheng Y, Wang X, et al. Stiffening of sickle cell trait red blood cells under simulated strenuous exercise conditions. Microsyst Nanoeng. 2016;2(1):16061. doi:10.1038/micronano.2016.61
8. Wirthwein DP, Spotswood SD, Barnard JJ, Prahlow JA. Death due to microvascular occlusion in sickle-cell trait following physical exertion. J Forensic Sci. 2001;46(2):399–401. doi:10.1520/JFS14982J
9. Akhtar MS, Qaw F, Borgio JF, et al. Spectrum of α -Thalassemia Mutations in Transfusion-Dependent β-Thalassemia Patients from the Eastern Province of Saudi Arabia. Hemoglobin. 2013;37(1):65–73. doi:10.3109/03630269.2012.753510
10. Borgio JF. Molecular nature of alpha-globin genes in the Saudi population. Saudi Med J. 2015;36(11):1271–1276. doi:10.15537/smj.2015.11.12704
11. Borgio JF, Abdulazeez S, Almandil NB, et al. The α3.7 deletion in α‑globin genes increases the concentration of fetal hemoglobin and hemoglobin A2 in a Saudi Arabian population. Mol Med Rep. 2018;17(1):1879–1884.
12. Principles of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications.
13. Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
14. Al Asoom L. Is cardiopulmonary fitness level a risk factor in young Saudi females? Journal of King Abdulaziz University - Medical Sciences. 2015;22(3):19–28. doi:10.4197/Med.22-3.3
15. Global Database on Body Mass Index: WHO; 2017 Available from: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html.
16. International Physical Activity Questionnaire. 2017.
17. ACSM’s guidelines for exercise testing and prescription. Ninth Edition Ed: Wolter Kluwer. Lippincott Williams & Wilkins; 2014.
18. Eissa M, Patel AA, Farag S, et al. Awareness and Attitude of University Students About Screening and Testing for Hemoglobinopathies: case Study of the Aseer Region, Saudi Arabia. Hemoglobin. 2018;42(4):264–268. doi:10.1080/03630269.2018.1541802
19. Al Asoom LI, Al Hariri MT. The association of adiposity, physical fitness, vitamin D levels and haemodynamic parameters in young Saudi females. J Taibah Univ Med Sci. 2018;13(1):51–57.
20. Almakhaita MM, Al Asoom LI, Rafique N, Latif R, Alduhishy AM. Validity of maximal oxygen consumption prediction equations in young Saudi females. Saudi Med J. 2019;40(8):789–796. doi:10.15537/smj.2019.8.24332
21. Al Asoom LI, Alsuwat HS, Rafique N, et al. Functional DNA variations associated with Saudi female with low VO. Am J Transl Res. 2019;11(6):3659–3670.
22. Straub AC, Lohman AW, Billaud M, et al. Endothelial cell expression of haemoglobin α regulates nitric oxide signalling. Nature. 2012;491(7424):473–477. doi:10.1038/nature11626
23. Straub AC, Butcher JT, Billaud M, et al. Hemoglobin α/eNOS coupling at myoendothelial junctions is required for nitric oxide scavenging during vasoconstriction. Arterioscler Thromb Vasc Biol. 2014;34(12):2594–2600. doi:10.1161/ATVBAHA.114.303974
24. Bowie LJ, Reddy PL, Beck KR. Alpha thalassemia and its impact on other clinical conditions. Clinics in Laboratory Medicine. 1997;17(1):97–108. doi:10.1016/S0272-2712(18)30234-8
25. Reddy PL, Bowie LJ, Jiang H. Blood pressure changes after intravenous administration of cell-free hemoglobin A and hemoglobin H in the rat. Nitric Oxide. 2000;4(2):139–146. doi:10.1006/niox.2000.0279
26. Etyang AO, Khayeka‐Wandabwa C, Kapesa S, et al. Blood Pressure and Arterial Stiffness in Kenyan Adolescents With α + Thalassemia. J Am Heart Assoc. 2017;6(4):4. doi:10.1161/JAHA.117.005613
27. Liem RI, Chan C, Vu T-HT, et al. Association among sickle cell trait, fitness, and cardiovascular risk factors in CARDIA. Blood. 2017;129(6):723–728. doi:10.1182/blood-2016-07-727719
28. Marlin L, Connes P, Antoine-Jonville S, et al. Cardiorespiratory responses during three repeated incremental exercise tests in sickle cell trait carriers. Eur J Appl Physiol. 2008;102(2):181–187.
29. Bile A, Le Gallais D, Mercier B, et al. Blood lactate concentrations during incremental exercise in subjects with sickle cell trait. Med Sci Sports Exerc. 1998;30(5):649–654. doi:10.1097/00005768-199805000-00002
30. Freund H, Lonsdorfer J, Oyono-Enguéllé S, Lonsdorfer A, Dah C, Bogui P. Lactate exchange and removal abilities in sickle cell trait carriers during and after incremental exercise. Int J Sports Med. 1995;16(7):428–434. doi:10.1055/s-2007-973032
31. Sara F, Hardy-Dessources M-D, Voltaire B, Etienne-Julan M, Hue O. Lactic response in sickle cell trait carriers in comparison with subjects with normal hemoglobin. Clin J Sport Med. 2003;13(2):96–101. doi:10.1097/00042752-200303000-00006
32. Le Gallais D, Prefaut C, Mercier J, Bile A, Bogui P, Lonsdorfer J. Sickle cell trait as a limiting factor for high-level performance in a semi-marathon. Int J Sports Med. 1994;15(7):399–402. doi:10.1055/s-2007-1021077
33. Thiriet P, Le Hesran JY, Wouassi D, Bitanga E, Gozal D, Louis FJ. Sickle cell trait performance in a prolonged race at high altitude. Med Sci Sports Exerc. 1994;26(7):914–918. doi:10.1249/00005768-199407000-00017
34. Diaw M, Samb A, Diop S, et al. Effects of hydration and water deprivation on blood viscosity during a soccer game in sickle cell trait carriers. Br J Sports Med. 2014;48(4):326–331. doi:10.1136/bjsports-2012-091038
35. Connes P, Sara F, Hardy-Dessources M-D, et al. Effects of short supramaximal exercise on hemorheology in sickle cell trait carriers. Eur J Appl Physiol. 2006;97(2):143–150. doi:10.1007/s00421-006-0155-3
36. Awodu OA, Famodu AA. Haemostatic variables and their relationship to body mass index and blood pressure in adult Nigerians with the sickle cell trait. Clin Hemorheol Microcirc. 2007;36(1):89–94.
37. Etyang AO, Wandabwa CK, Kapesa S, et al. Blood Pressure and Arterial Stiffness in Kenyan Adolescents With the Sickle Cell Trait. Am J Epidemiol. 2018;187(2):199–205. doi:10.1093/aje/kwx232
38. Oliveira R, Barker AR, Debras F, O’Doherty A, Williams CA. Mechanisms of blood pressure control following acute exercise in adolescents: effects of exercise intensity on haemodynamics and baroreflex sensitivity. Exp Physiol. 2018;103(8):1056–1066. doi:10.1113/EP086999
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.