")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Effects of Nature-Based Intervention in Occupational Health Care on Stress – A Finnish Pilot Study Comparing Stress Evaluation Methods
Authors Lipponen M , Hallikainen V, Kilpeläinen P
Received 8 December 2021
Accepted for publication 28 February 2022
Published 29 March 2022 Volume 2022:15 Pages 577—593
DOI https://doi.org/10.2147/JMDH.S353168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Maija Lipponen,1 Ville Hallikainen,2 Pekka Kilpeläinen3
1Unit of Bioeconomy and Environment, Natural Resources Institute Finland, Paltamo, Finland; 2Unit of Natural Resources, Natural Resources Institute Finland, Rovaniemi, Finland; 3Unit of Measurement Technology, Kajaani University Consortium, University of Oulu, Kajaani, Finland
Correspondence: Maija Lipponen, Unit of Bioeconomy and Environment, Natural Resources Institute Finland, Manamansalontie 90, Paltamo, FI-88300, Finland, Tel +35 8295322024, Email [email protected]
Purpose: To assess methodology and its limitations for measuring effects of nature-based intervention (NBI).
Patients and Methods: Participants were 11 middle-aged female health care workers with lowered capacity to work. NBI included six group appointments in six months study period. Heart rate variability (HRV) and self-reported pain and work exhaustion were measured pre-post study period. Salivary α-amylase samples were collected immediately before and after three individual interventions. Salivary cortisol samples were collected on the same three interventions, on three consecutive days starting from the day of intervention, to assess (a) month effect (pre-post study period) and (b) day effect (intervention day vs non-intervention day).
Results: Individual interventions resulted in increase in α-amylase activity. However, the average fold increase decreased from the 3.05 ± 1.20 of the first intervention to 1.91 ± 1.00 and 1.46 ± 0.77 in the second and third intervention, respectively (p < 0.001). Cortisol concentrations were lower on intervention days vs non-intervention days, the difference being indicative (p = 0.050). Pain and work exhaustion decreased during the study period, as well as HRV, although any of these changes was not statistically significant.
Conclusion: For a large-scale study, it would be ideal to select assays for both major pathways: hypothalamic-pituitary-adrenal axis can be measured by cortisol, whereas response via autonomic nervous system can be measured by HRV, when roles of sympathetic and parasympathetic nervous systems can be pinpointed separately. Salivary α-amylase can be used when continuous monitoring is not possible. Psychological well-being of participants should be surveyed, as well as their activities and moods on sampling days recorded.
Keywords: salivary cortisol, salivary α-amylase, heart rate variability, pain, work exhaustion
Plain Language Summary
Nature has many favorable impacts on well-being. Nature-based programs create an interesting new way to support people’s social, physical and mental health. At occupational health care nature environments are not widely used so far. In this study we aimed to try out a simple program suitable for occupational health care, to test and compare methods for monitoring stress and to evaluate sources of interfering factors. We noticed that participants’ salivary cortisol levels got lower on intervention days compared to days without intervention. We also found that salivary α-amylase increased during the intervention, but the increase was lower every time in consecutive appointments. They both are well-known stress markers. Other measures were heart rate variability and two self-reported questionnaires to assess the impacts over the study period. There were slight changes in these indices, but the difference was not significant. Because of small sample size, lack of a control group and other limiting conditions, the results are only indicative, but they are supported by the feedback from participants and health care professionals who experienced NBI as a good tool to promote well-being at work and free time. For future studies there is a need for several stress monitoring methods to obtain reliable overview on the effects of nature-based health care methods.
Introduction
Stress and stress-related illnesses are globally recognized as risk factors impacting workers’ physical and mental health.1 At the same time the relationship between nature and human health and well-being is of current interest to a number of organizations within diverse sectors.2 A recent systematic review underlined the benefits of exposure to nature in all-cause mortality, mortality by cardiovascular diseases, and mental health among adult populations.3 Natural or forest environments improve physical parameters such as heart rate, blood pressure and stress-hormone cortisol levels,4 and mental health parameters such as satisfaction, passion, and absenteeism.5 Exercising in natural environments has greater physical and mental health benefits than exercising indoors.6 Mindfulness exercises have been observed to effectively promote health and well-being of employees in various occupational settings.7 A recent study showed that the mental health and wellbeing outcomes of mindfulness exercises are greater when carried out in a natural environment compared with built environments.8 Improvements were sustained even one month after completion of the intervention. Interestingly, one previous study reported that staying in the forest environment with cognitive-behavioral therapy program gives better results compared to staying in the same environment without any programs among patients with major depressive disorder.9 This emphasizes the meaning not only of the nature on wellbeing but also the professional guidance in the nature to improve well-being.
In literature a nature-based intervention is described as an activity or process aimed to engage people in natural settings such as parks, forests or watersides with the goal of improving health-related outcomes for persons across the lifespan.10 NBIs are usually intended to increase the level of exposure to the natural environment.11 They generate a multitude of health benefits along multiple pathways12 through a variety of potential mechanisms.13 Nature-based interventions are typically based on two main theories. Attention restoration theory (ART)14 and stress reduction theory (SRT)15 explain restoration as a core process, which is assumed to be triggered by spending time in nature. According to the ART natural stimuli attract spontaneous interest and enable restoration of directed attention, feeling of positive emotions and reduction of stress.16,17 According to the SRT, individuals automatically and immediately exhibit positive affect toward natural, green environments resulting in stress-reducing psycho-physiological responses. The preferences for natural settings are assumed to have an evolutionary base; people are to some extent biologically more adapted to natural than built environments.18
Experimental designs for studying NBI are rather scarce in organizational contexts19 and in research of nature-related sciences20 due to both difficulties to organize and high realization costs. A recent synthesis summarizes that a majority of experimental studies have been conducted among students in simulated work settings instead of real work settings.21 The synthesis indicated positive effects on mental health indices and cognitive ability, while mixed results were found for recovery and restoration, work and life satisfaction, and psycho-physiological indicators. There is overall high risk of bias in individual studies due to the diversity of NBIs. However, no negative side effects or specific contraindications of NBIs have been determined.22 Only serious illness or allergies that prevent employees from going outside need to be determined prior to implementation.
This study explored empirically stress-relieving outcomes of a NBI on female health care employees who had stress-related problems and lowered capacity to work. The study was a pilot having three aims: (a) to try out a simple NBI suitable for occupational health care for identifying good practices in organizing the program and finalizing the planning of the program for a larger study; (b) to test and compare methods for monitoring effects of intervention and variation associated to the methods; and (c) to evaluate sources of uncertainties and interfering factors such as changing routines of weekdays and to evaluate also need of a control group. The hypothesis was that the simple NBI protocols may have detectable effects only on some indicators, the significance of which is strongly dependent on the magnitude of variation in the monitoring data and on sensitivity of the monitoring method for interfering factors.
The two main pathways by which psychological stress affects the body are the hypothalamic-pituitary-adrenal (HPA) axis and autonomic nervous system (ANS).23 They are highly coordinated and interconnected.24 The ANS is regulating via noradrenergic system also alertness, vigilance and arousal, the right amounts of which are beneficial for attention capacity and thus may have role in the restoration of attention.25 Its activity is also quicker to react on a stimulus and return to the basic level after the stimulus.26 Therefore, both pathways were monitored, salivary cortisol was used as a measure of HPA axis function whereas salivary α-amylase levels and heart rate variability (HRV) were measured for the activity of ANS. Salivary α-amylase is regarded as a non-invasive peripheral marker of sympathetic nervous system and noradrenergic activity whereas HRV indicates balance between sympathetic and parasympathetic nervous systems.27 Since the concept of stress includes biological and psychological factors, physiological evaluations as well as self-reporting should be integrated to stress evaluation. In this study, two self-reporting questionnaires were used to assess work exhaustion and pain which both are stress-related and affect the individual’s ability to work.
Materials and Methods
Study Design
Participants
The inclusion criteria of study persons targeted a group of health care workers at a municipal health center unit who had stress-related problems and lowered capacity to work according to a previous work exhaustion survey and HRV measurements. They already had had individual and group appointments with a physical therapist and psychologist in occupational health care. There was no selection for a specific diagnosis. Participation in the NBI was voluntary. Participants were chosen if they were motivated to make small changes in their everyday life during the intervention. This was asked by a short questionnaire prepared by the occupational health care unit. There were 12 workers, nurses and administrators, all women, from 38 to 57 years old, enrolled in the NBI. All of them agreed to participate in the study. All participants signed written informed consent before entry into the study. One of them dropped out during the program. The study was performed in accordance with the principles stated in the Declaration of Helsinki. The study was approved by the Regional Ethical Committee in Oulu, Finland (37 /2019) and a local joint authority of social and health care in Kainuu, Finland (2299/13 001 00/2019).
Intervention
Study persons participated in the intervention including six group appointments in the afternoon following a regular working day. The intervention was aimed to support health care workers’ health and wellbeing at an occupational healthcare center in northern Finland. The intervention was implemented in a collaboration between an occupational physician, a physical therapist and an occupational psychologist. One aim of the intervention was to gain for participants knowledge and tools to manage the stress in everyday life and finding new routines for recovery. This is a process that takes time and for this, the program was designed to last six months, from May to October 2019.
The NBI included physical and mindfulness exercises in nature environment which included parks, forests and watersides. The vegetation in parks consisted of grass, plant flowers and trees, mainly birch, pine and spruce (Figure 1). Waterside environments were a river flowing through a small town and a natural pond in an urban park. Physical exercises led by a physical therapist were walking, climbing stairs outdoors and working on outdoor gym in urban park environment. Mental exercises led by a psychologist consisted of mindfulness exercises and other mental exercises (eg visiting a favorite place in a forest environment28,29).
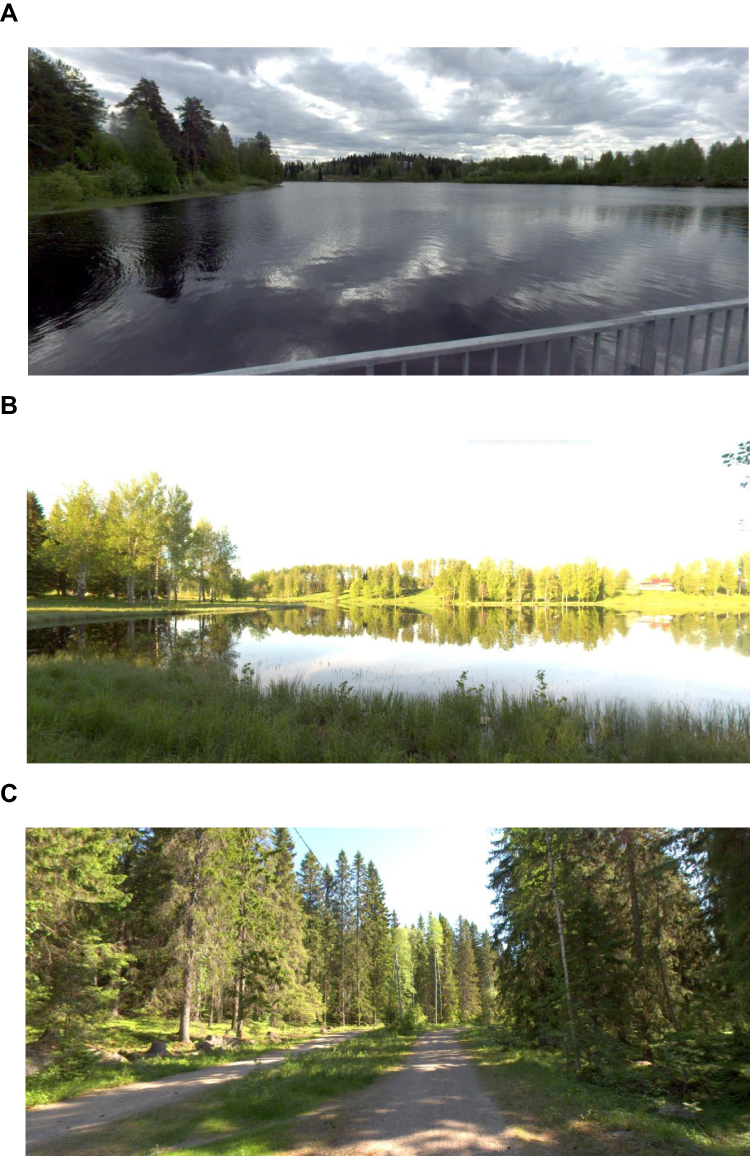 |
Figure 1 The mindfulness exercise on appointment 1 was held in a riverside environment (A), the conscious walking exercise on appointment 2 in a park next to a natural pond (B) and the favorite place exercise on appointment 6 in a recreational forest (C). |
Data Collection and Measurements
During the program the stress level of participants were followed by self-report questionnaires of pain and work exhaustion and physiological measurements of HRV, salivary cortisol and α-amylase (Figure 2). HRV was measured three days continuously in the beginning and at the end of the program to assess the (a) month effect (pre-post study period) and (b) day effect (intervention day vs non-intervention day). Cortisol and α-amylase were measured on different schedules to study two different phenomena; α-amylase reacts more sensitively to individual sessions while cortisol depicts more stable regulation over days. Therefore, α-amylase samples were collected immediately before and after the intervention at three individual interventions during the study period. Bedtime unstimulated saliva samples for cortisol analysis were collected at the same three interventions as α-amylase, three consecutive days at time, to assess (a) month effect (pre-post study period) and (b) day effect (intervention day vs non-intervention day). Besides comparison of intervention day vs non-intervention day, the interest was on the differences between the weekdays since the weekly rhythm affects stress and recovery. Self-reported questionnaires were filled on the first and last appointment to study pre-post study period effects.
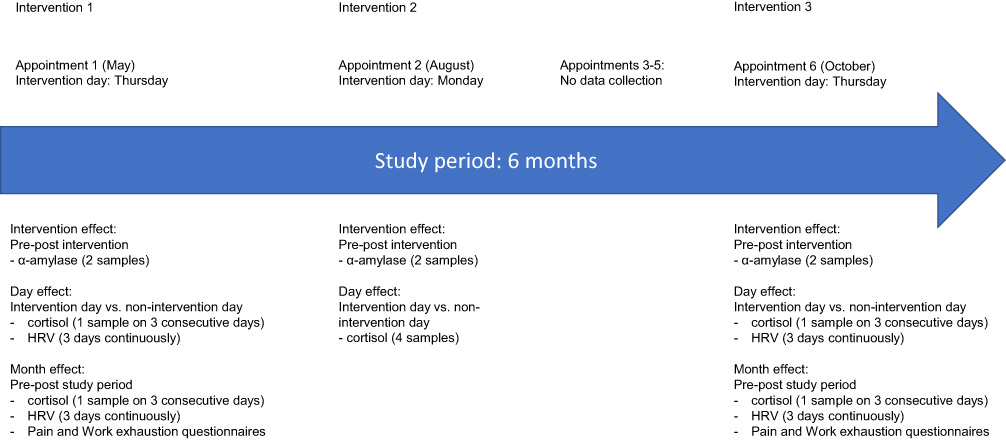 |
Figure 2 Study design of the NBI. |
On the first appointment in May (Thursday) the participants were given an introduction lecture about health and well-being benefits of exposure to natural environments (30 min) and instructions to give the saliva samples (15 min). First saliva samples for α-amylase analysis were collected (15 min). A mindfulness exercise (15 min) was done after a short walk (5 min) standing still on a riverside recreation area (Figure 1A) immediately near the water, followed immediately by a second saliva sample for α-amylase analysis (5 min). The subjects took the intervention day saliva sample for cortisol analysis on bedtime at home according to the instructions. Non-intervention day saliva samples were taken on the next two evenings (Fri-Sat) for cortisol analysis and HRV was measured from Thursday morning until Sunday morning continuously. A total of five saliva samples were taken per subject from which two samples were for α-amylase analysis and three samples for cortisol analysis.
On the second appointment in August (Monday) the participants were guided to walk calmly and independently with no significant physical exertion (30 min) on a nature-rich waterside environment consisting of a pond and urban forest park dominated by deciduous trees (Figure 1B). The saliva samples for α-amylase analysis were collected immediately before and after the walk and for cortisol analysis the participants took saliva sample at bedtime at home. Subjects took a bedtime saliva sample for cortisol analysis at home the following Thursday (non-intervention day), Friday and Saturday (non-intervention days). A total of six saliva samples were taken per subject from which two samples for α-amylase analysis and four samples for cortisol analysis. The third, fourth and fifth appointments were physical exercises outdoors (green exercise) and were not followed by measures.
The sixth appointment was held in October (Thursday). After a medium speed walk (15 min) in a recreational forest dominated of coniferous trees (Figure 1C) participants made an exercise in which they found and stayed at their favorite place (15 min) in the forest. There was no significant physical exertion during the exercise. The saliva samples for α-amylase analysis were collected immediately before and after the exercise. Subjects took a bedtime saliva sample for cortisol analysis at home. Non-intervention day saliva samples were taken on the next two evenings (Fri-Sat) for cortisol analysis. A total of five saliva samples were given per subject from which two samples for α-amylase analysis and three samples for cortisol analysis.
A total of six α-amylase samples and total of 10 cortisol samples were given per subject during the six months study period.
Salivary Cortisol and α-Amylase Analysis
Saliva was collected using SalivaBio Oral Swab (Salimetrics, State College, PA, USA) according to manufacturer’s instructions. For α-amylase assays, saliva was collected immediately (< 10 minutes) prior to and after interventions. For cortisol measurements, study subjects collected saliva at home in the evening at the same time (±1 h) each time. The subjects were instructed not to eat, drink or smoke 30 minutes before each evening samples, but to rinse their mouth with water 10 minutes prior to sample collection. All samples were kept at +4 °C until processed further in laboratory. Samples for α-amylase assay were processed in a following morning after the intervention. All samples collected from Thursday to Saturday evening for cortisol measurements were processed on Monday. A single series of samples collected on Monday were processed next day on Tuesday. Salivary cortisol is known to be stable at + 4 °C up to three months.30 In the laboratory, the swab containing saliva was centrifuged 1500 x g for 15 minutes in a collection tube (Salimetrics), saliva was aliquoted and frozen to −80°C until analysis.
On the day of analysis, samples were thawed and centrifuged 3500 x g for 10 min at room temperature. α-amylase was measured using commercial kinetic enzyme assay kit and duplicate samples as instructed by the kit provider (Cat No 1–1902, Salimetrics). Cortisol measurements were conducted using Shimadzu UHPLC liquid chromatograph Nexera X2 coupled to Shimadzu triple quadrupole mass spectrometer 8050 (Shimadzu, Kyoto, Japan) equipped with ESI ion source. Stock solutions of cortisol standard and internal standard were prepared to methanol. For quantification, seven dilutions between 0.1 and 25 ng/mL of hydrocortisone in 10% methanol were made. All samples were injected to LC-MSMS at least in triplicates, and despite of use of the internal standard, 20% of samples were analyzed also with duplicate pretreatment to control accuracy of the assay. The detailed UHPLC-MSMS method is described elsewhere.31
Salivary α-amylase activities were calculated from absorbance values of assays as instructed by the assay kit manufacturer, and the values of duplicate assays were averaged. The samples displaying RSD% > 10% were re-assayed. Salivary cortisol values were obtained from UHPLC-MS/MS data using standard curve and by averaging duplicate samples. When the RSD% of a sample was > 10%, additional sample injections to LC-MSMS were carried out or a pretreated duplicate was prepared and assayed.
Heart Rate Variability
HRV was measured three days continuously in the beginning and at the end of the program to assess the (a) month effect (pre-post study period) and (b) day effect (intervention day vs non-intervention day). HRV measurement was done by BodyGuard2 device (First Beat Technologies Ltd, Finland) fastened on the chest for three days on the same days as cortisol samples were collected (Thu-Sat). The device was taken off only for swimming, shower or sauna. First Beat technology is based on measuring consecutive heartbeats (R-R intervals). The square root of the mean squared differences of successive R-R intervals (RMSSD) represents the degree of parasympathetic nerve activity. Based on RMSSD values, length of sleep, recovery time per day and during sleep and amount of stress reactions per day as well as given study persons age, height, weight and possible medication and alcohol use, the program calculated scoring from 0 to 100 for (a) the sleep time recovery and (b) stress-recovery ratio.32 The value 0–29 is assumed to indicate low, 30–59 medium and 60–100 good recovery from stress according to the manufacturers data interpretation guidelines. Instead of daily mean RMSSD values, the scoring gives broader scope for the recovery rate of a study person.
Psychological Measures
Participants were asked to fill two self-reported questionnaires, the 15-item Bergen Burnout Indicator (BBI-15)33 and modified Örebro Musculoskeletal Pain Questionnaire34 on the first and last appointment (pre-post intervention). They both are standardized and validated questionnaires that had previously been used in similar research. The BBI-15 includes negative emotional (exhaustion), cognitive (cynicism), and behavioral (inadequacy) components of burnout. The BBI-15 total score is a sum of the three components and gives a quick overview to burnout level. It has been used to assess perceived stress at work and is widely used in occupational health care in Finland.
The pain questionnaire was based on the Örebro Musculoskeletal Pain Questionnaire and was modified by Occupational health Care of city of Helsinki. It measures pain experienced in everyday life identifying patients at risk of developing a persistent back problem. It evaluates duration of the current pain, absence from work, stress, mood and fear-avoidance beliefs all related to long-term pain problems.
Statistical Analysis and Modeling
Participants in this study represent a sample of population of Finnish middle-aged female health care workers. We analyzed the pre-test and post-test results of the questionnaires using a paired t-test.
In the statistical analysis (models) the response variables were 1) α-amylase, 2) cortisol, 3) HRVsleep and 4) HRVrecovery. The response variables were log-transformed in the modeling to normalize the distributions and achieve reasonable residuals. The parameter estimates and test in the Tables 1 and 2 and Supplementary Table 5 represents the values in the log-transformed scale. However, the estimates and the standard errors of estimates were returned to the original scale. The bias in the back-transformation was corrected by multiplying the predicted values by the ratio of observed and predicted mean.35
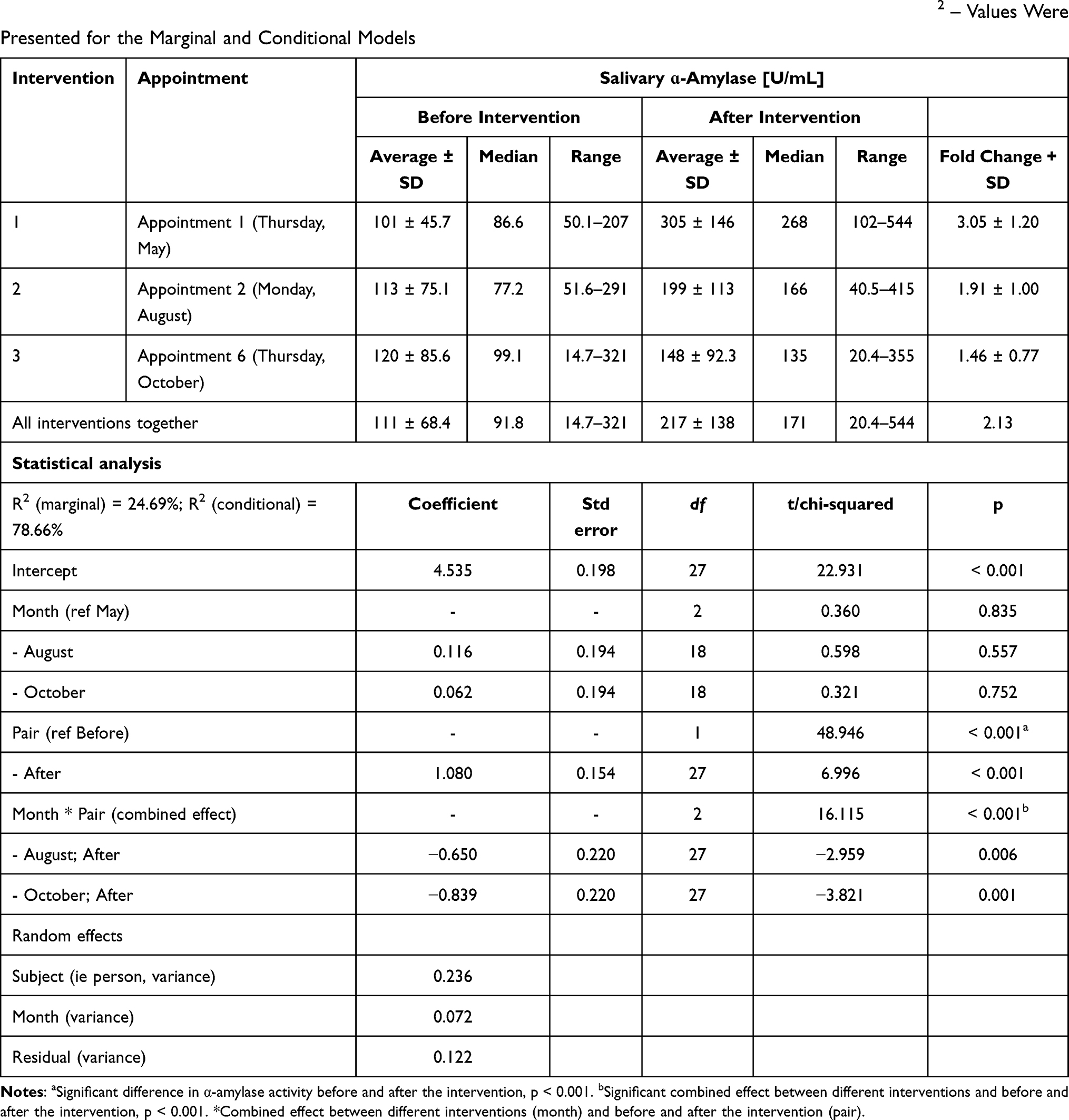 |
Table 1 Salivary α-Amylase Activities Before and After Nature-Based Interventions and Parameter Estimates and Tests of the General Linear Mixed Effects’ Model for α-Amylase. Std Err Denotes the Standard Error of the Estimates, t- and Chi-Squared Values are the Test Values for the Parameter Estimates or Type III Anova (Deviance) Tests, Df Denotes the Degrees of Freedom. R2 – Values Were Presented for the Marginal and Conditional Models |
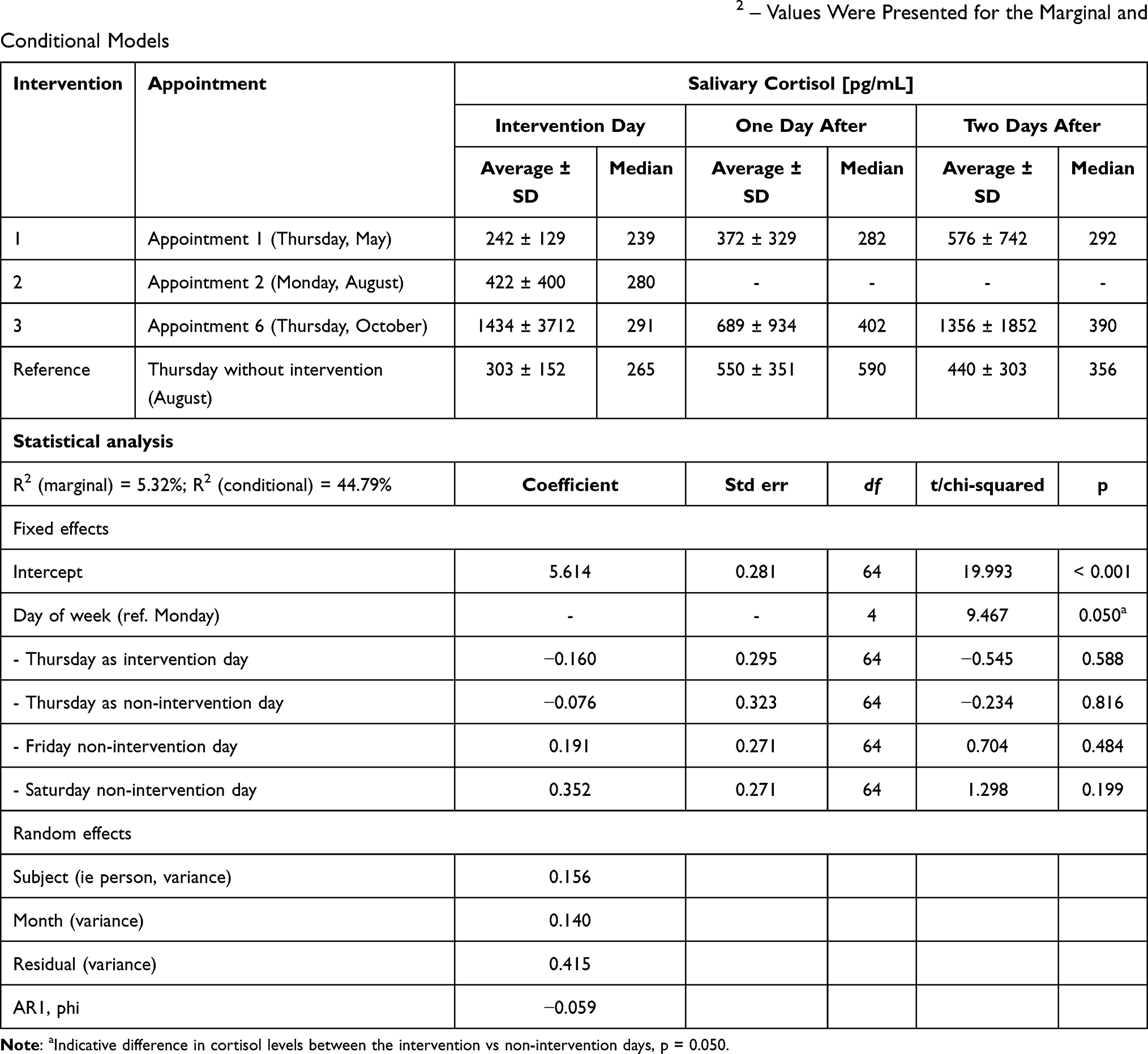 |
Table 2 Post Intervention Salivary Cortisol Levels and Parameter Estimates and Tests of the General Linear Mixed Effects’ Model for Cortisol. Std Err Denotes the Standard Error of the Estimates, t- and Chi-Squared Values are the Test Values for the Parameter Estimates or Type III Anova (Deviance) Tests, Df Denotes the Degrees of Freedom. R2 – Values Were Presented for the Marginal and Conditional Models |
Despite of the small data, we succeeded to build reasonable linear mixed effects models for the response variables in order to test the effects of (a) month (pre-post study period) and (b) the day of week (intervention day vs non-intervention day) and their interactions (a*b) to the response variables. These variables were treated as the fixed effects in the models. The fixed terms (variables and their interactions) in the final reported models were selected by taking all the terms in the model in the beginning of the modeling process and testing the significance of the terms by dropping the non-significant terms from the model one by one (backward selection). In addition, we computed the predictions of the models with their standard errors to illustrate the differences in the estimates.
A person was treated as a random subject in the models. Furthermore, month and day of week or measurement (before and after) nested within month were assumed to be nested within the subject (person). Thus, the models could be called as double repeated measure models, the first level representing the month and the second level the day of week or the measurement of before and after in the model for amylase.
If the day of week included more than two days (eg the measurements in Thursday, Friday and Saturday), the auto-regressive correlation structure (AR1) was used in the models for the lowest level observations (auto-regressive coefficient phi was estimated for the day of week), because it could be assumed that eg Thursday and Friday could be more strongly correlated than Thursday and Saturday. On the other hand, if there were only two measurements in the lowest level (measurements of before and after), the compound symmetry was assumed for the correlation structure. The correlation structure for months was assumed to be compound symmetry. This simplification was used to avoid too complicated model for the small data. In addition, the used statistical environment enabled the AR1-structure only for the lowest level observations.
The R statistical environment and its package nlme was used in the modeling. The nlme package estimated the parameter estimates and their significance values for the fixed effects, but only the parameter estimates for the random effects.36 The predictions for the parameter estimates were computed using R package effects.37,38 The coefficients of determination (R2) were computed using R package MuMIn.39
Results
The 11 of 12 enrollees continued until the end of the study with at least 11 subjects always involved in the interventions. One person discontinued and her results were excluded from statistical model. HRV was measured at least from 10 persons and saliva samples were collected from 11 persons each time.
Alpha-Amylase
Alpha-amylase activities were measured from saliva samples collected immediately (< 10 minutes) prior to and after interventions (Figure 2). The results and statistical model for α-amylase with the parameter estimates and tests are presented in Table 1 and Figure 3A and indicate that the interventions resulted in increase in α-amylase activity. The combined effect (Month * Pair) between different interventions and whether the sample was taken prior to or after the intervention on α-amylase activities was statistically significant, p value being < 0.001 (Table 1).
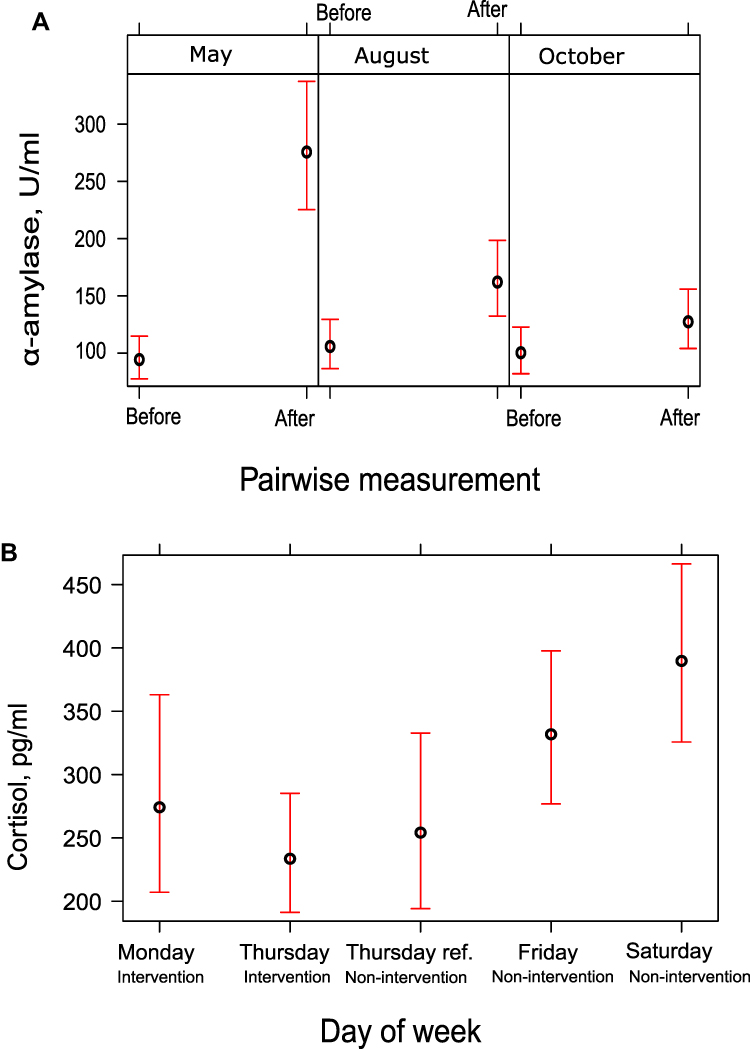 |
Figure 3 The predictions of the models for α-amylase (A) and cortisol (B). The explanatory variable in the cortisol model was day of week. In that model, Thursday was treated as an intervention day (Thursday) and a non-intervention reference day (Thursday ref.). Monday was an intervention day and Friday and Saturday non-intervention days. In the model for amylase, the predictions for the interaction effect of pairwise measurement (pre-post intervention) and month were presented. Point estimates (circles) and their standard errors were presented. |
However, the average fold increase decreased from the 3.05 ± 1.20 of the first intervention to 1.91 ± 1.00 and 1.46 ± 0.77 in the second and third intervention, respectively. The number of persons displaying increase of over 20% in α-amylase activity when values before and after interventions were compared were 10/10, 8/11 and 6/10. During the second and third intervention one of eleven and two of ten study persons showed decrease of over 20% in α-amylase activity (Supplementary Table 1). The α-amylase activities in all three interventions varied from 14.7 U/mL to 291 U/mL with an average of 111 ± 68.4 U/mL and median of 91.8 U/mL before the intervention, and from 20.4 U/mL to 544 U/mL with an average of 217 ± 138 U/mL and median of 171 U/mL after the intervention (Table 1). In each three interventions, the average α-amylase activities prior to interventions were rather equal: 101 ± 45.7, 113 ± 75.1 and 120 ± 85.6 U/mL, respectively, whereas in samples taken after the intervention the average of α-amylase activities decreased from the first to second and third intervention: 305 ± 146, 199 ± 133 and 148 ± 92.3 U/mL. Median activities behaved similarly: 86.6, 77.2 and 99.1 U/mL prior to and 268, 166 and 135 U/mL after interventions.
In the α-amylase activities of individual study persons (Supplementary Table 1), there are some interesting details. For example, basic α-amylase activity level appears to be personal. When 10 or 11 study persons in each intervention were arranged according to α-amylase activity prior to the intervention from highest to lowest, the largest difference in position of any person was 5 positions (Supplementary Table 2). The individual rather stable basic salivary α-amylase levels are an issue that has not been to our knowledge studied or reported previously, not at least in longer term study of 4–5 months. In particular, some of study persons had continuously high or very low α-amylase activities: 3 persons displayed prior to intervention in all sample collection times they participated (7 in total) enzyme activity that was amongst 4 highest in that intervention, and one study person had the lowest enzyme activity in 5 of 6 measurements, both prior and after the interventions (Supplementary Table 2). The magnitude of fold increase of α-amylase activity from prior to activity to the activity after the intervention varied more, but there were two persons who displayed in all three interventions fold increase that was amongst the three highest, and the person who had very low α -amylase activity had also in two interventions the lowest fold increase (the second of them actually < 1, ie enzyme activity decreased). The relative standard deviation (STD%) of all measured enzyme activities prior to and after interventions, respectively, were 61.6 and 63.9%, but the average STD% of enzyme activities of individual study persons were 37.2% and 46.5%, indicating that the higher variation of activities comes from differences between individuals, not from different effect of various intervention on an individual study person.
Cortisol
Altogether 10 saliva samples per study person were collected for cortisol assays (Figure 2) three of them on the evening of intervention (1 x Monday, 2 x Thursdays), and others on Thursday (1x), Friday (3x) and Saturday (3x) of the same week. The results and statistical model for cortisol with the parameter estimates and tests presented in Table 2 and Figure 3B indicate approximate differences in cortisol levels between the weekdays (intervention vs non-intervention days) (p = 0.050). The values varied from 61 pg/mL to 12617 pg/mL, average being 646 ± 1409 pg/mL and median 291 pg/mL (Table 2). Weekday averages and medians range from 422 ± 400 pg/mL (average) and 280 pg/mL (median) on Monday to an average 790 ± 1200 pg/mL on Saturday and a median 364 pg/mL on Friday. The individual cortisol values (Supplementary Table 3) indicate high variation between individual persons in basic cortisol levels and some single high peak values on stressful days. There were more high stress peaks on Saturdays compared to any other weekday, number of samples displaying cortisol level of > 1000 pg/mL was 7/33 on Saturday, 1/9 on Monday, 1/32 on Thursday and 4/32 on Friday.
Persons who had consistently high or low α-amylase activity did not have any consistent similarities in cortisol levels as a group. One of the study persons with high α-amylase activity displayed the lowest cortisol concentrations of the study, 6/10 measurements showed cortisol level below 100 pg/mL, when all other study persons in total had only one value below 100 pg/mL. Other two study persons with the high α-amylase activity had cortisol levels close to average, although they both displayed high cortisol peaks in some of the days (not on any day of interventions) and another of them displayed the highest single cortisol value of the study, 12617 pg/mL. The study person with exceptionally low α-amylase activity had either average or bit higher cortisol levels. This all indicates that a single result of high cortisol concentration or α-amylase activity does not demonstrate that the person is stressed. Instead, a comparison to personal basic level should be done, and values preferably monitored by several measurements and at least when it comes to cortisol, on consecutive days.
Heart Rate Variability
Heart rate variability was measured during the first (May) and last (October) intervention (pre-post study period) in three-day periods, on the same days as saliva samples were collected (Thu-Sat). Results for (a) the sleep time recovery scores HRVsleep and (b) stress-recovery ratio scores HRVrecovery are presented in Supplementary Table 4 and their statistical models in Supplementary Table 5.
The predictions for the day of week effect (intervention day vs non-intervention day) in (a) the sleep time recovery model HRVsleep were the following: Thursday (intervention) 33.08, Friday 34.85 (reference) and Saturday 44.31 (reference). The statistical predictions for the month effect (pre-post study period) in the (b) stress-recovery ratio model HRVrecovery were the following: May 47.81 and October 35.64. The differences between weekdays for HRVsleep or between months for HRVrecovery were not statistically significant (Supplementary Table 5).
Considering individual scores (Supplementary Table 4) the average of sleep time recovery was 44 ± 25, median 39 and range 12–100. Average of stress-recovery ratio was 42 ± 32, median 31 and range 3–100. (Supplementary Table 4). The individual HRV scores indicate high variation between individuals but also on the recovery of the same person at different days. Only 2/11 study persons showed good mean HRVrecovery (scores 60–100) and 3/11 good HRVsleep. in May and 2/11 and 2/11 in October, respectively. In May 4/11 showed low (0–29) HRVrecovery and 3/11 low HRVsleep. Other 5/11 showed medium (30–59) recovery.
When comparing to the cortisol values, study person I showed very high cortisol peaks but HRV indicated excellent recovery from stress. On the other hand, for example study person J showed cortisol values close to median levels but also good recovery according to HRV scores.
In May and October 5/11 and 5/10 persons (4 of them being the same individuals at both times), respectively, showed recovery during the intervention (results not shown). HRV does not correlate with α-amylase, however. For example, study person I had the highest α-amylase fold change factor (5.19) in May, but according to the HRV data, this person experienced recovery during the intervention. Whereas person H had the lowest α-amylase fold change factor (2.19) during the same measurement and he also showed recovery during the intervention according to HRV.
Psychological Measures
Psychological measures are represented in Supplementary Table 6. Pain questionnaire pre-test mean scores were 31 ± 14 and post-test 27 ± 20 (N = 7). The work exhaustion BBI-15 pre-test mean scores were 41 ± 15 and post-test 33 ± 10 (N = 8). There was decrease in both pain and work exhaustion, although not statistically significant.
Discussion
Previous studies applying NBIs to various age groups have shown a positive impact not only on physical health, but also on psychological health and social functioning.40,41 Research on specific physiologic benefits of NBIs through stress recovery exists but the mechanisms mediating effects are less known. The most studies have detected decreasing effect of nature settings on participants’ salivary cortisol levels.42 Salivary α-amylase is much less studied and depending on the type and physical strenuosity of the intervention, either increase or decrease of α-amylase during the intervention has been detected.43–45
In our study, salivary α-amylase was elevated immediately after each NBI, and there was slight but significant decrease in cortisol values on intervention days compared to other weekdays indicating different regulation of these stress markers. Moreover, during the six months study period there was no increase in HRV or decrease in cortisol but reductions in subjective pain and work exhaustion were identified even though any of these changes were not significant. This implies that physiological responses are separate from conscious psychological components. To increase the likelihood of detecting measurable changes in stress, an initiating, pre-exposure stressor may be needed in future studies.
The analysis of the outcome measures was unable to prove that NBI produced significant changes in physiological or psychological stress during the entire study period. This was not unexpected considering the small sample size and low statistical power of the study. The decrease, although not significant, in participants’ pain and work exhaustion indices suggests that NBI may offer new ways for participants to conserve resources to prevent burnout or pain-related disability to work. NBI may for example inspire to exercise more which can help managing pain caused by musculoskeletal diseases. These findings should be studied further to evaluate the usability of NBI in occupational health care.
Salivary cortisol values measured in this study are in agreement with recently published typical values of evening cortisol in saliva determined by LC/MSMS, namely 254 ± 145 pg/mL,46 that gives slightly lower values than immunoassays used in the most studies. The observed decreases in salivary cortisol on the intervention days were aligned with other studies where typically decreases of ~5% in cortisol levels have been observed in a variety of natural settings.42 A recent study of non-facilitated visits at sensory garden resulted in even greater (16% cf 5%) intervention effect on salivary cortisol.47 The presence of a statistically significant decrease in cortisol on intervention days versus non-intervention days, despite a low statistical power, does suggest potential contribution of NBI to the moderation of stress. In this pilot study, we wanted to look also at how different days of the week affect the results and how this should be taken into consideration in intervention studies. The weekly rhythm affected stress and recovery as expected. The inclusion of weekend days in this kind of study design may not be recommended since stress level as measured by salivary cortisol had more variation in weekend days than other weekdays.
Cortisol is the most common biomarker in stress studies. It can be measured for stress monitoring purposes in serum and plasma and reacts on both physiological and psychological stressors.48 Evening cortisol is a good marker for indicating stress load of the day, and how stressed a study person has been in general during few recent days. High day to day variation and variation between individual study persons means that the personal basic and control values must be known. More than one intervention per study person or a high number of study persons are needed to solve this problem. Also, personal control samples without interventions must be collected.
Salivary α-amylase is synthesized in acinar cells of the saliva glands and stored in secretory granules inside these cells until secretion is triggered by the sympathetic nervous system.26 Also its activity has variation between persons, and values should be compared to individual basic levels. The α-amylase values prior to the intervention matched well with the average (92.4 U/mL) and absolute range (3.1–423.1 U/mL) of activities reported by the kit manufacturer, and by other scientific studies49,50 for the enzyme activity in rest. As said, we detected significant increase in salivary α-amylase activity in all individual interventions. High intensity exercise is known to upregulate salivary α-amylase.51 Even walking in natural environment has been detected in two recent studies to increase α-amylase activity45 and this was explained by stating that physical activity connected to the NBI led to the upturn.
In a nature environment study44 during an 8-week study period, 36 urban dwellers were asked to spend time in an outdoor place that brings a sense of contact with nature, at least three times a week for a duration of 10 min or more. For salivary α-amylase, there was a 28.1%/h drop after adjusting for its diurnal rise of 3.5%/h, but only for participants that were least active sitting or sitting with some walking. In another similar study,45 salivary α-amylase increased in all tested environments from very build to very natural settings, though only the very built setting showed statistical significance for the within-group. The study noted that elevation in α-amylase indicates an activation of the neuro-endocrine mediated Sympatho-Adreno-Medullary (SAM, ~ noradrenergic) pathway during exposure to the very built setting and suggests that the participants were highly stressed in this location whereas in other environment increase in α-amylase may result only from physical activity.
However, in addition to stress response, sympathetic nervous system regulating secretion of salivary α-amylase is activated by a positive excitement and anticipatory enthusiasms.52,53 This effect has not been studied with α-amylase but is well known with electrodermal activity (increased galvanic skin response, skin conductance) that is also regulated by sympathetic nervous system.54,55 The excitement during the first appointment was likely the highest and could explain the highest fold increase of the first intervention. Alternatively, the fold change pattern may be explicated by the social strain caused by the group meetings. The physical stress of each intervention was light, and differences in physical stress of interventions may not explain differences in the fold increase.
Alpha-amylase is an excellent marker for monitoring stress and noradrenergic activity connected to a certain stimulus or situation, and immediate recovery from a stressful situation, but for the evaluation of this kind of interventions it may be too sensitive reacting on various stimulus and in particularly too time-dependent as a single assay, the peak values start to decrease in 10 minutes after a stress stimulus.48 When α-amylase assays are used to study impact of an intervention, more measurements during the day of intervention should be done to see the general stress level of the day before the intervention and after intervention to monitor whether the intervention supports relaxation and recovery from the working day stress in the evening. In addition, measuring concurrent emotional states could be helpful for interpreting results. Taking these limitations into account and when controlled appropriately, α-amylase may also offer an excellent tool to monitor noradrenergic stimulus to arousal and alertness, and thus potentially to attention capacity that could be measured by tests of its own after intervention.
When planning a NBI study, seasonal variation in stress marker levels may be one issue worth consideration. Cortisol levels increase in wintertime.56,57 In this study both mean and average cortisol levels were bit higher in October than in May and August, but the difference was not significant. The activity of sympathetic nervous system is higher in winter, and consequently eg heart rate and blood pressure are higher in winter.58,59 This may contribute to a slight increase of the α-amylase activity in the last intervention in October.
Heart rate variability (HRV) means the variation in time between consecutive heartbeats. It is universally accepted non-invasive marker of autonomic nervous system activity and is impacted by stress. The more variability there is between consecutive heartbeats (R-R interval), the better is one’s ability to achieve physiological balance between recovery and stress. Different HRV spectral components are associated with either the sympathetic or parasympathetic branches of the autonomic nervous system (ANS). For stress and recovery, HRV method provides absolute indices to express the strength of the reaction. The method evaluates the balance between stress and recovery by taking into consideration the strength of the reactions and duration of the states when producing an estimate.27
When measuring HRV over the study period, the same seasonable trend occurs as in cortisol. HRVrecovery was slightly higher in May than in October, which may be affected by the temperature and amount of daylight which are remarkably higher in May than October in Finland. When weekdays were compared, on intervention days cortisol levels were lower compared to non-intervention days, but the values were low also on reference Thursday when no intervention was carried out. In HRV measurements, the recovery from stress and the sleep quality got highest values on Saturday, which is a day off from work. On the other hand, cortisol levels, both average and median, increased for Saturday slightly. This is more a result of high single peak values than general increase in all levels (average increased more than median). The peak values may be brought about by heavy physical exercise or other physically strenuous activity such as cleaning typically done during weekends. HRV values were varying between individuals but also between the same person on different weekdays potentially reflecting how well previous night was slept. In recent literature, nature experience studies found statistically significant positive and negative effects or no effects on HRV, though measures varied and results were not consistent.43
When looking at individuals with continuously low cortisol levels (study person K, Supplementary Table 3), the HRV analysis showed poor or medium recovery (Supplementary Table 4). Prolonged exertion can lead to low cortisol production that does not respond normally to stimuli.60 When stressful situation lasts for a long time, cortisol values tend to drop down persistently. Low HRV scores of the study person supports this argument. Study person I showed very high cortisol peaks but HRV indicated excellent recovery from stress. On the other hand, for example study person J showed cortisol values close to median levels but also good recovery according to HRV scores. This indicates that peaks of cortisol might be caused by a single physical exertion, not always prolonged strain. Cortisol concentration may be high but if the parasympathetic nervous system is activated the person shows recovery by HRV.
There was no t-test pairwise correlation between any psychological and physiological variables. Two study persons with low pain scores at the end of the program had the highest cortisol levels and moderate HRVrecovery. One person showed severe work exhaustion scores at the end of program having rather high cortisol concentration which did not change significantly from the beginning. Even so, this person got maximum scores of HRVrecovery as the only study person in the first and the latter HRV measurement. One person with high pain scores and normal cortisol at the end, instead, showed very low HRVrecovery. Thus, any one of these measures alone may not describe reliably the work-related stress but several of them are needed to understand the physiological and psychological state of health of the individual.
Limitations of the Study
Although this study could identify intervention effects on measured parameters, there were several limitations. As mentioned, the small participant number of the study limited its statistical power, also control group was missing. Both limitations were due to budgetary and organizing constraints. Therefore, we wanted in this pilot study to analyse and describe individual level data to understand better the wide personal variation in results and factors effecting the variation. This must be taken into consideration when interpreting results. However, the computed models produced reasonable residuals and fit to the data. On the other hand, a bigger data would be needed to ensure the results and perhaps to find more significant effects.
In this study, a pre-test–post-test design was applied. This design is frequently used to assess the effectuality of forest recreation programs.61–63 The current study did not have a control group, however, which might degrade its internal validity. Adding a control group using indoor recreational activities (eg mindfulness program) may help to determine whether the reduced cortisol level was a result of NBI or simply a break from normal, more active day routines. Furthermore, a randomized, controlled trial could have been used to reduce bias. The results of this pilot study and detected variation can be used to evaluate required number of study persons for the larger study.
Study participants collected saliva samples for cortisol assays themselves at home. This created risk for errors in sample handling, for example exact times when study persons took their saliva samples was not controlled. They were advised to collect saliva at same time (±1 h) each time before going to bed. Neither did we control medication used that could have impacted hormone levels.64 For the study participants, holding the HRV device for several days can be annoying and there is a possibility of error in using the device. The calibration of device scores may also not be valid with all individual study persons. Self-report questionnaires measuring subjective experiences are the fastest and the most inexpensive way to gather data, but they run a risk of respondents answering subjectively and as they assume they are expected to answer.
Conducting an experimental field study includes the risk of exposure to extraneous variables making it in some cases impossible to empirically assess the validity of intervention. This variability cover both the normal diurnal variation and unforeseen outlier events eg unexpected stressful or exciting situations in each study persons’ personal life. The variables also fluctuate within and between appointments. Therefore, this kind of studies should typically include significantly more participants. The recruitment of participants from the local restricted geographic are in a mid-sized town in the Northern Finland also limits the generalizability of the study. The need for a large and diverse sample size rises from the diurnal rhythm of cortisol and α-amylase production which changes with age and stress level,45 socioeconomic factors,65 lifestyle factors such as sleeping patterns66 and weekdays as this study also suggests. The usefulness of α-amylase in this study was reduced by confounding effects of physical exertion and excitement in social situation. These effects must be taken into consideration through experimental design.
Conclusion
The purpose of this pilot study was to assess methodology and its limitations for measuring effects of nature-based intervention on unprovoked stress. The other goal was to determine how NBI works in practice at occupational health care. The decrease on participants’ cortisol levels detected in this study is supported by the feedback from the participants and the health care professionals who appreciated the NBI as a new method in promoting well-being at work and free time. The effects of NBIs in occupational health care should be addressed in future studies as well as their evaluation methods. NBI practices include diverse forms: sitting, walking, mental and physical exercises. While this indicates high applicability of NBIs, it also leaves them rather heterogeneous and difficult to compare. NBIs could benefit from more standardized practices to be more accepted as a reliable clinical approach. Accredited contents and consistent training for specialists are emerging.
Both common stress biomarkers, salivary α-amylase and cortisol, have high individual variation both in basic values and in response on stress stimulus. Therefore, the number of study persons in NBI has to be high enough, sampling times have to be constant in relation to intervention and there have to be several samples taken in particular for α-amylase assays to obtain personal reference values and to monitor time-dependent changes after intervention. For cortisol, personal reference values are needed from days without interventions. Weekends should be considered to differ from weekdays due to different routines.
Changes in HRV describe the balance between stress and recovery, but because the autonomic nervous system responds to both internal and external stimuli, many factors affect the heart rate intervals. For reliable assessment of psychological and physical well-being, other methods are preferably required alongside. Questionnaires can be used to screen situation of study persons at the beginning of the trial and to classify them to different groups, but they are not able to detect subtle changes, and in our opinion, they may not be reliable when re-used at the end of trials. The study persons have learnt the questionnaire and are also able to judge which kind of answers are expected from them.
As this study together with some previous showed different responses of two major stress response pathways, for a large-scale study, it would be ideal to select assays for both major pathways: hypothalamic-pituitary-adrenal axis can be measured by cortisol, whereas response via autonomic nervous system can be measured by HRV, when roles of sympathetic and parasympathetic nervous systems can be pinpointed separately. Salivary α-amylase can be used when continuous monitoring is not possible. Psychological well-being and situation of participants should be surveyed, and they should be asked to record their activities and moods on the days of sampling or measurements, as well as the most significant events on preceding days.
Acknowledgments
We gratefully acknowledge financial support of this study from the European Social Fund. The authors thank physical therapist Lenita Perhovaara, occupational psychologist Tuula Luhtaniemi and physician Päivi Cheney for all the advice and the practical implementation of the intervention. We express our gratitude to the informants who participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52(1):397–422. doi:10.1146/annurev.psych.52.1.397
2. Bowler DE, Buyung-Ali LM, Knight TM, Pullin AS. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health. 2010;10(1):456. doi:10.1186/1471-2458-10-456
3. van den Bosch M, Ode Sang Å. Urban natural environments as nature-based solutions for improved public health - A systematic review of reviews. Environ Res. 2017;158:373–384. doi:10.1016/j.envres.2017.05.040
4. Kuo M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front Psychol. 2015;6:1093. doi:10.3389/fpsyg.2015.01093
5. Bratman GN, Hamilton JP, Daily GC. The impacts of nature experience on human cognitive function and mental health. Ann N Y Acad Sci. 2012;1249(1):118–136. doi:10.1111/j.1749-6632.2011.06400.x
6. Thompson Coon J, Boddy K, Stein K, Whear R, Barton J, Depledge MH. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? a systematic review. Environ Sci Technol. 2011;2011(45):1761–1772. doi:10.1021/es102947t
7. Vonderlin R, Biermann M, Bohus M, Lysenko L. Mindfulness-based programs in the workplace: a meta-analysis of randomized controlled trials. Mindfulness. 2020;11:1–20. doi:10.1007/s12671-020-01328-3
8. Choe EY, Jorgensen A, Sheffield D. Does a natural environment enhance the effectiveness of Mindfulness-Based Stress Reduction (MBSR)? Examining the mental health and wellbeing, and nature connectedness benefits. Landsc Urban Plan. 2020:202.
9. Pálsdóttir AM, Sempik J, Bird W, van den Bosch M. Using nature as a treatment option. In: van den Bosch M, Bird W, editors. Oxford Textbook of Nature and Public Health. Oxford, UK: Oxford University Press; 2018:115–131.
10. Moeller C, King N, Burr V, Gibbs GR, Gomersall T. Nature-based interventions in institutional and organisational settings: a scoping review. Int J Environ Health Res. 2018;28(3):293–305. doi:10.1080/09603123.2018.1468425
11. Bloomfield D. What makes nature-based interventions for mental health successful? Bjpsych Int. 2017;14(4):82–85. doi:10.1192/S2056474000002063
12. Vujcic M, Tomicevic-Dubljevic J, Grbic M, Lecic-Tosevski D, Vukovic O, Toskovic O. Nature based solution for improving mental health and well-being in urban areas. Environ Res. 2017;158:385–392. doi:10.1016/j.envres.2017.06.030
13. Frumkin H, Bratman GN, Breslow SJ, et al. Nature contact and human health: a research agenda. Environ Health Perspect. 2017;125:075001.
14. Kaplan R, Kaplan S. The Experience of Nature: A Psychological Perspective. Cambridge: Cambridge University Press; 1989.
15. Ulrich RS. Natural versus urban scenes: some psychophysiological effects. Environ Behav. 1981;13(5):523–556. doi:10.1177/0013916581135001
16. Hartig T. Where best to take a booster break? Am J Prev Med. 2006;31(4):350. doi:10.1016/j.amepre.2006.06.003
17. Korpela K, De Bloom J, Kinnunen U. From restorative environments to restoration in work. Intelligent Build Int. 2015;7(4):215–223. doi:10.1080/17508975.2014.959461
18. Hartig T, Evans GW, Jamner LD, Davis DS, Gärling T. Tracking restoration in natural and urban field settings. J Environ Psychol. 2003;23(2):109–123. doi:10.1016/S0272-4944(02)00109-3
19. Nielsen K, Randall R, Albertsen K. Participants’ appraisals of process issues and the effects of stress management interventions. J Org Behav. 2007;28(6):793–810. doi:10.1002/job.450
20. Dunning T. Natural Experiments In The Social Sciences: A Design-Based Approach. (Strategies for Social Inquiry). Cambridge: Cambridge University Press. 2009:358.
21. Gritzka S, MacIntyre TE, Dörfel D, Baker-Blanc JL, Calogiuri G. The effects of workplace nature-based interventions on the mental health and well-being of employees: a systematic review. Front Psychiatry. 2020;28(11):323. doi:10.3389/fpsyt.2020.00323
22. Woo JM, Park SM, Lim SK, Kim W. Synergistic effect of forest environment and therapeutic program for the treatment of depression. J Korean for Soc. 2012;101:677–685.
23. Marques AH, Silverman MN, Sternberg EM. Evaluation of stress systems by applying noninvasive methodologies: measurements of neuroimmune biomarkers in the sweat, heart rate variability and salivary cortisol. Neuroimmunomodulation. 2010;17(3):205–208. doi:10.1159/000258725
24. Rotenberg S, McGrath JJ. Inter-relation between autonomic and HPA axis activity in children and adolescents. Biol Psychol. 2016;117:16–25. doi:10.1016/j.biopsycho.2016.01.015
25. Pajcin M, Banks S, White JM, et al. Decreased salivary alpha-amylase levels are associated with performance deficits during sleep loss. Psychoneuroendocrinology. 2017;78:131–141. doi:10.1016/j.psyneuen.2017.01.028
26. Kreibig SB. Autonomic nervous system activity in emotion: a review. Biol Psychol. 2010;84:394–421. doi:10.1016/j.biopsycho.2010.03.010
27. Rajendra Acharya U, Paul Joseph K, Kannathal N, Lim CM, Suri JS. Heart rate variability: a review. Med Biol Eng Comput. 2006;44(12):1031–1051. doi:10.1007/s11517-006-0119-0
28. Korpela K, Ylén M, Tyrväinen L, Silvennoinen H. Favorite green, waterside and urban environments, restorative experiences and perceived health in Finland. Health Promot Int. 2010;25(2):200–209. doi:10.1093/heapro/daq007
29. Korpela K, Ylén M. Effectiveness of favorite place prescriptions—a field experiment. Am J Prev Med. 2009;36:435–438. doi:10.1016/j.amepre.2009.01.022
30. Garde AH, Hansen AM. Long-term stability of salivary cortisol. Scand J Clin Lab Invest. 2005;65(5):433–436. doi:10.1080/00365510510025773
31. Kämäräinen S, Mäki M, Tolonen T, et al. Disposable electrochemical immunosensor for cortisol determination in human saliva. Talanta. 2018;188:50–57. doi:10.1016/j.talanta.2018.05.039
32. Firstbeat Technologies. Stress and Recovery Analysis Method Based on 24-Hour Heart Rate Variability. White paper by Firstbeat Technologies Ltd; 2014:134.
33. Salmela-Aro K, Rantanen J, Hyvönen K, Tilleman K, Feldt T. Bergen Burnout Inventory: reliability and validity among Finnish and Estonian managers. Int Arch Occup Environ Health. 2011;84(6):635–645. doi:10.1007/s00420-010-0594-3
34. Linton SJ, Boersma K. Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Orebro Musculoskeletal Pain Questionnaire. Clin J Pain. 2003;19(2):80–86. doi:10.1097/00002508-200303000-00002
35. Snowdon P. A ratio estimator for bias correction in logarithmic regressions. Can J for Res. 1991;21(5):720–724. doi:10.1139/x91-101
36. Pinheiro J, Bates D, DebRoy S, Sarkar D. Linear and nonlinear mixed effects models. R Package Version; 2019:97.
37. Fox J, Weisberg S. Visualizing fit and lack of fit in complex regression models with predictor effect plots and partial residuals. J Stat Softw. 2018;87(9):1–27. doi:10.18637/jss.v087.i09
38. Fox J, Weisberg S. An R Companion to Applied Regression. In: Thousand Oaks;
39. Bartoń K. MuMIn: multi-Model Inference. R Package Version; 2017.
40. Shin WS, Kim EI, Lee SI, Song SS, Kim JC. Forest health programs and their applications. J Korean Inst Recreation. 2001;5:37–44.
41. Song JH, Shin WS, Yeoun PS, Choi MD. The influence of forest therapeutic program on unmarried mothers’ depression and self-esteem. J Korean Soc. 2009;98:82–87.
42. Jones R, Tarter R, Miner Ross A. Greenspace interventions, stress and cortisol: a scoping review. Int J Environ Res Public Health. 2021;18(6):2802. doi:10.3390/ijerph18062802
43. Kondo MC, Jacoby SF, South EC. Does spending time outdoors reduce stress? A review of real-time stress response to outdoor environments. Health Place. 2018;51:136–150. doi:10.1016/j.healthplace.2018.03.001
44. Hunter MCR, Gillespie BW, Chen SY-P. Urban nature experiences reduce stress in the context of daily life based on salivary biomarkers. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.00010
45. Beil K, Hanes D. The influence of urban natural and built environments on physiological and psychological measures of stress–a pilot study. Int J Environ Res Public Health. 2013;10:1250–1267. doi:10.3390/ijerph10041250
46. Raff H, Phillips JM. Bedtime salivary cortisol and cortisone by LC-MS/MS in healthy adult subjects: evaluation of sampling time. J Endocr Soc. 2019. 2019(3):1631–1640.
47. Souter-Brown G, Hinckson E, Duncan S. Effects of a sensory garden on workplace wellbeing: a randomised control trial. Landsc Urban Plan. 2021;17:103997. doi:10.1016/j.landurbplan.2020.103997
48. Obayashi K. Salivary mental stress proteins. Clin Chim Acta. 2013;425:196–201. doi:10.1016/j.cca.2013.07.028
49. Perry GH, Dominy NJ, Claw KG, et al. Diet and the evolution of human amylase gene copy number variation. Nat Genet. 2007;10(10):1256–1260. doi:10.1038/ng2123
50. Fernández CI, Wiley AS. Rethinking the starch digestion hypothesis for AMY copy number variation in humans. Am J Phys Anthrop. 2017;163(4):645–657. doi:10.1002/ajpa.23237
51. Koibuchi ERI, Suzuki Y. Exercise upregulates salivary amylase in humans. A review. Exp Ther Med. 2014;7:773–777. doi:10.3892/etm.2014.1497
52. Petrakova L, Doering BK, Vits S, et al. Psychosocial stress increases salivary alpha-amylase activity independently from plasma noradrenaline levels. PLoS One. 2015;10(8):e0134561. doi:10.1371/journal.pone.0134561
53. Shiota MN, Neufeld SL. Yeung WH Moser SE, Perea, EF. Feeling good: autonomic nervous system responding in five positive emotions. Emotion. 2011;11:1368–1378. doi:10.1037/a0024278
54. Posada-Quintero HF, Chon KH. Innovations in electrodermal activity data collection and signal processing: a systematic review. Sensors. 2020;20(2):2479. doi:10.3390/s20020479
55. Ghiasi S, Greco A, Barbieri R, Pasquale Scilingo E, Valenza G. Assessing autonomic function from electrodermal activity and heart rate variability during cold-pressor test and emotional challenge. Sci Rep. 2020;10(1):5406. doi:10.1038/s41598-020-62225-2
56. Hadlow NC, Brown S, Wardrop R, Henley D. The effects of season, daylight saving and time of sunrise on serum cortisol in a large population. Chronobiol Int. 2014;31(2):243–251. doi:10.3109/07420528.2013.844162
57. Garay SM, Savory KA, Sumption LA, et al. Seasonal variation in salivary cortisol but not symptoms of depression and trait anxiety in pregnant women undergoing an elective caesarean section. Psychoneuroendocrinology. 2019;108:14–19. doi:10.1016/j.psyneuen.2019.05.029
58. Rosenthal T. Seasonal variations in blood pressure. Am J Geriatr Cardiol. 2004;13(5):267–272. doi:10.1111/j.1076-7460.2004.00060.x
59. Quer G, Gouda P, Galarnyk M, Topol EJ, Steinhubl SR. Inter- and intraindividual variability in daily resting heart rate and its associations with age, sex, sleep, BMI, and time of year: retrospective, longitudinal cohort study of 92,457 adults. PLoS One. 2020;15:e0227709. doi:10.1371/journal.pone.0227709
60. Hannibal KE, Bishop MD. Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys Ther. 2014;94(12):1816–1825. doi:10.2522/ptj.20130597
61. Zhou C, Yan L, Yu L, et al. Effect of short-term forest bathing in urban parks on perceived anxiety of young-adults: a pilot study in Guiyang, Southwest China. Chin Geogr Sci. 2018;28:1–12.
62. Chen HT, Yu CP, Lee HY. The effects of forest bathing on stress recovery: evidence from middle-aged females of Taiwan. Forests. 2018;9(7):403. doi:10.3390/f9070403
63. Takayama N, Saito K, Fujiwara A, Tsutsui S. Influence of five-day suburban forest stay on stress coping, resilience, and mood States. J Environ Inf Sci. 2018;03:49–57.
64. Strahler J, Skoluda N, Kappert MB, Nater UM. Simultaneous measurement of salivary cortisol and alpha-amylase: application and recommendations. Neurosci Biobehav Rev. 2017;83:657–677.
65. Karlamangla AS, Friedman EM, Seeman TE, Stawksi RS, Almeida DM. Daytime trajectories of cortisol: demographic and socioeconomic differences—findings from the National Study of Daily Experiences. Psychoneuroendocrinology. 2013;38(11):2585–2597. doi:10.1016/j.psyneuen.2013.06.010
66. Van Lenten SA, Doane LD. Examining multiple sleep behaviors and diurnal salivary cortisol and alpha-amylase: within- and between-person associations. Psychoneuroendocrinology. 2016;68:100–110. doi:10.1016/j.psyneuen.2016.02.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.