")
Back to Journals » International Journal of General Medicine » Volume 14
Effects of Modes and Timings of Delivery on Feto-Maternal Outcomes in Women with Severe Preeclampsia: A Multi-Center Survey in Mainland China
Received 24 August 2021
Accepted for publication 4 November 2021
Published 14 December 2021 Volume 2021:14 Pages 9681—9687
DOI https://doi.org/10.2147/IJGM.S335893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shao-Wen Wu, Wei-Yuan Zhang
Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Wei-Yuan Zhang
Department of Perinatal Medicine, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, People’s Republic of China
Email [email protected]
Background: Pregnancy termination is the only effective treatment for preeclampsia. However, there are controversies on the selection of modes of delivery. The objective was to evaluate whether mode of delivery in labor differentially affected the rate of adverse maternal outcomes related to severe preeclampsia.
Objective: This study aimed to evaluate whether the modes and timings of delivery affects adverse maternal outcomes in pre-eclampsia.
Methods: Clinical data from 2516 singleton pregnant women with severe preeclampsia were collected in a multicenter, large-sample, cross-sectional study in mainland China. The patients were divided into cesarean-delivery (CD) and vaginal-delivery (VD) categories and then into Group 1 (≤ 27+ 6 weeks), Group 2 (28– 33+ 6 weeks), Group 3 (34– 36+ 6 weeks), and Group 4 (≥ 37 weeks) according to the mode of delivery and gestational weeks. All data were exported into the SPSS software and analyzed by the Student’s t-tests or Mann–Whitney U-tests and the chi-squared test.
Results: A total of 2516 singleton pregnant women with severe preeclampsia were collected and the overall cesarean section rate was 84.9%. The vaginal delivery rates among the four groups were significantly different with 70%, 19.7%, 6.6%, 15.1% in groups 1, 2, 3, 4, respectively (P< 0.05), while perinatal mortality was lower in the CD groups than VD groups (3.3% vs 50.4%, P< 0.05). The neonatal asphyxia rate was significantly higher with CD than with VD in Group 2 (36.4% vs 12.9%, P< 0.05). The perinatal mortality with CD, 3, and 4 was significantly lower than with VD (10.0% vs 68.5% in Groups 2, 2.3% vs 28.3% in Groups 3, 0.8% vs 5.6% in Groups 4, all P< 0.05).
Conclusion: Most pregnant women with severe preeclampsia opted for a cesarean section in China. The lower perinatal mortality was associated with cesarean section, but the rate of maternal PPH or mortality was not related with the mode of delivery. So cesarean section is the safer delivery mode for the pregnant women complicated with severe preeclampsia.
Keywords: cesarean section, complications, mode of delivery, severe preeclampsia, vaginal delivery
Introduction
Preeclampsia is a disease specifically related to pregnancy, with a reported incidence of 3%; it greatly impairs both maternal and neonatal health.1 It is the largest contributor to adverse outcomes and complications including renal and liver failure, pulmonary edema, placental abruption, and eclampsia.2–4 These complications may occur in up to 30% of women with severe preeclampsia either before, during, or immediately after delivery.2,4,5
Although the etiology and progression of preeclampsia is not fully cleared, Silvia Fogacci reported that a call for action to definitively had addressed vitamin D supplementation as a possible intervention strategy in preventing preeclampsia in pregnancy.6 It is well accepted that delivery is the only definitive treatment.7,8 However, there are several opinions on the selection of delivery mode.9 On the one hand, vaginal delivery may be more favorable for the long-term prognosis of preterm babies and result in shorter hospitalization periods for pregnant women, but the induction may increase the possibility of Cesarean section due to the unfavorable cervix.10,11 On the other hand, pregnancy termination through Cesarean section increases the risk of hemorrhagic complications owing to the low tolerance for blood loss, thus increasing maternal complications afterwards.12 Therefore, no consensus has been obtained on the preferred delivery mode in pregnant women with severe preeclampsia.
The objective of this study was to evaluate whether the mode of delivery affected the rate of adverse maternal outcomes related to severe preeclampsia, such as the rate of postpartum hemorrhage or maternal death. A multicenter, large-sample, cross-sectional study in mainland China retrospectively analyzed the relations between the delivery modes and the maternal and neonatal outcomes to provide evidence for treating preeclampsia.
Materials and Methods
Ethics Approval
The study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of the Beijing Obstetrics and Gynecology Hospital, Capital Medical University. Informed written consent was obtained by all participants.
Data Collection
Questionnaire
The researchers developed the questionnaire from a chart review focused on medical records including maternal age, gravidity, parity, body mass index (BMI) before pregnancy, weight gain during pregnancy, pregnancy complications, gestational age, mode of delivery, newborn gender, birth weight, neonatal Apgar score, and rate of neonatal intensive care unit (NICU) admission.
Data Collection
From May 2012 to June 2012, the data was collected and entered into the computer network database, and data quality control was carried out at the same time. The data includes the delivery results of various hospitals in 2011.
Diagnostic Criteria
Preeclampsia was defined as the occurrence of hypertension (systolic blood pressure ≥ 140 mmHg and diastolic blood pressure ≥90 mmHg) for the first time after 20 weeks with significant proteinuria (>300mg/dl in 24 hours urine or dipstick measurement of +1 or) or in association with any biochemical or hematological abnormality.13 Postpartum haemorrhage (PPH) is defined as a blood loss >500 mL more of blood from the genital tract within 24 hours of the birth of a baby.14 Maternal deaths included those occurring during pregnancy or in the first 42 days postpartum.15 Fetal distress refers to the comprehensive symptoms that endanger the health and life of the fetus due to acute or chronic hypoxia in the uterus, which was mostly diagnosed when fetal tachycardia (fetal heart rate above 160 beats per minutes), fetal bradycardia (fetal rate below 100 beats per minutes), deceleration or lack of acceleration occurred.16 Neonatal asphyxia is a general term for neonatal encephalopathy resulting from events during labor, and delivery refers to fetal hypercarbia and hypoxemia and was diagnosed by the Apgar score in one minute less than seven and umbilical cord gas whose pH is less than 7.0 and/or BE≥12 mmol/L.17 Stillbirth and perinatal death were defined as delivery of a baby in the perinatal period, which failed to show any signs of life after 20 weeks of gestational age.18
Cesarean section refers to the incision of the abdominal and uterine wall to remove the fetus weighing more than 1000g and placenta after 28 weeks of pregnancy. Vaginal delivery is defined as the removal process of the fetal and placenta via vagina including operative vaginal delivery.
Data Analysis
The subjects were divided into a vaginal-delivery category (instrumental vaginal delivery, breech extraction, and assisted-breech delivery were included) and Cesarean-section category according to the mode of delivery. They were each further subdivided into four groups according to gestational age: ≤27 + 6 weeks, Group 1 (n = 70, 2.8% of the total); 28–33 + 6 weeks, Group 2 (n = 547, 21.7%); 34–36 + 6 weeks, Group 3 (n = 695, 27.7%); and ≥37 weeks, Group 4 (n = 1204, 47.8%).
All data were exported into the SPSS software from the database (v.22.0; SPSS Inc., Chicago, IL, USA) for statistical analysis. Continuous variables were shown with the mean ± SD or the median (and interquartile range). Baseline characteristics between the two groups were analyzed by the Student’s t-tests for variables with normal distribution after the Levene’s test and the Mann–Whitney U-tests for variables with skewed distributions. Categorical data were expressed by frequency (percentage) and the differences in frequency between the two groups were analyzed by the chi-squared test. P<0.05 was considered statistically significant in both unadjusted and adjusted analyses.
Results
The data were shown in Figure 1 by step-by-step description. The Demographic characteristics in preeclamptic women were shown in Table 1. Among the 2516 cases of pregnant women with severe preeclampsia, 380 cases delivered vaginally, accounting for 15.1% of the total; and 2136 cases were Cesarean deliveries, accounting for 84.9%. As shown in Figure 2, the vaginal birth rates among the four groups were significantly different (χ2 = 212.88, P = 0.000), of which Groups 1 and 2 were significantly higher than the other two groups (χ2 1–2 = 82.621, P = 0.000; χ2 1–3 = 234.892, P = 0.000; χ2 1–4 = 138.631, P = 0.000; χ2 2–3 = 48.547, P = 0.000; χ2 2–4 = 7.020, P = 0.008), while the vaginal delivery rate for Group 4 was significantly higher than that for Group 3 (χ2 3–4 = 27.773, P = 0.000).
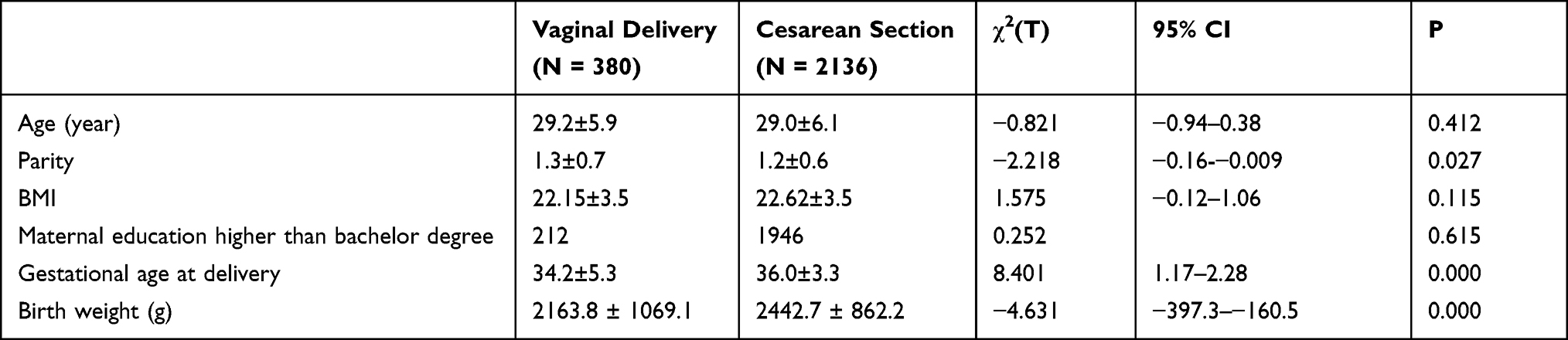 |
Table 1 Demographic Characteristics in Preeclamptic Women [(Mean, SD, (N, %)] |
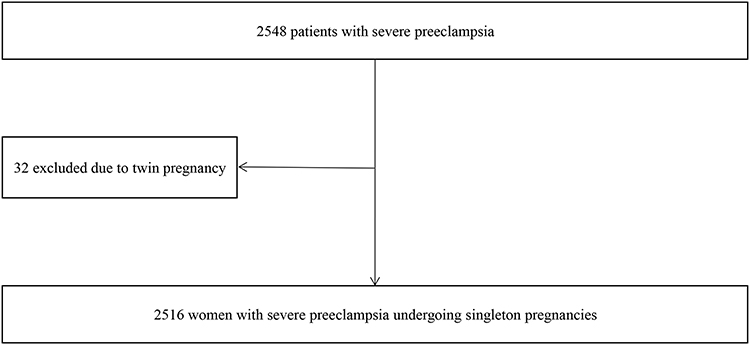 |
Figure 1 The step-by-step description of the analysis of data. |
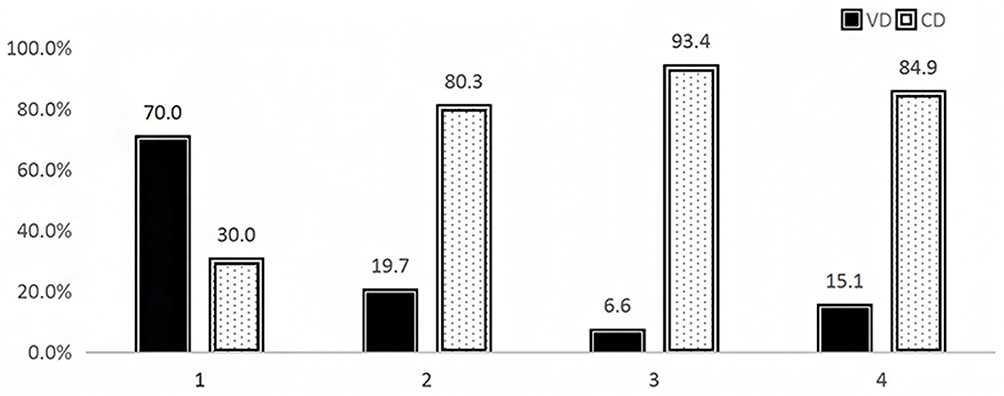 |
Figure 2 The delivery modes in the four groups (χ2 = 212.88, P = 0.000). Abbreviations: CD, cesarean-section delivery; VD, vaginal delivery. Notes: Group 1 (≤27+ 6 weeks), Group 2 (28–33+ 6 weeks), Group 3 (34–36+ 6 weeks), and Group 4 (≥37 weeks). |
Our results showed that the perinatal mortality for Cesarean section was significantly lower than that for vaginal delivery (χ2 = 684.1, P = 0.000), whereas the incidence of either fetal distress or neonatal asphyxia was not significantly different (Table 2). The maternal postpartum hemorrhage and death rates for different modes of delivery did not show statistical differences. The incidence of postpartum hemorrhage in different gestational age groups was also not significantly different (χ2 = 6.044, P = 0.110) (Table 3) but appeared to show a tendency to increase. Analysis of the effects of different modes of delivery for different gestational age groups (Groups 2, 3, and 4) showed no differences in the incidence of postpartum hemorrhage (P = 0.328, P = 1.000, and P = 0.277, respectively) (Figure 3).
 |
Table 2 Comparison of Maternal Complications in Different Groups [(Mean, SD, (N, %)] |
 |
Table 3 Comparison of Maternal Complications Among Different Groups [N, %] |
 |
Figure 3 Maternal complications of different delivery modes among the four groups [N, %]. Abbreviations: CD, cesarean-section delivery; VD, vaginal delivery; PPH, postpartum hemorrhage. Notes: Group 1 (≤27+ 6 weeks), Group 2 (28–33+ 6 weeks), Group 3 (34–36+ 6 weeks), and Group 4 (≥37 weeks). |
Analysis of the perinatal outcomes of different delivery modes in different gestational age groups found that the incidence of fetal distress with different delivery modes in each group was not significantly different. In Group 2, the neonatal asphyxia rate was significantly higher with Cesarean section than with vaginal delivery (P = 0.000). In Groups 2, 3, and 4, perinatal mortality was significantly lower with Cesarean section relative to vaginal delivery (all P = 0.000) (Table 4).
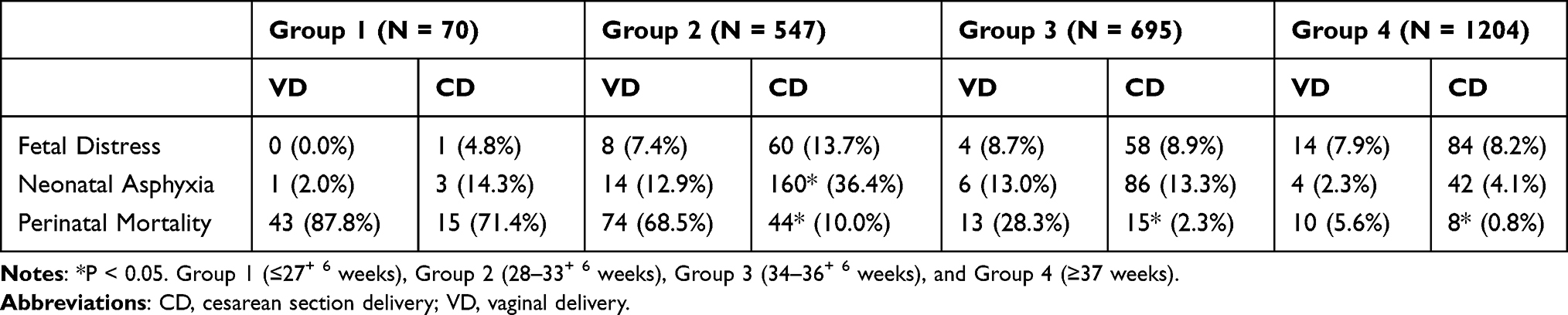 |
Table 4 Comparison of Perinatal Complications of Different Delivery Methods at Different Gestational Ages [N, %] |
Discussion
In the current study, we found that most pregnant women with severe preeclampsia terminated pregnancy by Cesarean section in mainland China, and the lower perinatal mortality was associated with Cesarean section but the rate maternal PPH and mortality were not related to the mode of delivery in severe preeclampsia. The reported Cesarean section rate currently varies widely. The majority of clinical reports shows a preference for Cesarean section for pregnancy termination, and the Cesarean section rate is therefore significantly higher than the rate of vaginal delivery.19 This study also confirmed that the Cesarean section rate in severe preeclampsia is as high as 84.9%, consistent with previous reports.20,21 Kim et al conducted a retrospective study of 3505 cases of women undergoing singleton pregnancies at over 24 weeks of gestation who were diagnosed with preeclampsia, and their data show that, regardless of maternal age or parity, or whether the fetus was full-term or not, the Cesarean section rate was still higher in pregnant women with preeclampsia than in those without.22 Still, many investigators recommend induction of labor for pregnant women with preeclampsia.23,24 Researchers have confirmed that, for preeclamptic patients, the failure rate of labor induction increased more than four-fold, and the Cesarean section rate increased more than two-fold.25 Patients with severe preeclampsia are already in critical condition, and Cesarean section is always performed to save the life of the patient; therefore, Cesarean section does not reduce maternal mortality rate. In the current study, we report that the incidence of postpartum hemorrhage is similar for pregnant women with severe preeclampsia and for those who used different modes of delivery, which is at variance with other reports.20 Potential reasons for this include the fact that, in most of the pregnant women with preeclampsia, epidural anesthesia was used, and active blood pressure control measures were administered during the Cesarean section, so the blood loss is less than normal pregnancy; thus, the risk of postpartum hemorrhage was reduced.26 Due to the specific hemodynamic factors associated with preeclampsia, blood exhibits a concentrated state, and the resulting hypertension increases the risk of cerebral hemorrhage and other cardiovascular diseases, and neonatal risks such as placental abruption also increase. All of these factors, then, need to be considered for the time period encompassing the second stage of labor. Thus, when pregnant women with severe preeclampsia fail to respond to initial therapy, clinicians tend to consider shortening the second stage of labor by using instrumental vaginal delivery or episiotomy, thus causing excessive bleeding during vaginal delivery.27 For pregnant women with severe preeclampsia, vaginal delivery may be attempted upon full assessment of the maternal and neonatal conditions, and complications should be closely monitored during the process; the pregnancy should then be terminated by emergent Cesarean section once maternal or neonatal health is found to be endangered.
Our study shows that lower perinatal mortality was associated with Cesarean section in patients with severe preeclampsia after 28 weeks of gestational age. Due to the pathophysiologic changes in preeclampsia, vascular spasms can lead to decreased placental perfusion, and, thus, a lengthy vaginal delivery may intensify fetal hypoxia. Cesarean section can instead deliver the baby rapidly and remove it from the adverse intrauterine environment as soon as possible. English et al reported that, for severe preeclampsia before 32 weeks, Cesarean section should be the preferred mode of delivery, and vaginal delivery should be attempted for patients over 34 weeks.28 Chen et al retrospectively analyzed the delivery methods and pregnancy outcomes of low-birth-weight children in the Chinese mainland, and found that stillbirth and neonatal mortality rates of children designated as having low birth weight were significantly lower with Cesarean delivery than with vaginal delivery (0.5% vs 5.2%; 1.0% vs 6.9%, respectively).29 Reddy et al retrospectively studied 4352 preterm neonates at gestational ages 24 to 31+ weeks, and found that, for preterm head-first pregnancies at a gestation age of 28–31+6 weeks, the perinatal mortality rate was significantly higher with elective vaginal delivery than with Caesarean section (6.0% vs 1.5%, respectively).30 The possible cause for this may be that, during the process of vaginal delivery, increased uterine contractions cause reduced uterine blood flow, which, in turn, increases the possibility of fetal hypoxia and low-birth-weight babies. This is especially true for those severely preeclamptic mothers whose fetuses present with growth restriction and low birth weight due to placental vascular spasm. Cesarean section can instead avoid the escalating neonatal hypoxia caused by vaginal delivery and may preclude possible neonatal intracranial hemorrhage and infection caused by vaginal delivery.
In conclusion, for pregnancy termination in pregnant women with severe preeclampsia, the mode of delivery should be chosen after full assessment of the maternal and neonatal outcomes, and Cesarean section should be performed in cases of emergency or when short-term vaginal delivery is impossible.
This study still has some deficiencies. For example, the data is from the survey ten years ago. With the progress of neonatal rescue technology, the choice of delivery mode may be more individualized. Especially, pregnant women with preeclampsia before 28 weeks may choose to actively rescue newborns. Due to regional differences, the medical level is different in different regions, which may affect the prognosis of pregnant women and newborns. In addition, this study is only a retrospective study, and a randomized controlled study is needed to evaluate the impact of delivery methods on maternal and infant outcomes of preeclampsia.
In summary, Most pregnancies among women with severe preeclampsia were terminated by Cesarean section in China. The lower perinatal mortality was associated with Cesarean section, but the rate of maternal PPH and mortality were not related with the mode of delivery in severe preeclampsia. We suggest the cesarean section is more suitable for the preeclampsia pregnant women for better neonatal outcome.
Acknowledgments
This study was supported by the Special Research Fund in Non-profit Health Care Industry of the People’s Republic of China (grant No. 201002013 to WYZ) and funded by Chinese Ministry of Health research funding specialized for public welfare and National Key R & D Program of China (2016YFC1000403). Thanks Liying Zou, Yi Chen and Yan Ruan in Beijing Obstetrics and Gynecology Hospital, Capital Medical University for collecting data and the questionnaire.
Disclosure
None of the authors have any conflicts of interest with regards to this work.
References
1. Lo JO, Mission JF, Caughey AB. Hypertensive disease of pregnancy and maternal mortality. Curr Opin Obstet Gynecol. 2013;25(2):124–132. doi:10.1097/GCO.0b013e32835e0ef5
2. Gifford RW, August PA, Cunningham FG, et al. Report of the national high blood pressure education program working group on high blood pressure in pregnancy. Am J Obstet Gynecol. 2000;183(1):S1–S22. doi:10.1067/mob.2000.107928
3. American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy: report from the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131. doi:10.1097/01.AOG.0000437382.03963.88
4. Mol BWJ, Roberts CT, Thangaratinam S, Magee LA, de Groot CJM, Hofmeyr GJ. Pre-eclampsia. Lancet. 2016;387(10022):999–1011. doi:10.1016/S0140-6736(15)00070-7
5. Douglas KA, Redman CW. Eclampsia in the United Kingdom. BMJ. 1994;309(6966):1395–1400. doi:10.1136/bmj.309.6966.1395
6. Fogacci S, Fogacci F, Banach M, et al; Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) Group. Vitamin D supplementation and incident preeclampsia: a systematic review and meta-analysis of randomized clinical trials. Clin Nutr. 2020;39(6):1742–1752. doi:10.1016/j.clnu.2019.08.015
7. Amorim MMR, Souza ASR, Noronha Neto C. Planned cesarean section versus planned vaginal delivery for severe preeclampsia. Cochrane Database Syst Rev. 2011;11:CD009430.
8. Roberts JM, Funai EF. Chapter 35: pregnancy-related hypertension. In: Creasy RK, Resnik R, Iams JD, Lockwood CJ, Moore TJ, editors. Creasy & Resnik’s Maternal Fetal Medicine: Principles and Practice. Vol. 6. Philadelphia, PA: Saunders; 668; 2009.
9. Noronha Neto C, Souza ASR, Amorim MMR. Tratamento da pre-eclampsia baseado em evideˆncIas [Evidence-based treatment of preeclampsia]. Rev Bras Ginecol Obstet. 2010;32:459–468.
10. Alanis MC, Robinson CJ, Hulsey TC, Ebeling M, Johnson DD. Early-onset severe preeclampsia: induction of labour vs elective Caesarean delivery and neonatal outcomes. Am J Obstet Gynecol. 2008;199:
11. Drife J. Mode of delivery in the early preterm infant (<28 weeks). BJOG. 2006;113:S81–5.
12. Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity In the United States. Obstet Gynecol. 2009;113:1299–1306. doi:10.1097/AOG.0b013e3181a45b25
13. ACOG technical bulletin. Hypertension in pregnancy. Number 219–January 1996 (replaces no. 91, February 1986). Committee on technical bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 1996;53(2):175–183.
14. WHO Guidelines Approved by the Guidelines Review Committee. WHO Guidelines for the Management of Postpartum Haemorrhage and Retained Placenta. Geneva: World Health Organization; 2009.
15. Clark SL. Strategies for reducing maternal mortality. Semin Perinatol. 2012;36(1):42–47. doi:10.1053/j.semperi.2011.09.009
16. Gray Cunningham F, eds. Williams OBSTETRICS.
17. Executive summary: neonatal encephalopathy and neurologic outcome, second edition. Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy. Obstet Gynecol. 2014;123(4):896–901. doi:10.1097/01.AOG.0000445580.65983.d2
18. Smith GC, Fretts RC. Stillbirth. Lancet. 2007;370(9600):1715–1725. doi:10.1016/S0140-6736(07)61723-1
19. Pacher J, Brix E, Lehner R. The mode of delivery in patients with preeclampsia at term subject to elective or emergency Cesarean section. Arch Gynecol Obstet. 2014;289(2):263–267. doi:10.1007/s00404-013-2936-3
20. Amorim MM, Katz L, Barros AS, Almeida TS, Souza AS, Faúndes A. Maternal outcomes according to mode of delivery in women with severe preeclampsia: a cohort study. J Matern Fetal Neonatal Med. 2015;28(6):654–660. doi:10.3109/14767058.2014.928689
21. Zhang Y, Li W, Xiao J, Chen S. The complication and mode of delivery in Chinese women with severe preeclampsia: a retrospective study. Hypertens Pregnancy. 2014;33(3):283–290. doi:10.3109/10641955.2013.874440
22. Kim LH, Cheng YW, Delaney S, Jelin AC, Caughey AB. Is preeclampsia associated with an increased risk of Cesarean delivery if labor is induced? J Matern Fetal Neonatal Med. 2010;23(5):383–388. doi:10.3109/14767050903168432
23. Ben-Haroush A, Yogev Y, Glickman H, Kaplan B, Hod M, Bar J. Mode of delivery in pregnant women with hypertensive disorders and unfavorable cervix following induction of labor with vaginal application of prostaglandin E. Acta Obstet Gynecol Scand. 2005;7:665–671.
24. Coppage KH, Polzin WJ. Severe preeclampsia and delivery outcomes: is immediate cesarean delivery beneficial? Am J Obstet Gynecol. 2002;186(5):921–923. doi:10.1067/mob.2002.124041
25. Xenakis EM, Piper JM, Field N, Conway D, Langer O. Preeclampsia: is induction of labor more successful? Obstet Gynecol. 1997;89(4):600–603. doi:10.1016/S0029-7844(97)00043-4
26. Lambert G, Brichant JF, Hartstein G, Bonhomme V, Dewandre PY. Preeclampsia: an update. Acta Anaesthesiol Belg. 2014;65(4):137–149.
27. Hypertension in Pregnancy: The Management of Hypertensive Disorders During Pregnancy. NICE Clinical Guidelines, No. 107.National Collaborating Centre for Women’s and Children’s Health (UK). London: RCOG Press; 2010.
28. English FA, Kenny LC, McCarthy FP. Risk factors and effective management of preeclampsia. Integr Blood Press Control. 2015;8:7–12. doi:10.2147/IBPC.S50641
29. Chen Y, Wu L, Zhang W, Zou L, Li G, Fan L. Delivery modes and pregnancy outcomes of low birth weight infants in China. J Perinatol. 2016;36(1):41–46. doi:10.1038/jp.2015.137
30. Reddy UM, Zhang J, Sun L, Chen Z, Raju TN, Laughon SK. Neonatal mortality by attempted route of delivery in early preterm birth. Am J Obstet Gynecol. 2012;207(2):
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.