")
Back to Journals » Journal of Pain Research » Volume 15
Effects of Lidocaine on Motor-Evoked Potentials and Somatosensory-Evoked Potentials in Patients Undergoing Intraspinal Tumour Resection: Study Protocol for a Prospective Randomized Controlled Trial
Authors Yue H, Zhou M , Chong Y, Cheng M , Qiao H, Lu Y, Cui W
Received 19 October 2021
Accepted for publication 13 January 2022
Published 2 February 2022 Volume 2022:15 Pages 287—297
DOI https://doi.org/10.2147/JPR.S345091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Hongli Yue,1,* Man Zhou,2,* Yingzi Chong,1 Miao Cheng,1 Hui Qiao,3 Yu Lu,1 Weihua Cui1
1Department of Anesthesiology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 3Department of Neurophysiology, Beijing Neurosurgical Institute, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Lu; Weihua Cui
Department of Anesthesiology, Beijing Tian Tan Hospital, Capital Medical University, No. 119, Nan Si Huan Xi Lu, Fengtai District, Beijing, 100070, People’s Republic of China
, Tel +8613661067447
; +8613651315600
, Fax +861059976658
, Email [email protected]; [email protected]
Purpose: At present, it is believed that intravenous (IV) infusion of lidocaine can inhibit hyperalgesia, relieve postoperative acute and chronic pain, and accelerate the rehabilitation of patients. However, studies of its effects on necessary electrophysiological monitoring during neurosurgery are few, and the results are controversial. This study assumes that the propofol-remifentanil based anaesthesia combined with lidocaine in patients undergoing intraspinal tumour resection will not have adverse effects on motor-evoked potentials (MEPs) or somatosensory-evoked potentials (SEPs).
Study Design and Methods: This is a prospective, randomized, placebo-controlled double-blind trial. A total of 96 patients undergoing intraspinal tumour resection will be randomly allocated to lidocaine and placebo group. The lidocaine group will receive IV lidocaine during anaesthesia, while the placebo group will receive the same dose of normal saline with the same infusion rate and infusion time, and the anaesthesia procedures of the two groups will be the same. All patients will be monitored the MEPs and SEPs of all four limbs during operation. The primary outcome will be the MEP amplitudes of both upper limbs at the end of operation. The secondary outcome measures will be the other electrophysiological parameters at the end of operation, the incidence of alert events for all four limbs, and the incidence of false positive events.
Discussion: The purpose of this study is to evaluate the effects of IV infusion of lidocaine on SEPs and MEPs during intraspinal tumour resection to determine whether electrophysiological monitoring can accurately reflect the integrity of nerve functions while infusing lidocaine and to explore the possibility of lidocaine use during intraspinal tumour resection as an anaesthesia option.
Keywords: motor-evoked potentials, somatosensory-evoked potentials, intraspinal tumour resection, lidocaine
Background
The spinal cord has complex structure and contains various neural pathways that are responsible for the sensory conduction and motor control of the body and viscera. The most important goal of intraspinal tumour resection is to maximally preserve the integrity of the nerve conduction pathway during the resection.1 In recent years, with the development of electrophysiological monitoring technology, motor-evoked potentials (MEPs) and somatosensory-evoked potentials (SEPs) have been widely used during intraspinal tumour resection to help surgeons to remove lesions to the greatest possible extent while minimizing nerve injuries and protecting spinal cord functions.2 The essential factors and difficulties of anaesthesia management during intraspinal tumour resection include providing satisfactory anaesthesia and avoiding the effects of anaesthetics on electrophysiological monitoring as much as possible.
Currently, total intravenous (IV) anaesthesia with the continuous infusion of propofol and remifentanil is clinically recommended. However, the continuous infusion of large doses of remifentanil can easily cause postoperative hyperalgesia, aggravate postoperative pain, increase the postoperative demand for opioids, and cause postoperative respiratory depression, delayed recovery, gastrointestinal dysfunction, and other side effects.3,4 In recent years, with the increasing adoption of the enhanced recovery after surgery (ERAS) concept, anaesthesiologists are committed to reducing opioid dosages, lowering the incidence of perioperative complications, and promoting patients’ rapid recovery by optimizing all aspects of perioperative anaesthesia and analgesia.
Lidocaine, a multipurpose anaesthetic, has been used for local anaesthesia, nerve blocks, intrathecal anaesthesia, general anaesthesia, and ventricular arrhythmia for a long time. In recent years, increasing numbers of studies have found that perioperative IV infusion of lidocaine can reduce the dosage of opioids, inhibit hyperalgesia, relieve postoperative acute or chronic pain, alleviate postoperative nausea and vomiting, and shorten the duration of intestinal paralysis, thus accelerating patients’ recovery and reducing postoperative cognitive dysfunction.5–7 According to the published research results for the combined infusion of lidocaine in other types of surgeries, it is expected that perioperative combined infusion of lidocaine could effectively prevent hyperalgesia caused by large doses of remifentanil, neuropathic pain cause by the disease itself, and pain induced by intraoperative tissue injuries, thereby better controlling postoperative acute and chronic pain, reducing the total dose of opioids, reducing the side effects caused by extensive use of opioids, and leading to positive effects for patients’ rehabilitation.
However, the effects of lidocaine on intraoperative electrophysiological monitoring are still inconclusive. One case report showed that the SEP amplitudes in the lower limbs decreased by 50% and the latencies increased by 5% after the intraoperative injection of lidocaine (1 mg/kg) in two patients during scoliosis surgery.8 Another 16 patients observational study found decreased amplitudes and prolonged latencies of SEPs after continuous infusion of lidocaine at 4 mg/kg/h followed by intraoperative injection of lidocaine at 3 mg/kg.9 However, contrary to these findings, one retrospective study and one randomized crossover study have suggested that continuous infusion of 1–1.5 mg/kg/h lidocaine during surgery has no effect on SEPs and MEPs.10,11 Whether lidocaine influences intraoperative electrophysiological monitoring, whether its effects on electrophysiological monitoring are related to drug concentration, and whether electrophysiological monitoring can accurately reflect the integrity of nerve functions under anaesthesia are still unclear, and further studies are necessary. We would like to conduct this randomized controlled study testing the effect of moderate doses of lidocaine on electrophysiological monitoring and provide high-level clinical evidence.
This single-centre, prospective, randomized, placebo-controlled, double-blind trial is designed to evaluate the effects of IV infusion of lidocaine on electrophysiological monitoring during intraspinal tumour resection. The primary outcome measures will be the MEP amplitudes of both upper limbs at the end of operation. The secondary outcome measures will be the MEP latencies of both upper limbs, the MEP latencies and amplitudes of both lower limbs, the SEP latencies and amplitudes of all four limbs at the end of operation, the incidence of alert events for all four limbs, and the incidence of false positive events.
Study Design and Methods
This single-centre, prospective, randomized, placebo-controlled, double-blind trial is designed to evaluate the effects of IV infusion of lidocaine on electrophysiological monitoring during intraspinal tumour resection.
All of the patients participating in this study will undergo intraspinal tumour resection at Beijing Tiantan Hospital, Capital Medical University. The flow chart for this study is shown in Figure 1, and the trial schedule is presented in Table 1. The investigators will screen, recruit, and follow the patients. All of the investigators will receive the same training.
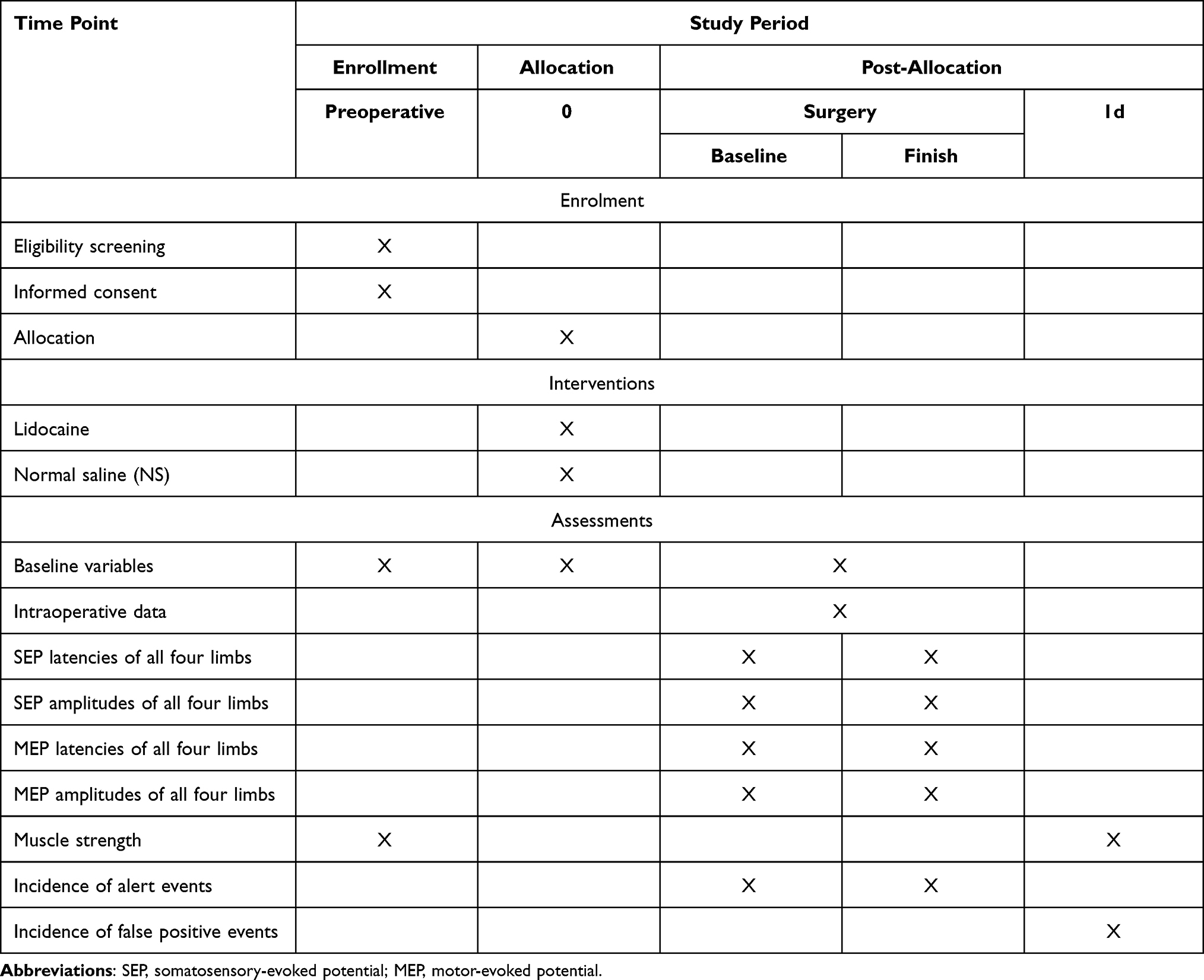 |
Table 1 Trial Schedule |
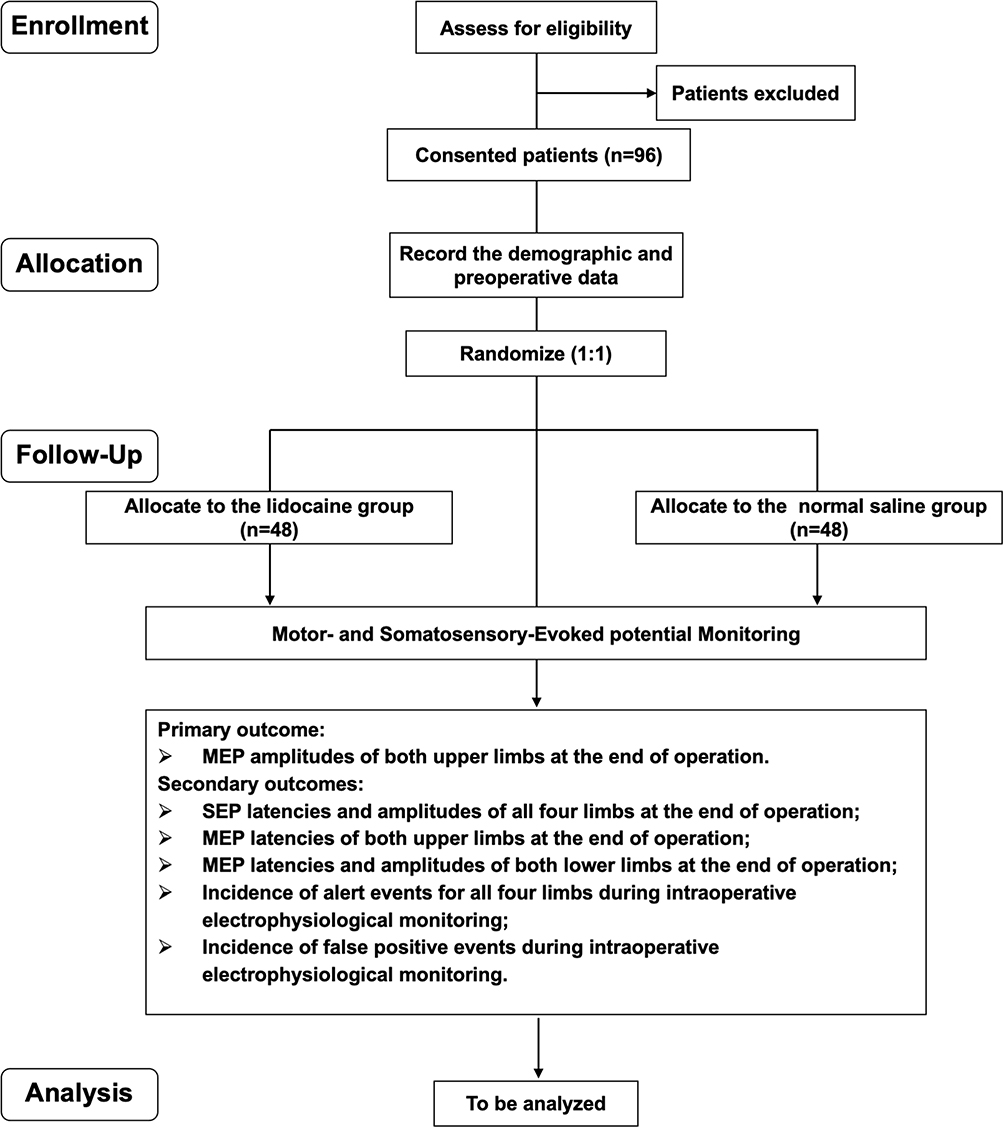 |
Figure 1 Flowchart of the study procedure. Abbreviations: SEP, somatosensory-evoked potential; MEP, motor-evoked potential. |
Approval of the Study Protocol
All of the study procedures will be conducted in accordance with Declaration of Helsinki (October 19, 2013). The study protocol (protocol version 1.0) was approved by the Medical Ethics Committee, Beijing Tiantan Hospital, Capital Medical University (KY2017-063-02) and has been registered with chictr.org.cn (ChiCTR1900021134). This trial is a part of the clinical trial, A New Strategy of Anesthesia and Analgesia for Intraspinal Tumor Surgery with Intravenous Lidocaine. We have previously published another study protocol about the effects of intravenous lidocaine on postoperative pain control,12 and this study protocol is about the effects of intravenous lidocaine on intraoperative electrophysiological monitoring during intraspinal tumour resection.
If the study may impact on the potential benefit of the patient or patient safety, we will amend the protocol. Such amendment will be approved by the Medical Ethics Committee.
Informed Consent
All of the participants will sign informed consent forms and will be given time to decide whether to participate in this study. The study participants will have the right to know all relevant information and will be allowed to withdraw from the study at any time during the process without any restrictions. The participants’ information will be protected.
Study Population
The Inclusion Criteria are as Follows
- Elective resection for thoracolumbar intraspinal tumours under general anaesthesia;
- Intraoperative electrophysiological monitoring;
- American Society of Anaesthesiologists (ASA) Grade I–II;
- Age 18–65 years.
The Exclusion Criteria are as Follows
- History of drug abuse, psychiatric disorders, other central nervous system diseases or obesity (>130% of standard body weight);
- Cardiovascular diseases and unstable hypertension;
- Long-term chronic pain or sensory disturbance of the upper limbs;
- Communication disorders;
- Contraindications for propofol, opioids and lidocaine (eg, allergy, cardiac conduction block, porphyria).
Randomization and Blinding
The subjects will be randomly allocated into a lidocaine group (experimental group) and a placebo group (control group) at a 1:1 ratio. Random grouping will be performed using a computer-generated random number list. The grouping information will be sealed in opaque envelopes, and the subjects, neurosurgeons, anaesthesiologists, neurophysiologists, and the doctors providing the follow-up will not know the grouping information. The investigator responsible for the study will open the opaque envelope containing the patient’s grouping information before the operation and will fill a 50-mL syringe labelled “study protocol” with either 1000 mg of lidocaine or an equal amount of normal saline.
Subject Eligibility and Identification
Patients will be visited one day prior to their operation to evaluate their eligibility for enrolment. All of the enrolled patients will be informed of all related information, including the purpose, procedures, benefits, and potential risks of the study, and will have time to decide whether to participate. Each participant will sign an informed consent form. The investigators will complete a qualification questionnaire that includes the items listed in the case report form (CRF) and the patient’s demographic characteristics, including age (years), sex (male or female), height, weight, and ASA grade. Patients who do not meet the inclusion criteria will be excluded.
Intervention
All participants will be randomly divided into a lidocaine group (Group L) and a placebo group (Group C). In Group L, lidocaine 1 mg/kg will be injected intravenously during anaesthesia induction, and lidocaine 2 mg/kg/h will be continuously administered during anaesthesia maintenance. In Group C, an equivalent amount of normal saline will be administered. The anaesthesia schemes used in the study will be implemented by the anaesthesiologists. The anaesthesiologists and neurophysiologists will be unaware of the grouping information.
Perioperative Anaesthesia Management
Preoperative Visit and Evaluation
Patients will be visited at one day prior to the operation to sign informed consent forms, and the muscle strength of the lower limbs will be measured by the neurosurgeon.
Intraoperative Anaesthesia
All patients will be anaesthetized according to the standard anaesthesia scheme. After the patient is sent to the operating room, the IV pathway will be opened, and non-invasive blood pressure (BP), electrocardiogram, pulse oxygen saturation, bispectral index (BIS VISTA, COVIDIEN company, USA), and radial artery catheterization will be performed under local anaesthesia to monitor arterial pressure. After anaesthesia induction, neuroelectrophysiological monitoring (including the SEPs and MEPs of all four limbs) monitoring will be performed.
Midazolam 0.03 mg/kg will be given for sedation once the patient is in the operating room, and sufentanil 0.3 μg/kg, lidocaine 1 mg/kg (Group L)/equal amount of normal saline (Group C), and propofol 1.5–3 mg/kg will be administered in sequence. Rocuronium 0.3 mg/kg will be administered once the patient is no longer conscious and the BIS reaches 40–60, and tracheal intubation will be performed after muscle relaxation is achieved. The continuous infusion rate of propofol (4–8mg/kg/h) and remifentanil (0.05–0.25μg/kg/min) will be used to maintain anaesthesia and adjusted according to the operation and intraoperative monitoring results. The infusion rate of lidocaine (Group L)/equal amount of normal saline (Group C) will be kept at 0.1 mL/kg/h, which equals to 2mg/kg/h of lidocaine in Group L. No additional sufentanil or muscle relaxants will be administered during surgery. The end-tidal carbon dioxide partial pressure (ETCO2) will be maintained at 35–45 mmHg during anaesthesia. Ondansetron 8 mg and tramadol 100 mg will be given for preventing vomiting and shivering immediately after the incision is sutured. The anaesthesiologists will stop administering propofol according to clinical conditions when the surgery is near completion. The infusion of remifentanil and the investigational drug will be discontinued at the end of the operation. When the tidal volume is > 6 mL/kg, PETCO2 is < 45 mmHg, and swallowing and cough reflexes return to normal, the tracheal tube will be removed. After tracheal extubation, the participants will be shifted to the postanesthetic care unit and closely monitored for 2 hours. The participants will be administered sufentanil for pain control. And the participants will continuously use patient control analgesia pump for acute pain in the ward.
The patients’ vital signs will be closely monitored during operation. Anaesthesiologists can give patients vasoactive drugs, crystalloids, and colloids according to the patient’s clinical conditions to keep the BP within 20% of baseline BP, and a body temperature of 36.0–37.0 °C and a BIS of 40–60 will be ensured.
Electrophysiological Monitoring
Electrophysiological monitoring will be performed by experienced neurophysiologists, and the SEPs and MEPs of the upper and lower limbs will be monitored with the Cadwell Cascade neurophysiologic monitoring system (Cascade, Cadwell Laboratories Inc, WA, USA).
After anaesthesia induction, the monitoring electrodes will be placed according to the international 10–20 system electrode placement. The monitoring electrodes used will be subcutaneous needle electrodes. SEPs will be stimulated by a constant current. The needle electrodes used to monitor the upper limbs will be placed on both wrists to stimulate the median nerves, responses will be recorded by electrodes C3’ and C4’ (2 cm behind C3 and C4, respectively), and reference electrodes will be placed at Fz. The needle electrodes for monitoring the lower limbs will be placed on both ankles to stimulate the posterior tibial nerve, responses will be recorded by electrode Cz’, and reference electrodes will be placed at Fz. The stimulation intensity will be 20–50 mA, and the stimulation frequency will be 2.1–4.7 Hz. MEPs will be stimulated by transcranial electrical stimulation using a constant electric stimulator, and spiral electrodes will be placed at C3 and C4. Subcutaneous needle electrodes will be placed at the thenar and hypothenar, the tibialis anterior and the abductor hallucis muscles on both sides. The stimulation voltage will start at 100 V and will be gradually increased at 25-V intervals as needed. The stimulation voltage will range from 100–400 V, the pulse duration will be 75 µs, and stimulus frequency will be 8/time.
During the operation, the amplitudes and latencies of reliable waveforms of SEPs and MEPs will be recorded with moderate stimulation, and spinal cord functions will be evaluated according to the SEP and MEP results measured under neuroelectrophysiological monitoring. The stimulus intensity or voltage will be adjusted when the wave amplitude decreased significantly. The SEP stimulation intensity will not exceed 50 mA and the MEP stimulation voltage will not exceed 400 V. Before (baseline) and after tumour resection, the upper limbs will be stimulated at an intensity of 25 mA, and the lower limbs will be stimulated at an intensity of 35 mA. The latencies, amplitudes (N20P25 and P40N55 amplitudes for upper and lower limbs respectively), and stimulation time of the SEPs in all four limbs will be recorded. Both sides will be stimulated at an intensity of 250 V, and the onset latencies, amplitudes, and stimulation time of the MEPs in all four limbs will be recorded. The baseline measurement will be performed 20–30 min after tracheal intubation when the TOF ratio reach 0.9, and the last measurement will be performed at the end of operation. Incidences of amplitude decreases > 50% and latency prolongations > 10% in the SEPs and MEPs will be recorded; these conditions are defined as alert events. The data of all patients will be collected. Special surgical procedures and medication periods that could interfere with electrical signals will be avoided during data collection.
Patients will be excluded from the study if the following situations occurs: allergic reactions to lidocaine; drug infusion time > 6 h; serious intraoperative cardiovascular events that cannot be corrected with symptomatic treatment; or discontinuation of electrophysiological monitoring for non-anaesthesia-related reasons.
Follow-Up
One day after the operation, the muscle strength of both lower limbs will be measured by the neurosurgeon. False positive events (amplitude decreases > 50% or latency prolongation > 10%, but the muscle strength did not weaken) in SEPs and MEPs will be analysed in both groups.
Outcomes
The purpose of this study is to evaluate the interference of IV infusion of lidocaine with SEP and MEP monitoring during intraspinal tumour resection and to explore the safety of lidocaine use during such surgeries.
Baseline Data
The patients’ age (years), sex (male or female), height, weight, tumour location (extramedullary or intramedullary tumour), and muscle strength of all four limbs will be tested before enrolment. The following data will be collected during the operation: anaesthesia duration, dosage of propofol and remifentanil, BP, heart rate (HR), BIS, etc.
Primary Outcomes
MEP amplitudes of both upper limbs at the end of operation.
Secondary Outcomes
- SEP latencies and amplitudes of all four limbs at the end of operation;
- MEP latencies of both upper limbs at the end of operation;
- MEP latencies and amplitudes of both lower limbs at the end of operation;
- Incidence of alert events for all four limbs during intraoperative electrophysiological monitoring;
- Incidence of false positive events during intraoperative electrophysiological monitoring.
Sample Size Calculation
Based on our previous research, we predict that there will be no significant difference in intraoperative electrophysiological monitoring effects between Group L and Group C. PASS V.11 software (NCSS, Kaysville, Utah, USA) was used to calculate the sample size, with the postoperative MEP amplitudes of both upper limbs as the primary endpoint. According to the pre-experiment results, references, and clinical experience, the expected MEP amplitude of the upper limbs in Group C is 600 μV, and a significant difference was defined as a 50% decrease in the MEP amplitude of the upper limbs in Group L. The sample size was calculated with an equivalence test with an alpha level of 0.05, a beta level of 0.2, and a loss-to-follow-up rate of 10%. The total sample size required for each group was 96. Therefore, a total of 96 patients (48 patients in each group) will be enrolled in this study.
Statistical Analysis
Statistical Analysis System (SAS) version 9.2 (SAS Institute, Cary, NC) and EmpowerStats software (www.empowerstats.com; X&Y Solutions Inc., Boston MA) will be used for the data analysis. The Kolmogorov-Smirnov test will be adopted to test the normality of continuous variables, such as age, weight, height, anaesthesia duration, operation duration and BIS. Normal distribution data will be expressed as mean ± standard deviation (SD), and the t-test will be adopted. Non-normal distribution data will be expressed as median and quartile, and the non-parametric test will be adopted. Sex, ASA grade, operation type, muscle strength, alert events, and false positive events will be statistically analysed using the non-parametric test or the rank sum test. The amplitudes and latencies of the SEPs and MEPs will be statistically analysed with the equivalence test. P < 0.05 will be considered statistically significant.
Reporting of Adverse Events
All adverse events related to the study will be closely monitored, and details such as their nature, severity, and treatments will be recorded in the CRF until these events disappear and the patient’s condition becomes stable Adverse events will be immediately reported to the principal investigator when they occur, and their severity, causes, and consequences will be identified. The chi-square test or Fisher’s exact test will be used to compare all adverse events between the two groups.
Discussion
This single-centre, prospective, randomized, placebo-controlled, double-blind trial is designed to evaluate the effects of IV infusion of lidocaine on electrophysiological monitoring during intraspinal tumour resection. Patients will receive a single IV injection of lidocaine at 1.0 mg/kg, followed by the continuous infusion of lidocaine at 2 mg/kg/h or the same amount of normal saline during the operation. The effects of IV infusion of lidocaine on electrophysiological monitoring will be determined by comparing the latencies and amplitudes of SEPs and MEPs between the two groups.
Intraspinal tumour resection is often performed under the guidance of electrophysiological monitoring. Electrophysiologists evaluate the integrity of nerve functions during surgery by applying intraoperative neurophysiological monitoring (IOM) and provide feedback regarding intraoperative changes in nerve functions to the surgical team in real time to prompt surgeons to take early intervention measures.2 Since the 1970s, IOM has been widely used in spinal surgeries such as scoliosis correction, intramedullary or extramedullary tumour resection, and anterior or posterior decompression for widening spinal canal stenosis13 to ensure the timely detection of spinal cord and nerve root injuries due to various causes (such as mechanical traction, ischemia, and anaesthesia) during surgery and to effectively issue alarms, reduce iatrogenic nerve injuries and postoperative neurological dysfunction, and actively improve the prognosis of patients.
However, IOM is easily affected by anaesthetics, vital signs, and other factors. Therefore, anaesthesiologists should choose appropriate anaesthetics to avoid the influence of anaesthetics on the latencies and amplitudes of SEPs and MEPs while meeting surgical needs. Studies have found that high concentrations of inhaled anaesthetics and muscle relaxants can reduce the amplitudes of evoked potentials and prolong their latencies.2 Therefore, total IV anaesthesia (TIVA) is recommended for surgeries guided by MEP and SEP monitoring, and different low-dose drugs with complementary effects can be added to provide satisfactory anaesthesia and minimize the influences of single large doses of drugs on evoked potential monitoring. At present, the most commonly used clinical anaesthesia scheme is propofol combined with high-dose opioids,14 especially remifentanil, an ultrashort-acting opioid. However, high-dose remifentanil can cause hyperalgesia; increase the perioperative need for opioids and the incidences of nausea and vomiting, urinary retention and intestinal obstruction; and prolong the recovery time after surgery.3,4 One problem that anaesthesiologists have been trying to solve is determining what auxiliary drugs should be used to relieve hyperalgesia caused by high-dose remifentanil and reducing the demand for opioids and the occurrence of side effects during perioperative period. Lidocaine may solve this problem. The addition of lidocaine during the perioperative period can reduce the use of opioids. Previous studies have shown that lidocaine can exert analgesic effects through various mechanisms. First, lidocaine can block the sodium channel in nerve fibres and inhibit the polysynaptic reflex induced by C fibres and Aδ fibres, thus inhibiting the abnormal discharges of injured primary nerve cells and blocking pain conduction.7,15 Second, lidocaine can block the expression of N-methyl-aspartate receptor (NMDAR) in the dorsal horn of the spinal dorsal15 and offers good control of neuropathic pain caused by space-occupying diseases in the spinal canal and hyperalgesia caused by opioids.16–18 Third, lidocaine can inhibit the activation of leukocytes through inhibiting nuclear factor kB (NF-kB) and protein kinase C pathways,19 lower the release of inflammatory factors, alleviate tissue injuries,20 promote the production of interleukin-1 receptor antagonists, and block nerve transmission from injured sites, thus playing anti-inflammatory and analgesic roles.21
Increasing numbers of studies have found that IV infusion of lidocaine can relieve postoperative pain, reduce perioperative opioid use, relieve nausea and vomiting, reduce postoperative cognitive dysfunction, inhibit inflammatory reaction, and shorten the duration of intestinal paralysis and length of stay for abdominal surgeries,22,23 spinal surgeries,24 head and neck surgeries,25 urological surgeries,20 and gynaecological surgeries.26
At present, there is still no study of IV infusion of lidocaine for intraspinal tumour resection. Whether IV infusion of lidocaine can be used for anaesthesia in intraspinal tumour resection depends on whether it effects electrophysiological monitoring. The effects of IV infusion of lidocaine on SEPs and MEPs are still inconclusive. Some scholars believe that lidocaine can affect cell electrical activity and thus interfere with electrophysiological monitoring. In the study of Schubert et al,9 intravenous lidocaine 3 mg/kg bolus followed by infusion at 4 mg/kg/h was injected into 16 patients undergoing abdominal or orthopaedic surgery under sufentanil-based anaesthesia, to observe its effects on SEPs. The plasma-drug concentrations of lidocaine at different time points after administration were measured. The study of Schubert et al found that IV administration of lidocaine at clinical therapeutic plasma-drug concentrations could reduce the amplitudes of SEPs and prolong their latencies. Chaves-Vischer et al8 reported that the SEP amplitudes decreased or even disappeared, and the latencies prolonged after IV administration of 1 mg/kg lidocaine in two patients undergoing scoliosis surgery. However, some studies have reported different conclusions. In the study by Sloan et al,10 129 patients undergoing spinal surgeries under total IV anaesthesia with propofol and opioids were reviewed. Among them, 50 patients were given 1.5 mg/kg/h lidocaine after induction, and the SEPs and MEPs monitoring of these patients was not disturbed. Urban et al11 conducted a cross-over prospective study examined the intrapatient effects of the addition of lidocaine to balanced anaesthesia on MEPs and SSEPs during multilevel posterior spinal fusion. It showed that 1 mg/kg/h lidocaine did not affect MEP threshold voltages and SEP amplitudes within patient.
Whether lidocaine influences IOM, whether its influence on electrophysiological monitoring is related to drug concentration, and whether electrophysiological monitoring can accurately reflect the integrity of nerve function under anaesthesia are still unclear at present and require further studies.
In this study, the latencies and amplitudes of SEPs and MEPs in the upper and lower limbs will be recorded to evaluate the effects of continuous IV infusion of lidocaine on electrophysiological monitoring during intraspinal tumour resection, thereby exploring the safety of the addition of lidocaine in such surgeries.
Space-occupying lesions in the thoracolumbosacral spinal canal often cause abnormal sensory activity of the lower limbs in patients, while the upper limbs are not affected. To eliminate the interference of disease itself and the surgical operation, the upper limbs will be the main observation object in the proposed study. In addition, the intraoperative monitoring of MEPs is more susceptible than SEPs to drug interference, and the amplitude is more sensitive than the latency and can reflect the clinical situation quickly.2 Therefore, the MEP amplitudes of both upper limbs will be the primary outcome measures in this study. To confirm whether the electrophysiological monitoring considered in this study can accurately guide surgery, the SEPs and MEPs of both lower limbs were selected as secondary outcome measures. In previous studies, amplitude decreases > 50% or latency prolongation > 10% in SEPs and MEPs were regarded as having guiding clinical significance and were considered alert criteria.27,28 However, there are false positive events during operation (eg, when alerts occur during surgery, but no organic injury to the limb nerves is observed after surgery) because monitoring results are influenced by many factors, and most alert events are caused by non-operative factors. To better confirm the guiding significance of electrophysiological monitoring indicators under the anaesthesia scheme considered in this study, the incidences of intraoperative alert events and false positive events will also be included as secondary outcome measures.
In this study, the latencies and amplitudes of SEPs and MEPs will be recorded at two key time points, ie, before tumour resection (baseline) and after tumour resection. The effects of long-term continuous infusion of 2 mg/kg/h lidocaine or an equal amount of normal saline on electrophysiological monitoring of all four limbs will be compared at the end of the operation. Special surgical procedures, special medications, and periods in which vital signs fluctuate greatly will be avoided, and indexes such as BP, HR, and anaesthesia depth at these time points will be recorded.
Many aspects of anaesthesia management can affect intraoperative electrophysiological monitoring. Therefore, except for the use of lidocaine, both groups in this study will receive the same anaesthesia scheme. The dose of muscle relaxant will be reduced by half during induction, and no additional anaesthesia will be added during surgery. Invasive BP, body temperature, and anaesthesia depth will be closely monitored, and circulatory and respiratory stability will be maintained to minimize the influences of other factors on electrophysiological monitoring. If electrophysiological monitoring abnormalities affect the normal operation and monitoring in ways that cannot be explained by other intraoperative factors and are suspected to be related to the investigational drug, the experiment will be terminated immediately, and relevant events will be recorded.
Medication safety is one of the concerns of this study. When the plasma-drug concentration of lidocaine is more than 5 μg/mL, it may affect the central nervous system (causing drowsiness, unconsciousness, euphoria, diplopia, epilepsy), cardiovascular system (causing hypotension, bradycardia, arrhythmia, cardiac arrest), respiratory system (causing shortness of breath, apnoea), and the blood (causing methemoglobinemia).21 Previous studies have shown that the plasma-drug concentration of lidocaine is generally maintained at 2–5 μg/mL when lidocaine is given intravenously at 1.5–3 mg/kg/h, which is far lower than the toxic dose.29 In this study, low-concentration lidocaine (2 mg/kg/h) will be used for intraoperative infusion, and all of the participants will be closely monitored. The drug will be discontinued immediately if the patient presents adverse events related to lidocaine, such as signs of systemic toxicity (headache, tinnitus, metallic taste, seizure, abnormal electrocardiogram), refractory hypotension, and bradycardia. In addition, if lidocaine is infused intravenously for more than 6 h, it will be discontinued, and the participant will be excluded.
Potential limitations of this study are that the plasma-drug concentration of lidocaine will not be measured, which could cause insufficient guidance for determining the plasma-drug concentration of lidocaine in target-controlled infusion (microcomputer-controlled infusion) during electrophysiological monitoring in the future.
In summary, this study is designed as a single-centre, prospective, randomized, placebo-controlled, double-blind trial that aims to evaluate the effects of IV infusion of lidocaine on SEPs and MEPs during intraspinal tumour resection and explore its possible application in such surgeries as a potential new anaesthetic option.
Trial Status
This trial was registered with chictr.org.cn on January 29, 2019 (identification no. ChiCTR1900021134), was approved by the Medical Ethics Committee, Beijing Tiantan Hospital, Capital Medical University on October 31, 2017 (No. KY2017-063-02), and was estimated to be completed in July 2022.
Data Sharing Statement
The collected data will be stored in a secure repository at Beijing Tiantan Hospital. The datasets will be available from the chief investigator upon reasonable request.
Acknowledgments
Beijing Municipal Administration of Hospitals Incubating Program (No. PX2019019).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Matsuyama Y, Sakai Y, Katayama Y, et al. Surgical results of intramedullary spinal cord tumor with spinal cord monitoring to guide extent of resection. J Neurosurg Spine. 2009;10(5):404–413. doi:10.3171/2009.2.SPINE08698
2. Nunes RR, Bersot CDA, Garritano JG. Intraoperative neurophysiological monitoring in neuroanesthesia. Curr Opin Anaesthesiol. 2018;31(5):532–538. doi:10.1097/ACO.0000000000000645
3. Weibel S, Jelting Y, Pace NL, et al. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults. Cochrane Database Syst Rev. 2018;6:CD009642. doi:10.1002/14651858.CD009642.pub3
4. Koppert W, Schmelz M. The impact of opioid-induced hyperalgesia for postoperative pain. Best Pract Res Clin Anaesthesiol. 2007;21(1):65–83. doi:10.1016/j.bpa.2006.12.004
5. Li J, Wang G, Xu W, Ding M, Yu W. Efficacy of intravenous lidocaine on pain relief in patients undergoing laparoscopic cholecystectomy: a meta-analysis from randomized controlled trials. Int J Surg. 2018;50:137–145. doi:10.1016/j.ijsu.2018.01.001
6. Reeves DJ, Foster AE. Continuous intravenous lidocaine infusion for the management of pain uncontrolled by opioid medications. J Pain Palliat Care Pharmacother. 2017;31(3–4):198–203. doi:10.1080/15360288.2017.1313356
7. Dunn LK, Durieux ME. Perioperative use of intravenous lidocaine. Anesthesiology. 2017;126(4):729–737. doi:10.1097/ALN.0000000000001527
8. Chaves-Vischer V, Brustowicz R, Helmers SL. The effect of intravenous lidocaine on intraoperative somatosensory evoked potentials during scoliosis surgery. Anesth Analg. 1996;83(5):1122–1125. doi:10.1213/00000539-199611000-00042
9. Schubert A, Licina MG, Glaze GM, Paranandi L. Systemic lidocaine and human somatosensory-evoked potentials during sufentanil-isoflurane anaesthesia. Can J Anaesth. 1992;39(6):569–575. doi:10.1007/BF03008320
10. Sloan TB, Mongan P, Lyda C, Koht A. Lidocaine infusion adjunct to total intravenous anesthesia reduces the total dose of propofol during intraoperative neurophysiological monitoring. J Clin Monit Comput. 2014;28(2):139–147. doi:10.1007/s10877-013-9506-x
11. Urban MK, Fields K, Donegan SW, et al. A randomized crossover study of the effects of lidocaine on motor- and sensory-evoked potentials during spinal surgery. Spine J. 2017;17(12):1889–1896. doi:10.1016/j.spinee.2017.06.024
12. Yue H, Zhou M, Lu Y, Chen L, Cui W. Effect of intravenous lidocaine on postoperative pain in patients undergoing intraspinal tumor resection: study protocol for a prospective randomized controlled trial. J Pain Res. 2020;13:1401–1410. doi:10.2147/JPR.S249359
13. Nash CL
14. Liu HY, Zeng HY, Cheng H, Wang MR, Qiao H, Han RQ. Comparison of the effects of etomidate and propofol combined with remifentanil and guided by comparable BIS on transcranial electrical motor-evoked potentials during spinal surgery. J Neurosurg Anesthesiol. 2012;24(2):133–138. doi:10.1097/ANA.0b013e31823dfb2e
15. Wang Q, Ding X, Huai D, Zhao W, Wang J, Xie C. Effect of intravenous lidocaine infusion on postoperative early recovery quality in upper airway surgery. Laryngoscope. 2020;131(1):E63–E69. doi:10.1002/lary.28594
16. Cui W, Li Y, Li S, Wang R, Li J. Systemic administration of lidocaine reduces morphine requirements and postoperative pain of patients undergoing thoracic surgery after propofol-remifentanil-based anaesthesia. Eur J Anaesthesiol. 2010;27(1):41–46. doi:10.1097/EJA.0b013e32832d5426
17. Cui W, Li Y, Li S, et al. Systemic lidocaine inhibits remifentanil-induced hyperalgesia via the inhibition of cPKCgamma membrane translocation in spinal dorsal horn of rats. J Neurosurg Anesthesiol. 2009;21(4):318–325. doi:10.1097/ANA.0b013e3181abbde5
18. Kim YC, Castaneda AM, Lee CS, Jin HS, Park KS, Moon JY. Efficacy and safety of lidocaine infusion treatment for neuropathic pain: a randomized, double-blind, and placebo-controlled study. Reg Anesth Pain Med. 2018;43(4):415–424. doi:10.1097/AAP.0000000000000741
19. Chang YC, Liu CL, Liu TP, Yang PS, Chen MJ, Cheng SP. Effect of perioperative intravenous lidocaine infusion on acute and chronic pain after breast surgery: a meta-analysis of randomized controlled trials. Pain Pract. 2017;17(3):336–343. doi:10.1111/papr.12442
20. Moeen SM, Moeen AM. Usage of intravenous lidocaine infusion with enhanced recovery pathway in patients scheduled for open radical cystectomy: a randomized trial. Pain Physician. 2019;22(2):E71–E80. doi:10.36076/ppj/2019.22.E71
21. Yardeni IZ, Beilin B, Mayburd E, Levinson Y, Bessler H. The effect of perioperative intravenous lidocaine on postoperative pain and immune function. Anesth Analg. 2009;109(5):1464–1469. doi:10.1213/ANE.0b013e3181bab1bd
22. Zhao JB, Li YL, Wang YM, et al. Intravenous lidocaine infusion for pain control after laparoscopic cholecystectomy: a meta-analysis of randomized controlled trials. Medicine. 2018;97(5):e9771. doi:10.1097/MD.0000000000009771
23. Cooke C, Kennedy ED, Foo I, et al. Meta-analysis of the effect of perioperative intravenous lidocaine on return of gastrointestinal function after colorectal surgery. Tech Coloproctol. 2019;23(1):15–24. doi:10.1007/s10151-019-1927-1
24. Kim KT, Cho DC, Sung JK, et al. Intraoperative systemic infusion of lidocaine reduces postoperative pain after lumbar surgery: a double-blinded, randomized, placebo-controlled clinical trial. Spine J. 2014;14(8):1559–1566. doi:10.1016/j.spinee.2013.09.031
25. Choi GJ, Kang H, Ahn EJ, et al. Clinical efficacy of intravenous lidocaine for thyroidectomy: a prospective, randomized, double-blind, placebo-controlled trial. World J Surg. 2016;40(12):2941–2947. doi:10.1007/s00268-016-3619-6
26. Wang T, Liu H, Sun JH, Wang L, Zhang JY. Efficacy of intravenous lidocaine in improving post-operative nausea, vomiting and early recovery after laparoscopic gynaecological surgery. Exp Ther Med. 2019;17(6):4723–4729. doi:10.3892/etm.2019.7497
27. Stecker MM, Robertshaw J. Factors affecting reliability of interpretations of intra-operative evoked potentials. J Clin Monit Comput. 2006;20(1):47–55. doi:10.1007/s10877-005-9006-8
28. Hernandez-Palazon J, Izura V, Fuentes-Garcia D, Piqueras-Perez C, Domenech-Asensi P, Falcon-Arana L. Comparison of the effects of propofol and sevoflurane combined with remifentanil on transcranial electric motor-evoked and somatosensory-evoked potential monitoring during brainstem surgery. J Neurosurg Anesthesiol. 2015;27(4):282–288. doi:10.1097/ANA.0000000000000157
29. Digala LP, Lucchese S. IV lidocaine infusion leading to the toxic levels in serum causing asystole - a case report. Headache. 2020;60(1):269–270. doi:10.1111/head.13699
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.