")
Back to Journals » International Journal of Women's Health » Volume 12
Effects of Labor Epidural Analgesia on Short Term Neonatal Morbidity
Authors Salameh KM , Anvar Paraparambil V, Sarfrazul A, Lina Hussain H , Sajid Thyvilayil S, Samer Mahmoud A
Received 26 August 2019
Accepted for publication 3 January 2020
Published 4 February 2020 Volume 2020:12 Pages 59—70
DOI https://doi.org/10.2147/IJWH.S228738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Khalil Mohd Salameh, Vellamgot Anvar Paraparambil , Abedin Sarfrazul, Habboub Lina Hussain, Salim Sajid Thyvilayil , Alhoyed Samer Mahmoud
Department of Pediatrics and Neonatology, Al Wakra Hospital, Hamad Medical Corporation, Al Wakra, Qatar
Correspondence: Khalil Mohd Salameh
Department of Pediatrics and Neonatology, Al Wakra Hospital, Hamad Medical Corporation, Al Wakra, Qatar
Tel +974 40114258
Email [email protected]
Background: Epidural Analgesia (EA) is the most effective and most commonly used method for pain relief during labor. Some researchers have observed an association between EA and increased neonatal morbidity. But this observation was not consistent in many other studies.
Objectives: The primary objective of the study was to examine whether exposure to epidural analgesia increased the risk of NICU admission. The secondary objectives included the risks of clinical chorioamnionitis, instrumental delivery, neonatal depression, respiratory distress, birth trauma, and neonatal seizure during the first 24 hours of life.
Methods: This was a retrospective cohort study involving 2360 low-risk nulliparous women who delivered at AWH, Qatar, during the two years between January 2016 December and 2017. Short-term neonatal outcomes of the mothers who received EA in active labor were compared with a similar population who did not receive EA. As secondary objectives, labor parameters like maternal temperature elevation, duration of the second stage of labor, and instrumental delivery were compared.
Results: Significantly higher numbers of neonates were admitted to the NICU from the EA group (P< 0.001, OR 1.89, 95% CI 1.45 to 2.46). They were more likely to have respiratory distress (P=0.01, OR 1.49, 95% CI 1.07 to 2.07), birth injuries (P=0.02, OR =1.71, 95% CI 1.06 to 2.74), admission temperature> 37.5 °C (P= 0.04, OR 3.40, 95% CI 1.00 to 11.49), need for oxygen on the first day (P=0.04, OR 1.44, 95% CI 1.01 to 2.07) and receive antibiotics (P< 0.001, OR 2.06,95% CI 1.47 to 2.79). There was no difference in the Apgar score at 1 minute (P=0.12), need of resuscitation at birth (P=0.05), neonatal white cell count (P=0.34), platelet count (P=0.38) and C reactive protein (P=0.84). Mothers who received EA had a lengthier second stage (P< 0.001), temperature elevation > 37.5°C (P< 0.001, OR 7.40, 95% CI 3.93 to 13.69) and instrumental delivery (P< 0.001, OR 2.13, 95% CI 1.69 to 2.68).
Conclusion: EA increases NICU admission, antibiotic exposure, neonatal birth injuries, need for positive pressure ventilation at birth, and respiratory distress in the first 24 hours of life. Mothers on epidural analgesia have prolonged second stage of labor, a higher rate of instrumental delivery, meconium-stained amniotic fluid, fetal distress, and temperature elevation.
Keywords: epidural analgesia, neonatal morbidity, NICU admission
Definitions
Short term neonatal morbidity-sick conditions of neonates during the early neonatal period. For the current study, any morbidity during the first 24 hours of age like the need for NICU admission, respiratory distress, birth trauma, etc.
Chorioamnionitis (intraamniotic infection): Infection of the placenta and the amniotic membranes.
Apgar score: the standard code used for coding the condition at birth and the need for resuscitation in neonates.
Nulliparous women: women with no previous history of delivery.
Significant congenital anomaly: any birth defect which needs NICU admission
Introduction
Morbidity during the immediate neonatal period is distressing to the babies, parents, and healthcare workers. Birth asphyxia, birth injuries, infections, and respiratory distress are among the leading morbidities during the immediate neonatal period. Affected babies often need admission to NICU. Although essential for meticulous care of sick neonates, the NICU stay separates the baby from the mother, causes parental anxiety, breastfeeding failure, and puts the baby at risk for medical errors and healthcare-associated infections. This is in addition to the cost factors. Maternal factors like prolonged labor, instrumental delivery, and intrapartum fever may contribute to these morbidities.1–3
Good pain relief is one of the most critical factors related to patient satisfaction4,5 and EA is the most effective and most widely accepted method of pain relief during labor. Internationally, the rate of epidural use varies between 20–70% of all deliveries.2,6–8 Administration of local anesthetic along with the opioid analgesic to the lumbar epidural space is very effective in attaining labor analgesia.9 EA and CSE are the two most widely accepted techniques. Systemic hypotension and pruritus are the two most common side effects of EA. Both techniques have similar effects on the neonatal outcome.64
Previous studies have shown a higher rate of the prolonged second stage of labor and instrumental delivery with EA.6 Instrumental delivery and prolonged labor increase neonatal morbidity.1 Additionally, EA is associated with a significantly higher incidence of maternal intrapartum fever.2,10,11 Maternal fever during labor increases the risk of neonatal morbidity.3,12 Some studies have shown that neonates born to mothers with epidural associated fever have a higher likelihood of being investigated and treated for neonatal sepsis.2,13 However, many other studies failed to show any significant effects of epidural analgesia on neonatal outcomes.6,14
Most of the previous studies focused on maternal outcomes along with a few aspects of neonatal outcome.2,3,6,13 Our search did not identify similar published studies from the Middle East. During the year 2017, 58 % of nulliparous mothers received EA in our institution. As these numbers are high, even rare adverse effects are likely to be significant. Since many of these adverse effects are likely to be dependent on individual obstetric and neonatal management practices, it was justifiable to study the neonatal effects of EA, if any, in our setting. The result could be potentially used while educating mothers seeking labor analgesia.
Objectives
Primary Objective
to study retrospectively whether exposure to EA increased the risk of NICU admission for babies born at AWH between 1st January 2016 and 17th December 2017.
Secondary objectives
- To study whether EA exposure increased the risk of –instrumental delivery, neonatal depression, respiratory distress, and neonatal seizure during the first day.
- To study the rate of epidural associated fever in low-risk nulliparous women and its relation to sepsis workup and antibiotic use in neonates.
Materials and Methods
This was a retrospective cohort study involving all the low-risk nulliparous women who delivered at Al Wakra Hospital, Qatar, during the 2 years from January 2016 to December and 2017.
The Medical Research Centre and the Institutional Review Board (IRB), Hamad Medical Corporation approved the study. Since it was retrospective and all subjects were coded and de-identified, the need for consent was waived off by the IRB.
The study group consisted of low-risk nulliparous women who received EA in active labor. A similar population of mothers who did not receive EA served as control. The short-term outcomes of their neonates were compared between the groups.
Nulliparous mothers are more likely to have prolonged labor, and the effects of EA are likely to be more pronounced. This also provided a more homogenous population.
The Method of Analgesia
In the EA group, all the mothers received EA in active labor after the cervical dilatation was 4 cm or more. Combined spinal-epidural (CSE) was the technique used. The epidural catheter was inserted into the L3-L4 lumbar intervertebral space in the sitting position. Spinal Bupivacaine (0.5%) was delivered by Whitacre G27 spinal needle, followed by epidural infusion of fentanyl and levobupivacaine.
Inclusion Criteria
Singleton delivery, nulliparous mother, gestational age at birth 37 and 41+6 weeks, birth weight between 2.5 and 4 Kg, mother in active labor at least for an hour and cephalic presentation
Exclusion Criteria
Multiple pregnancy, gestation <37 weeks or more than 41+6 weeks, elective LSCS, emergency LSCS within one hour of onset of labor, precipitate labor, pre-existing obstetric risk factors which may affect the neonatal outcome (hypertension, GBS bacteriuria, spontaneous premature rupture of membranes >18 hours, fever at the onset of labor, STD), mother received general anesthesia or morphine during labor, birth weight <2.5kg ≥4kg, major congenital anomalies or inborn errors of metabolism, neonates with culture-proven early-onset sepsis, NICU admission for reasons like jaundice and social reason, admission after 24 hours of life, mother’s age <18 years and >40 years, fetal presentations other than cephalic and incompletely documented parameters
The short-term outcomes of neonates in the two groups (EA and non-EA) were compared.
Study Population and Study Setting
The study was conducted at NICU – AWH. Neonatal and maternal files were examined for all deliveries between January 2016 and December 2017 (24 months).
Data Collection & Confidentiality
Complete delivery statistics for the study period was obtained from the Medical records Department, AWH. Term, nulliparous, singleton live births were selected from this. Elective LSCS, low birth weight and large for gestational age babies were then excluded. The further exclusion was performed by detailed verification of the electronic medical record (Cerner Millenium) of each patient. All links to the identity were destroyed at the end of data collection and verification.
Maternal data included age, parity, gestational age, need for labor induction, duration of the second stage of labor, mode of delivery, instrumental delivery, pathological CTG (baseline fetal heart rate <100, reduced or increased variability/sinusoidal pattern, repetitive late or prolonged decelerations), meconium-stained amniotic fluid, peak intrapartum temperature, suspected chorioamnionitis, placental histopathology and culture and whether received EA or not.
Newborn data included, birth weight, sex, Apgar score at 1 and 5 minutes, need for positive pressure ventilation, need of NICU admission, reason for NICU admission, seizure during the first 24 hours, highest level of respiratory support and its duration, whether received antibiotics during the first 24 hours, duration of antibiotic therapy, length of NICU stay, lab/radiological parameters, C reactive protein during the first 24 hours, leukocyte count and platelet count.
The data was in the safe custody of the Principal Investigator. The electronic data was stored in the office computer of the NICU and protected by a password. After entering the data, the papers with coded identity were stored locked in the personal locker of PI, located inside the NICU duty room.
Data Analysis
Anonymous data were collected and entered into a standard electronic database chart designed according to the study design and objectives. Descriptive statistics were used to summarize all clinical data of mother & baby and outcome variables as needed for NICU admission, the reason for admission, treatment needed, etc. The results were reported with mean and standard deviation (SD) or frequencies and percentages as per the type of data. Associations between two or more qualitative variables were assessed using the chi-square (χ2) test or Fisher Exact test as appropriate. Quantitative variables mean between two and more than two independent groups were analyzed using the unpaired t-test and one-way analysis of variance (ANOVA). The logistic regression test was applied to calculate the Odds Ratio of outcome in the epidural exposed and non-exposed group. All P values presented were two-tailed, and P values <0.05 were considered as statistically significant. All Statistical analyses were done using statistical packages SPSS 22.0 (SPSS Inc. Chicago, IL) software.
Results
Between Jan 2016 and Dec 2017, AWH recorded 10,802 live births. Among these, 3121 were nulliparous mothers (Figure 1). Step 1 exclusion was performed by reviewing the labor room registry and medical records data. This step excluded 305 patients including preterm, post-term, low birth weight, large for gestational age, multiple gestations, elective Caesarian section, and delivery outside the labor room or operation theatre. Second step exclusion was performed by reviewing the individual maternal files. This step excluded further 354 subjects who had risk factors (leaking >18 hours, hypertension, positive GBS carrier state or other significant medical illnesses), precipitate labor, LSCS within one hour of onset of labor, presentation other than cephalic, incompletely documented files or who received general anesthesia or opioid analgesia. The third step excluded 102 subjects by reviewing the baby file. This step excluded significant congenital malformations, incomplete documentation, admission after 24 hours of age or admission for the mother’s sake (sick, postpartum mother).
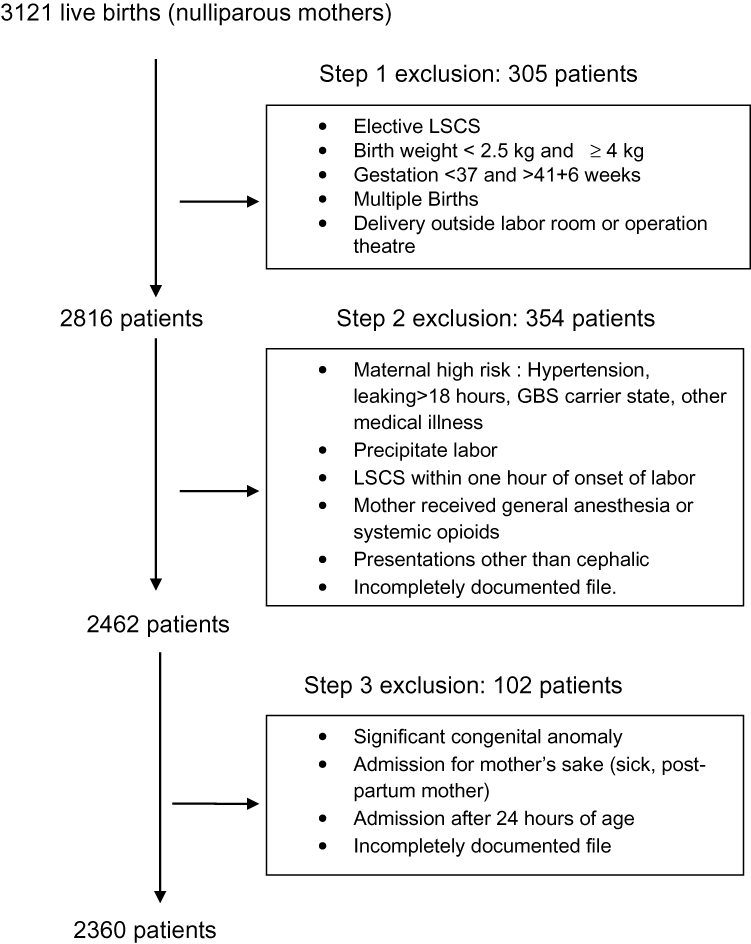 |
Figure 1 Flow chart: exclusion process. |
The final cohort consisted of 2360 patients. Among them, 1490 subjects received EA and 870 received no analgesia.
Baseline maternal and neonatal characteristics included mother’s age, gestational age, induced labor, gestational diabetes, sex, and birth weight These were compared between the EA and non-EA groups (Table 1). Except for gestational age and birth weight, there were no statistically significant differences between the baseline parameters. The statistical significance observed for gestational age (mean difference 0.19 weeks) and birth weight (mean difference 0.089 kg) was not clinically significant.
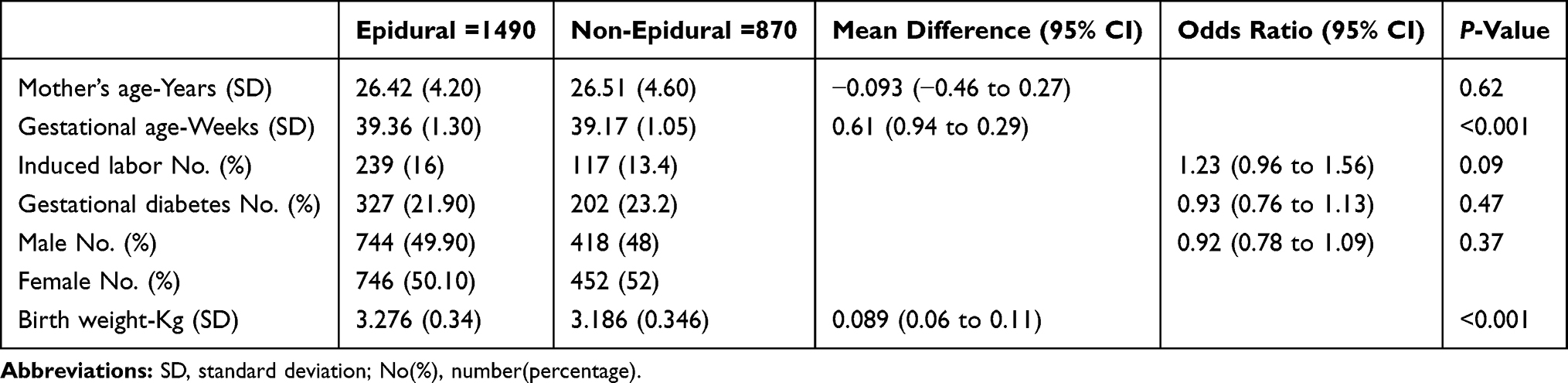 |
Table 1 Baseline Maternal and Neonatal Characteristics |
The duration of the second stage of labor was significantly higher in the EA group (P<0.001) with a mean difference of 49.36 minutes (95% CI 40.45 to 58.28). Mothers in the EA group also had higher peak intrapartum temperature (P<0.001, Mean difference 0.12°C, 95% CI 0.09 to 0.14). EA group had a higher chance of having intrapartum temperature >37.5 °C (P<0.001, OR 7.40, 95% CI 3.93 to 13.69). Fetal distress (P<0.001, OR 1.60, 95% CI 1.30 to 1.98), meconium staining of amniotic fluid (P=0.01, OR 1.31, 95%CI 1.05 to 1.62) and need for instrumental delivery (P<0.001, OR 2.13, 95% CI 1.69 to 2.68) were significantly higher in the EA group. There was no difference in the rate of LSCS (P=0.72) (Table 2).
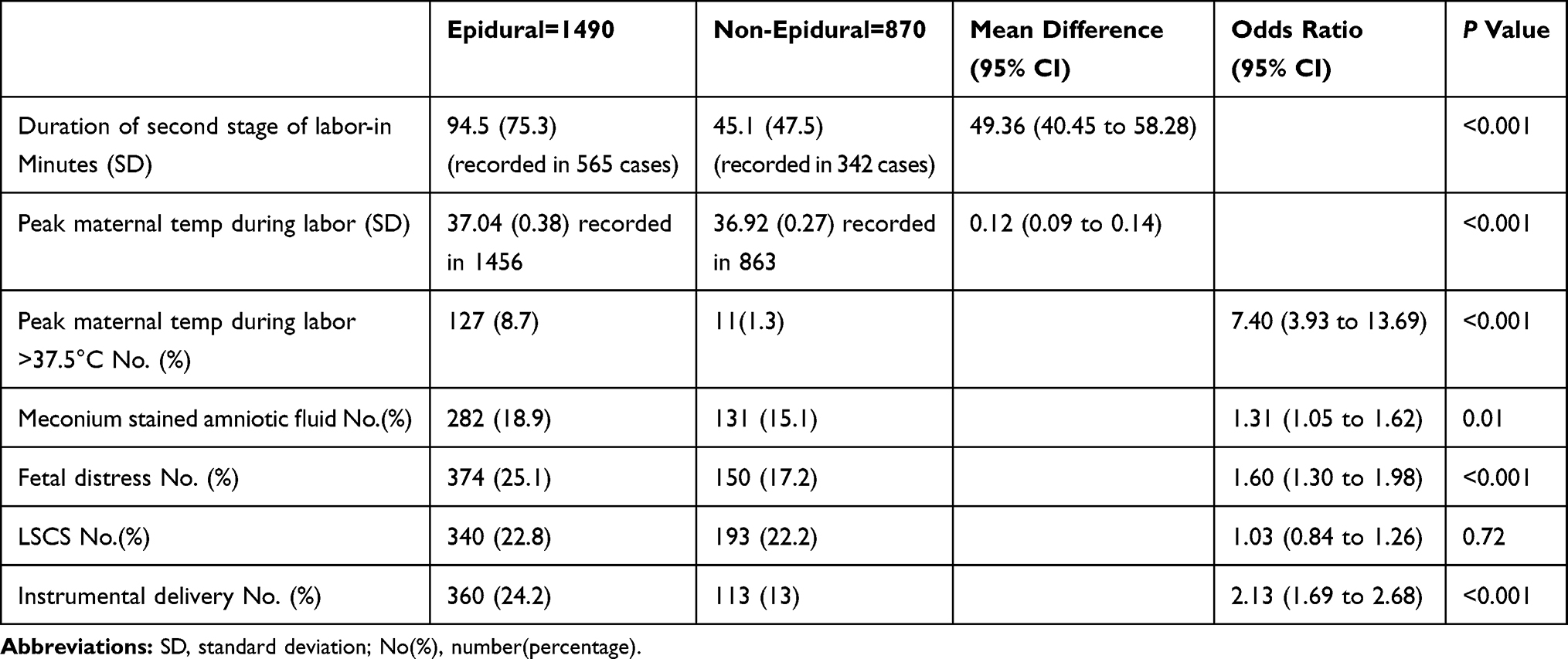 |
Table 2 Maternal Outcomes in EA |
In Table 3, we have compared cord arterial pH, Apgar score at 1 and 5 minutes, birth injury and need of resuscitation at Birth. The birth injury was more frequent in the EA group (P=0.02, OR 1.71, 95% CI 1.06–2.74). There was no difference in Apgar score, cord pH and need for resuscitation at birth. Table 4 shows a comparison of the clinical parameters of neonates. Our primary outcome measure, NICU admission, was significantly higher in the EA group – (P<0.001, OR 1.89, 95% CI 1.45 to 2.46). Among other parameters, neonatal admissions due to suspected maternal chorioamnionitis were significantly higher in the EA group (P<0.001, OR 4.30, 95% CI 2.44 to 7.58). A substantially higher number of neonates in the EA group received antibiotics on day 1 (P<0.001, OR 2.06, 95% CI 1.47 to 2.79).
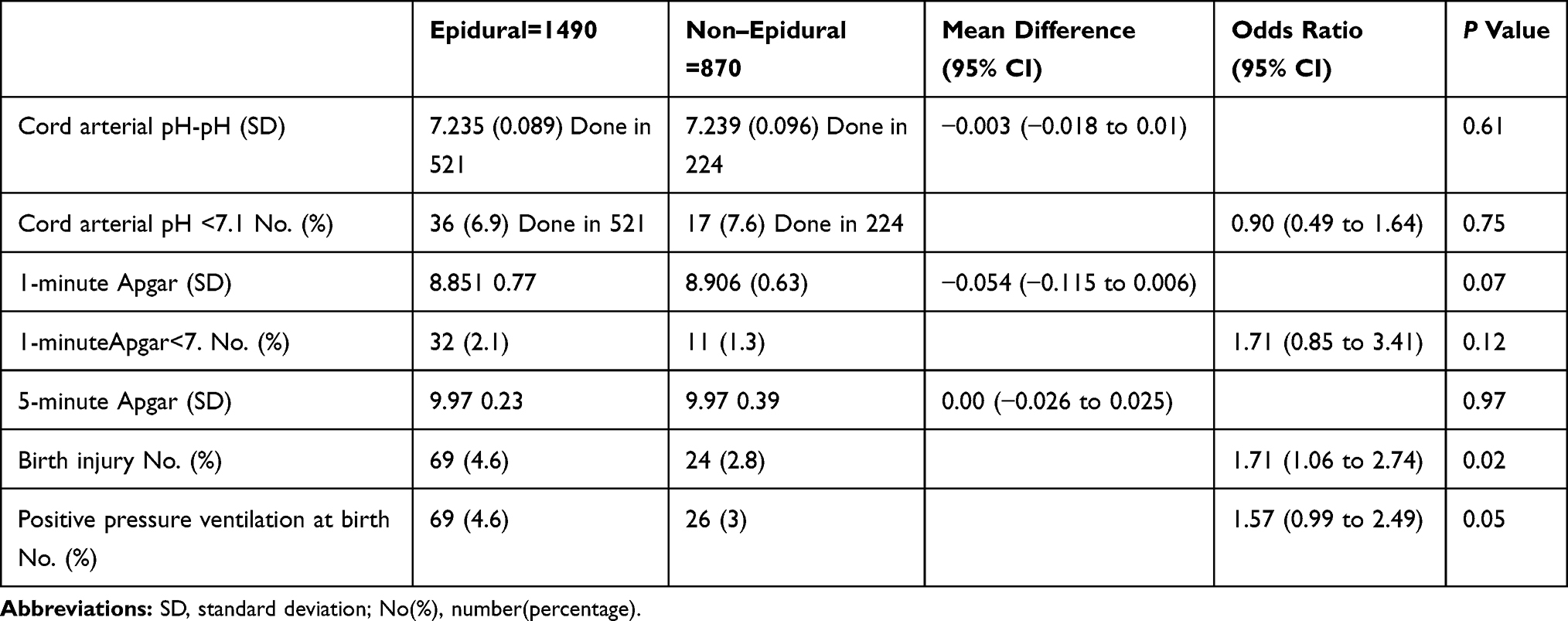 |
Table 3 Perinatal Outcome |
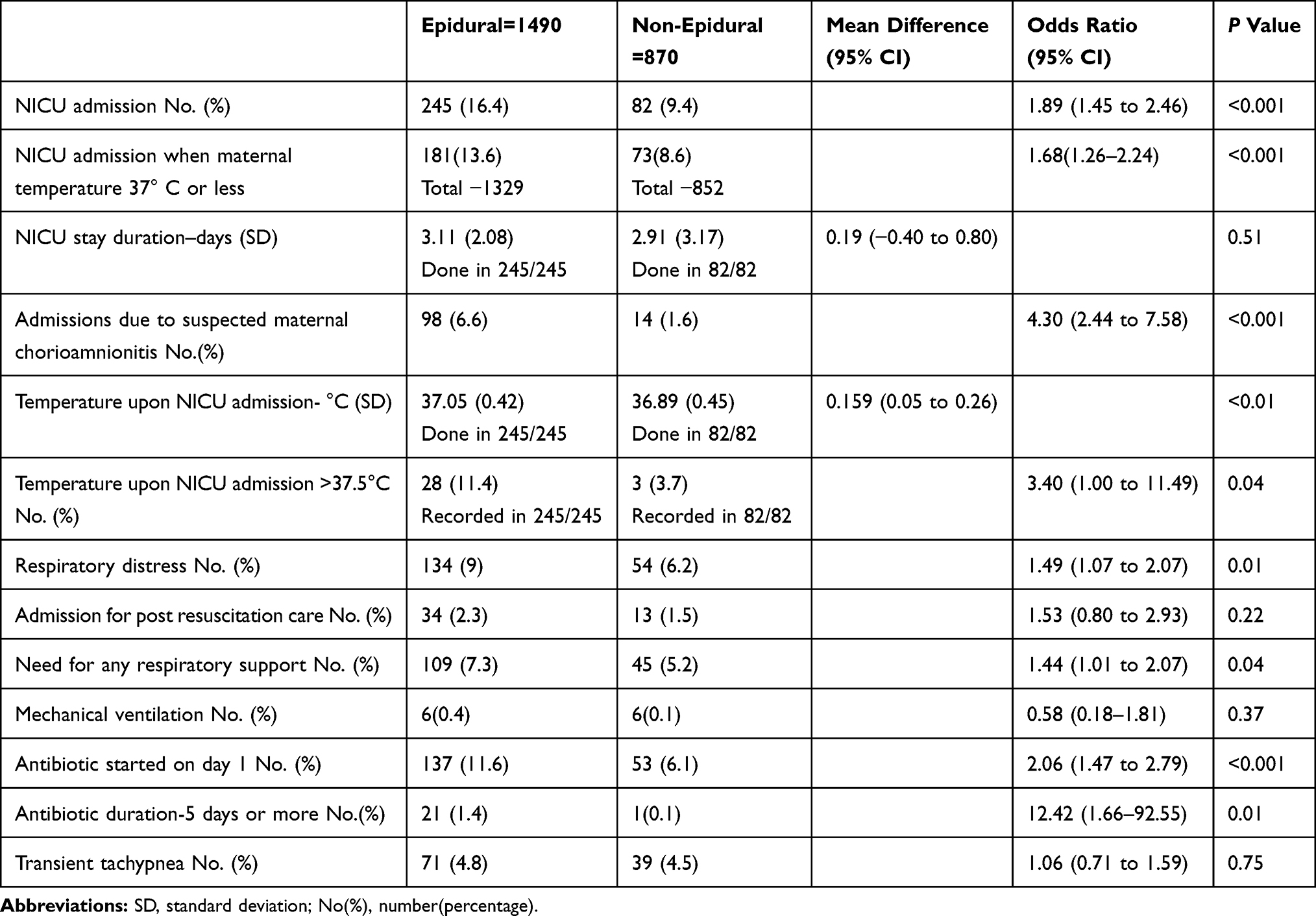 |
Table 4 Effect of Epidural Analgesia on Neonatal Clinical Parameters |
Among babies admitted to NICU, lab parameters were not significantly different between the two groups (Table 5).
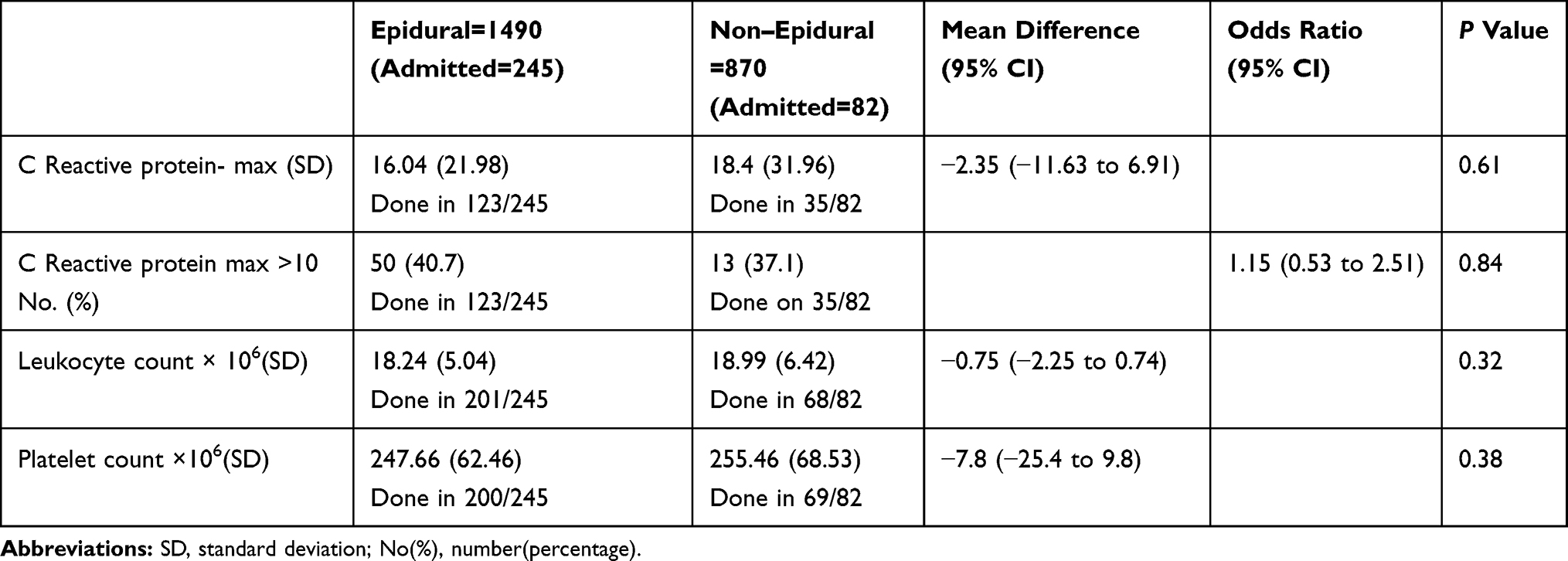 |
Table 5 Effect of Epidural Analgesia on Neonatal Lab Parameters (Done in the Patients Who Needed NICU Admission) |
Discussion
Our final cohort consisted of 2360 subjects. Among them, 1490 (63%) received Epidural Analgesia. The overall use rate of EA in our institution is 33%. The higher rate observed in the study population was attributable to the exclusion of non-nulliparous mothers and elective Caesarian deliveries. In recent years its use has increased worldwide, being used between 20–70% of all deliveries.2,6–8
Baseline maternal and neonatal characteristics (mother’s age, gestational age, nationality, induced labor, gestational diabetes, sex, and birth weight) did not differ between the groups. The statistically significant differences observed in gestational age and birth weight were not clinically significant. This observation was noted in previous studies also.7,15 Gestational diabetes is associated with significant neonatal morbidity.16,65,66 There was no significant difference between the groups in terms of the number of gestational diabetic mothers.
Neonates in the epidural group were more likely to get admitted to NICU. They were more likely to have respiratory distress, birth injuries, admission temperature >37.5 °C, need for positive pressure ventilation at birth, and receive antibiotics.
Mothers in the epidural group had a significantly higher intrapartum temperature, clinical chorioamnionitis, lengthier second stage, more fetal distress, and instrumental delivery.
A significantly higher number of neonates were admitted to NICU from the EA group (P<0.001, OR 1.89, 95% CI 1.45 to 2.46). Several studies that examined the association of EA with NICU admission found conflicting results. A 10 Years Retrospective study in Austria by Kraft et al18 observed an increased rate of NICU admission in the EA group. A similar result was seen in studies by Rouse et al,19 Herrera-Gómez et al8 and Wisborg et al.20
Conversely, a recent Cochrane meta-analysis by Anim-Somuah et al14 concluded that EA is not associated with a higher rate of NICU admission. Previous studies by Wang et al62 and Soncini et al21 also did not find an association between EA and NICU admission. The difference in observation could be partially due to the difference in the NICU admission criteria of different institutions. Many institutions have observation rooms attached to the delivery rooms, facilitating short-term observation. Our facility allows observation in the delivery room for up to 2 hours. As intravenous medications are not administered in the postnatal ward, all babies requiring intravenous therapy were admitted to NICU.
The chief reasons for NICU admission included suspected neonatal sepsis, post-resuscitation observation, observation of significant birth injuries, transient tachypnea, and meconium aspiration.
Admissions due to suspected maternal chorioamnionitis were significantly higher in the epidural group (P<0.001, OR 4.30, 95% CI 2.44 to 7.58). Abramovici et al69 found a strong correlation between EA and clinical chorioamnionitis in the mother (OR 8.3, 95% CI 2.63–26.40).
Neonates born in the EA group are more likely to receive antibiotics on the first day of life (P<0.001, OR 2.06,95% CI 1.47 to 2.79). They were also more likely to receive antibiotics for more than five days (P=0.01, OR 12.42, 95% CI 1.68–92.5). None of the babies had a positive blood culture. We did not find any published studies which compared the antibiotic duration. EA is associated with significant intrapartum temperature elevation.2,10,11 Intrapartum maternal fever increases the likelihood of neonatal admission for sepsis evaluation. Many of the previous researches demonstrated the association between EA and antibiotic use in neonates. A large population-based study by White et al13 found that neonates born to women who received an epidural had 1.26 times increased odds of antibiotic treatment. Lieberman et al,28 Goetzl et al,63 Heesen et al,29 and Wisborg et al20 found similar association. In the long term, antibiotic exposure is associated with necrotizing enterocolitis and altered gut microbiome22–25. Altered neonatal gut microbiome may increase the risks of chronic diseases like atopy.26,27
Kaul et al30 did not find any association between EA and antibiotic use in neonates. Capogna31 suggested that, while the number of neonates receiving sepsis evaluations varies between institutions, epidural exposure did not increase the incidence of neonatal sepsis.
Interestingly, the increased risk for NICU admission persisted even when the mothers without temperature elevation (<37.5 °C) were analyzed separately (P<0.001, OR 1.68,95% CI 1.26–2.24). Goetzl et al63 studied the rate of neonatal sepsis evaluation among mothers who received epidural analgesia and remained afebrile. They found that neonatal sepsis evaluation rate was higher in the epidural group even when the mothers were afebrile (OR 3.1, 95% CI 2–4.7).
More newborns in the EA group had admission temperature >37.5 °C (P=0.04, OR 3.40, 95% CI 1.00 to 11.49). Fetal temperature increases proportionate to the maternal temperature.68 Kaul et al,30 Wasson et al,71 and Agakidis et al72 also observed neonatal temperature elevation in association with EA.
Neonatal Birth injuries were more frequent in the EA group. (P=0.024, OR 1.71, 95% CI 1.06 to 2.74). Armani et al32 observed a significantly higher incidence of cephalhematoma in the EA group. In our study, mothers who received EA had more instrumental deliveries (P<0.001, OR 2.13, 95% CI 1.69 to 2.68). Neonatal birth trauma is strongly correlated to be an operative vaginal delivery.36 Birth trauma was documented in 3.9 % of the whole sample. Cephalhematoma was the most frequent injury noted (40% of all birth injuries). Others included clavicle fracture, mild subgalleal bleeding, brachial plexus injury, significant scalp laceration, cut injuries, facial paralysis, and deep forceps mark with significant bruising.
In admitted babies, we looked for the predominant symptom during the first 24 hours. Respiratory distress was the most frequent symptom (54%). 22 % of babies were asymptomatic (admitted for post-resuscitation observation or suspected neonatal sepsis due to maternal chorioamnionitis). Remaining babies had hypoactivity, poor sucking or vomiting.
We found that babies from the EA group were significantly more likely to have respiratory distress during the first 24 hours (P=0.01, OR 1.49, 95% CI 1.07 to 2.07). Although the need for oxygen was slightly more in the epidural group (P=0.04, OR 1.44, 95% CI 1.01 to 2.07), there was no difference in the need for mechanical ventilation. (P=0.25).
Kumar et al33 conducted a case-control study of NICU admitted babies. They found that Epidural analgesia increased the incidence of respiratory distress in the immediate newborn period.
Two babies from EA and one baby from non-EA group developed seizure during the first 24 hours. Greenwell34 observed increased encephalopathy and neonatal seizures with EA. This was correlated to the maternal temperature elevation. Wisborg et al20 also observed a higher incidence of neonatal convulsions with epidural analgesia. A study by Tornell et al2 found an association between EA and neonatal encephalopathy. Wang et al67 examined the neonatal adaptive score at 2 hours and 24 hours. No difference was observed between EA and non-EA group.
Among admitted babies, symptoms like poor sucking (P=0.26) hypoactivity (P=0.79) and vomiting (P=1) were not different between the groups. The mean length of stay was also comparable (P=0.51).
Mothers who received EA had a lengthier second stage (P<0.001). The recent Cochranemeta-analysis by Anim-Somuah et al14 had confirmed this observation. Many previous studies had similar findings.35–37 Zhang et al38 and Mousa et al39 did not find any association between EA and prolonged second stage. In our study, Instrumental vaginal deliveries were more frequent in the EA group (P<0.001, OR 2.13, 95% CI 1.69 to 2.68). The vast majority of previous studies had observed this association between EA and increased instrumental delivery.6,7,14,15,36,40 However, the post hoc subgroup analysis of a recent Cochrane review14 showed that this effect is not seen in recent studies (after 2005), suggesting that modern approaches to epidural analgesia in labor did not increase this outcome.
Pathological CTG (baseline fetal heart rate <100, reduced or increased variability/sinusoidal pattern, repetitive late or prolonged decelerations) findings were more frequent in the epidural group (P<0.001, OR1.65, 95% CI 1.30 to 1.98).
Neuraxial analgesia during labor has been associated with fetal heart rate (FHR) abnormalities with an incidence ranging from 4% to 21%.41–47 One of the suggested mechanisms of fetal bradycardia is that the rapid onset of analgesia can lead to an imbalance of plasma adrenaline and noradrenaline, which may result in uterine hypertonus. Other proposed mechanisms include hypotension and aortocaval compression. A study by Leighton et al17 did not find any association between EA and fetal heart rate changes.
Maternal temperature >37.5°C was significantly more frequent in the EA group (P<0.001, OR 7.40, 95% CI 3.93 to 13.69). Most of the previous studies observed this relationship.2,11,14,48 The maternal temperature of more than 37.5°C is strongly associated with neonatal encephalopathy.12 The proposed mechanisms of epidural induced fever include inflammatory response, oxidative stress, alteration in sympathetic stimulation, and subclinical chorioamnionitis. Patients with suspected chorioamnionitis were significantly higher in the epidural group (P<0.001 OR 4.30, 95% CI 2.44 to 7.58). This is attributable to the higher rate of elevated maternal temperature in the EA group. Confirmatory tests for chorioamnionitis (placental culture or histopathology) were done only in 51% clinical chorioamnionitis. There was no difference in the number of confirmed chorioamnionitis between the epidural and nonepidural groups (P=0.62). This may be explained by the fact that epidural analgesia and maternal fever are associated with a higher rate of histologic chorioamnionitis.70
Meconium staining of the amniotic fluid may be a sign of fetal hypoxia. We compared the rate of meconium-stained fluid between the two groups. We found a statistically significant association between EA and meconium-stained amniotic fluid (P=0.01, OR 1.31, 95% CI 1.05 to 1.62) Kism et al49 found a higher rate of meconium-stained fluid in association with EA. But the majority of previous studies did not find any association between EA and meconium-stained amniotic fluid.17,50,51
The rate of LSCS was similar in EA and non-EA groups. (P=0.72, OR 1.03, 95% CI 0.84 to 1.26). Although some of the previous studies have reported a higher rate of LSCS with EA,52 the vast majority of studies showed that EA is not associated with an increase in the LSCS rate.14,49,53–55
Low cord arterial pH is a significant risk factor for neonatal mortality, hypoxic-ischemic encephalopathy, intraventricular hemorrhage, and periventricular leucomalacia.55 We did not find any association between EA and cord arterial pH <7.1 (P=0.75, OR 0.90, 95% CI 0.49 to 1.64). Majority of previous studies had similar observation.7,17,18,56–58 Hintz et al59 and Tawhid Soderholm et al15 found a decrease in cord arterial pH <7.1 in association with EA. One study19 observed better cord pH in patients with EA.
We did not find any association between EA and Apgar score <7 at 1 minute (P=0.12, OR 1.71 95% CI 0.85 to 3.41). At 5 minutes, only 3 patients had an Apgar score <7. Apgar score at 5 minutes <7 is significantly associated with neurological disability, which may persist years postnatally.60 Almost all the previous studies on neonatal effects of EA examined Apgar score at birth. Our findings on Apgar score correlate well with the majority of the previous studies. These include the recent Cochrane analysis by Anim-Somuah14 and many other studies.6,7,17,54,61 None of them found any correlation between EA and 5 minute Apgar score. A recent study by Wang et al62 also found no association between EA and Apgar score at one or 5 minutes. The correlation of low 1 minute Apgar with epidural analgesia observed by Hincz Petal59 and Herrera-Gómez et al8 might be attributable to the difference in the opioid used.
We examined the need for any positive pressure ventilation at birth. There was no difference between the groups (P=0.05, OR 1.57, 95% CI 0.99 to 2.49) Herrera-Gomez et al8 and Greenwell et al34 observed the increased need for any assisted ventilation in the EA group. Antonio et al7 and Naito et al58 looked for the need for advanced resuscitation and did not find any difference between the groups.
There is strong evidence that EA is associated with maternal fever.2,6,14,48 Hence there is a theoretical possibility that the inflammatory response aroused by EA may extend to the fetus and hence may affect the White cell, platelets or C reactive protein. We compared the lab parameters of the neonates. There was no difference in the mean white cell count (P=0.32), mean platelet count (P=0.38) and C reactive protein >10 mg/dL (P=0.845). Our search did not identify any published study which looked for the association between EA and these parameters.
Conclusion
Our study suggests that labor EA adversely affects the short-term neonatal outcome. It increases the NICU admission rate, antibiotic exposure, neonatal birth injuries, respiratory distress, and need for oxygen in the first 24 hours of life. But no effects were observed on the Apgar score, need for resuscitation, mechanical ventilation rate, and neonatal lab parameters. Mothers on epidural analgesia had a prolonged second stage of labor, a higher percentage of instrumental delivery, meconium-stained amniotic fluid and fever. The need for Caesarian delivery remains unaffected. Healthcare staff needs to provide information on this topic to all pregnant women who request for EA. The main limitation of this study is the retrospective design. Well-designed prospective studies addressing the safety of EDA are needed.
Abbreviations
EA, Epidural Analgesia; NICU, Neonatal Intensive Care Unit; AWH, Al Wakra Hospital; CSE, Combined Spinal Epidural analgesia.; LSCS, Lower segment Caesarian Section; STD, Sexually transmitted diseases; GBS, Group B Streptococcus; OR, Odds Ratio; CI, Confidence Interval; SD, Standard Deviation.
Acknowledgments
We owe our deep gratitude to the staff of the Medical Research Centre (MRC) for their continuous support throughout the study. We would like to recognize the invaluable assistance from Dr. P. Chandra of MRC during design and statistical analysis. We express our heartfelt appreciation to Ms. Manjulabhama OM, Ms. Amal GA Shakweer and Ms. Cinderella Zapa for their kind assistance in data collection and entry.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sandstrom A, Altman M, Cnattingius S, et al. Durations of second stage of labor and pushing and adverse neonatal outcomes: a population-based cohort study. J Perinatol. 2017;37:236. doi:10.1038/jp.2016.214
2. Tornell S, Ekeus C, Hultin M, Hakansson S, Thunberg J, Hogberg U. Low Apgar score, neonatal encephalopathy, and epidural analgesia during labour: a Swedish registry-based study. Acta Anaesthesiologica Scandinavica. 2015;59:486–495.
3. Leiberman E, Lang J, Richardson DK, Frigoleto FD, Heffner LJ, Cohen A. Intrapartum maternal fever and neonatal outcome. Pediatrics. 2000;105:8–13.
4. Volmanen P, Sarvela J, Akural EI, Raudaskoski T, Korttila K, Alahuhta S. Intravenous remifentanilvs. epidural levobupivacaine with fentanyl for pain relief in early labour: a randomised, controlled, double-blinded study. Acta Anaesthesiol Scand. 2008;52:249–255. doi:10.1111/aas.2008.52.issue-2
5. Madden K, Middleton P, Cyna AM, Matthewson M, Jones L. Hypnosis for pain management during labour and childbirth. Cochrane Database Syst Rev. 2016;5CD009356.
6. Anim-Somuah M, Smyth RM, Jines L. Epidural versus non-epidural or no analgesia in labor. Cochrane Database Syst Rev. 2011;12:CD000331.
7. Antonio HM, Julian JR, Maria MC, María UB, Milagros MA, Juan GS. Epidural analgesia and neonatal morbidity: a retrospective cohort study. Int J Environ Res Publ Health. 2018;15(10):2092. doi:10.3390/ijerph15102092
8. Herrera GA, Garcia MO, Ramos TJ, De Luna BE, Ruiz C, Ocana PFM. A retrospective study of the association between epidural analgesia during labour and complications for the newborn. Midwifery. 2015;31:613–636. doi:10.1016/j.midw.2015.02.013
9. Li Y, Hu C, Fan Y, Wang H, Xu H. Epidural analgesia with amide local anesthetics, bupivacaine, and ropivacaine in combination with fentanyl for labor pain relief: a meta-analysis. Med Sci Monit. 2015;21:921–928.
10. Segal S. Labour epidural analgesia and maternal fever. Anesth Analg. 2010;111:1467–1475.
11. Goetz L, Rivers J, Zinghelboim I, Wali A, Badell M, Suresh MS. Intrapartum epidural analgesia and maternal temperature regulation. Obstet Gynecol. 2007;109:687–689. doi:10.1097/01.AOG.0000255976.14297.f6
12. Impley L, Greenwood C, MacQuillan K, Reynolds M, Sheil O. Fever in labour and neonatal encephalopathy: a prospective cohort study. BJOG. 2011;108:594–597.
13. White A, Olson D, Messacar K. A statewide assessment of association between epidural analgesia, maternal fever, and neonatal antibiotics in Colorado 2007–2012. Arch Dis Fetal Neonatal Ed 2017 Mar. 2012;102(2):F120–F125. doi:10.1136/archdischild-2015-309985
14. Anim-Somuah M, Smyth RMD, Cyna AM, Cuthbert A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst Rev. 2018;5:CD000331.
15. Tawhid Soderholm N, Turkmen S .Impact of epidural analgesia in labour on neonatal and maternal outcomes. Open J Obstetrics Gynecol. 2018;8:767–779. doi:10.4236/ojog.2018.89080
16. Cordero L, Treuer SH, Landon MB, Gabbe SG. Management of infants of diabetic mothers. Arch PediatrAdolesc Med. 1998;152:249.
17. Leighton BL, Halpern SH. The effects of epidural analgesia on labour, maternal, and neonatal outcomes: a systemic review. Am J Obstet Gynecol. 2002;186:S69–S77. doi:10.1067/mob.2002.121813
18. Kraft F, Wohlrab P, Kiss H, Helmer H, Klein KU. Epidural anesthesia during routine childbirth: a 10 years retrospective analysis from the national birth registry Austria. AINS. 2018;53(S 01):S8.
19. Rouse DJ, Weiner SJ, Bloom SL, et al. Second-stage labor duration in nulliparous women: relationship to maternal and perinatal outcomes. Am J Obstet Gynecol. 2009;201:357e1–7. doi:10.1016/j.ajog.2009.08.003
20. Wisborg K, Hansen AK, Henriksen TB. Intrapartum epidural analgesia and adverse neonatal outcome. Arch Dis Child. 2008;93:pw195.
21. Soncini E, Grignaffini A, Anfuso S, Cavicchioni O. Epidural analgesia during labour: maternal, fetal and neonatal aspects. Minerva Ginecol. 2003;55(3):263–269.
22. Alexander VN, Northrup V, Bizzarro MJ. Antibiotic exposure in the newborn intensive care unit and the risk of necrotizing enterocolitis. J Pediatr. 2011;159:392–397. doi:10.1016/j.jpeds.2011.02.035
23. Penders J, Thijs C, Vink C, et al. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006;118:511–521. doi:10.1542/peds.2005-2824
24. Tanaka S, Kobayashi T, Songjinda P, et al. Influence of antibiotic exposure in the early postnatal period on the development of intestinal microbiota. FEMS Immunol Med Microbiol. 2009;56:80–87. doi:10.1111/fim.2009.56.issue-1
25. Weintraub AS, Ferrara L, Deluca L, et al. Antenatal antibiotic exposure in preterm infants with necrotizing enterocolitis. J Perinatol. 2012;32:705–709. doi:10.1038/jp.2011.180
26. MurgasTorrazza R, Neu J. The developing intestinal microbiome and its relationship to health and disease in the neonate. J Perinatol. 2011;31(Suppl 1):S29–34. doi:10.1038/jp.2010.172
27. Van Nimwegen FA, Penders J, Stobberingh EE, et al. Mode and place of delivery, gastrointestinal microbiota, and their influence on asthma and atopy. J Allergy Clin Immunol. 2011;128:948–955. doi:10.1016/j.jaci.2011.07.027
28. Lieberman E, Lang JM, Frigoletto F
29. Heesen M, Klohr S, Van deVelde M. Labour epidural analgesia and anti-infectious management of the neonate: a meta-analysis. J Perinat Med. 2012;40(6):625–630. doi:10.1515/jpm-2012-0064
30. Kaul B, Vallejo M, Ramanathan S, Mandell G. Epidural labor analgesia and neonatal sepsis evaluation rate: a quality improvement study. Anesth Analg. 2001;93:986–990.
31. Capogna G, Camorica M. Epidural analgesia for childbirth: effects of newer techniques on neonatal outcome. Paediatr Drugs. 2004;6:375–386.
32. Armani M, Gaggiano C, Dallaglio S, Romanini E, Sospiri C, Magnani C. Are there any strategies to improve neonatal outcomes associated with epidural analgesia in labour? Acta Biomed. 2013;84:117–123.
33. Kumar M, Chandra S, Ijaz Z, SenthilSelvan A. Epidural analgesia in labour and neonatal respiratory distress: a case-control study. Arch Dis Child Fetal Neonatal Ed. 2014;99(2):F116–F119. doi:10.1136/archdischild-2013-304933
34. Greenwell EA, Wyshak G, Ringer SA, Johnson LC, Rivkin MJ, Lieberman E. Intrapartum temperature elevation, epidural use, and adverse outcome in term infants. Pediatrics. 2012;129:E447–E454. doi:10.1542/peds.2010-2301
35. Zimmer EZ, Jakobi P, Itskovitz-Eldor J, et al. Adverse effects of epidural analgesia in labour. Eur J Obstet Gynecol Reprod Biol. 2000;89:153–157. doi:10.1016/S0301-2115(99)00191-8
36. Sharma SK, McIntire DD, Wiley J, Leveno KJ. Labour analgesia and cesarean delivery: an individual patient meta-analysis of nulliparous women. Anesthesiology. 2004;100(1):142–148. doi:10.1097/00000542-200401000-00023
37. Fernandez G. Obstetric epidural analgesia: the relationship between obstetric variables and the course of labour. Rev Esp Asnestesiol Reanim. 2004;51:121–127.
38. Zhang M, Yang HX, Li HY, Shi HX, Qu Y. Influence of combined spinal-epidural analgesia and epidural analgesia on the progress of labour. Zhonghua Fu Chan KeZaZhi. 2005;40:365–368.
39. Mousa WF, Al-Metwalli R, Mostafa M. Epidural analgesia during labour vs. no analgesia: a comparative study. Saudi J Anaesth. 2012;6:36–40. doi:10.4103/1658-354X.93055
40. Liu EHC, Sia ATH. Rates of cesarean section and instrumental vaginal delivery in nulliparous women after low concentration epidural infusions or opioid analgesia: a systematic review. BMJ. 2004;328(7453):1410. doi:10.1136/bmj.38097.590810.7C
41. Demissie K, Rhoads GG, Smulian JC, et al. Operative vaginal delivery and neonatal and infant adverse outcomes: population-based retrospective analysis. BMJ. 2004;329(7465):24–29. doi:10.1136/bmj.329.7456.24
42. Nielsen PE, Erickson JR, Abouleish EI, Perriatt S, Sheppard C. Fetal heart rate changes after intrathecalsufentanil or epidural bupivacaine for labor analgesia: incidence and clinical significance. Anesth Analg. 1996;(1996(83):742–746. doi:10.1213/00000539-199610000-00014
43. Palmer CM, Maciulla JE, Cork RC, Nogami WM, Gossler K, Alves D. The incidence of fetal heart rate changes after intrathecal fentanyl labor analgesia. Anesth Analg. 1999;(1999(88):577–581. doi:10.1213/00000539-199903000-00021
44. Carvalho B, Fuller AJ, Brummel C, Durbin M, Riley ET. Fetal oxygen saturation after combined spinal-epidural labor analgesia: a case series. J Clin Anesth. 2007;19:476–478. doi:10.1016/j.jclinane.2007.01.009
45. Vercauteren M, Bettens K, Van Springel G, Schols G, Van Zundert J. Intrathecal labor analgesia: can we use the same mixture as is used epidurally? Int J Obstet Anesth. 1997;6:242–246. doi:10.1016/S0959-289X(97)80031-3
46. Van de Velde M, Vercauteren M, Vandermeersch E. Fetal heart rate abnormalities after regional analgesia for labor pain: the effect of intrathecalopioids. Reg Anesthesia Pain Med. 2001;26:257–262.
47. Patel NP, El-Wahab N, Fernando R, et al. Fetal effects of combined spinal-epidural vs. epidural labour analgesia: a prospective, randomized double-blind study. Anaesthesia. 2014;69:458–467. doi:10.1111/anae.12602
48. Dashe JS, Rogers BB, McIntire DD, Leveno KJ. Epidural analgesia and intrapartum fever: placental findings. Obstet Gynecol. 1999;93(3):341–344. doi:10.1016/s0029-7844(98)00415-3
49. Kim SK, Friedman P, Madan I, Haltigin C, Arrow M, Ogunyemi D. Term meconium stained amniotic fluid: maternal and neonatal risks. Obstetrics Gynecol. 2018;131:157S. doi:10.1097/01.AOG.0000533115.08057.34
50. Angeliki Antonakou DP. The effect of epidural analgesia on the delivery outcome of induced labour: a retrospective case series. Obstet Gynecol Int. 2016;2016:5740534.
51. Li JZ, Wang MS, Ji XH, et al. Efficacy and delivery outcomes of women underwent double-catheter epidural block during labor. Ma FGZhonghua Fu Chan KeZaZhi. 2010;45(11):81924.
52. Liang CC. Does intrapartum epidural analgesia affect nulliparous labour and postpartum urinary incontinence? Chang GUNG Medical J. 2007;30:161–167.
53. Deshmukh VL, Ghosh SS, Yelikar KA, Gadappa SN. Effects of epidural labour analgesia in mother and foetus. J Obstetrics Gynecol India. 2018;68(2):111–116. doi:10.1007/s13224-017-1063-7
54. Dipti Agrawal B, ManjeetArora A, Gurha P. The effect of epidural analgesia on labour, mode of delivery and neonatal outcome in nullipara of India. J ClinDiagn Res. 2014;8(10):OC03–OC06.
55. Malin GL, Morris RK, Khan KS. Strength of association between umbilical cord pH and perinatal and long term outcomes: systematic review and meta-analysis. BMJ. 2010;340:c1471. doi:10.1136/bmj.c1471
56. Newton ER, Schroeder BC, Knape KG, Bennett BL. Epidural analgesia and uterine function. Obstet Gynecol. 1995;85:749–755.
57. Lieberman E, O’Donoghue C. Unintended effects of epidural analgesia during labor: a systematic review. Am J Obstetrics Gynecol. 2002;186:S31–S68. doi:10.1016/S0002-9378(02)70181-6
58. Naito Y, Ida M, Yamamoto R, Tachibana K, Kinouchi K, The effect of labor epidural analgesia on labor, delivery, and neonatal outcomes: a propensity score-matched analysis in a single Japanese institute. JA Clin Rep. 2019;5:40. doi:10.1186/s40981-019-0260-z
59. Hincz P, Podciechowskil L, Grzesiak M, Horzelski W, Wilczyflski J. Epidural analgesia during labor: a retrospective cohort study on its effects on labour, delivery, and neonatal outcome. Ginekol Pol. 2014;85(12):923–928. doi:10.17772/gp/1883
60. Ehrenstein V. Association of Apgar scores with death and neurologic disability. Clin Epidemiol. 2009;1:45–53. doi:10.2147/CLEP
61. Anim-Somuah M, Smyth R, Howell C. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2005;4:CD000331.
62. Wang Q, Zheng S-X, Yu-Fei N, Lul Y-Y, Zhang B, Hu Q-QLM-P. The effect of labor epidural analgesia on maternal-fetal outcomes: a retrospective cohort study. Arch Gynecol Obstet. 2018;298(1):89–96. doi:10.1007/s00404-018-4777-6
63. Goetzl L, Cohen A, Frigoletto F
64. Simmons SW, Taghizadeh N, Dennis AT, et al. Combined spinal-epidural versus epidural analgesia in labour. Cochrane Database Syst Rev. 2012;10:CD003401.
65. MichaelWeindling A. Offspring of diabetic pregnancy: short-term outcomes. Semin Fetal Neonatal Med. 2009;14:111. doi:10.1016/j.siny.2008.11.007
66. Yang J, Cummings EA, O’connell C, Jangaard K. Fetal and neonatal outcomes of diabetic pregnancies (2006). Obstet Gynecol. 2006;108:644.
67. Wang K, Cao L, Deng Q, et al. The effects of epidural/spinal opioids in labour analgesia on neonatal outcomes: a meta-analysis of randomized controlled trials. Can J Anaesth. 2014;61:695–709. doi:10.1007/s12630-014-0185-y
68. Morishima HO, Glaser B, Niemann WH, James LS. Increased uterine activity and fetal deterioration during maternal hyperthermia. Am J Obstet Gynecol. 1975; 121:531–539.
69. Abramovici A, Szychowski JM, Biggio JR, Sakawi Y, Andrews WW, Tita AT. Epidural use and clinical chorioamnionitis among women who delivered vaginally. Am J Perinatol. 2014;31(11):1009–1014. doi:10.1055/s-00000009
70. Roberts DJ, Celi AC, Riley LE, et al. Acute histologic chorioamnionitis at term: nearly always noninfectious. PLoS One. 2012;7(3):e31819. doi:10.1371/journal.pone.0031819
71. Wassen MMLH, Winkens B, Dorssers EMI, Marcus MA, Moonen& RMJ, Roumen FJME. Neonatal sepsis is mediated by maternal fever in labor epidural analgesia. J Obstet Gynaecol (Lahore). 2014;34(8):679–683. doi:10.3109/01443615.2014.925858
72. Agakidis C, Agakidou E, Philip Thomas S, Murthy P, John Lloyd D. Labor epidural analgesia is an independent risk factor for neonatal pyrexia. J Maternal Fetal Neonatal Med. 2011;24:1128–1132. doi:10.3109/14767058.2010.545923
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.