")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Effects of desensitizing dentifrices on the reduction of pain sensitivity caused by in-office dental whitening: a double-blind controlled clinical study
Authors Pierote JJA, Barbosa IF, Prieto LT, Lima DANL , Paulillo LAMS, Aguiar FHB
Received 20 December 2018
Accepted for publication 18 April 2019
Published 29 July 2019 Volume 2019:11 Pages 219—226
DOI https://doi.org/10.2147/CCIDE.S198940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Josué Junior Araujo Pierote, Isabel Ferreira Barbosa, Lúcia Trazzi Prieto, Débora Alves Nunes Leite Lima, Luís Alexandre Maffei Sartini Paulillo, Flávio Henrique Baggio Aguiar
Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas (UNICAMP), Piracicaba, São Paulo, Brazil
Objective: The purpose of this study was to clinically evaluate the influence of desensitizing dentifrices applied through a plastic tray on reducing the pain sensitivity and color variation caused by in-office dental whitening and to evaluate differences among such dentifrices through a controlled double-blind clinical study.
Materials and methods: A prospective study was conducted with 48 individuals between 18 and 30 years without gender distinction. For the dental whitening, 35% hydrogen peroxide was used in three clinical sessions. After each whitening session, the volunteers used a plastic tray containing one of the dentifrices (sucralose– S, sodium fluoride – SF, arginine and calcium carbonate – ACC, and 5% potassium nitrate – PN) for 4 hrs during the night. The evaluation of the sensitivity associated with the use of the plastic tray in each whitening session was performed using the analog numerical scale with scores from 0 to 10. The color variation (ΔE) was determined with a spectrophotometer. The pain sensitivity data were submitted to the multivariate analysis of variance with repeated measurements and a Lambda Wilks test (p<0.05). To analyze the color variation, a one-way ANOVA was applied (p<0.05).
Results: The ACC and 5% NP groups showed a reduction in sensitivity in relation to the other groups (p<0.05). There was a reduction in sensitivity after placement of the tray with dentifrice. The color evaluation associated with the dentifrice showed no difference (p=0.9186).
Conclusion: The use of desensitizing dentifrices with ACC or 5% NP in a plastic tray was effective for the reduction of pain sensitivity, and the use of a desensitizing dentifrice did not decrease the effectiveness of whitening.
Keywords: tooth whitening, dentifrice, sensitivity
Introduction
The color of teeth depends on their intrinsic and extrinsic coloration. Intrinsic staining is associated with light reflection and absorption by enamel and dentin. The main causes of intrinsic tooth darkening are aging, pulpal necrosis, fluorosis and the use of drugs such as tetracycline.1 Furthermore, extrinsic darkening is associated with accumulation of stains on the enamel surface2,3 caused by consumption of coffee, tea, red wine, carrots, oranges and tobacco.3,4
Vital whitening is a conservative and noninvasive alternative for aesthetic alteration of the smile when compared to other clinical techniques, eg, enamel microabrasion, direct restorations, ceramic veneers and prosthetic crowns.1,5,6 Dental whitening is a conservative technique and has shown a high success rate in the treatment of darkened teeth.7,8
Gingival irritation and teeth sensitivity are the collateral effects most frequently reported during the whitening, although they are usually mild and transient.1,7–10 However, such collateral effects can be more intense and motivate the patients to give up the whitening.11–13
Among the explanations for whitening related pain, the Brännström’s hydrodynamic theory is the most accepted.14 This theory suggests that dental sensitivity might be caused by fluid movement in the dentinal tubules.15 This movement would activate nociceptors and result in the perception of pain.1,15 Moreover, the diffusion of hydrogen peroxide through the enamel and dentin reaching the pulp, and the acidic pH of the whitening gel may cause transient painful sensitivity.6,12,16,17
Some techniques can be used to eliminate such collateral effects. Among these are the reduction of the concentration of hydrogen peroxide, administration of painkillers and anti-inflammatories, and use of desensitizers.7,11,18 However, such techniques are usually used in the dental office with no recommendations for the patient regarding what to do at home to minimize the effects of pain sensitivity posttreatment.7,11
There are different dentifrices on the market for attenuating tooth sensitivity.19–22 In addition to this indication, such dentifrices may aid in reducing and/or eliminating dental sensitivity caused by the whitening treatment. Thus, desensitizing dentifrices can be an option to reduce the adverse effects of whitening agents18–20 because they decrease the excitability of nerve fibers present in the pulp or promote the obliteration of dentin tubules.22 The reduction of excitability in the nerve fibers occurs due to the diffusion of potassium salts through the enamel and dentin. The potassium salts reach the nerve endings and affect the transmission of the nerve impulses,11,19 reducing or eliminating the pain through the action of substances containing potassium nitrate (PN).21 On the other hand, the occlusion of dentinal tubules reduces the permeability of the dentin and blocks the hydrodynamic mechanism by means of substances containing sodium fluoride (SF) or arginine and calcium carbonate (ACC).21
However, during oral hygiene, the desensitizing dentifrices remain in contact with the tooth for a short time, which may not be enough to eliminate or reduce the pain sensitivity caused by in-office dental whitening. Thus, there is a need for methods that complement toothbrushing with desensitizing dentifrices.7,11 Due to this, the use of desensitizing dentifrices in a plastic tray may be a new alternative to reduce the pain sensitivity caused by dental whitening.7,11
The advantages of applying desensitizing dentifrices to a plastic tray are the ease of making the tray by the dentist, the low cost of both the plastic tray and the dentifrice, the ease of use by the patient at home, and the possibility of using the same plastic tray for at-home whitening and mixed technique.7,11
The objective was to clinically evaluate the influence of desensitizing dentifrices applied through a plastic tray on reducing the pain sensitivity and color variation caused in-office dental whitening through a controlled double-blind clinical study. Our hypothesis was that the use of dentifrices with a plastic tray could reduce the dental sensitivity due to the longer time of contact with the dental surface without interfering with the color variation.
Materials and methods
Ethical approval
This study was submitted to and approved by the research ethics committee of the Piracicaba Dental School (FOP-UNICAMP) affiliated with the National Commission for Research Ethics of Brazil (CONEP) according to protocol number 104/2015. The Clinical Trials Register (ClinicalTrials) was obtained with the protocol number NCT03019224. All the volunteers signed a free informed consent form. Clinical Trials was reported according to the CONSORT Statement standard protocol. This study was descriptive and was conducted in full accordance with the World Medical Association Declaration of Helsinki.23
Tested materials
Four types of dentifrices were used for the study of desensitizing dentifrices used in the plastic tray (Table 1).
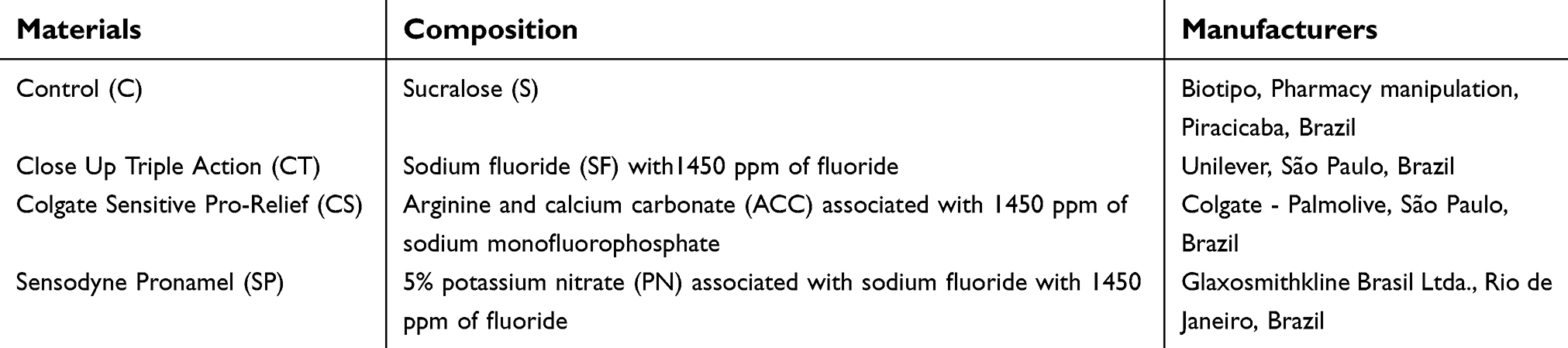 |
Table 1 Materials and composition used in study with desensitizing dentifrices applied in plastic tray |
Experimental design
This is a double-blind controlled study using volunteers (48) who were randomly divided into four groups. The sample calculation was applied, and a sample of 12 volunteers per group resulted. The dentifrice was studied at four levels that consisted of three experimental levels and one control level. The response variables were numerical analog scale and color variation (ΔE).
Selection and preparation of the volunteers
Patients who came to the postgraduate dental clinic for whitening were invited to participate in the study. They were informed by the researcher (dentist) about all the aspects of the study, including the fact that they might discontinue their participation at any moment during the treatment. In addition, it was made clear that their participation was voluntary and that refusal to participate would not result in any penalty or loss of benefits.
If the patient chose to participate in the study, they had to sign a free informed consent form before the clinical evaluation was started.
The criteria for selection and exclusion of the volunteers were as follows: (1) Inclusion criteria: age of 18–30 years, good oral and general health, noncarious anterior tooth with color shade higher than A2 in the Vita Classic scale (VITA Zahnfabrink, Bad Säckingen, Germany). (2) Exclusion criteria: smoker, pregnant or breastfeeding, previous dental whitening, parafunctional habits, dentin sensitivity and nonvital discoloration.
The general clinical evaluation of the volunteers was performed by asking them about their health conditions. A clinical mirror and probe were used for intraoral clinical examination and interproximal and periapical radiographs were taken for radiographic examination. This evaluation helped determine whether the patients met the inclusion criteria set in the study and resulted in a sample of 48 volunteers.
Supra-gingival scaling of calculus with periodontal curettes and root planning with rubber cups at low rotation and water/pumice paste was done to oral adequacy. Dental arches were molded with alginate (Hydrogum, Zhermack Clinical, Italy) to obtain a model (Herodent type III, Coltene, Rio de Janeiro, Brazil) for making the plastic tray, which was used in association with the dentifrices after the dental whitening sessions.
One week before starting the experiment, toothbrushes (Slim Soft, Colgate-Palmolive, São Paulo, Brazil) and standard dentifrice (Colgate Total 12, Colgate-Palmolive, São Paulo, Brazil) were given to each volunteer. The volunteers received guidelines on oral hygiene and recommendations to use only the dentifrice and toothbrush provided for oral hygiene until the start of the whitening sessions.
Clinical procedures
The evaluation of the tooth color was performed using a spectrophotometer (Easyshade, Vident, Brea, CA, USA). The color was analyzed with the tooth hydrated before the start of the first whitening session and one week after.
The spectrophotometer was always used in the same position as determined by a silicon guide (Express XT, 3M ESPE, Sumaré, SP, Brazil). An opening was made in the guide to the buccal surface of the upper left central incisor, allowing the color of the tooth to be evaluated with the tip of the spectrophotometer at the height of the middle third.
The color was determined by an EasyShade spectrophotometer and the data (L, a, b) were used in the CIELab system for indicating the following value: (E) Color comparison was made before the first and after the last treatment sessions, resulting in a difference between both colors (ΔE).3
The clinical procedures were performed under relative isolation using a lip retractor (Arcflex, FGM, Joinville, SC, Brazil) and dental cotton rollers to apply a gingival protection barrier (Top Dam, FGM, Joinville, SC, Brazil) extending from the right first molar to the left first molar in both arches.
The gingival protection barrier was placed over the margins and gingival papilla corresponding to the areas receiving the whitening gel with approximately 3 mm in height and photopolymerized for 20 s for each group of three teeth. Photoactivation was performed with high power LEDs (light intensity =600 mw/cm2) (RadiiCal, São Paulo, SP, Brazil).
The desensitizing gel containing 5% PN associated with 2% SF (Desensibilize KF 2%, FGM, Joinville, SC, Brazil) was applied with a microbrush (Brush KG, KG Sorensen, Cotia, SP) on the buccal surface from the right first molar to the left first molar in both arches and remaining for 10 mins.7 Then, the desensitizer was removed with a water jet and a disposable plastic suction cannula.
The handling of 35% hydrogen peroxide (Whiteness HP, FGM, Joinville, SC, Brazil) followed the manufacturer’s recommendations. The gel remained in contact with the buccal surface of the teeth for 15 mins and was removed with a disposable plastic suction cannula and water wash. This procedure was performed three times per clinical session. The volunteers underwent three whitening clinical sessions with a one-week interval between them.
During the clinical whitening sessions, each volunteer used an unidentified dentifrice corresponding to their experimental group. The experimental group was determined by means of a draw made by a dentist who did not participate in the study. Thus, the researcher (dentist) who provided the dentifrice and the volunteer were not aware of which experimental group the latter belonged to (ie, double blind).
After the first session, each volunteer received a plastic tray and instructions for using the dentifrice as described. The dentifrice should be placed in small quantities on the buccal side of the plastic tray at the region corresponding to the right first molar to the left first molar in both arches. The set was taken to the buccal cavity and pressed onto the buccal surface of the tooth until the dentifrice made contact with the tooth structure. Excessive dentifrice should be removed with dental cotton rolls and the volunteers used the plastic tray with dentifrice during sleep (for 4 hrs) on the same night that the whitening session was performed. The next morning, the patient washed and dried the plastic tray before storing it in the case. The volunteers received the guidelines for using the tray containing the specific dentifrice according to their experimental group only on the night of the whitening session. In addition, the volunteers should use the same dentifrice throughout the experiment.
For sensitivity analysis, we have used the numerical analog scale7 with scores ranging from 0 to 10 at six moments: before the placement of the tray in the first whitening session (S1), after placement of the tray in the first whitening session (S2), before the placement of the tray in the second whitening session (S3), after placement of the tray in the second whitening session (S4), before the placement of the tray in the third whitening session (S5), after placement of the tray in the third whitening session (S6). In relation to the dentifrices: Control (C), Close Up Triple Action (CT), Colgate Sensitive Pro-Relief (CS), Sensodyne Pronamel (SP) were used in the plastic tray.
Statistical analysis
For a sensitivity analysis, the multivariate analysis of variance test for repeated measurements and the Lambda Wilks test at a 5% probability level were used to determine the differences between the studied groups (C, CT, CS and SP) at the evaluation times (S1, S2, S3, S4, S5 and S6).
One-way ANOVA was applied for color variation (ΔE) in relation to the dentifrices C, CT, CS, SP used in the plastic tray.
In both tests, the Bioestat software 5.0 was used and values of p<0.05 were considered statistically significant.
Results
At the end of 4 weeks, 48 participants had completed the study and no participants had interrupted their participation (Figure 1).
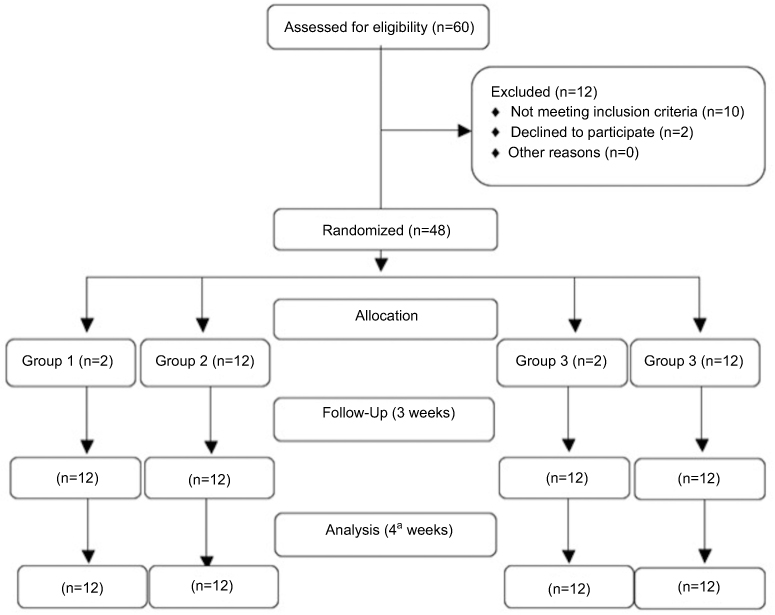 |
Figure 1 The consort flow chart. |
The groups were compared two by two, and the results showed that there was a statistically significant difference between C and SP (p=0.0001); CT and SP (p=0.0003); CS and C (p=0.0022); CS and CT (p=0.0062); CS and SP (p=0.0488). However, when comparing CT and C, there was no significant difference between them (p=0.9681).
Figure 2 illustrates the behavior of each dentifrice as a function of time. In this graph, it may be observed that after the application in the tray and a brushing with the active principles 5% PN (SP) and ACC (CS), there was a significant reduction of pain sensitivity. On the other hand, the same result did not occur with S (C) and the group with SF (CT). The dentifrice with 5% PN (SP) presented the greatest reduction in sensitivity after its application in the tray.
Figure 2 also shows that for sensitivity analyses in relation to application time, a significant reduction of sensitivity was found after placement of the plastic tray with dentifrice in each whitening session: the first – S2, the second – S4 and the third – S6 when it was compared to the application times before: the first – S1, the second – S3 and the third session – S5.
One-way ANOVA was applied for color evaluation in relation to each dentifrice and showed that there was no significant color difference after the whitening (p=0.9186) (Table 2).
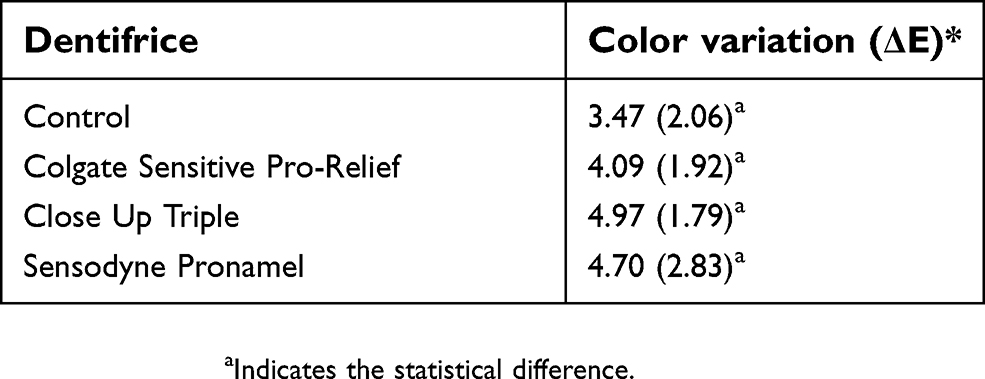 |
Table 2 Color variation (ΔE): means (standard deviations) and one-way ANOVA |
Discussion
The hypothesis that the use of dentifrices associated with a plastic tray could reduce dental sensitivity due to the longer time of contact with the dental surface, but without interfering in the color variation was accepted.
In relation to the dentifrice and time, it was observed that S (C) had results similar to those of group SF (CT). Sucralose is made from sugar and tastes like sugar; however, it is not recognized by the body as a carbohydrate and therefore has zero calories. In addition, it is not used as food by oral bacteria that cause dental caries and has no effect on sensitivity.24
One of the hypotheses that may explain the absence of a desensitizing effect of SF in the present study is that in three weeks the deposition of fluoride compounds in the dentin may not have been enough to obliterate tubules and to smooth the movement of fluids inside.24–26 The SF in small and constant concentrations only becomes able to reduce dentin sensitivity in the fourth week of use.25–27 This fact may be even more complicated when only the enamel is exposed, ie, in this study, there was no exposed dentin and direct contact occurred between the toothpaste and the enamel surface.
The S (C) present a significant difference in relation to dentifrices containing ACC (CS), which act by obliterating the canaliculus of the dentin, and thus prevent the movement of the dentin fluids and still assist in the remineralization of the dentin.24,28 The combination of ACC (CS) is capable of being deposited on surfaces of exposed dentin to physically block and seal the open dentinal tubules.25,26,29–31 This technology (CS) has shown that it physically promotes the obliteration and formation of a plug in the exposed dentinal tubules and is able to alleviate dentin hypersensitivity.25,26,29–31
This new technology provides clinically proven benefits for rapid and long-lasting relief from dentin hypersensitivity and demonstrates that ACC works together to accelerate the natural mechanisms of tubule occlusion and form a protective layer on the dentin surface.32 Clinical findings show that toothpastes containing ACC provide significant relief of dentin sensitivity.29,30
Sucralose (C) presents a significant difference in relation to dentifrices containing 5% PN (SP), which act by blocking the nerve activity of the nerve fibers of the pulp through the decrease of the sensory excitability of the nociceptors.4,5,19
PN diffuses through the enamel and dentin to the nerve endings of the sensory fibers, reducing the excitability of the nerve fibers by inhibiting the movement of the sodium and potassium ions around the sensory fibers. Thus, this results in modulation or suppression of pain sensation.21,22,28 Because of this mechanism, potassium salts have been suggested as an effective treatment for sensitivity caused by tooth whitening.19,28 The study demonstrates that the use of PN can be more effective than fluoride in reducing sensitivity after dental whitening, as in other studies.22,33
Reducing sensitivity during the period of tooth whitening is beneficial because it improves the patient’s comfort and commitment to the treatment.19,33 The use of a plastic tray with dentifrice has become an efficient procedure in reducing the sensitivity caused by in-office dental whitening. Our evaluation of sensitivity in relation to the application time has shown that sensitivity values after placement of the tray (S2, S4, S6) were different and significantly lower at all application times. This happened because the use of the plastic tray allowed for longer contact time between the dentifrice and the dental surface which inhibited the pain.22,28,33
Therefore, dentifrices did not influence the results of whitening since no significant difference in color shades was observed between the groups evaluated. It was expected that the dentifrice containing ACC (CS) could influence the diffusion of the whitening gel due to its mechanism of action, which is similar to that of fluoride, because both promote the obliteration of dentinal tubules and the modification of enamel permeability.34 However, the hydrogen peroxide molecule is very small and can penetrate the interstitial spaces between the enamel prisms. This probably explains the similar results of color variation after whitening obtained for the different groups.7,35,36,37
This study has shown an effective alternative for reducing the pain sensitivity associated with tooth whitening by using dentifrice in a plastic tray.
The limitations associated with the present study are related to the need for observing the volunteers for a longer period of time in order to evaluate the sensitivity and color stability after the whitening. This will require further studies with longer follow-up periods.
Conclusions
The use of desensitizing dentifrice containing 5% PN or ACC in a plastic tray was effective in reducing the pain sensitivity caused by in-office dental whitening.
The dentifrices used in this study did not affect the efficacy of the hydrogen peroxide used in the in-office whitening.
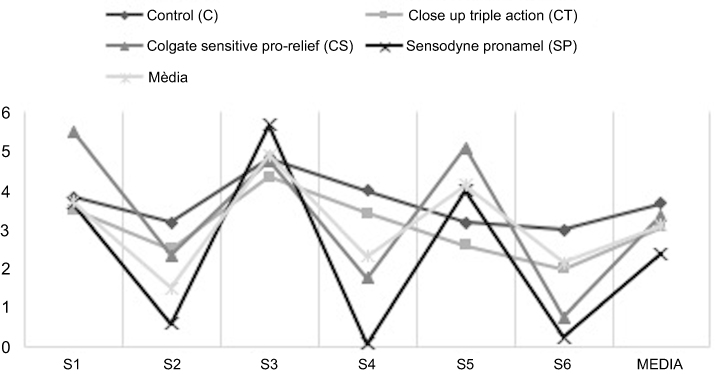 |
Figure 2 Mean and standard deviations for interaction dentifrice and time. |
Acknowledgments
The authors are grateful to CAPES (Coordination for the Improvement of Higher Education Personnel) for the financial support via scholarship.
Disclosure
LTP reports grants from CAPES. The authors report no other conflicts of interest in this work during the conduct of the study.
References
1. Charakorn P, Cabanilla LL, Wagner WC, et al. The effect of preoperative ibuprofen on tooth sensitivity caused by in-office bleaching. Oper Dent. 2009;34:131–135. doi:10.2341/08-33
2. Da Costa JB, McPharlin R, Paravina RD, Ferracane JL. Comparison of at-home and in-office tooth whitening using a novel shade guide. Oper Dent. 2010;35:381–388. doi:10.2341/09-344-C
3. Joiner A. The bleaching of teeth: a review of the literature. J Dent. 2006;34:412–419. doi:10.1016/j.jdent.2006.02.002
4. Haywood VB. Treating sensitivity during tooth whitening. Compend Contin Educ Dent. 2005;26:11–20.
5. Goldberg M, Grootveld M, Lynch E. Undesirable and adverse effects of tooth-whitening products: a review. Clin Oral Investig. 2010;14:1–10. doi:10.1007/s00784-009-0302-4
6. Leonard RH
7. Tay LY, Kose C, Loguercio AD, Reis A. Assessing the effect of a desensitizing agent used before in-office tooth bleaching. J Am Dent Assoc. 2009;140:1245–1251.
8. Zekonis R, Matis BA, Cochran MA, Al Shetri SE, Eckert GJ, Carlson TJ. Clinical evaluation of in-office and at-home bleaching treatments. Oper Dent. 2003;28:114–121.
9. Dahl JE, Pallesen U. Tooth bleaching–a critical review of the biological aspects. Crit Rev Oral Biol Med. 2003;14:292–304.
10. Tam L. Effect of potassium nitrate and fluoride on carbamide peroxide bleaching. Quintessence Int. 2001;32:766–770.
11. Loguercio AD, de Cerqueira RR, Hofstaetter FL, et al. Assessing the effect of a desensitizing agente on dental sensitivity and effectiveness of bleaching. Rev Assoc Paulo Cir Dent. 2013;67:64–67.
12. Pimenta IC, Pimenta LAF. Home tooth whitening: risks and benefits: what the clinician needs to know. Rev Bras Odontol. 1998;55:195–200. in Portuguese.
13. Schulte JR, Morrissette DB, Gasior EJ, Czajewski MV. The effects of bleaching application time on the dental pulp. J Am Dent Assoc. 1994;125:1330–1335.
14. Brannstrom M. Dentin sensitivity. Arsb Goteb Tandlak Sallsk. 1964;21:15–35.
15. Soares JC, Silva NR, Quagliatto OS, et al. Tooth bleaching clinical evaluation with industrialized and drugstore manipulated carbamide peroxide gel. Rev Odontol UNESP. 2006;35:69–74.
16. Browning WD, Cho SD, Deschepper EJ. Effect of a nano-hydroxyapatite paste on bleaching-related tooth sensitivity. J Esthet Restor Dent. 2012;24:268–276. doi:10.1111/j.1708-8240.2011.00437.x
17. Armenio RV, Fitarelli F, Armenio MF, et al. The effect of fluoride gel use on bleaching sensitivity: a double-blind randomized controlled clinical trial. J Am Dent Assoc. 2008;139:592–597.
18. Browning WD, Haywood VB, Hughes N, et al. Prebrushing with a potassium nitrate dentifrice to reduce tooth sensitivity during bleaching evaluated in a practice-based setting. Compend Contin Educ Dent. 2010;31:220–225.
19. Cummins D. The efficacy of a new dentifrice containing 8.0% arginine, calcium carbonate, and 1450 ppm fluoride in delivering instant and lasting relief of dentin hypersensitivity. J Clin Dent. 2009;20:109–114.
20. Sowinski J, Ayad F, Petrone M, et al. Comparative investigations of the desensitising efficacy of a new dentifrice. J Clin Periodontol. 2001;28:1032–1036.
21. Marini I, Checchi L, Vecchiet F, Spiazzi L. Intraoral fluoride releasing device: a new clinical therapy for dentine sensitivity. J Periodontol. 2000;71:90–95. doi:10.1902/jop.2000.71.1.90
22. Athuluru D, Reddy C, Sudhir KM, et al. Evaluation and comparison of efficacy of three desensitizing dentifrices on dentinal hypersensitivity and salivary biochemical characteristics: a randomized controlled trial. Dent Res J. 2017;14:150–157.
23. Vano M, Derchi G, Barone A, et al. Reducing dentine hypersensitivity with nano-hydroxyapatite toothpaste: a double-blind randomized controlled trial. Clin Oral Investig. 2017;22:313–320.
24. Basting RT, Amaral FL, Franca FM, Flório FM. Clinical comparative study of the effectiveness of and tooth sensitivity to 10% and 20% carbamide peroxide home-use and 35% and 38% hydrogen peroxide in-office bleaching materials containing desensitizing agents. Oper Dent. 2012;37:464–473. doi:10.2341/11-337-C
25. Bonafe E, Loguercio AD, Reis A, Kossatz S. Effectiveness of a desensitizing agent before in-office tooth bleaching in restored teeth. Clin Oral Investig. 2014;18:839–845. doi:10.1007/s00784-013-1055-7
26. Ayad F, Ayad N, Zhang YP, DeVizio W, Cummins D, Mateo LR. Comparing the efficacy in reducing dentin hypersensitivity of a new toothpaste containing 8.0% arginine, calcium carbonate, and 1450 ppm fluoride to a commercial sensitive toothpaste containing 2% potassium ion: an eight-week clinical study on Canadian adults. J Clin Dent. 2009;20:10–16.
27. Hamlin D, Williams KP, Delgado E, et al. Clinical evaluation of the efficacy of a desensitizing paste containing 8% arginine and calcium carbonate for the inoffice relief of dentin hypersensitivity associated with dental prophylaxis. Am J Dent. 2009;22:16–22.
28. Schiff T, Delgado E, Zhang YP, et al. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentine hypersensitivity. Am J Dent. 2009;22:9A–15A.
29. Petrou I, Heu R, Stranick M, et al. A breakthrough therapy for dentin hypersensitivity: how dental products containing 8% arginine and calcium carbonate work to deliver effective relief of sensitive teeth. J Clin Dent. 2009;20:23–31.
30. Thiesen CH, Rodrigues Filho R, Prates LH, Sartori N. The influence of desensitizing dentifrices on pain induced by in-office bleaching. Braz Oral Res. 2013;27:517–523. doi:10.1590/S1806-83242013000600012
31. Basting RT, Rodrigues AL
32. Auschill TM, Hellwig E, Schmidale S, Sculean A, Arweiler NB. Efficacy, side-effects and patients‘ acceptance of different bleaching techniques (OTC, in-office, at-home). Oper Dent. 2005;30:156–163.
33. de Silva Gottardi M, Brackett MG, Haywood VB. Number of in-office light-activated bleaching treatments needed to achieve patient satisfaction. Quintessence Int. 2006;37:115–120.
34. Sulieman M, Addy M, MacDonald E, Rees JS. The effect of hydrogen peroxide concentration on the outcome of tooth whitening: an in vitro study. J Dent. 2004;32:295–299. doi:10.1016/j.jdent.2004.01.003
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.