")
Back to Journals » Clinical Interventions in Aging » Volume 16
Effects of Caregiver Dementia Training in Caregiver–Patient Dyads on Psychotropic Drug Prescription: A Randomized Controlled Study
Authors Birkenhäger-Gillesse EG , Janus SI, Achterberg WP , Zuidema SU
Received 5 April 2021
Accepted for publication 27 May 2021
Published 26 July 2021 Volume 2021:16 Pages 1449—1453
DOI https://doi.org/10.2147/CIA.S314412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Elizabeth G Birkenhäger-Gillesse,1,2 Sarah IM Janus,1 Wilco P Achterberg,3 Sytse U Zuidema1
1Department of General Practice and Elderly Care Medicine, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 2Laurens Care Centers, Division Long Stay, Rotterdam, the Netherlands; 3Department of Public Health and Primary Care, Leiden University Medical Center, Leiden, the Netherlands
Correspondence: Elizabeth G Birkenhäger-Gillesse
Laurens Care Centers, Division Long Stay, Pres. Rooseveltweg 22, Rotterdam, 3068 TR, the Netherlands
Tel +31619699113
Email [email protected]
Purpose: Does participating in a multicomponent intervention targeting caregivers change the prescription rates of psychotropic drugs of caregivers or the person with dementia (PWD) they live with and care for.
Patients and Methods: Participants were 142 dyads of community-dwelling cohabiting caregivers and PWD randomized to intervention or control (care as usual). Participating caregivers received the intervention in a holiday accommodation over five days in groups of two to six dyads. During this time, caregivers attended 14 psychoeducational group sessions on relevant emotional, relational, practical, financial, and social changes related to living with PWD. These sessions were delivered by a psychologist, a physiotherapist, an occupational therapist, an elderly care physician, a dietician and a social worker and included combating social isolation, planning for the future, re-rolling, medical aspects of dementia, fitness, therapeutic use of facilities, nutrition and using community services. The design was a randomized controlled trial. Outcomes were compared 3 months after baseline. Drug use for both caregivers and PWD were reported as all psychotropic drug use and specified as antipsychotic, antidepressant, and anxiolytic and hypnotic drug use based on Anatomical Therapeutic Chemical (ATC) classifications.
Results: Compared to the control group, no significant difference was observed in psychotropic drug use by 3 months after baseline among caregivers (p 0.22 MD − 0.08 95% CI − 0.20– 0.05) or PWD (p 0.61, MD 0.04 95% − 0.12– 0.21) in the intervention group.
Conclusion: A multicomponent course for caregivers living with PWD did not affect psychotropic drug use by either person. This may be explained by the low level of baseline drug use and the lack of the prescribing physician involvement in the present study. The low baseline drug use likely reflects selection bias for caregiver participants who were more inclined to use psychosocial interventions in preference to psychotropic medication, making them more likely to participate in caregiver training.
Keywords: caregiver, dementia, psychotropic drugs, psychosocial intervention, training
Introduction
About 70% of people with dementia (PWD) live in the community.1 Dutch demographic and prevalence data indicate that about 35% of these share a household with their primary caregiver.2,3 Unfortunately, most PWD experience behavioral and psychological symptoms of dementia at some point in the course of their illness.4 Clinical guidelines recommend nonpharmacological approaches as the first-line approach to treating these symptoms,5 advocating that psychotropic drugs should be prescribed with restraint due to their limited effectiveness and the frequency of side effects. However, in clinical practice, psychotropic drugs are frequently prescribed to community-dwelling PWD, with percentages varying from 29% to 50% depending on the stage of dementia.6–8
Caregivers of PWD also experience high and persistent burden that contributes to a decline in their own mental health. Therefore, psychotropic drug use is higher among these than in the general population.9,10 Reported utilization rates vary by drug type, with 4–13% using antidepressants, 13–22% using anxiolytics, and 3–8% using sedatives and hypnotics.9–11 Evidence suggests that caregiver characteristics predict psychotropic drug use, and not the severity of disease in the PWD or the perception of how well he or she is supported.9 Interventions aimed at supporting both the PWD and the caregiver may therefore reduce neuropsychiatric symptoms in PWD and promote good mental health in their caregivers, which in turn, may reduce psychotropic drug use.
We have previously published our findings on the effect of our “More at Home with Dementia” multicomponent dementia training for the caregivers of PWD.12 Analyses indicated that participating caregivers experienced fewer role limitations due to physical and emotional function, that they had better acceptance and coping, and experienced less stress.12 However, there was no effect on the primary outcome, care-related quality of life. Positive outcomes identified by qualitative analysis included better acceptance and coping and improved knowledge of dementia an available community services and facilities. It may be expected that these outcomes have led to different behaviors including better coping and consequently had influence on psychotropic drug use of the caregiver and the PwD as well. Therefore, in this study, we aimed to analyze whether psychotropic drug use in PWD or caregivers was decreased by the multicomponent dementia training intervention.
Methods
Design and Participants
Participants were recruited to the intervention, which we called “More at Home with Dementia”, either by referral or by self-referral. The randomized controlled trial included 142 dyads of cohabiting caregivers and PWD that we randomized to either intervention (training program) or control groups (care as usual). Randomization was performed by the research assistant who was blind to the pre-fixed treatment allocations. Included were people with dementia with a confirmed diagnosis of dementia who live at home with their primary caregiver and both the caregiver and the PwD are able to understand Dutch. Excluded were PwD who showed aggressive or wandering behaviors. Data were obtained at baseline and after 3 and 6 months. Details of the study have been published elsewhere,12–14 a full description of the intervention and measurements, and the effects on primary and secondary outcomes. Before starting, the study was submitted for approval to the Human Research Ethics Committee of the University of Groningen, the Netherlands which concluded that no assessment was needed based on relevant Dutch law concerning scientific research in humans. Also, this study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from all participating caregivers and, if possible, from the PwD. The trial has been registered at the Dutch Trial Register; Trial ID, NTR5775.
Intervention and Control Groups
Participating caregivers received training in groups of two to six dyads for 5 days in a holiday accommodation setting. During the intervention, caregivers attended 14 psychoeducational group sessions on relevant emotional, relational, practical, financial, and social changes associated with living with PWD. These sessions were delivered by a psychologist, a physiotherapist, an occupational therapist, an elderly care physician, a dietician and a social worker and included combating social isolation, planning for the future, re-rolling, medical aspects of dementia, fitness, therapeutic use of facilities, nutrition and using community services. Two sessions were scheduled on the first and last day and on the other days each morning and afternoon 2 sessions were given. Also, time was reserved to get to know each other and for leisure activities. The physicians of PWD and their partners were not involved. Participants in the control group received care as usual, which mostly comprised a dementia case manager, respite care in day care centers, other support groups, or a combination of these.
Measurements
Psychotropic drug use was coded according to the Anatomical Therapeutic Chemical (ATC) classification of the World Health Organization.15 Medications were categorized as follows: a) all psychotropics (excluding antidementia drugs), b) antipsychotics, c) antidepressants, and d) hypnotics and anxiolytics. The primary outcome of the effect analysis was care-related quality of life (CarerQol-7D). Other outcomes of interest were the self-rated burden, health, and mood symptoms of caregivers together with the neuropsychiatric symptoms, quality of life, and agitation in PWD. At meetings after 3- and 6-months caregivers were asked to expand on questions on their experiences during the intervention week, what knowledge they had used and what difference the intervention had made to their life.
Statistical Analysis
To analyze differences in psychotropic drug use between the intervention and control groups, we performed Pearson’s chi-square tests, assuming that observations were independent and normally distributed. In addition, we performed independent-samples t-tests to compute mean differences and 95% confidence intervals. As baseline characteristics did not point to selective attrition, we did not correct for baseline characteristics. Statistical analyses were undertaken using IBM SPSS, Version 24 (IBM Corp., Armonk, NY, USA).
Results
Of the 142 participants that were randomized in the study groups, 12 of the 71 couples in the intervention group and 21 of the 71 couples in the control group dropped out before the study began. Another 4 participants in the control group did not provide information about their medication use, leaving 59 and 46 eligible for baseline analysis respectively. No differences in baseline characteristics of intervention and control group were observed regarding sex, age, educational level, born in the Netherlands or Reisberg Global Deterioration Scale score (PwD).12,14 Table 1 shows the psychotropic drug use at baseline and at 3 months after the intervention for caregivers and PWD, including a comparison with the control group. No differences were observed in overall psychotropic drug use (number of participants using at least one psychotropic drug) or in antipsychotic, antidepressant, or hypnotic and anxiolytic drug use. Of the 19 caregivers who used psychotropic drugs at baseline, 8 (42%) dropped out of the study; by contrast, only 12 (14%) of the 88 caregivers who did not use psychotropic drugs dropped out.
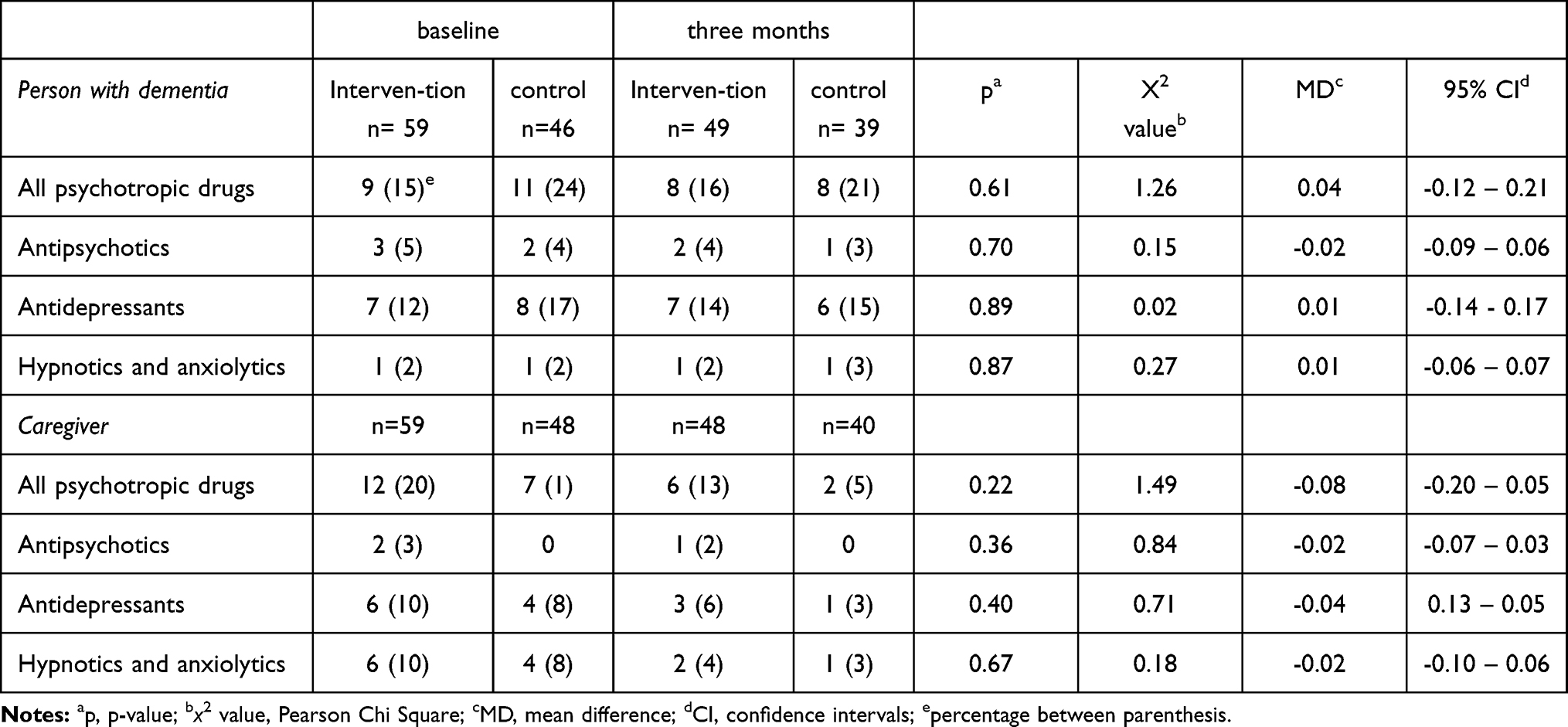 |
Table 1 Number (and Percentage) of Participants Using Psychotropic Medication Use of the Intervention and Control Group at Baseline and After Three Months Including the Difference Between the Intervention and Control Value at Three Months in p-value, Chi Square Value, Mean Difference and 95% Confidence Interval |
Among PWD at 3 months, 1% more in the intervention group and 3% fewer in the control group used at least one psychotropic drug, though the differences between groups were not significant at this time (p 0.61, MD 0.04 95% −0.12–0.21). Among the caregivers at 3 months, 7% fewer in the intervention group and 10% fewer in the control group used at least one psychotropic drug, though again differences between groups were not significant at this time (p 0.22 MD −0.08 95% CI −0.20–0.05). Finally, the change in psychotropic drug use from baseline to 3 months was not significant for either the PwD (MD −0.01, 95% CI −0.15–0.13) or the caregivers (MD 0.07, 95% CI −0.07 to 0.21).
Discussion
The More at Home with Dementia intervention did not reduce psychotropic drug use in either caregivers or PWD. Although the relatively small number of participants and relatively high dropout rates of caregivers using psychotropic drugs is a limitation of this study, we think our findings are of value and can help direct future research.
The lack of effect of the intervention on psychotropic drug use in PWD is consistent with the effects reported for other programs on psychosocial interventions aiming to lower psychotropic drug use. If psychosocial interventions are to lower psychotropic drug use in any meaningful way, there must be culture changes in nursing homes and greater involvement by prescribing physicians.16 Indeed, the lack of involvement by the physicians of participants in the present intervention could explain the lack of effect on drug use by PWD. Moreover, 15–24% of PWD in the present study used psychotropic drugs, which was much lower than the previously reported figures of 29% for the Netherlands17 and 50% for elsewhere.6–8 This suggests that the prescription rate for psychotropic drug use was already limited, possibly due to selection bias; that is, caregivers who are more inclined to look for alternatives to psychotropic medication might be more motivated to participate in a caregiver training intervention.
Concerning the caregivers, our qualitative data indicated that they experienced less stress and more confidence regarding caregiving tasks after the intervention. However, this did not translate into less psychotropic use compared to the control group. In contrast to data in the literature, psychotropic drug use seemed to decrease in the 3-month period after baseline in both the intervention and the control groups. However, we observed higher dropout rates among caregivers who used psychotropic drugs at baseline compared with those who did not, perhaps indicating a higher burden. The decline in both groups could reflect bias due to selective dropout.
Conclusion
A multicomponent intervention aimed at caregivers of PWD did not reduce psychotropic drug use compared to that in a control group. In PWD, psychotropic drug use at baseline and 3 months was low compared with the prevalence reported in existing literature. Further research into the impact of multicomponent interventions aimed at caregivers of PWD should incorporate general practitioners who can then optimize psychotropic drug prescribing for spousal caregivers and PWD during follow-up.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We thank Dr Robert Sykes (www.doctored.org.uk) for providing editorial services for the final drafts of this manuscript.
Funding
The study was funded by a grant of the ZonMw program Memorabel, project number 733050601. Part of this grant was provided for by “Alzheimer Nederland.” ZonMw is the governmental Netherlands organization for health research and development. The study was also funded by the THEIA foundation of Zilveren Kruis health insurance and by Laurens Care Centers, Rotterdam, the Netherlands.
Disclosure
The authors declare that they have no competing interests. However, there were two commercial sources of funding (THEIA foundation of Zilveren Kruis Health Insurance and Laurens Care Centers, Rotterdam, the Netherlands). The commercial funders had no role in the design, conduct, analysis and final publication decisions of the study.
References
1. Volksgezondheidenzorg.info. Bilthoven: RIVM; 2021. Available from: https://www.volksgezondheidenzorg.info/onderwerp/dementie/cijfers-context/huidige-situatie#node-aantal-personen-met-dementie-zorg.
2. Centraal-Bureau-voor-de-Statistiek. Opendata.cbs.nl. the Hague: Centraal Bureau voor de Statistiek; 2021. Available from: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/80117ned/table?ts=1555962502614.
3. Ott A, Breteler MM, van Harskamp F, et al. Prevalence of Alzheimer’s disease and vascular dementia: association with education. The Rotterdam study. BMJ. 1995;310(6985):970–973. doi:10.1136/bmj.310.6985.970
4. Borsje P, Wetzels RB, Lucassen PL, Pot AM, Koopmans RT. The course of neuropsychiatric symptoms in community-dwelling patients with dementia: a systematic review. Int Psychogeriatr. 2015;27(3):385–405. doi:10.1017/S1041610214002282
5. Zuidema SU, Smalbrugge M, Bil WME, et al. Multidisciplinairy guideline problem behaviour in Dementia [multidisciplinaire Richtlijn Probleemgedrag bij mensen met dementie]. Utrecht, The Netherlands: Verenso; 2018.
6. Joling KJ, Koppel MT, van Hout HPJ, et al. Psychotropic drug prescription rates in primary care for people with dementia from recorded diagnosis onwards. Int J Geriatr Psychiatry. 2021;36:443–451.
7. Maust DT, Langa KM, Blow FC, Kales HC. Psychotropic use and associated neuropsychiatric symptoms among patients with dementia in the USA. Int J Geriatr Psychiatry. 2017;32(2):164–174. doi:10.1002/gps.4452
8. Orsel K, Taipale H, Tolppanen AM, et al. Psychotropic drugs use and psychotropic polypharmacy among persons with Alzheimer’s disease. Eur Neuropsychopharmacol. 2018;28(11):1260–1269. doi:10.1016/j.euroneuro.2018.04.005
9. Clipp EC, George LK. Psychotropic drug use among caregivers of patients with dementia. J Am Geriatr Soc. 1990;38(3):227–235. doi:10.1111/j.1532-5415.1990.tb03496.x
10. Martín-García R, Martín-Avila G, la Rubia-marcos MD, et al. Consumption of drugs and nonpharmacological therapies in caregivers of patients with Alzheimer’s disease: a case-control study in Madrid. Dement Geriatr Cogn Dis Extra. 2016;6(1):68–77. doi:10.1159/000442942
11. Välimäki T, Gilmartin-Thomas JF, Bell JS, Selander T, Koivisto AM. Longitudinal study of medication use in caregivers of people with Alzheimer’s disease - Kuopio ALSOVA study. Dementia. 2020;19(5):1573–1585.
12. Birkenhäger-Gillesse EG, Achterberg WP, Janus SIM, Kollen BJ, Zuidema SU. Effects of caregiver dementia training in caregiver-patient dyads: a randomized controlled study. Int J Geriatr Psychiatry. 2020;35(11):1376–1384. doi:10.1002/gps.5378
13. Birkenhager-Gillesse EG, Kollen BJ, Zuidema SU, Achterberg WP. The “more at home with dementia” program: a randomized controlled study protocol to determine how caregiver training affects the well-being of patients and caregivers. BMC Geriatr. 2018;18(1):252. doi:10.1186/s12877-018-0948-3
14. Birkenhäger-Gillesse EG, Achterberg WP, Janus SIM, Zuidema SU. Caregiver dementia training in caregiver-patient dyads: process evaluation of a randomized controlled study. Int J Geriatr Psychiatry. 2021;36(1):127–135. doi:10.1002/gps.5404
15. World-Health-Organization. Anatomical therapeutic classification. Geneva; 2020. https://www.who.int/toolkits/atc-ddd-toolkit.
16. Birkenhäger-Gillesse EG, Kollen BJ, Achterberg WP, Boersma F, Jongman L, Zuidema SU. Effects of psychosocial interventions for behavioral and psychological symptoms in dementia on the prescription of psychotropic drugs: a systematic review and meta-analyses. J Am Med Dir Assoc. 2018;19(3):
17. Borsje P, Lucassen P, Wetzels RB, Pot AM, Koopmans R. Neuropsychiatric symptoms and psychotropic drug use in patients with dementia in general practices. Fam Pract. 2018;35(1):22–28. doi:10.1093/fampra/cmx061
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.