")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Effects of a Milk-Based Meal Replacement Program on Weight and Metabolic Characteristics in Adults with Severe Obesity
Authors Rafey MF , Murphy CF, Abdalgwad R , Kilkelly K, Griffin H, Beatty N, O'Shea PM , Collins C , McGrath R , Hynes M , Davenport C, O'Donnell M, Finucane FM
Received 7 August 2019
Accepted for publication 15 November 2019
Published 23 January 2020 Volume 2020:13 Pages 197—205
DOI https://doi.org/10.2147/DMSO.S226327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Mohammed F Rafey,1,2,* Conor F Murphy,1,2,* Razk Abdalgwad,1,2 Katriona Kilkelly,1 Helena Griffin,1 Niamh Beatty,1 Paula M O’Shea,3 Chris Collins,2,4 Robert McGrath,1 Mary Hynes,1 Colin Davenport,1,2 Martin O’Donnell,2 Francis M Finucane1,2
1Bariatric Medicine Service, Centre for Diabetes, Endocrinology and Metabolism, Galway University Hospitals, Galway, Ireland; 2HRB Clinical Research Facility, National University of Ireland, Galway, Ireland; 3Department of Clinical Biochemistry, Galway University Hospitals, Galway, Ireland; 4Department of Surgery, Galway University Hospitals, Galway, Ireland
*These authors contributed equally to this work
Correspondence: Francis M Finucane
Bariatric Medicine Service, Centre for Diabetes, Endocrinology and Metabolism, Galway University Hospital, Galway, Ireland
Tel +353 91 542711
Email [email protected]
Objective: Low energy meal replacement regimens can induce short-term weight loss in patients with severe obesity, but usually require specially formulated dietary supplements. We sought to determine the effects of a milk-based meal replacement program on anthropometric and metabolic characteristics in adults with severe obesity.
Methods: We conducted a retrospective cohort study of patients attending our hospital-based bariatric medicine service who completed a 24-week program consisting of eight weeks of milk-based meal replacement followed by weight stabilisation and maintenance phases. Patients were seen fortnightly by the bariatric physician, nurse and dietitian. We assessed changes in anthropometric and metabolic outcomes in completers at 0, 8, 16 and 24 weeks.
Results: Of 105 program completers available for follow-up, 53.3% were female. Mean age was 51.1± 11.2 years. Body weight decreased from 144.0± 27.6 kg at baseline to 121.1± 25.0 kg at 24 weeks (P< 0.001), a mean total body weight loss of 15.9± 6.0%, with a reduction in body mass index from 50.6± 8.0 to 42.6± 7.6 kg m− 2 (P< 0.001). In patients with diabetes, haemoglobin A1c decreased from 66.3± 13.0 to 48.3± 13.5 mmol/mol (P< 0.001) and diabetes medication use decreased significantly. There were significant improvements also in lipid profiles and reductions in antihypertensive medication use.
Conclusion: These preliminary findings suggest that completion of a 24-week milk-based meal replacement program has large effects on important outcomes in adults with severe obesity. However, attrition was high. Prospective assessment of the efficacy, safety, durability and cost-effectiveness of this intervention seems warranted.
Keywords: hypocaloric diet, milk, lifestyle modification, obesity treatment, type 2 diabetes
Introduction
With the rising prevalence of severe obesity,1 the need to develop effective treatment options for affected individuals continues to increase. Although bariatric surgery is an efficacious and cost effective intervention,2 only 10% of eligible patients choose this option.3 Other domains of bariatric care need to be developed and evaluated. Several studies have confirmed the benefits of structured lifestyle interventions in different patient subgroups, including those with non-diabetic hyperglycaemia,4 prevalent cardiovascular disease5 or established type 2 diabetes.6,7 However, meaningful, sustained reductions in weight over time are difficult to achieve with lifestyle modification alone.8 In a recent large general practice-based cohort study of severely obese adults in the UK, the annual probability of achieving 5% weight loss was one in eight for men and one in seven for women.9 Some suggest a meaningful improvement in health requires a weight loss of 10%,7 though we have found improvements in health in our bariatric patients after more modest weight loss.10
Several studies have described the use of low energy liquid diets (LELDs, ~1200 kcal/day) as components of intensive lifestyle modification programs for the treatment of obesity. Typical initial weight loss is approximately 10kg6,11 but often weight regain limits the longer term efficacy of these interventions.8,12 Side effects of low energy diets include constipation, dizziness, alopecia, nausea, headache, diarrhoea, abdominal pain and cholelithiasis.13 While participant retention in some meal replacement studies is good,6,11 attrition rates of 50% are common.8,14 Another limitation is that commercial meal replacement programs can be expensive, with some analyses suggesting they are prohibitively cost ineffective.15 Semi-skimmed milk is a potential low-cost alternative to commercially produced meal replacement supplements. Milk whey protein attenuates muscle loss16 and preserves myofibrillar protein synthesis17 in adults with obesity during very low calorie diets. Milk reduces appetite, calorie intake and body weight18 and alters post-prandial glucose and lipid metabolism19 in men with obesity. In mice, milk casein-derived peptides reduce high-fat diet-induced adipose tissue inflammation.20 A recent trial showed that drinking low fat milk made children feel fuller and eat less later in the day compared to juice or water.21
The feasibility, efficacy and safety of a semi-skimmed milk-based meal replacement program for adults with severe obesity have not previously been described. In our bariatric clinic, we introduced a milk-based LELD in 2013, providing patients with approximately 1200 kcal/day over eight weeks, with a subsequent 16-week period of food reintroduction, as outlined below. For this study, we sought to conduct a retrospective analysis of patient characteristics, key anthropometric and metabolic outcomes and attrition rates in patients attending the program, in order to inform more robust design of prospective studies or potential randomised controlled trials for future evaluations of the efficacy and safety of a semi-skimmed milk-based meal replacement program.
Methods
Study Design, Population and Setting
This was a single-center, retrospective cohort study, conducted in accordance with STROBE guidelines.22 The study population included bariatric patients who were referred to our milk-based meal replacement program. During the program patients attended the bariatric clinic every two weeks for 24 weeks (14 visits in total), met the nurse, dietitian and physician at each visit, had periodic blood tests performed and had weight, height and blood pressure measurements taken. All baseline and follow-up measures for the program were conducted in the Bariatric Medicine Clinic at the Centre for Diabetes, Endocrinology and Metabolism in Galway University Hospitals (GUH).
Inclusion and Exclusion Criteria
Male and female patients aged 18 years or older, referred to the bariatric service for assessment of severe obesity were eligible for inclusion. Our clinical practice is to define severe obesity as a body mass index (BMI) ≥40 kg m−2 (or ≥35 kg m−2 with co-morbidities such as type 2 diabetes or obstructive sleep apnea syndrome). Patients must have been willing to attend all the 14 scheduled study visits. Females of childbearing potential who were pregnant, breast-feeding or intended to become pregnant or were not using adequate contraceptive methods were not considered eligible for the program. Those with a recent myocardial infarction (within six months), untreated arrhythmia, untreated left ventricular failure, recent cholelithiasis (within the past year), hepatic or renal dysfunction, type 1 diabetes, untreated major psychiatric disorders, eating disorders, cancer, previous bariatric surgery, a BMI <35 kg m−2 or those deemed unlikely to attend for the full program (e.g. frequent clinic non-attendance) were excluded from the program.
Ethics Approval
The study was approved by the Galway University Hospitals’ Central Research Ethics Committee in December 2017 (ref CA 1900). As the program was part of standard clinical care for patients attending our service between 2013 and 2016 and was not a prospective research study, we did not prospectively obtain written informed consent from patients to use their data for research purposes. Considering recent changes in European legislation regarding the use of personal data (the General Data Protection Regulation (GDPR)), we have only used data in this study from the subgroup of patients who agreed to this retrospectively and provided written informed consent.
Measurements
Weight was measured on a Tanita® scale and height with a Seca® wall-mounted stadiometer, according to departmental standard operating procedures. Blood pressure was measured with an automated oscillometric device (Omron®) using a large cuff on the right arm, after participants had been seated quietly for five minutes. Three measures were recorded at one-minute intervals. A 12-lead electrocardiogram was performed to exclude occult ischemic heart disease or cardiac arrhythmia. Bloods were drawn after an overnight fast for glucose, renal and lipid profiles. All blood samples were processed locally in the Galway University Hospitals’ Department of Clinical Biochemistry (certified to ISO 15189 2007 accreditation standard). Glycated haemoglobin (HbA1c) was measured with HPLC (Menarini® HA8160 auto-analyzer). Total cholesterol was measured using the CHOP-PAP method. High density lipoprotein (HDL)-cholesterol and triglycerides were measured using the enzymatic and the GPO-PAP methods, respectively (COBAS® 8000 modular analyzer). Low-density lipoprotein (LDL)-Cholesterol was derived with the Friedewald equation. Information relating to antihypertensive, lipid lowering, and antidiabetic medication use at baseline and at the end of 24 weeks was extracted from the medical records of each participant.
Intervention
The milk-based LELD consisted of three continuous eight-week phases, each with fortnightly visits to the bariatric medicine clinic. During the first (weight loss) phase from weeks one to eight inclusive, an exclusively milk-based liquid diet was prescribed, consisting of approximately 2.5 liters per day of semi skimmed milk (depending on calculated protein requirements23,24) divided in seven portions throughout the day in equal doses, with additional sodium replacement, vitamin, mineral and fiber supplementation, equating to approximately 1200 kcal/day. The dietary composition of 100 mL of semi-skimmed milk included protein (3.5 g), carbohydrate (5 g, of which sugars 5 g) and fat (1.5 g). (An example of the dietary composition of the milk diet for a typical patient is provided in supplementary file) Throughout this phase, renal and liver profiles were assessed every two weeks and the patient was seen by the consultant endocrinologist, bariatric nurse and dietitian at each visit. During the second phase (weight stabilization) from weeks nine to sixteen inclusive, there was a gradual re-introduction of low-calorie meals from a set menu over eight weeks, according to protocol under the supervision of the bariatric dietitian with fortnightly visits continuing. During the third phase (weight maintenance) from weeks 17 to 24 inclusive, the liquid component of the diet was stopped completely and a fully solid isocaloric diet was restarted, based on individualized meal plans, under the supervision of the bariatric dietitian.
Outcome Measures
The primary outcome measure was body weight. Within the cohort, there were distinct subgroups of patients for whom specific outcomes were more relevant, such as those with type 2 diabetes. There were several secondary outcome variables, including BMI, percentage excess body weight, blood pressure, HbA1c, and lipid profiles. We set the threshold for an elevated HbA1c (“high HbA1c”) as “yes” if HbA1c ≥ 48 mmol/mol. We derived an a priori categorical variable for prevalent “dyslipidaemia” as “yes” if LDL-Cholesterol was ≥1.8 mmol/l in patients with diabetes, or ≥3.0 mmol/l in patients without diabetes at baseline, based on European Society of Cardiology guidelines.25 Then we defined the presence of poor blood pressure control (“hypertensive”) as “yes” if the systolic blood pressure (SBP) was ≥150 mmHg (in patients ≥60 years) or ≥140 mmHg (in patients <60 years) or if the diastolic blood pressure (DBP) was ≥ 90 mmHg (regardless of age).26 Of note, we were unable to classify patients as having hypertension or not as we did not prospectively record this in the medical notes in a consistent fashion, though we did record whether specific blood pressure medications were used at baseline and follow-up. We repeated the categorisation of all the above variables at each time point over 8, 16 and 24 weeks. Lastly, we derived a categorical variable “achieved 10% weight loss” as “yes” or “no” depending on whether the total percentage body weight loss was above this threshold at 8, 16 and 24 weeks.
Statistical Methods
Summary statistics (mean, standard deviation, range (or for categorical variables, the number, n and proportion, %)) for age, sex, height, diabetes status, weight, BMI, severe BMI status, percentage excess body weight (%EBW, defined relative to a BMI of 25 kgm−2), SBP, DBP, high HbA1c status, hypertensive status, dyslipidemia status, achieved 10% weight loss, total-, LDL-, HDL-cholesterol and triglyceride and HbA1c were obtained for times 0, 8, 16 and 24 weeks. We derived a surrogate measure of insulin resistance from the triglyceride: HDL-cholesterol ratio (THDLR).27,28 In order to convert our mmol/l values to the equivalent United States values (mg/dl), we applied a conversion factor of 38.67 for HDL-cholesterol and 88.57 for triglycerides. Information on reasons for withdrawal from the intervention was not routinely recorded.
Continuous explanatory variables were compared using the two-sample t-test or Mann Whitney Test as appropriate, while categorical explanatory variables were compared using the Chi-Square test. For completers, repeated measures ANOVA was used to determine whether there were statistically significant changes over time in outcome measures. All analyses were performed using SPSS version 24.
Results
Between January 2013 and Oct 2018, 260 patients were enrolled into the milk-based meal replacement program at the Bariatric Medicine clinic in Galway University Hospitals. Of these, 139 (53.5%) completed all 24 weeks of the intervention, with 121 (46.5%) discontinuing the intervention. From 139 completers, 105 (75.5%) agreed to participate in this study and provided written informed consent. Given that 1867 new patients were seen in our bariatric service over the six-year study period, 13.9% of newly referred bariatric patients ultimately participated in our milk program.
The baseline characteristics of the 105 patients who completed the intervention and consented to study participation are described in Table 1. Of these, 56 (53.3%) were female and mean age was 51.1±11.2 (range 18–71.6) years. Obesity-related comorbidities were prevalent, with 35.2% of patients diagnosed with diabetes, 61.9% treated for hypertension and 40.9% on lipid lowering therapy. Changes in anthropometric and metabolic characteristics in intervention completers at 8, 16 and 24 weeks are shown in Table 1. There was a 22.9±9.5 kg reduction in weight as anticipated (Figure 1), with a reduction in BMI of 8.0±3.2 kg m−2 (P<0.001). The proportion of patients losing 10% or more of their body weight at weeks 8, 16 and 24 was 59%, 87.6% and 86.7%, respectively (P=0.002), the proportion loosing 15% or more was 11.4%, 43.8%, 48.6% respectively (P=0.002).
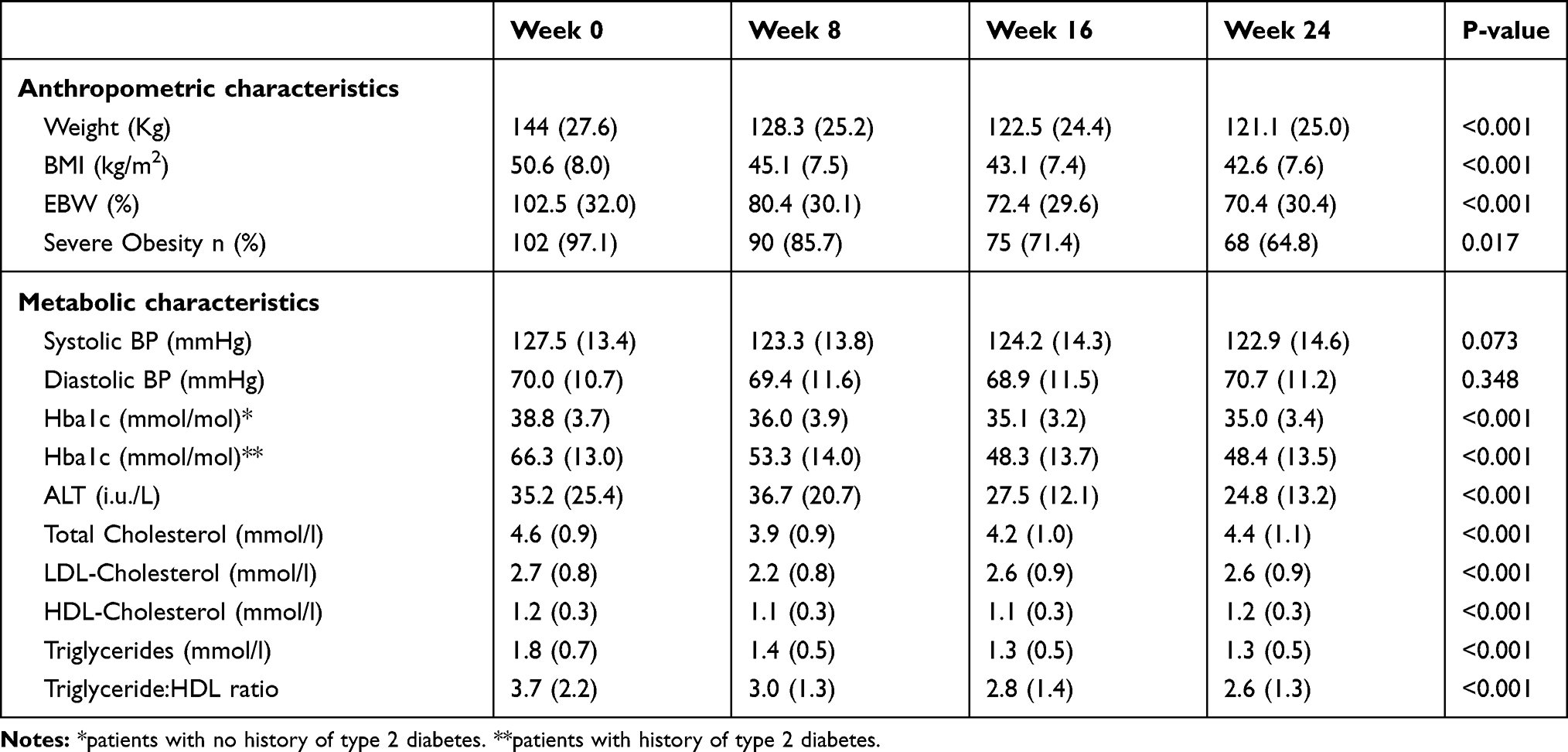 |
Table 1 Changes in Anthropometric and Metabolic Variables Over Time in 105 Patients Completing the Milk Programme |
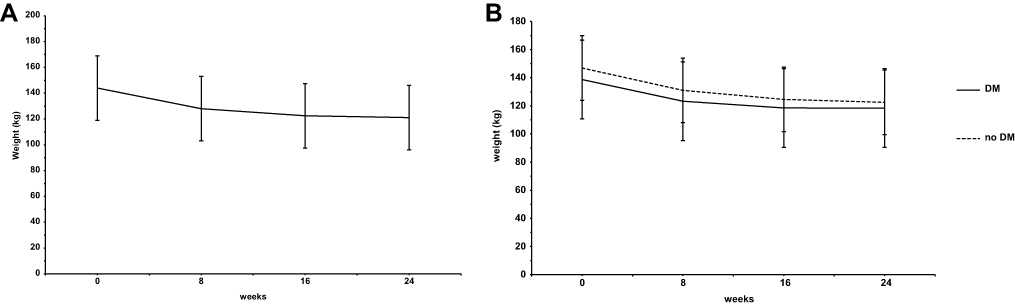 |
Figure 1 (A, B) Changes in total body weight over 24 weeks in the whole cohort, and in patients with and without diabetes, separately. |
There were no statistically significant changes in the systolic or diastolic blood pressure over time but the number of completers taking antihypertensive therapy fell from 68 (64.7%) at baseline to 37 (35.2%) at 24 weeks, a reduction of 29.5% (P<0.001). Specifically, of 25 (28.5%) taking angiotensin receptor blockers at baseline, 15 (14.2%) remained on these at follow-up, a reduction of 40% (P<0.001). Of 30 (26.4%) taking angiotensin converting enzyme inhibitors at baseline, 21 (20%) remained on these at follow-up, a reduction of 30.0% (P<0.001). Of 24 (22.9%) taking calcium channel blockers at baseline, 6 (5.7%) remained on these at follow-up, a reduction of 75% (P<0.001). Of 31 (29.5%) taking beta-blockers at baseline, 28 (26.7%) remained on these at follow-up, a reduction of 9.7% (P<0.001). Of 31 (29.5%) taking diuretics at baseline, 16 (15.2%) remained on these at follow-up, a reduction of 48.4% (P<0.001). Of 6 (5.7%) taking alpha-blockers at baseline, 2 (1.9%) remained on these at follow-up, a reduction of 66.7% (P<0.001).
There were statistically and clinically significant improvements in all components of the lipid profile, though unexpectedly these were most pronounced at 8 weeks and were somewhat attenuated by 24 weeks as shown in Table 1, despite the progressive weight loss observed during that time. Moreover, there was a reduction in the proportion of patients with elevated LDL cholesterol from 46.7% to 43.8% between baseline and follow up (P<0.001). We were careful to avoid either the introduction or cessation of any lipid lowering therapy during the duration of the intervention. Of 39 (37.1%) completers who were taking statin therapy at baseline, all but one continued this throughout the intervention, with four patients also taking ezetimibe at baseline and follow-up. The reduction in the triglyceride: HDL cholesterol ratio was consistent with an increase in insulin sensitivity with the intervention.
We noted a significant reduction in HbA1c over time in the 37 patients with diabetes, equivalent to a 16.3±13.6 mmol/mol reduction by 24 weeks, with an effective normalisation to the diagnostic threshold for diabetes of 48 mmol/mol (P<0.001). There was also a significant reduction in HbA1c in patients without prevalent diabetes. Of 10 patients requiring insulin at baseline, five (50%) had stopped it by 24 weeks (P<0.001). Of 15 patients taking sulphonylureas, 13 (86.7%) stopped these (P<0.001) while 14 (77.8%) of 18 patients taking GLP-1 receptor agonists had stopped these by 24 weeks (P<0.001). Similarly, seven of nine (77.8%) patients stopped dipeptidyl peptidase inhibitors (P<0.001), while one patient taking pioglitazone discontinued this at the start of the intervention. Three of six patients taking sodium glucose co-transporter 2 (SGLT2) inhibitor drugs remained on these throughout the intervention (P<0.001), while 35 of 38 patients remained on metformin throughout (P<0.001). The number of patients on two or more antidiabetic medications came down from 32 to 9, a reduction of 71.9% (P<0.001). In the five patients who remained on insulin, their dose came down from 123.1±21.6 to 28.7±13.4 units per day (P<0.001), a reduction of 76.7%.
Patients with diabetes who completed the program were slightly older and with a lesser degree of obesity than completers without diabetes. We observed a worse lipid profile in patients without diabetes, which we think may be due to a higher prevalence of statin use in patients with diabetes versus those patients without diabetes (64.9 vs 22.1%, P<0.001). Notwithstanding the differences in adiposity at baseline, there was no difference in the anthropometric response to the intervention in completers with versus those without diabetes, as shown in Figures 1–4.
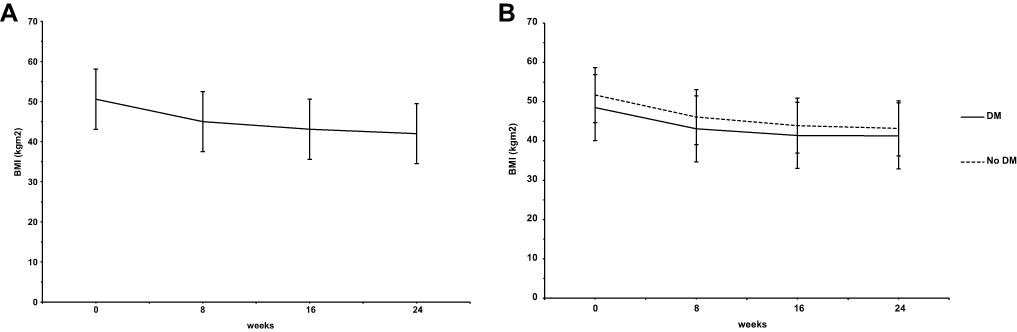 |
Figure 2 (A, B) Changes in body mass index over 24 weeks in the whole cohort, and in patients with and without diabetes, separately. |
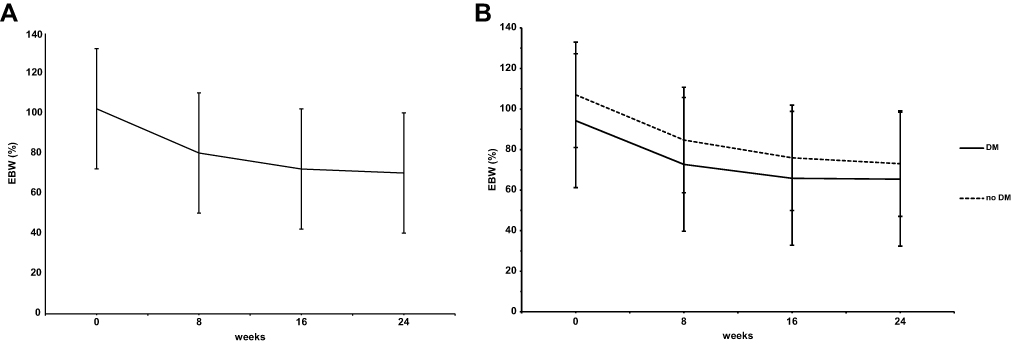 |
Figure 3 (A, B) Changes in percentage excess body weight over 24 weeks in the whole cohort, and in patients with and without diabetes, separately. |
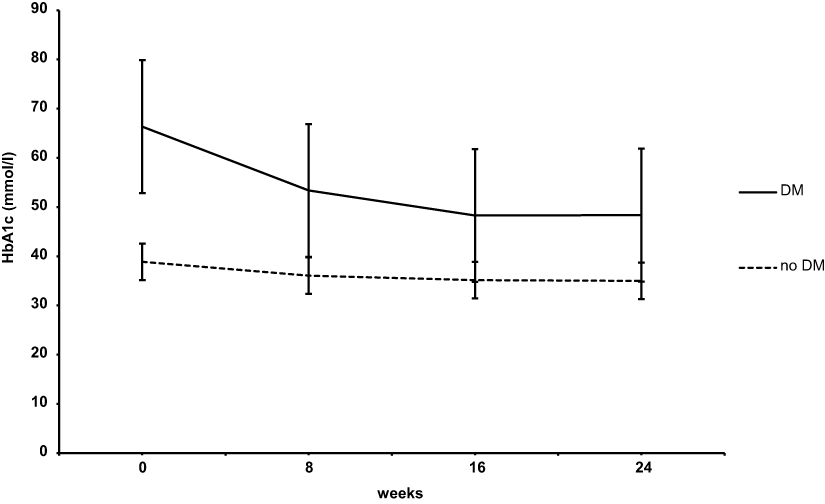 |
Figure 4 Changes in HbA1c over 24 weeks in patients with and without diabetes, separately. |
Discussion
These preliminary findings from a retrospective cohort of adults with severe obesity suggest that in the subgroup of patients who completed our 24-week, milk-based meal replacement program, there were significant reductions in excess weight and improvements in associated metabolic characteristics. These changes were much larger than those observed with a more conventional lifestyle modification program we run in a similar patient population, where mean weight loss in completers of a ten-week structured diet and physical activity program was 2.7kg.10
Notwithstanding the relatively high drop-out rate, the fact that 54% of patients were able to tolerate the intensive schedule of clinic visits and the very significant curtailment of dietary intake, particularly in the first eight weeks, is surprising to many. The mechanisms underlying a likely reduction in appetite are unclear. Ketosis has been shown to attenuate the increases in ghrelin and appetite that occur with dietary restriction29 and in recent years there has been a growing interest in the role of therapeutic ketosis in weight loss interventions.30 However, we do not routinely measure ketones as part of the milk intervention, so their contribution to our findings is uncertain. Moreover, given that patients were not carbohydrate restricted per se, the levels of ketosis may have been physiologically insignificant. These could and should be measured in future clinical trials of the intervention. It may be that the unique constituents of milk might account for some of the benefits seen in our intervention, though an aetiological trial with an equivalent non-milk-based meal replacement substrate would need to be done to clarify this issue.
Future, prospective studies will also need to address the cost-effectiveness of the intervention. While out of pocket costs for patients over six months for the milk and the fibre, salt, fish oil and micronutrient supplements are relatively modest (our approximate estimate is €446 per patient) 14 outpatient clinic visits over half a day with nurse, consultant, dietitian, registrar and secretarial time as well as overheads cost the Irish health service approximately €1088. Whether this represents good value for money, particularly with high attrition rates, remains to be determined.
We are likely to have underestimated the proportion of patients with dyslipidaemia by focussing only on LDL-cholesterol to define this arbitrarily rather than applying cut-offs to total cholesterol and triglycerides also. However, we believe that the large reductions in these individual components of the lipid profile are convincing and compelling, particularly given that statin therapy was neither initiated nor stopped during the intervention.
The influence of changes in physical activity energy expenditure on overall energy balance in the context of a significant reduction in energy intake is an important consideration in this study. It may be that physical activity energy expenditure (relative to body weight) might actually have increased in these patients, particularly if mobility improved. Future studies should address this important confounding variable. Similarly, as we have no data on body composition, it is not possible to determine the extent to which changes occurred specifically in lean and fat tissue mass and prospective studies should address this limitation.
Arguably our most important limitation is the lack of follow-up data for the patients who started the intervention but dropped out. It must be emphasised, therefore that this work is not a description of the effectiveness or efficacy of the milk-program but serves as a useful estimate of the effect size of the intervention as well as the attrition rate, to inform the development of future randomised controlled trials. While we think it is unlikely, it is possible that some of those who dropped out may have had significant weight regain or serious adverse events that precluded continued participation, which we would not be aware of, which is why we have avoided any attempt to compare data in completers and non-completers using last- or mean- observation carried forward analyses, for example. Nor can we comment on the safety of the intervention, as this would require prospective collection of information as well as ongoing follow-up in patients who dropped out of the intervention. While participant retention in some studies is good,11,31 attrition rates similar to ours here are not uncommon.8,14,32 Thus, our per-protocol analyses of outcome changes in intervention completers is likely to have introduced some bias, residual confounding and possibly type 1 statistical error. However, even randomised controlled trials of meal replacement programs have had methodological limitations. In one systematic review of 45 trials of non-surgical long-term weight loss maintenance interventions in adults with obesity, only 10 had robust allocation concealment, 17 described some form of blinding and 25 were deemed to handle incomplete data well.33 Other reviews have confirmed that poor allocation concealment and blinding are particularly prevalent in trials of LELDs.34 Hence, there is scope for enhanced rigour in similar future trials in order to reduce the potential for bias, residual confounding and type 1 errors. Clearly, it would be desirable to have information about safety outcomes and patients who drop out of the intervention in these trials, consistent with STROBE guidelines.22 Finally, the durability of weight loss and weight maintenance after the intervention is completed needs to be assessed in prospective follow-up studies. Weight regain is a universal challenge with almost all dietary interventions.8 Whether the degree of weight loss with the milk diet predicts the response to subsequent bariatric interventions such as surgery or drug therapy remains to be determined.
Conclusions
Notwithstanding the limitations in this study, we believe that our findings are novel and important particularly in the context of planning more robust prospective observational and randomised controlled trial assessment of the milk diet intervention. Such studies will need to extend the follow-up period well beyond the completion of the intervention, as weight regain is a well-established problem in the longer term.8,12 Ultimately this might help to broaden and refine the range of therapeutic options for adults affected by obesity.
Author Contributions
MFR and CM drafted the manuscript, devised a data collection strategy and helped with data analysis and interpretation. RA, NB, CB and RMG helped with data collection and revised the manuscript. KK, HG and MH delivered the intervention, helped with data collection and revising the manuscript. MOD helped with study design, data analysis and manuscript writing. POS processed biochemistry samples, collated metabolic data and revised the manuscript. CC and CD revised the manuscript. FMF designed and supervised the study, drafted the manuscript and is the guarantor for the study findings. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
MFR, CFM, RA, KK, HG, NB, PMO, CC, RM, MH and MO have no relevant conflicts to declare. CD and FMF have received honoraria, travel grants, unrestricted educational grants and served on advisory boards for Novo Nordisk, Eli Lilly, Pfizer Inc., Sanofi-Aventis, Astra Zeneca, Merck Sharp and Dohme, Boehringer Ingelheim, Janssen and Novartis. The authors report no other conflicts of interest in this work.
References
1. Sturm R, Hattori A. Morbid obesity rates continue to rise rapidly in the United States. Int J Obes. 2013;37(6):889–891. doi:10.1038/ijo.2012.159
2. Colquitt JL,Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014;(8):CD003641.
3. Jennings A, Hughes CA, Kumaravel B, et al. Evaluation of a multidisciplinary Tier 3 weight management service for adults with morbid obesity, or obesity and comorbidities, based in primary care. Clin Obes. 2014;4(5):254–266. doi:10.1111/cob.2014.4.issue-5
4. Li G, Zhang P, Wang J, et al. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: a 23-year follow-up study. The Lancet. 2014;2(6):474–480. doi:10.1016/S2213-8587(14)70057-9
5. Clark AM, Hartling L, Vandermeer B, et al. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med. 2005;143(9):659–672. doi:10.7326/0003-4819-143-9-200511010-00010
6. Lean ME, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet. 2017;391(10120):541–551.
7. Gregg EW, Jakicic JM, Blackburn G, et al. Association of the magnitude of weight loss and changes in physical fitness with long-term cardiovascular disease outcomes in overweight or obese people with type 2 diabetes: a post-hoc analysis of the Look AHEAD randomised clinical trial. The Lancet. 2016;4(11):913–921.
8. Franz MJ, VanWormer JJ, Crain AL, et al. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc. 2007;107(10):1755–1767. doi:10.1016/j.jada.2007.07.017
9. Fildes A, Charlton J, Rudisill C, et al. Probability of an obese person attaining normal body weight: cohort study using electronic health records. Am J Public Health. 2015;105(9):e54–9. doi:10.2105/AJPH.2015.302773
10. Crowe C, Gibson I, Cunningham K, et al. Effects of an eight-week supervised, structured lifestyle modification programme on anthropometric, metabolic and cardiovascular risk factors in severely obese adults. BMC Endocr Disord. 2015;15:37. doi:10.1186/s12902-015-0038-x
11. Christensen P. Comparison of a low-energy diet and a very low-energy diet in sedentary obese individuals: a pragmatic randomized controlled trial. Clin Obes. 2011;1.
12. Anderson JW, Vichitbandra S, Qian W, et al. Long-term weight maintenance after an intensive weight-loss program. J Am Coll Nutr. 1999;18(6):620–627. doi:10.1080/07315724.1999.10718897
13. Anderson JW, Conley SB, Nicholas AS. One hundred pound weight losses with an intensive behavioral program: changes in risk factors in 118 patients with long-term follow-up. Am J Clin Nutr. 2007;86(2):301–307. doi:10.1093/ajcn/86.2.301
14. Ryan DH, Johnson WD, Myers VH, et al. Nonsurgical weight loss for extreme obesity in primary care settings: results of the Louisiana obese subjects study. Arch Intern Med. 2010;170(2):146–154. doi:10.1001/archinternmed.2009.508
15. Finkelstein EA, Kruger E. Meta- and cost-effectiveness analysis of commercial weight loss strategies. Obesity. 2014;22(9):1942–1951. doi:10.1002/oby.v22.9
16. Verreijen AM, Verlaan S, Engberink MF, et al. A high whey protein-, leucine-, and vitamin D-enriched supplement preserves muscle mass during intentional weight loss in obese older adults: a double-blind randomized controlled trial. Am J Clin Nutr. 2015;101(2):279–286. doi:10.3945/ajcn.114.090290
17. Hector AJ, Marcotte GR, Churchward-Venne TA, et al. Whey protein supplementation preserves postprandial myofibrillar protein synthesis during short-term energy restriction in overweight and obese adults. J Nutr. 2015;145(2):246–252. doi:10.3945/jn.114.200832
18. Tahavorgar A, Vafa M, Shidfar F, et al. Whey protein preloads are more beneficial than soy protein preloads in regulating appetite, calorie intake, anthropometry, and body composition of overweight and obese men. Nutrition Res. 2014;34(10):856–861. doi:10.1016/j.nutres.2014.08.015
19. van Meijl LE, Mensink RP. Effects of milk and milk constituents on postprandial lipid and glucose metabolism in overweight and obese men. Br J Nutr. 2013;110(3):413–419. doi:10.1017/S0007114512005314
20. Aihara K, Osaka M, Yoshida M. Oral administration of the milk casein-derived tripeptide Val-Pro-Pro attenuates high-fat diet-induced adipose tissue inflammation in mice. Br J Nutr. 2014;112(4):513–519. doi:10.1017/S0007114514001147
21. Mehrabani S, Safavi SM, Mehrabani S, et al. Effects of low-fat milk consumption at breakfast on satiety and short-term energy intake in 10- to 12-year-old obese boys. Eur J Nutr. 2016;55(4):1389–1396. doi:10.1007/s00394-015-0956-4
22. von Elm E, Altman DG, Egger M, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
23. British Dietetic Association. A Pocket Guide to Clinical Nutrition. The Parenteral & Enteral Nutrition Group of the British Dietetic Association; 2011.
24. Lee HA, Hartley TF. A method of determining daily nitrogen requirements. Postgrad Med J. 1975;51(597):441–445. doi:10.1136/pgmj.51.597.441
25. Catapano AL, Graham I, De Backer G, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37(39):2999–3058. doi:10.1093/eurheartj/ehw272
26. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
27. Gaziano JM, Hennekens CH, O’Donnell CJ, et al. Fasting triglycerides, high-density lipoprotein, and risk of myocardial infarction. Circulation. 1997;96(8):2520–2525. doi:10.1161/01.CIR.96.8.2520
28. McLaughlin T, Reaven G, Abbasi F, et al. Is there a simple way to identify insulin-resistant individuals at increased risk of cardiovascular disease? Am J Cardiol. 2005;96(3):399–404. doi:10.1016/j.amjcard.2005.03.085
29. Sumithran P, Prendergast LA, Delbridge E, et al. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur J Clin Nutr. 2013;67(7):759–764. doi:10.1038/ejcn.2013.90
30. Hallberg SJ, McKenzie AL, Williams PT, et al. Effectiveness and safety of a novel care model for the management of Type 2 Diabetes at 1 year: an open-label, non-randomized, controlled study. Diabetes Ther. 2018;9(2):613–621.
31. Miller GD, Nicklas BJ, Davis C, et al. Intensive weight loss program improves physical function in older obese adults with knee osteoarthritis. Obesity (Silver Spring). 2006;14(7):1219–1230. doi:10.1038/oby.2006.139
32. Thomson RL, Buckley JD, Noakes M, et al. The effect of a hypocaloric diet with and without exercise training on body composition, cardiometabolic risk profile, and reproductive function in overweight and obese women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2008;93(9):3373–3380. doi:10.1210/jc.2008-0751
33. Dombrowski SU, Knittle K, Avenell A, et al. Long term maintenance of weight loss with non-surgical interventions in obese adults: systematic review and meta-analyses of randomised controlled trials. BMJ. 2014;348:g2646. doi:10.1136/bmj.g2646
34. Bueno NB, de Melo ISV, de Oliveira SL, et al. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Br J Nutr. 2013;110(7):1178–1187. doi:10.1017/S0007114513000548
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.