")
Back to Journals » Journal of Pain Research » Volume 16
Effectiveness of Thoracic Spine Manipulation on the Management of Neck Pain: A Systematic Review and Meta-Analysis of Randomized Control Trials
Authors Tsegay GS , Gebregergs GB , Weleslassie GG , Hailemariam TT
Received 17 April 2022
Accepted for publication 4 February 2023
Published 27 February 2023 Volume 2023:16 Pages 597—609
DOI https://doi.org/10.2147/JPR.S368910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Gebrerufael Solomon Tsegay,1 Gebremedhin Berhe Gebregergs,2 Gidey Gomera Weleslassie,1 Teklehaimanot Tekle Hailemariam1
1Department of Physiotherapy, School of Medicine, College of Health Sciences and Ayder Comprehensive Specialized Hospital, Mekelle University, Mekelle, Tigray, Ethiopia; 2Department of Epidemiology, School of Public Health, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia
Correspondence: Gebrerufael Solomon Tsegay, College of health Sciences, Mekelle University, P.O. Box 1871, Mekelle, Tigray, Ethiopia, Tel +251914041691, Email [email protected]
Abstract: There are contradicting findings regarding the effect of thoracic spine manipulation in decreasing pain and disability in patients with chronic mechanical neck pain. Hence, the purpose of this review was to evaluate the current evidence on the effectiveness of thoracic spine thrust manipulation in decreasing pain intensity, and neck disability among subjects with chronic mechanical neck pain. We made a comprehensive search of literature published between 2010 and 2020 from the electronic databases of PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, and Physiotherapy Evidence Database (PEDro). We adhered to Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA). The methodological quality was assessed by the PEDro scale, and the level of evidence rated by Grading of Recommendations Assessment, Development, and Evaluation (GRADE) software. Finally, a meta-analysis was done using RevMan 5.3 with a random-effects model to calculate the mean difference (MD) and 95% confidence intervals for pain and disability. Eight eligible randomized controlled trials were identified with a total of 457 participants. The quality assessment of the included studies was found to be fair in quality (mean PEDro score of 6.63/10). The overall GRADE of the review showed low to moderate level of evidence. Effect size estimates of the studies showed modest differences in pain reduction, as it revealed a significant effect in Visual Analog Scale ((VAS) 0– 100mm) (MD − 12.46; 95% CI: − 17.29, − 7.64), and Pain Numeric Rating Scale ((PNRS) 0– 10 pts) (MD − 0.8; 95% CI: − 1.60, − 0.10). The thoracic manipulation also resulted in a significant effect in decreasing neck disability, in which the mean difference in Neck disability index (NDI) showed (MD − 6.46; 95% CI: − 10.43 − 2.50). This review suggested that thoracic spine manipulation was effective in reducing pain and neck disability in all adults with chronic mechanical neck pain compared to other interventions.
Keywords: chronic neck pain, manual therapy, mechanical neck pain, neck pain, spinal manipulation and thoracic manipulation
Introduction
Neck pain is a common condition worldwide which is increasing in the general population and most people experience at some point in their lifetime.1 The movement pattern and daily activities can be affected with ultimate impact on the social participation and economy of individuals.2,3 The one-year prevalence for neck pain has been reported to range between 16.7% and 75.1%.4 According to the Global Burden of Disease 2010 study, neck pain ranked 4th highest in terms of disability as measured by years lived with disability (YLDs), and 21st in terms of overall burden, and in 2015 neck pain reported as the leading cause of disability in most countries.5,6
The common classification of neck pain is mechanical neck pain.7 Although the definition varies among different research studies, mechanical neck pain is most commonly defined as pain located in the cervical spine or cervicothoracic junction that is elicited and/or exacerbated by cervical motion and/or palpation of cervical musculature.7–10 Recently, the Cochrane Collaboration (2015) suggested categorizing patients based on symptom duration: acute (<6 weeks), subacute (6–12 weeks), and chronic (>12 weeks).11 Acute, subacute, and chronic stages are time-based stages helpful in classifying patient conditions. A clinical practice guideline on neck pain stated that time-based stages help make treatment decisions based on the irritability of tissues on neck conditions.12
Neck pain management may be applied using a different treatment approach’s like; medications, manual therapy, and exercises. Manual therapies contribute to improve pain and function in adults with neck pain.13,14 The intrinsic biomechanical linkage of the thoracic with the cervical spine, disturbances in the biomechanics of the thoracic spine could be a primary contributor to neck pain.15 Thoracic manipulation alone or in combination with other physiotherapy treatments was used to reduce cervical spine pain, improve function and cervical range of motion (CROM).10,16
Evidence has begun to emerge in support of thoracic spine thrust manipulation as an intervention in the management of non-specific neck pain and acute mechanical neck pain.7,10,17–19 The effect of these interventions on patients with chronic neck pain has been inconsistent; for instance, pain relief was obtained in the studies that compare thoracic manipulation alone or in combination with the control or comparison group.20–24 However, no statistically significant differences were found in the intragroup or intergroup analyses of the experimental and placebo groups regarding the intensity of neck pain at rest in the immediate or short-term post-intervention evaluations. Similarly, the study that compares cervical manipulation to thoracic manipulation did not indicate a statistically significant group-by-time interaction for chronic neck pain.25–27 Hence, the main objective of this review is to evaluate the current evidence on the effectiveness of thoracic manipulation on decreasing pain intensity and neck disability on subjects with chronic mechanical neck pain.
Materials and Methods
Protocol and Registration
This systematic review and meta-analysis were registered in the PROSPERO database as (CRD42020204983) accessed at https://www.crd.york.ac.uk/PROSPERO and conducted according to the PRISMA guidelines.28
Eligibility Criteria
Inclusion Criteria
Randomized control trials available in full text and written in the English languages that were recently conducted within the last 10 years (2010–2020). It was decided to use the year 2010 as a cut off because a preliminary search conducted by the authors did not reveal any substantial literature on this topic prior to the year 2010. Studies looking at participants with only chronic mechanical neck pain and age ≥18 years that compared the effect of thoracic manipulation with other managements were included.
Exclusion Criteria
Studies that were not matched to the objective of this review, with low quality of PEDro score <4/10 and studies that compared two thoracic manipulation techniques, not specifically explained the participants’ symptom duration or with acute neck pain, and studies without the outcome of interests were excluded from this review.
Study Type
Any published randomized controlled trial (RCT) in a full-text form that investigated the effect of thoracic manipulation on subjects with chronic mechanical neck pain was included.
Participants
The participants were adults with age ≥18 years and both sexes (male and female) with a chronic mechanical type of neck pain.
Interventions
The intervention of interest was thoracic manipulation (TM). The technique could be provided multiple times to a single spinal region or various spinal regions during a single session or over multiple sessions. Co-interventions could also be included within the treatment session if these were also included in the comparison group. This allows for differences in treatment effect to be attributed to the addition of TM in the experimental group.
Comparison
The studies need to compare thoracic spine thrust manipulation to any other non-thrust manipulation, mobilization, exercise, and no intervention or placebo.
Outcomes
The outcomes of interest for this systematic review were pain and disability. Across all studies, the pain was measured using either the Numeric Pain Rating Scale (NPRS; 0–10pts) or the Visual Analog Scale (VAS; 0–100mm), and Disability was assessed using either the Neck Disability Index (NDI; 0–100%) or the Northwick Park Pain Questionnaire (NPQ; 0–100%).
Search Strategy
Beginning in June 2020, the authors comprehensively searched articles relevant to this meta-analysis using the electronic databases of PubMed, CINAHL, Cochrane Library, and PEDro data bases. The search was restricted to RCT, written only in English language, and conducted from 2010 to 2020. We used the following terms or keywords independently or in combination: (thoracic manipulation, thoracic thrust manipulation, neck pain, manipulation, thrust, cervical, and chronic neck pain filtered with RCTs, full text, human participants, and duration <10 years) (Table 1).
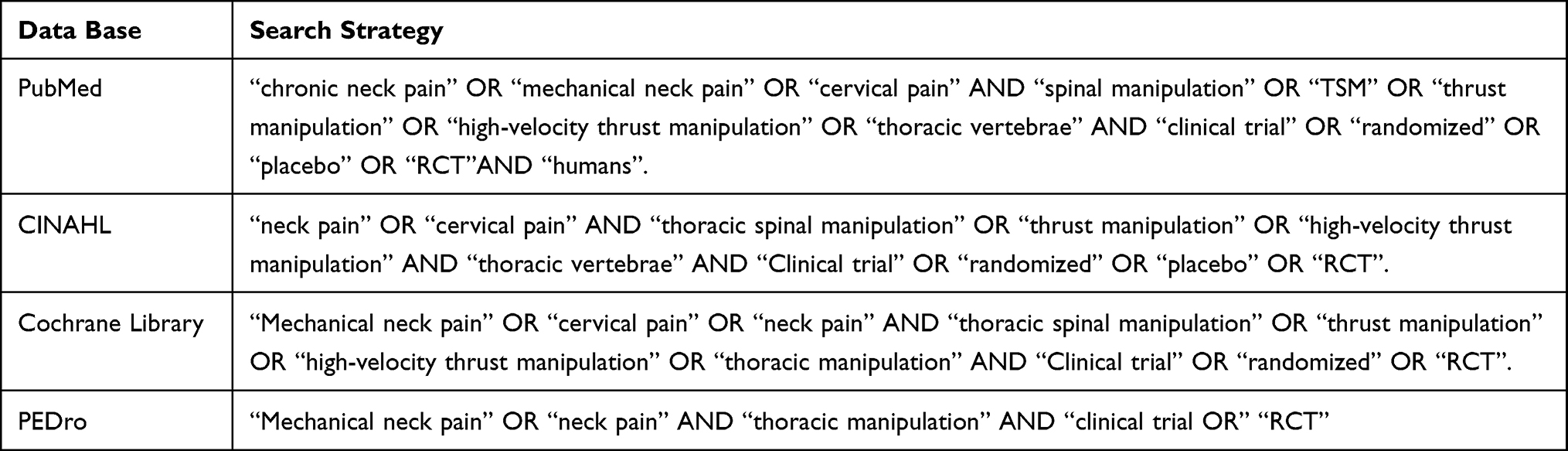 |
Table 1 The Literature Search Strategy |
The goal behind the search strategy was to identify all potential RCTs that assessed the role of thoracic spine manipulation in the management of individuals with CMNP. The authors (GS, GG, and TT) comprehensively searched articles relevant to this meta-analysis. After the computerized search was completed, reference lists of all selected articles were searched by the authors (GS and GG) to identify additional related articles. Each author (GS, GG, and TT) examined all titles and abstracts to determine initial study eligibility. Full-text articles were then re-evaluated for specific inclusion criterion by (GS and GG).
Selection of Studies
We employed the predetermined inclusion criteria to screen for relevant full-text trials. An article was included for appraisal, data extraction and analysis based on the eligibility criteria.
Quality Assessment
The methodological qualities of the selected articles were critically appraised with 11-item Physiotherapy Evidence Database (PEDro) scale (Table 2).29 PEDro scale is a validated tool to assess the methodological quality of physical therapy and rehabilitation trials. Two authors (GS and GG) who were physiotherapy professionals and more familiar with the scale independently scored each of the included articles, and then the discrepancies resolved through further discussion until consensus was met. A study was considered to be of “high” quality if the PEDro score of 7 or above, “fair” quality if the score of 5–6, and “poor” quality if the score was 4 or below.30
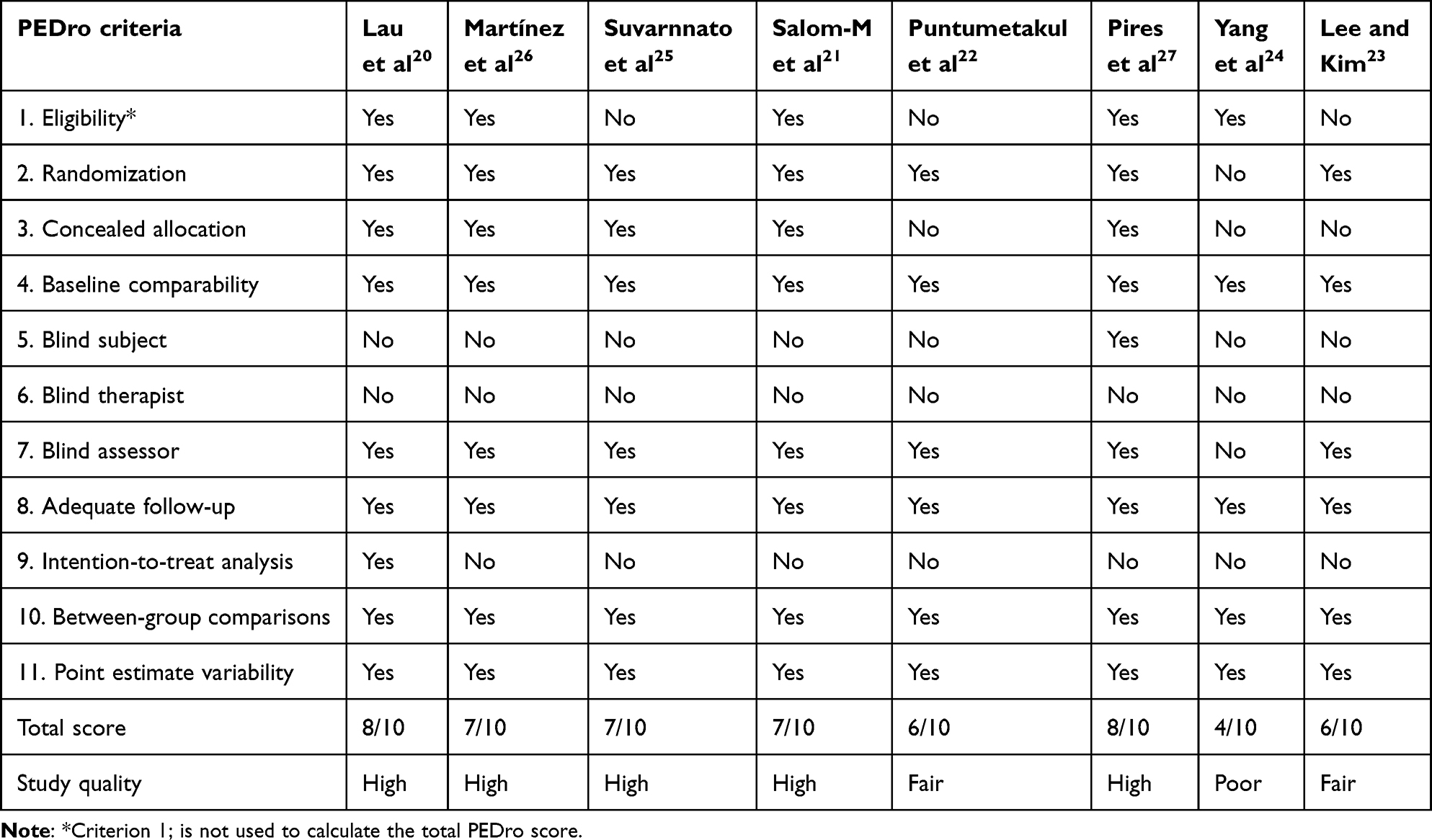 |
Table 2 Quality of Articles (PEDro Scale) |
To assess the overall body of evidence, the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was also utilized for all included studies. There are five domains used in the GRADE system, including the risk of bias, the inconsistency of results, indirectness of evidence, imprecision, and reporting bias.11,31 Randomized controlled trials begin with a high-quality evidence classification but may be downgraded if one or more of the above-described domains are present.31
Data Extraction
Two investigators (GS and GB) extracted data using a standardized data extraction form. We extracted data like sample size, age, outcome measures, interventions performed (including manipulation techniques or approach and treatment frequency), and treatment given to the comparative group, follow-up time, and results. Mean difference (MD) with standard deviation (SD) was extracted for the identified outcomes. Similarity and differences of the findings were putted and discussed.
Analysis
Data analysis was conducted using RevMan 5.3. The post-intervention scores and standard deviations (SD) were inputted into the meta-analysis. For all meta-analyses, a random-effects model with inverse variance method was used to calculate weighted mean differences and 95% CI. When there were multi-group data, we selected the common and clinically relevant comparison. Heterogeneity between trials was assessed using the I2 statistic. The I2 statistic describes the percentage of variability in effect estimates that was due to heterogeneity rather than sampling error (chance): less than 40% suggests that heterogeneity was not important, and above 75% suggests considerable heterogeneity. Values between 40% and 75% suggest moderate-to-substantial heterogeneity.32 The pooled data for each outcome were reported as weighted mean differences with a 95% confidence interval (CI).
Result
Study Selection
Searching of literature was done from different data bases. During the first search, a total of 745 articles were found from an electronic database. After removing the duplications, 312 articles were left. Of the 24 full-text articles 16 were excluded using the eligibility criteria. Finally, eight RCTs that matched the review objective were included in the meta-analysis. PRISMA flow diagram was used to show the searching and identifying the relevant articles (Figure 1).
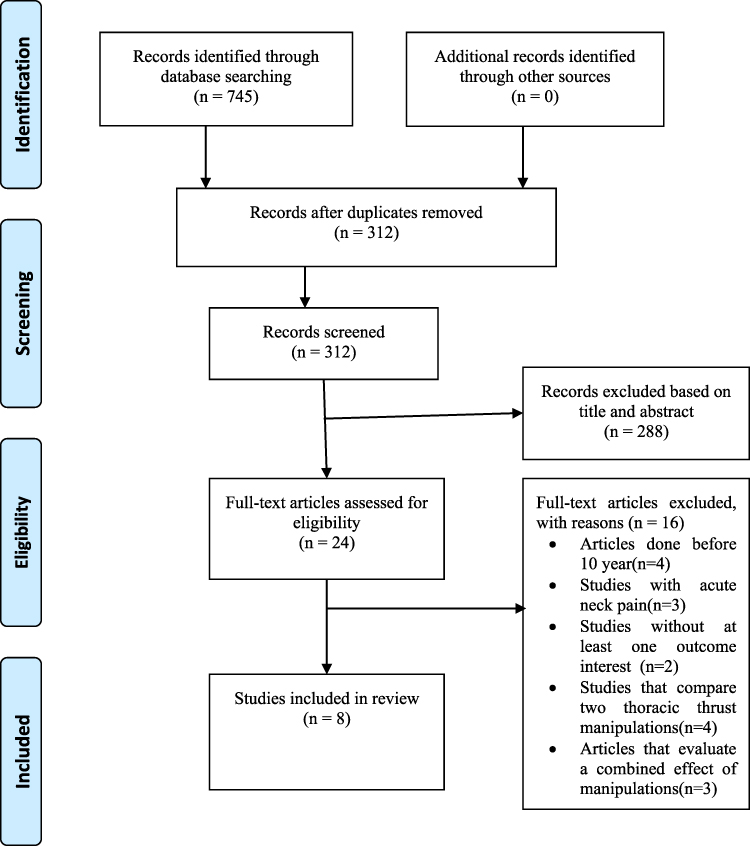 |
Figure 1 Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) flow diagram of study selection. |
Description of Studies
The studies chosen for inclusion in this meta-analysis were all randomized clinical trials investigating the effects of TSM on pain and neck disability among patients with CMNP compared to various other interventions. A total of 385 participants with a range from 30 to 120 were included across all 8 studies.20–26 All of the studies included both male and female participants with the age range 18–60 except one article27 in which all the participants were young women with chronic mechanical neck pain. All studies included participants with CMNP that were randomly assigned to either the TSM group or a comparison group. The follow-up times varied between studies from immediate to 6 months post-intervention. All studies investigated pain (NPRS or VAS), and three studies assessed disability (NDI). Comparison of thoracic manipulation was done with placebo22,25,27 thoracic spine mobilization,21 cervical manipulation,26 and co-interventions like infrared, craniocervical deep flexor exercise, and cervical stability training.20,23,24 The result of the articles were synthesized, analyzed, and discussed for the conclusion of the review, and a summary of these included articles is presented in Table 3.
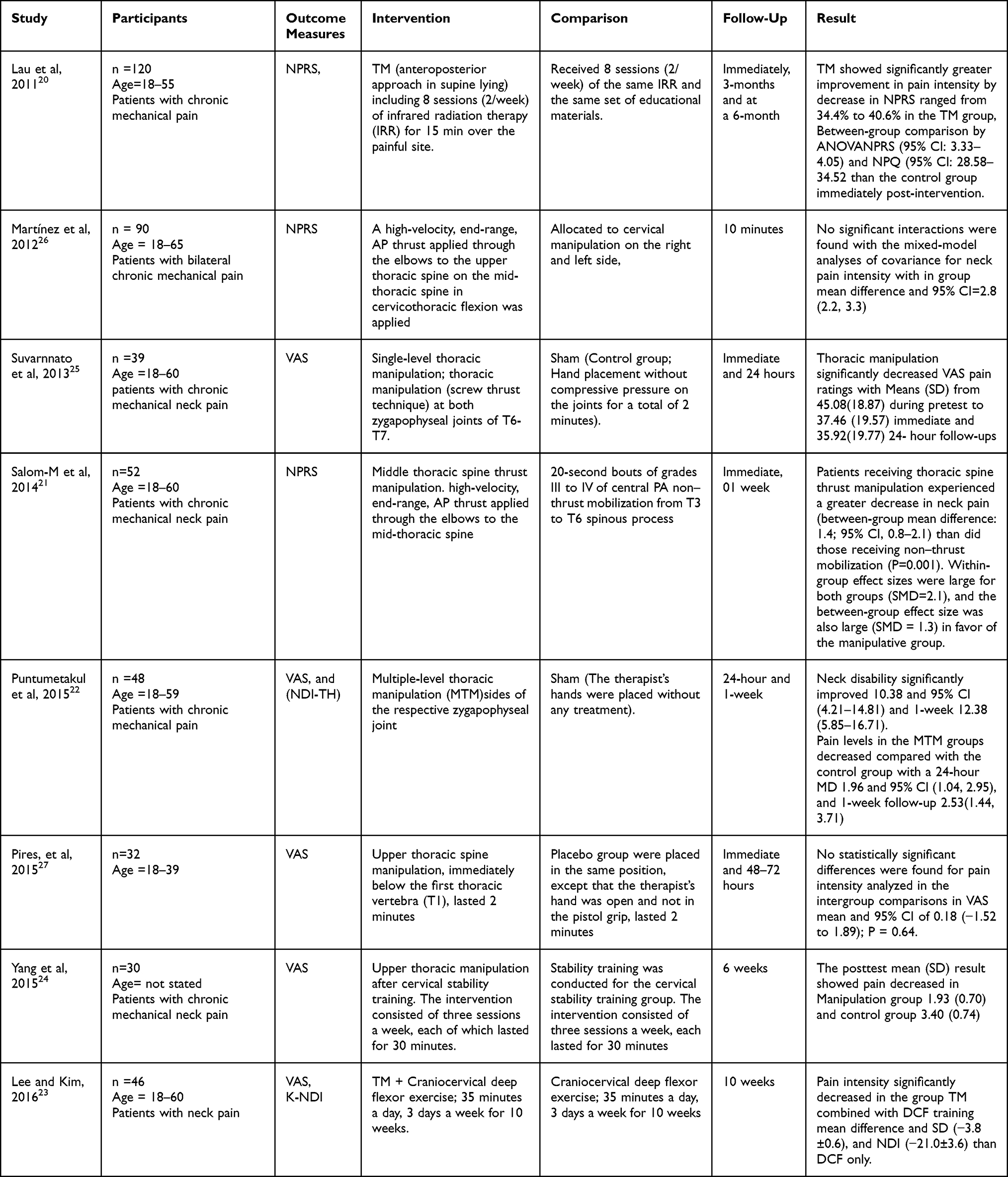 |
Table 3 Characteristics of the Included Studies |
Methodological Quality Assessment
These articles were then assessed for quality utilizing a PEDro scale and presented in Table 2. The score of the included articles ranged from 4 to 8 with a mean score of 6.63/10 (SD=±1.3), indicating that the average quality of the included studies is fair or moderate. Five studies20,21,25–27 were found to be of high quality, two articles22,23 of “fair” quality, and one article24 of “poor” quality. None of the studies blinded the treating clinicians or therapists, and only one article27 met the criterion regarding blinding of subjects as it is known that blinding is difficult to the patient and impossible to blind the care provider in manual treatments.
A formal grading of evidence was conducted using the GRADEpro software to provide an overall level of evidence for thoracic manipulation in the management of CMNP. The individual level ranged from low to high, and overall level of evidence (certainty) of the body of this study ranged from low to moderate. It is presented in Table 4 and Table 5.
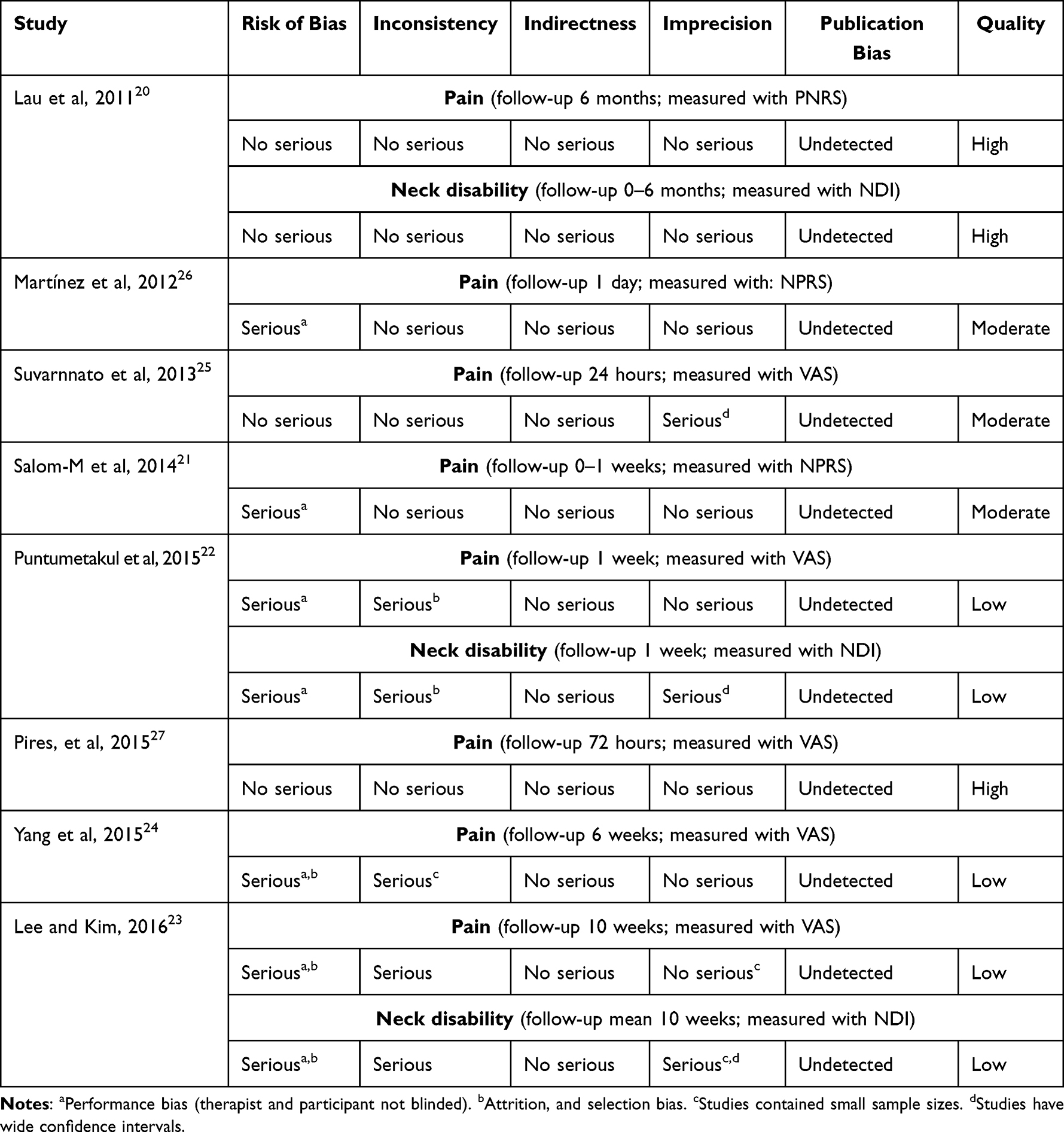 |
Table 4 GRADE Evidence Profile of Individual Articles |
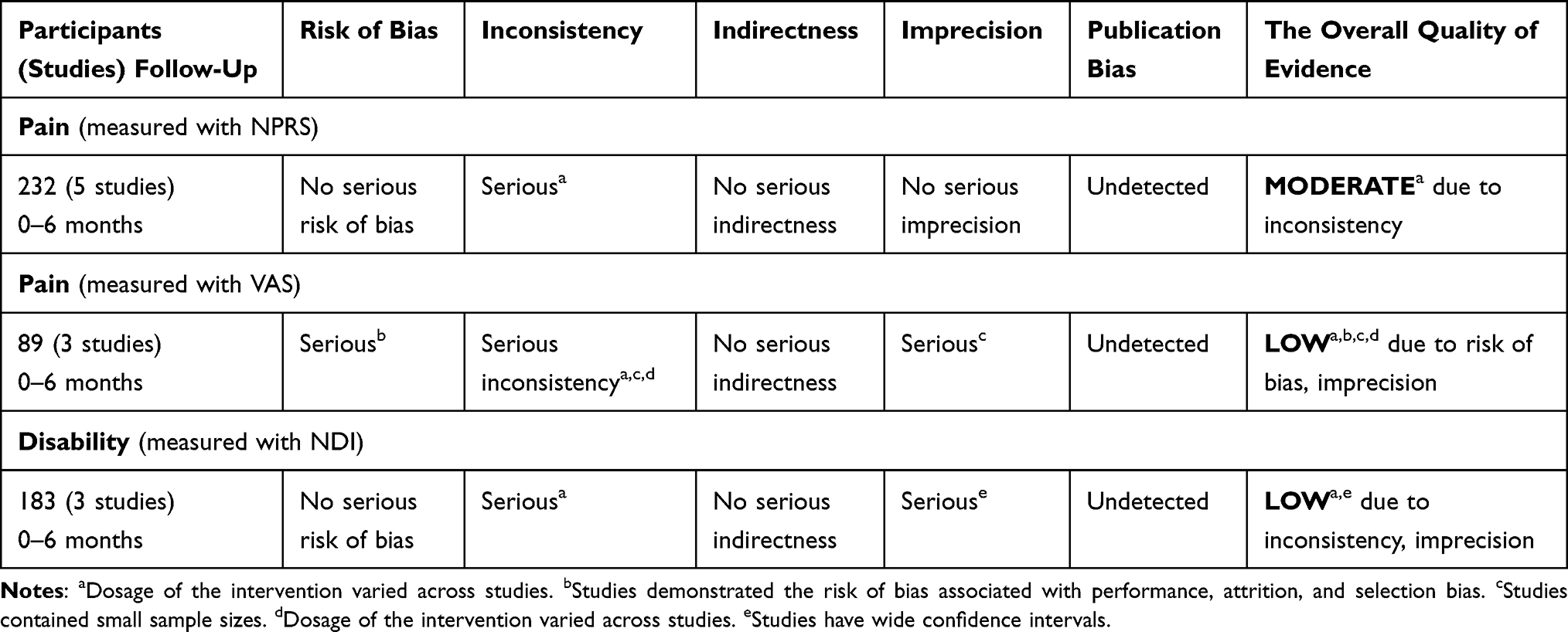 |
Table 5 GRADE Overall Evidence Profile |
Synthesis of Results
This review provides evidence on the effectiveness of TSM to reduce pain intensity and decrease neck disability on subjects with chronic mechanical neck pain. Some of the articles compare thoracic thrust manipulation with non-thrust, cervical thrust manipulation, and with a group out of intervention. The result of these articles are summarized and discussed. Statistical significance was determined by a p-value of <0.05 or 95% confidence interval.
Pain Intensity
Pain intensity was accessed in all eight studies with outcome measures of (VAS and NPRS).20–27 Pain relief was attained in most of the studies.20–24 Between-group differences for pain achieved by the thoracic spine thrust manipulation group were not only statistically significant but also clinically meaningful decrease in NPRS ranged from 34.4% to 40.6% in the TM group in immediate post-treatment, which was maintained for the 3 and 6-month follow-up similarly, patients receiving thoracic spine thrust manipulation experienced a greater decrease in neck pain between-group mean difference: 1.4; 95% CI (0.8–2.1) than did those receiving thoracic spine non–thrust mobilization within 10-minute post-intervention.20,21
The study that investigated the acute effects of single-level thoracic manipulation (STM) and multiple-level thoracic manipulations (MTM) on chronic mechanical neck pain result showed pain level at rest significantly decreased after MTM1.96; 95% CI (1.04–2.95) and 2.35; 95% CI (1.44–3.71) at 24-hour and 1-week follow-up, respectively.22 A study that assessed the effect of thoracic manipulation (TM) and deep craniocervical flexor (DCF) training on the pain intensity of the patients revealed that the improvements in pain intensity were more significant in group TM combined with DCF training (MD and SD =−3.8±0.6) than in the group that received DCF training alone after 10 weeks’ follow-up time.23 According to the post-intervention comparison of the upper thoracic manipulation and cervical stability training versus cervical stability training groups, there were significant differences in the pain values.24
However, the result of the study that compared right and left cervical manipulation to thoracic manipulation did not indicate a statistically significant group-by-time interaction for neck pain. All three groups experiencing a similar decrease in neck pain after the intervention.26 Similarly, a study conducted to investigate the effects of thoracic manipulation versus mobilization on chronic neck pain results at the 24-hour follow-up demonstrated VAS ratings significantly decreased for both treatment groups. However, there was no statistically significant difference in pain at rest between the three groups 24 hours after the intervention.25 In a study conducted to assess the immediate and short-term effects of upper thoracic spine manipulation on pain intensity and myoelectric activity of the sternocleidomastoid muscles in young women with chronic neck pain, no statistically significant differences were found in the intragroup or intergroup analyses of the experimental and placebo groups regarding the intensity of neck pain at rest in the immediate or short-term post-intervention evaluations.27
In this systematic review and meta-analysis, the immediate or short-term effect of thoracic manipulation on pain intensity in patients with chronic mechanical pain was examined by pooling data from eight studies that used self-reported NPRS and VAS. Meta-analysis of the five studies22–25,27 with a total 151 participants that measures pain by VAS (0–100mm) revealed a significant effect (MD −12.46; 95% CI: −17.29, −7.64; I2 = 52%, p < 0.001) (Figure 2), and a meta-analysis of three studies20,21,26 that measures pain by PNRS (0–10 points) revealed a significant effect (MD −0.85; 95% CI: −1.60, −0.10; I2 = 61%, p = 0.03) at immediate follow-up (Figure 3).
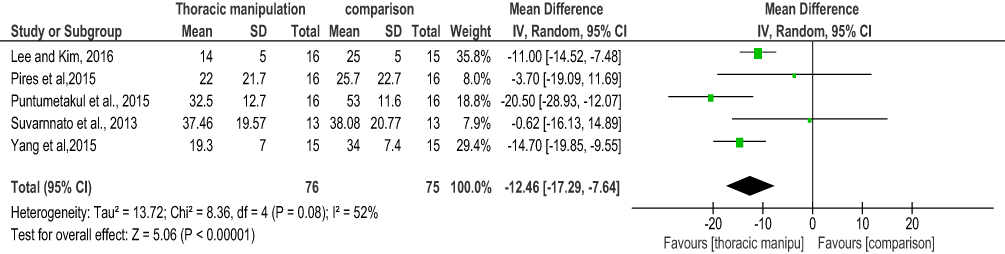 |
Figure 2 A meta-analysis on the effect of thoracic spine manipulation (TSM) for pain using visual analog scale (VAS). |
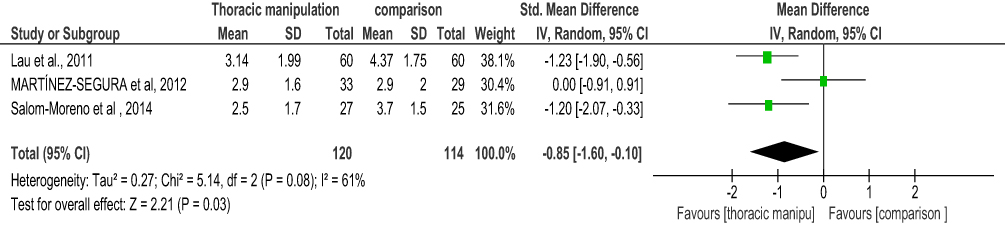 |
Figure 3 A meta-analysis on the effect of thoracic spine manipulation (TSM) for pain using numeric pain rating scale (NPRS). |
Neck Disability
The neck disability was accessed in three studies20,22,23 with 183 participants. The result of a study that compares experimental groups that received TM and a control group without the manipulative procedure revealed the TM group significantly decrease in neck disability compared to the control group with a between-group difference of 6–8.9 points.20 Similarly, in the study that investigated the acute effects of single-level (STM) and multiple-level thoracic manipulations (MTM) on CMNP the neck disability in the STM and MTM groups was significantly lowered by 8–12 points than the control group at 24-hour and 1-week follow-up.22 The NDI of a group that receives thoracic manipulation combined with deep craniocervical flexion training was reduced by a change of 5.9 points than that of a group with deep craniocervical flexion training alone.23
In this systematic review and meta-analysis, the immediate or short-term effect of thoracic manipulation on neck disability in patients with chronic mechanical pain was examined by pooling data from these three studies. Meta-analysis of the three studies20,22,23 with a total 183 participant measure neck disability revealed a significant effect (MD −6.46; 95% CI: −10.43–2.50; I2 = 57%, p = 0.001) at immediate follow-up (Figure 4).
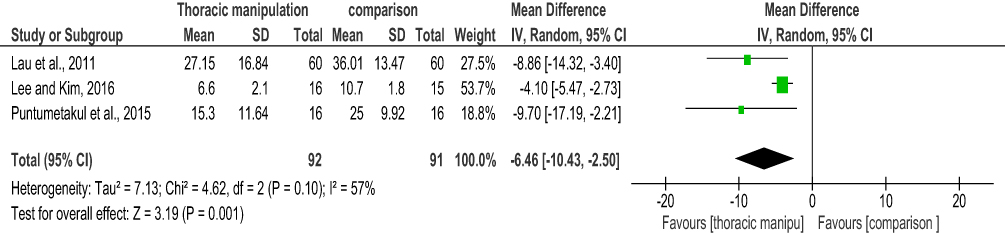 |
Figure 4 A meta-analysis on the effect of thoracic spine manipulation (TSM) on neck disability. |
Discussion
This systematic review and meta-analysis evaluated the effect of TSM in patients with chronic mechanical neck pain. To the limit of our knowledge, this is a preliminary systematic review study to evaluate the effect of TSM among subjects with chronic mechanical neck pain. This systematic review includes eight recent RCTs conducted within 10 years with a mean PEDro score of fair quality of evidence and the GRADE level of evidence found to be low to high for individual studies, and low-to-moderate overall evidence of the review.
The review provides evidence that thoracic manipulation alone or in combination with other treatments has produced an immediate and short-term effect to improve pain and neck disability among patients with chronic mechanical neck pain. The summary pooled effect of this meta-analysis favors the experimental or thoracic manipulation group with the effect size of −0.85 and-12.46 for the studies that assessed pain using PNRS and VAS measurements, respectively. Similarly, the summary effect on neck disability was −6.46 in favor of the thoracic manipulation group. This finding is consistent with the results of previous studies investigating thoracic manipulation for neck pain.17–19 TSM is more beneficial than thoracic mobilization, cervical mobilization, and standard care in the short-term, but no better than cervical manipulation or placebo thoracic spine manipulation to improve pain and disability among patients with mechanical neck pain (MNP)17 and nonspecific neck pain.18 Similarly, a systematic review that compares thoracic manipulation versus mobilization found that there is a significant amount of evidence for the short-term benefits of thoracic manipulation in treating patients with mechanical neck pain.19 This may support the concept of the intrinsic biomechanical linkage of the thoracic with the cervical spine, and disturbances in the biomechanics of the thoracic spine could be a primary contributor to neck pain.15
The current review used only participants with chronic mechanical neck pain. The included studies compare the intervention or thoracic manipulation with sham techniques or placebo,22,25,27 thoracic spine mobilization,21 and cervical manipulation.26 Co-interventions like infrared and educational material, craniocervical deep flexor exercise, and cervical stability training20,23,24 were included within the treatment session as these were also included in the comparison group which shows the differences in treatment effect to be attributed to the addition of TM in the experimental group. However, regardless of the comparative interventions, the results of the review suggested that treatment programs which incorporate thoracic spine thrust manipulation have larger treatment effects on the outcome measures. Including TM in the experiment group with co-interventions in both groups can bring clinically important differences in decreasing the pain and neck disability among the participants.
There is moderate heterogeneity among the included studies with I2 = 52%, 57%, and 61%. This might be because most of the included studies investigated different control interventions, different doses, and techniques of experimental intervention, another possible source of heterogeneity might be a large variance in sample size, from 26 in the Suvamnato study25 to 120 in the Lau study.20 Though this heterogeneity questions the overall validity of conducting meta-analysis, the included articles were fair in methodological quality and moderate level of evidence the authors consider meta-analysis valuable in providing an overall treatment effect of TSM as it is relevant and may aide in the clinical decision-making process in the management of individuals with MNP.
The studies described different thoracic spine thrust manipulation techniques. The specific site to which the thrust manipulation was applied also varied among studies, with four RCTs attempting to provide the thrust manipulation at one or more generic locations of the mid-thoracic and upper thoracic spine with a patient in supine line elbow flexed anteroposterior thrust manipulation was done.20,21,23,26 A study extrapolated on the decision for the location for thoracic spine thrust manipulation, recognizing that the technique does not target specific vertebral segments.33 In contrast, to suggested clinical practice, Suvernato et al attempted to specifically manipulate a single segment that was determined to be hypo-mobile during joint mobility testing.25 Puntamutakul et al investigated both single and multiple thoracic manipulations by comparing with the control group in which the therapist’s hand was placed without any treatment.22 Nevertheless, outcomes among the current studies did not appear to be influenced by the specific technique or rationale for application.
The follow-up intervals for all studies included in this review were relatively short. The current literature has individual reports for treatment effectiveness immediately following the treatment within 24 hours. Only one study assessed the post-intervention outcome immediately, 3-months, and at a 6-month follow-up time.20 Although various follow-up intervals have been included, long-term outcomes have not been reported.
Implications for Clinical Practice
This review and meta-analysis found that thoracic manipulation provide the immediate and short-term effect to improve pain and neck disability among patients with chronic mechanical neck pain. So clinicians or physiotherapists can apply the techniques of high-velocity low amplitude (HVLA) thoracic thrust manipulation as a choice of treatment to decrease pain and neck disability for patients with chronic mechanical neck pain.
Implications for Future Research
Future studies are needed to identify the most effective technique of thoracic thrust manipulation for each specific type of neck pain (acute, subacute, chronic, mechanical, and no mechanical). Its long-term effect with a longer follow-up time and to conduct a review of studies focused on the effect of thoracic spine manipulation as a single modality.
Strengths and Limitation
This review had strengths like it followed the PRISMA guidelines, registered in the PROSPERO, evidence quality of the studies assessed by PEDRo and GRADE, and all the included articles are recently published RCTs. Despite the strengths, this review had potential limitations. Inclusion of fair to low quality evidence articles, potential limitation of search, and inclusion of only English language articles as this might cause a chance of missing articles published in non-English languages. Lack of homogeneity among the included studies was also one of the main limitations, which might be due to the review was not specific to the follow-up time of the articles.
Conclusion
This systematic review and meta-analysis indicate that thoracic spine thrust manipulation reduces pain and neck disability in all adults with chronic mechanical neck pain compared with other interventions. While the findings of this review support the clinical benefit of TSM for reducing pain, clinicians should interpret these findings carefully as the overall quality of evidence ranges from low to moderate.
Ethical Approval
Ethical approval or patient consent was not required since the present study was a review of previously published literature.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoy DG, Protani M, De R, et al. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783–792. doi:10.1016/j.berh.2011.01.019
2. Hoy D, Brooks P, Blyth F, et al. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24(6):769–781. doi:10.1016/j.berh.2010.10.002
3. Constand MK, MacDermid JC. Effects of neck pain on reaching overhead and reading: a case–control study of long and short neck flexion. BMC Sports Sci Med Rehabil. 2013;5:21. doi:10.1186/2052-1847-5-21
4. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population. Eur Spine. 2006;15:834–848.
5. Hoy D, March L, Woolf A, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1309–1315. doi:10.1136/annrheumdis-2013-204431
6. Lipton RB, Schwedt TJ, Friedman BW. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602.
7. Cross KM, Kuenze C, Grindstaff T, et al. Thoracic spine thrust manipulation improves pain, range of motion, and self-reported function in patients with mechanical neck pain: a systematic review. J Orthop Sports Phys Ther. 2011;41(9):633–642. doi:10.2519/jospt.2011.3670
8. Cleland JA, Childs MJD, McRae M, et al. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10(2):127–135. doi:10.1016/j.math.2004.08.005
9. Fernández-De-Las-Peñas C, Cleland JA, Huijbregts P, et al. Repeated applications of thoracic spine thrust manipulation do not lead to tolerance in patients presenting with acute mechanical neck pain: a secondary analysis. J Man Manip Ther. 2009;17(3):154–162. doi:10.1179/jmt.2009.17.3.154
10. Gross A, Miller J, D’Sylva J, et al. Manipulation or mobilisation for neck pain: a Cochrane Review. Man Ther. 2010;15(4):315–333. doi:10.1016/j.math.2010.04.002
11. Furlan AD, Malmivaara A, Chou R, et al. 2015 updated method guideline for systematic reviews in the Cochrane back and neck group. Spine. 2015;40(21):1660–1673.
12. Blanpied PR, Gross AR, Elliott JM, et al. Neck pain: revision 2017: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American physical therapy association. J Orthop Sports Phys Ther. 2017;47(7):A1–A83. doi:10.2519/jospt.2017.0302
13. González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, et al. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial. Man Ther. 2009;14(3):306–313. doi:10.1016/j.math.2008.04.006
14. Vincent K, Maigne J-Y, Fischhoff C, et al. Systematic review of manual therapies for nonspecific neck pain. Joint Bone Spine. 2013;80(5):508–515. doi:10.1016/j.jbspin.2012.10.006
15. Flynn T, Wainner RS, Whitman JM, et al. The immediate effect of thoracic spine manipulation on cervical range of motion and pain in patients with a primary complaint of neck pain-technical notes. Orthop Divi Rev. 2007;2007:32.
16. Karas S, Olson Hunt MJ. A randomized clinical trial to compare the immediate effects of seated thoracic manipulation and targeted supine thoracic manipulation on cervical spine flexion range of motion and pain. J Man Manip Ther. 2014;22(2):108–114. doi:10.1179/2042618613Y.0000000052
17. Masaracchio M, Kirker K, States R, et al. Thoracic spine manipulation for the management of mechanical neck pain: a systematic review and meta-analysis. PLoS One. 2019;14(2):e0211877. doi:10.1371/journal.pone.0211877
18. Huisman PA, Speksnijder CM, de Wijer A. The effect of thoracic spine manipulation on pain and disability in patients with non-specific neck pain: a systematic review. Disabil Rehabil. 2013;35(20):1677–1685. doi:10.3109/09638288.2012.750689
19. Young JL, Walker D, Snyder S, et al. Thoracic manipulation versus mobilization in patients with mechanical neck pain: a systematic review. J Man Manip Ther. 2014;22(3):141–153. doi:10.1179/2042618613Y.0000000043
20. Lau HMC, Chiu TTW, Lam T-H. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain–a randomized controlled trial. Man Ther. 2011;16(2):141–147. doi:10.1016/j.math.2010.08.003
21. Salom-Moreno J, Ortega-Santiago R, Cleland JA, et al. Immediate changes in neck pain intensity and widespread pressure pain sensitivity in patients with bilateral chronic mechanical neck pain: a randomized controlled trial of thoracic thrust manipulation vs non–thrust mobilization. J Manipulative Physiol Ther. 2014;37(5):312–319. doi:10.1016/j.jmpt.2014.03.003
22. Puntumetakul R, Suvarnnato T, Werasirirat P, et al. Acute effects of single and multiple level thoracic manipulations on chronic mechanical neck pain: a randomized controlled trial. Neuropsychiatr Dis Treat. 2015;11:137. doi:10.2147/NDT.S69579
23. Lee K-W, Kim W-H. Effect of thoracic manipulation and deep craniocervical flexor training on pain, mobility, strength, and disability of the neck of patients with chronic nonspecific neck pain: a randomized clinical trial. J Phys Ther Sci. 2016;28(1):175–180. doi:10.1589/jpts.28.175
24. Yang J, Lee B, Kim C. Changes in proprioception and pain in patients with neck pain after upper thoracic manipulation. J Phys Ther Sci. 2015;27(3):795–798. doi:10.1589/jpts.27.795
25. Suvarnnato T, Puntumetakul R, Kaber D, et al. The effects of thoracic manipulation versus mobilization for chronic neck pain: a randomized controlled trial pilot study. J Phys Ther Sci. 2013;25(7):865–871. doi:10.1589/jpts.25.865
26. Martínez-Segura R, de-la-Llave-Rincón AI, Ortega-Santiago R, et al. Immediate changes in widespread pressure pain sensitivity, neck pain, and cervical range of motion after cervical or thoracic thrust manipulation in patients with bilateral chronic mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2012;42(9):806–814. doi:10.2519/jospt.2012.4151
27. Pires PF, Packer AC, Dibai-Filho AV, et al. Immediate and short-term effects of upper thoracic manipulation on myoelectric activity of sternocleidomastoid muscles in young women with chronic neck pain: a randomized blind clinical trial. J Manipulative Physiol Ther. 2015;38(8):555–563. doi:10.1016/j.jmpt.2015.06.016
28. Hutton B, Rochwerg B, Lamontagne F, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
29. Sherrington C, Herbert RD, Maher CG, Moseley AM. A database of randomized trials and systematic reviews in physiotherapy. Man Ther. 2000;5(4):223–226.
30. Walser RF, Meserve BB, Boucher TR. The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials. J Man Manip Ther. 2009;17(4):237–246. doi:10.1179/106698109791352085
31. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
32. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019;10:ED000142. doi:10.1002/14651858.ED000142
33. Cleland JA, Mintken PE, Carpenter K, et al. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial. Phys Ther. 2010;90(9):1239–1250. doi:10.2522/ptj.20100123
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.