")
Back to Journals » International Journal of General Medicine » Volume 14
Effectiveness of Chromosomal Microarray Analysis for Prenatal Diagnosis of Fetal Echogenic Intracardiac Focus: A Single-Center Experience
Authors Huang H , Cai M , Liu L, Xu L , Lin N
Received 19 March 2021
Accepted for publication 5 May 2021
Published 21 May 2021 Volume 2021:14 Pages 1991—1997
DOI https://doi.org/10.2147/IJGM.S311800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hailong Huang,1,* Meiying Cai,1,* Linyu Liu,1,2 Liangpu Xu,1 Na Lin1
1Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fujian Key Laboratory for Prenatal Diagnosis and Birth Defect, Fuzhou City, Fujian Province, 350001, People’s Republic of China; 2School of Clinical Medicine, Fujian Medical University, Fuzhou City, Fujian Province, 350122, People’s Republic of China
*These authors contributed equally to this work.
Correspondence: Liangpu Xu; Na Lin
Fujian Maternity and Child Health Hospital, Affiliated Hospital of Fujian Medical University, Fujian Key Laboratory for Prenatal Diagnosis and Birth Defect, No. 18 Daoshan Road, Gulou District, Fuzhou City, Fujian Province, 350001, People’s Republic of China
Tel +86-0591-87554929
Email [email protected]; [email protected]
Background: Echogenic intracardiac focus (EIF) is a common ultrasound finding during pregnancy. However, the correlation between fetal EIF and cardiac abnormality remains in dispute until now. The study aimed to examine the association of fetal EIF with chromosomal abnormality by means of chromosomal microarray analysis (CMA).
Materials and Methods: A total of 192 pregnant women with fetal EIF undergoing amniocentesis or umbilical cord blood puncture were recruited and assigned into groups A (8 cases with isolated EIF alone), B (75 cases with EIF and other cardiac malformations) and C (109 cases with EIF and extracardiac malformations). All fetuses underwent karyotyping analysis and CMA simultaneously. The detection of chromosomal abnormality and copy number variations (CNVs) were compared.
Results: Chromosomal karyotyping identified 5 fetuses with chromosomal abnormality, including 3 cases with trisomy 21, one fetus with Turner’s syndrome, and one fetus with chromosome 8 mosaicism, while CMA detected 6 additional fetuses with CNVs, including 2 fetuses with pathogenic CNVs and 4 fetuses with variants of uncertain significance (VOUS). There was no significant difference among groups A (0), B (5.33%) and C (6.42%) in terms of the prevalence of chromosomal abnormality (P> 0.05). Among the 4 fetuses with VOUS, pregnancy continued in 2 fetuses, and pregnancy was terminated in other 2 fetuses.
Conclusion: An isolated EIF may not correlate with chromosomal abnormality. However, CMA is recommended in fetuses with CMA complicated by other abnormal cardiac ultrasound findings, which facilitates the prediction of fetal outcomes during the genetic counseling and precision assessment of prognosis.
Keywords: echogenic intracardiac focus, chromosomal microarray analysis, copy number variation, prenatal diagnosis, pregnant outcome
Introduction
Echogenic intracardiac focus (EIF), a common ultrasound finding during pregnancy, is described to be a local echogenic area appearing in single-sided or bilateral cardiac cavity.1–3 It is estimated that EIF is detected in 5% of second-trimester ultrasound examinations.4–6 Previous studies have demonstrated that fetal EIF is associated with an increased risk of Down syndrome and trisomy 13 (T13),7–9 and fetuses with an EIF may have other structural cardiac malformations.10 The identification of an EIF by ultrasonography is an incentive for further prenatal diagnoses to evaluate the risk of fetal outcomes.11 Chromosomal karyotyping analysis has been found to fail to detect copy number variations (CNVs) in small fragments, and chromosomal microarray analysis (CMA) may be used as a supplement to conventional karyotyping.12–14 This study aimed to examine the association between fetal EIF and the risk of chromosomal abnormality, and our data may provide insights into prenatal diagnosis and genetic counseling in fetuses with an EIF.
Subjects and Methods
Subjects
A total of 192 pregnant women with fetal EIF undergoing amniocentesis or umbilical cord blood puncture at the Center for Prenatal Diagnosis of Fujian Provincial Maternity and Children’s Hospital (Fuzhou, China) from December 2015 to December 2018 were recruited. The pregnant women had a mean age of 29 years (range, 21 to 41 years) and gestational ages of 18+2 to 34+5 weeks. All pregnant women had no medical history of hypertension or diabetes, and all women had no viral infections or were exposed to known teratogens during pregnancy. All fetuses were assigned into three groups. Fetuses in Group A had isolated EIF alone (n = 8), and those in Group B had EIF and other cardiac malformations (n = 75), while fetuses with EIF and abnormal extracardiac ultrasound findings were assigned to Group C (n = 109).
Karyotype Analysis
Amniotic fluid (122 samples) and umbilical cord blood samples (70 samples) were collected from the 192 fetuses through B-mode ultrasound-guided abdominal puncture, amniocentesis and amniocentesis, respectively. All prenatal samples were routinely cultured, mounted on slides and subjected to G-banding karyotype analysis on a GSL-120 Streamlines Cytogenetic Analysis System (Leica Microsystems; Mannheim, Germany). At least 40 karyotypes were counted for each case, and 5 karyotypes were randomly selected for analysis.
CMA Detection
CMA detection was performed as described previously.15 Briefly, approximately 10 mL of amniotic fluid was sampled from each fetus and centrifuged, and the sediment was collected. Genomic DNA was extracted from amniotic fluid cells using the QIAampDNA Blood Mini Kit (Qiagen; Hilden, Germany), digested, amplified, purified, fragmented, labeled and hybridized to the array on the Affymetrix SNP Array 6.0 (Affymetrix; Santa Clara, CA, USA). The CytoScan HD array, which includes the copy number variation (CNV) probe and SNP probe, may detect CNV, mosaic (mosaic proportion >10%) and loss of heterozygosity (LOH). All data analyses were performed using the software Chromosome Analysis Suite (ChAS) version 3.2 (Affymetrix; Santa Clara, CA, USA), and the interpretation of CNVs was identified using online public databases, including the database of genomic variants (DGV, http://projects.tcag.ca/variation), the DECIPHER database (htts://decinher.sanger.ac.uk/), the OMIM database (http://www.omim.org), the International Standards for Cytogenomic Arrays (ISCA) Consortium and Public Database (https://www.iscaconsortium.org/), the CAGdb database (http://www.cagdb.org/), the CHDWiki database and the NCBI database. CNV was classified as pathogenic, variants of uncertain significance (VOUS) and benign, and pathogenic CNVs detected by CMA were further validated using fluorescence in situ hybridization (FISH) assay. Peripheral blood was sampled from the parents of the fetus with VOUS for CMA detection, and the type of CNV was identified by means of CMA and pedigree analysis.
Ethical Statement
This study was approved by the Ethics Review Committee of Fujian Provincial Maternity and Children’s Hospital. All procedures were performed following the Declaration of Helsinki, as well as international and national laws, guidelines and regulations. All pregnant women and their spouses received prenatal genetic counseling and signed informed consent with a detailed description of invasive diagnosis and CMA.
Statistical Analysis
All statistical analyses were conducted using the statistical software SPSS version 20.0 (SPSS, Inc.; Chicago, IL, USA). The detection of CNVs was compared among groups using chi-square test or Fisher’s exact test, with a P value of <0.05 indicative of statistical significance.
Results
Karyotype Analysis
Among the 192 fetuses with EIF, chromosomal karyotyping identified 5 cases with chromosomal abnormality (2.6% prevalence), including 3 fetuses with T21, one fetus with Turner’s syndrome, and one fetus with chromosome 8 mosaicism.
Fetal Chromosomal Abnormality by CMA
CMA was successfully performed in all 192 samples, and the overall prevalence of chromosomal abnormality was 5.73%, which included chromosomal abnormality (5 fetuses) and CNVs (6 fetuses). Inconsistent ratio of chromosome 8 mosaicism was detected between karyotyping (47,XY,+8[5]/46,XY[140]) and CMA (8p23.3q24.3(158,048–146,295,771)×2–3mosaicism), and the six fetuses with CNVs included 2 fetuses with pathogenic CNVs and 4 fetuses with VOUS (Table 1).
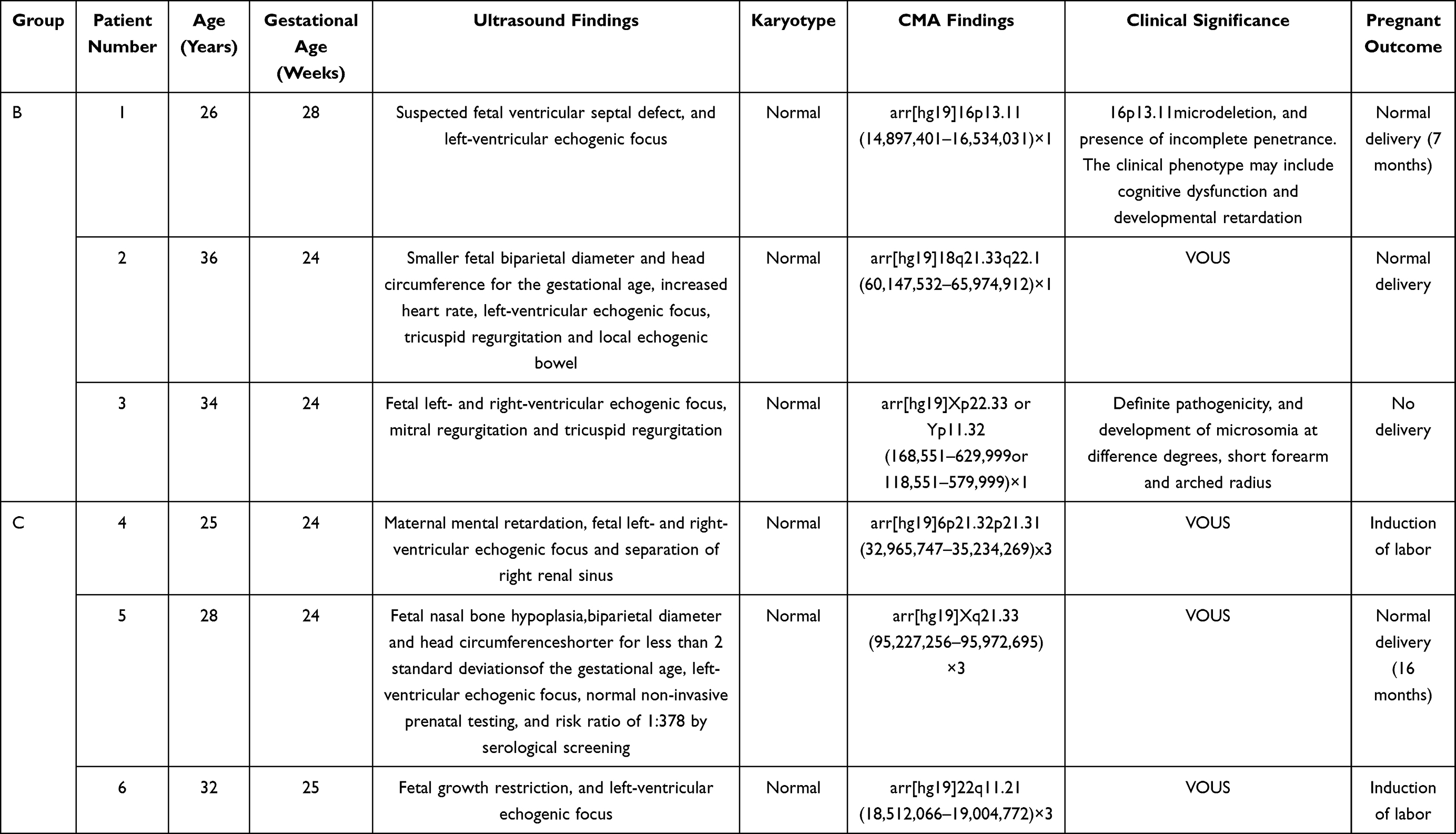 |
Table 1 Demographic, Clinical Features and Pregnant Outcomes of 7 Fetuses with Chromosomal Abnormalities |
Detection of CNVs in Different Groups
The rate of CNVs detected by CMA in group A, B and C was 0/8 (0%), 4/75 (5.33%), 7/109 (6.42%), respectively. In addition, there was no significant difference in the detection of CNVs among groups A, B and C (P > 0.05) (Table 2).
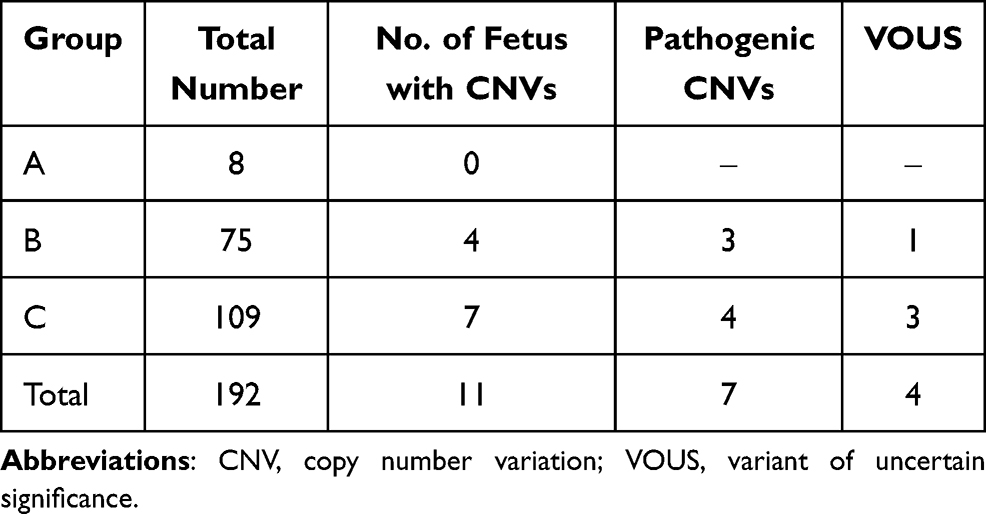 |
Table 2 Detection of CNVs in Fetuses with Diverse Ultrasound Findings |
Fetal Follow-Up Outcomes
The pregnancy was terminated in 5 fetuses with abnormal chromosome numbers. Of the 4 fetuses with VOUS, pregnancy termination was done in two fetuses (case numbers 4 and 6), and pregnancy continued in the other two fetuses (case numbers 2 and 5), both having good development after birth. Of the remaining 2 fetuses with pathogenic CNVs, one was terminated for pregnancy and one had no abnormal phenotypes 7 months after birth (Table 2).
Discussion
As an ultrasound soft marker, the prevalence of EIF is estimated to be 2% to 6% on fetal echocardiography.7,16 Previous studies have shown a high rate of fetal cardiac abnormality if EIF occurs in the left or right ventricle alone, or in bilateral ventricles.10,17–19 However, fetal EIF was also found to be not associated with a significant increase in the risk of structural cardiac abnormality.20 Precision diagnosis of EIF by echocardiography is therefore of great importance for the decision of pregnancy.11
EIF is most likely to gradually weaken, shrink and even disappear with the increase in the gestational age.1 In this study, all fetuses with an isolated EIF were followed up, and no severe diseases or symptoms were seen. This is not in agreement with previous studies showing a correlation between fetal EIF and congenital heart diseases.10,21,22 Currently, karyotyping, FISH, multiplex ligation-dependent probe amplification (MLPA) and CMA are major tools used to detect the chromosomal abnormality in fetuses with ultrasound soft markers.23,24 Chromosomal karyotype analysis is limited by the success rate of culture and the resolution, while CMA is effective to detect abnormality of chromosomal fragments with >1 kb in size and microduplication and microdeletion syndromes.25 The introduction and developments of CMA allow the detection of chromosomal abnormality which is not identified by karyotyping, and such an assay has been extensively employed in the diagnosis of fetal growth restriction and retardation, mental disorder, autism and multi-organ malformations.26–28
In the current study, we employed CMA to detect 192 fetuses with EIF, and no chromosomal abnormality was found in fetuses with EIF alone, which may be associated with the small sample size of the isolated EIF. In addition, CMA detected a 5.33% prevalence rate of chromosomal abnormality in Group B and 6.42% in Group C, with no significant difference seen between these two groups (P > 0.05). Our data demonstrate that EIF is not associated with an increase in the risk of fetal cardiac malformations and shows no significant correlations with fetal structural cardiac abnormality. In this study, CMA showed a 5.73% overall detection of chromosomal abnormality, which increased by 3.13% as compared to karyotype analysis, and among fetuses with normal karyotypes, CMA still identified chromosomal microdeletions/microduplications, and pathogenic CNVs. Previous studies have proved that CMA is feasible to improve the detection of chromosomal abnormality and may serve as a supplement for conventional karyotype analysis during the prenatal diagnosis.12–14 Taken together, CMA is therefore strongly recommended for prenatal diagnosis of EIF, which may provide more accurate genetic proof for prenatal counseling and prediction of fetal outcomes.12
In the present study, CMA detected chromosomal mosaicism in a fetus and CNVs in 6 fetuses with EIF, in addition to aneuploidy. CMA detected a mosaicism of the 8p23.3q24.3 in one case, which is reported to manifest mental retardation, cardiac malformation and dysgenesis of the corpus callosum;29 however, there are also fetuses with a mosaicism of the 8p23.3q24.3 presenting normal phenotypes.30 Mosaicism remains a major concern during the prenatal genetic counseling.31 Since mosaic cells are present in different embryonic layers of diverse proportions, and fetuses with a mosaicism present a wide range of clinical phenotypes, it is very difficult to predict the pregnant outcomes of fetuses with a low-level T8mosaicism in amniotic fluid or umbilical cord blood samples.32 Previous studies have reported that a chromosome 8 mosaicism has a primary ultrasound feature of intra-uterine growth retardation or shows no remarkable phenotype.30 The fetus with a chromosome 8 mosaicism detected by CMA in this study presented with multiple cardiac abnormalities, which is in agreement with the clinical phenotype caused by a mosaicism, suggesting that cardiac abnormality may be indicative of a chromosome 8 mosaicism during the prenatal diagnosis. In addition, we detected an Xp22.33 or Yp11.32 microdeletion in Case 3, and such a microdeletion is likely to be associated with the SHOX gene.33 Loss of the SHOX gene function may cause microsomia, Madelung’s deformity of the wrist, joint movement restriction and Leri-Weill dyschondrosteosis.34
Although CMA has shown great values in prenatal diagnosis, this assay may detect VOUS, pathogenic CNVs in adulthood, and disease carriers.35 Results from the NICHD trial showed that CMA identified 1.8% of the study fetuses with possible benign CNVs and 1.6% with possible pathogenic CNVs.36 This VOUS may be attributed to rare or new CNVs, or due to variable penetrance.37 In this study, CMA identified a 1.6 Mb deletion on the 16p13.11 region. This region is overlapped with the 16p13.11 recurrent region (including the MYH11 gene), which contains susceptible foci of neurocognitive disorders.38 Patients with a chromosome 16p13.11 microdeletion syndrome mainly manifest bradykinesia, facial deformity, microcephaly, gastroesophageal reflux disease (GERD) and congenital heart defects, and the carriage of chromosome 16p13.11 microdeletions is less than 1% in normal populations.39 Similar cases have been reported in DGV, DECIPHER and ISCA databases, which show the definite pathogenicity of 16p13.11 microdeletions; however, 16p13.11 microdeletion is also considered as VOUS or benign and incomplete clinical penetrance. Our follow-up results showed no obvious abnormality in this fetus 7 months after birth, which may be attributed to the benign CNVs or limitation of the follow-up period that is insufficient to identify the development of potential neurocognitive disorders. In the current study, we detected that Case 6 carried 22q11.21 microduplications, which is partially overlapped with the chromosome 22q11.2 recurrent (DGS/VCFS) region (proximal, A-B); however, this region did not contain key pathogenic genes. The frequency of 22q11.21 microduplication is very likely to be higher than that of 22q11.2 microdeletion in normal populations, and this microduplication is approximately 3 Mb in size, which has clinical phenotypes of cardiac defects, velopharyngeal insufficiency, hearing impairment, growth retardation, cognitive deficits, behavioral abnormality, epilepsy and facial deformity.40 In this study, Case 6 had the ultrasound findings associated with the phenotype of CNVs, and we found no insufficient pathogenic proof; however, the likelihood of pathogenicity cannot be excluded. Due to the presence of VOUS, many microduplications and microdeletions of unknown clinical significance require further pedigree analyses to validate their associations with pathogenicity. However, many patients refuse to undergo further pedigree analyses due to economic factors, which is a concern during the prenatal diagnosis.
Conclusions
In summary, CMA is effective to improve the detection of chromosomal abnormality, and shows a high sensitivity for detection of chromosomal microdeletions or microduplications. The results of the present study demonstrate a low proportion of chromosomal abnormality in fetuses with an isolated EIF. However, CMA is recommended in fetuses with CMA complicated by other abnormal cardiac ultrasound findings, which facilitates the prediction of fetal outcomes during the genetic counseling and precision assessment of prognosis.
Acknowledgments
This study was supported by a grant from the Natural Science Foundation of Fujian Province (grant no. 2017J01238).
Disclosure
The authors declare no competing interests.
References
1. Winn VD, Sonson J, Filly RA. Echogenic intracardiac focus: potential for misdiagnosis. J Ultrasound Med. 2003;22(11):1207–1214. doi:10.7863/jum.2003.22.11.1207
2. Maria DR, Paola P, Francesco C, et al. Sonographie marker8 for early diagnosis of fetal malformations. World J Radio. 2013;28(10):356–371.
3. Bradley KE, Santulli TS, Gregory KD, et al. An isolated intracar-diac echogenic focus as a marker for aneuploidy. Am J Obstet Gynecol. 2005;192(6):2021–2026. doi:10.1016/j.ajog.2005.03.033
4. Rodriguez R, Herrero B, Bartha JL. The continuing enigma of the fetal echogenic intracardiac focus in prenatal ultrasound. Curr Opin Obstet Gynecol. 2013;25(2):145–151. doi:10.1097/GCO.0b013e32835e14eb
5. Benacerraf BR. The role of the second trimester genetic sono-gram in screening for fetal Down syndrome. Semin Perinatol. 2005;29(6):386–394. doi:10.1053/j.semperi.2005.12.003
6. Sood M, Rochelson B, Krantz D, et al. Are second trimester minor sonographic maFkel8 for Down syndrome useful in patients who have undergone fimt-trimester combined screening. Am J Obstet Gynecol. 2010;203(4):408–411. doi:10.1016/j.ajog.2010.05.030
7. Lorente AMR, Moreno-Cid M, Rodríguez MJ, et al. Meta-analysis of validity of echogenic intracardiac foci for calculating the risk of down syndrome in the second trimester of pregnancy. Taiwan J Obstet Gynecol. 2017;56(1):16–22. doi:10.1016/j.tjog.2016.11.002
8. Winter TC, Anderson AM, Cheng EY, et al. Echogenic intracardiac focus in 2nd-trimester fetuses with trisomy 21: usefulness as a US marker. Radiology. 2000;216(2):450–456. doi:10.1148/radiology.216.2.r00au32450
9. Agathokleous M, Chaveeva P, Poon LC, Kosinski P, Nicolaides KH. Meta-analysis of second-trimester markers for trisomy 21. Ultrasound Obstet Gynecol. 2013;41(3):247–261. doi:10.1002/uog.12364
10. Chiu G, Zhao A, Zhang B, Zhang T. Intracardiac echogenic focus and its location: association with congenital heart defects. J Matern Fetal Neonatal Med. 2019;32(18):3074–3078. doi:10.1080/14767058.2018.1558200
11. Bettelheim D, Deutinger J, Bernaschek G. The value of echogenic foci (‘golfballs’) in the fetal heart as a marker of chromosomal abnormalities. Ultrasound Obstet Gynecol. 1999;14(2):98–100. doi:10.1046/j.1469-0705.1999.14020098.x
12. Levy B, Wapner R. Prenatal diagnosis by chromosomal microarray analysis. FertilSteril. 2018;109(2):201–212.
13. Wapner RJ, Martin CL, Levy B, et al. Chromosomal microarray versus karyotyping for prenatal diagnosis. N Engl J Med. 2012;367(23):2175–2184. doi:10.1056/NEJMoa1203382
14. Pauta M, Grande M, Rodriguez-Revenga L, Kolomietz E, Borrell A. Added value of chromosomal microarray analysis over karyotyping in early pregnancy loss: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2018;51(4):453–462. doi:10.1002/uog.18929
15. Huang H, Cai M, Wang Y, Liang B, Lin N, Xu L. SNP array as a tool for prenatal diagnosis of congenital heart disease screened by echocardiography: implications for precision assessment of fetal prognosis. Risk Manag Healthc Policy. 2021;14:345–355. doi:10.2147/RMHP.S286001
16. Mirza FG, Ghulmiyyah L, Tamim H, et al. Echogenic intracardiac focus on second trimester ultrasound: prevalence and significance in a Middle Eastern population. J Matern Fetal Neonatal Med. 2016;29(14):2293–2296. doi:10.3109/14767058.2015.1083549
17. Wei M, Zhang J, Liu ZY, et al. Correlation between fetal intracardiac echogenic foci and chromosome and heart function. Chin Med J. 2018;98(47):3864–3867.
18. Wax JR, Donnelly J, Carpenter M, et al. Childhood cardiac function after prenatal diagnosis of intracardiac echogenic foci. J Ultrasound Med. 2003;22(8):783–787. doi:10.7863/jum.2003.22.8.783
19. Degani S, Leibovitz Z, Shapiro I, Gonen R, Ohel G. Cardiac function in fetuses with intracardiac echogenic foci. Ultrasound Obstet Gynecol. 2001;18(2):131–134. doi:10.1046/j.1469-0705.2001.00433.x
20. Wolman I, Jaffa A, Geva E, et al. Intracardiac echogenic focus: no apparent association with structural cardiac abnormality. Fetal Diagn Ther. 2000;15(4):216–218. doi:10.1159/000021009
21. Carriço A, Matias A, Areias JC. How important is a cardiac echogenic focus in a routine fetal examination? Rev Port Cardiol. 2004;23(3):459–461.
22. Chitra N, Vijayalakshmi IB. Fetal echocardiography for early detection of congenital heart diseases. J Echocardiogr. 2017;15(1):13–17. doi:10.1007/s12574-016-0308-2
23. Norton ME. Follow-up of sonographically detected soft markers for fetal aneuploidy. SeminPerinatol. 2013;37(5):365–369.
24. Stefanovic V. Soft markers for aneuploidy following reassuring first trimester screening: what should be done? Curr Opin Obstet Gynecol. 2015;27(2):151–158.
25. Lin CZ, Qi BR, Hu JS, Huang YD, Huang XQ. Chromosome 15q13 microduplication in a fetus with cardiac rhabdomyoma: a case report. MolCytogenet. 2019;12:24.
26. Xie Y, Sun X. Chromosomal microarray analysis in prenatal diagnosis. Clin Exp Obstet Gynecol. 2017;44(2):177–179.
27. Dugoff L, Norton ME, Kuller JA. The use of chromosomal microarray for prenatal diagnosis. Am J Obstet Gynecol. 2016;215(4):B2–B9. doi:10.1016/j.ajog.2016.07.016
28. Lo JO, Shaffer BL, Feist CD, Caughey AB. Chromosomal microarray analysis and prenatal diagnosis. Obstet Gynecol Surv. 2014;69(10):613–621.
29. Chen CP, Hsu CY, Chern SR, Wu PS, Chen SW, Wang W. Prenatal diagnosis of mosaic trisomy 8 by amniocentesis in a fetus with ventriculomegaly and dysgenesis of the corpus callosum. Taiwan J Obstet Gynecol. 2020;59(1):127–129. doi:10.1016/j.tjog.2019.11.020
30. Saks E, Mccoy MC, Damron J, Kelly TE. Confined placental mosaicism for trisomy 8 and intra-uterine growth retardation. Prenat Diagn. 1998;18(11):1202–1204.
31. Eggermann T, Soellner L, Buiting K, Kotzot D. Mosaicism and uniparentaldisomy in prenatal diagnosis. Trends Mol Med. 2015;21(2):77–87. doi:10.1016/j.molmed.2014.11.010
32. Verma RS, Kleyman SM, Conte RA. Chromosomal mosaicisms during prenatal diagnosis. Gynecol Obstet Invest. 1998;45(1):12–15. doi:10.1159/000009915
33. Huber C, Cusin V, Le Merrer M, et al. SHOX point mutations in dyschondrosteosis. J Med Genet. 2001;38(5):323. doi:10.1136/jmg.38.5.323
34. Falcinelli C, Iughetti L, Percesepe A, et al. SHOX point mutations and deletions in Leri-Weill dyschondrosteosis. J Med Genet. 2002;39(6):E33. doi:10.1136/jmg.39.6.e33
35. Leavitt K, Goldwaser T, Bhat G, Kalia I, Klugman SD, Dolan SM. Chromosomal microarray in prenatal diagnosis: case studies and clinical challenges. Per Med. 2016;13(3):249–255. doi:10.2217/pme-2015-0003
36. Stoll BJ, Hansen NI, Bell EF, et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010;126(3):443–456. doi:10.1542/peds.2009-2959
37. Clift K, Macklin S, Halverson C, McCormick JB, Abu Dabrh AM, Hines S. Patients’ views on variants of uncertain significance across indications. J Commun Genet. 2020;11(2):139–145. doi:10.1007/s12687-019-00434-7
38. Smith AE, Jnah A, Newberry D. Chromosome 16p13.11 microdeletionsyndrome in a newborn: a case study. Neonatal Netw. 2018;37(5):303–309. doi:10.1891/0730-0832.37.5.303
39. Nagamani SC, Erez A, Bader P, et al. Phenotypic manifestations of copy number variation in chromosome 16p13.11. Eur J Hum Genet. 2011;19(3):280–286. doi:10.1038/ejhg.2010.184
40. Yu A, Turbiville D, Xu F, et al. Genotypic and phenotypic variability of 22q11.2 microduplications: an institutional experience. Am J Med Genet A. 2019;179(11):2178–2189. doi:10.1002/ajmg.a.61345
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.