")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Effectiveness of Alcohol and Aldehyde Spray Disinfectants on Dental Impressions
Authors Al Shikh A, Milosevic A
Received 3 October 2019
Accepted for publication 14 January 2020
Published 13 February 2020 Volume 2020:12 Pages 25—30
DOI https://doi.org/10.2147/CCIDE.S233336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Ayesha Al Shikh,1 Alexander Milosevic2
1Hamdan Bin Mohammed College of Dental Medicine, Mohammed Bin Rashid University (MBRU) of Medicine and Health Sciences, Dubai, United Arab Emirates; 2Department of Prosthodontics, Hamdan Bin Mohammed College of Dental Medicine, Mohammed Bin Rashid University (MBRU) of Medicine and Health Sciences, Dubai, United Arab Emirates
Correspondence: Alexander Milosevic
Tel +971 52 9548125
Email [email protected]
Background: The gold standard for disinfection of dental impressions is by immersion although spray techniques are also available. This study compared the effectiveness of alcohol and aldehyde spray disinfectants on analogue dental impressions in a hospital setting.
Materials and Methods: Impressions were swabbed after removal from the mouth (pre-disinfection) and after spraying (post-disinfection) with either a non-aldehyde alcohol-based disinfectant, Bossklein (Silsden, W Yorks, BD20 0EF, UK) or a glutaraldehyde-based alcohol-free disinfectant, MD520 (Dürr Dental, 74321 Bietigheim-Bissingen, Germany). Swabs were transported to the microbiology laboratory in Amies medium and plated onto sheep blood agar within 2 hrs. Plates were incubated for 3 days at 37°C then at room temperature for 3 days. After incubation, all plates were examined for microbial growth.
Results: A total of 87 impressions were assessed (alginate = 41; poly-vinyl siloxane (PVS) = 31; polyether = 15). The counts were categorized into two groups: no growth or growth present. Post-disinfection contamination was present on six alginate and six PVS impressions but only one polyether impression (x2 = 1.27, P > 0.05, NSS). Analysis of post-disinfection growth according to impression and disinfectant found significantly more contaminated PVS impressions with the alcohol-based spray than with the aldehyde spray (x2 = 5.37, p < 0.05). Disinfection with the aldehyde-based spray resulted in only two contaminated impressions, both in alginate.
Conclusion: Alcohol-based spray disinfection of dental impressions may be less effective than aldehyde spray and full immersion of impressions is recommended. Careful wetting or soaking of all surfaces of impressions is very important when using a spray.
Keywords: spray disinfection effectiveness, dental impressions, contamination
Introduction
Prevention of cross-infection between the dental surgery and the laboratory is of paramount importance to protect patients and staff.1 Dental impressions are considered potentially infectious items as they are contaminated with patient’s saliva and blood. Pathogens, if present in high enough number, can survive several days on impressions and then can be transferred onto set gypsum material.2
Impression materials cannot tolerate heat sterilization therefore they must be disinfected chemically. Sterilization is a process intended to kill all microorganisms and is the highest level of microbial decontamination that can be achieved. Disinfection is a less lethal process than sterilization and is intended to kill disease-producing microorganisms but not bacterial endospores.3
Disinfectants are classified into three levels (high, intermediate and low), based on their efficiency against vegetative bacteria, tubercle bacilli, fungal spores, lipid and non-lipid containing viruses and bacterial endospores.4 Examples of each type are: ethylene oxide gas and immersion glutaraldehyde solutions for the high level. Chlorine compounds, formaldehyde, iodophors, alcohol and phenolic disinfectants are intermediate level. Simple quaternary compounds, simple phenolics and detergents are considered low level and are not used in dentistry.4 The Spaulding classification states the required level of processing/reprocessing for critical, semi-critical and non-critical items of medical equipment/devices.5 Critical items are those that enter sterile tissue such as dental implants and require sterilization, semi-critical are those that contact mucous membranes such as dental impressions and require high-level disinfection whilst non-critical devices contact intact skin such as a Willis bite gauge and only need low-level disinfection.5 Dental impressions thus pose an intermediate or semi-critical risk to laboratory workers and require an intermediate to high level of disinfection as sterilization is not possible.5 Dental impressions must be cleaned preferably by brushing and/or rinsing under running water of all debris including blood and saliva followed by disinfection. The British Dental Association Health Technical Memorandum 01–05 recommends disinfection and decontamination of dental impressions prior to sending them to laboratories and furthermore states that dentists have the sole responsibility of doing so.6 All impressions should be labelled accordingly.6
Both immersion and spraying have been recommended for disinfection of impressions. The advantage of spraying is that it uses less solution, and often the same disinfectant can be used for general disinfection of operatory surfaces but immersion is considered the most reliable because all exposed surfaces of the tray material are covered by the disinfectant.7–9 Immersion, however, may lead to distortion and/or surface changes because of imbibition in the case of gels, such as alginate, and polyethers can expand and swell excessively after 10 mins immersion.10–14 Such a technique, in comparison to spraying, minimizes the risks of incomplete coverage and the hazard of disinfectant inhalation by the user.13 On the other hand, spraying is considered by some as a suitable disinfection method that also decreases the chances of impression distortion that may occur following prolonged immersion.15 Considerations in selecting a disinfectant and technique include the type of impression material and personal preference. The ADA urges all practicing dentists, dental auxiliaries and dental laboratories to employ appropriate infection control procedures as described in the 2003 CDC Guidelines and 2016 CDC Summary.16,17 Best practice is not always followed as 72% of impressions received at a Swedish dental laboratory yielded bacterial growth and a questionnaire survey of laboratory technicians in Jordan reported that 71% of respondents did not receive labelled impressions from dentists and were thus uninformed regarding disinfection status of impressions.2,18 Consequently, some of the responding laboratories disinfected the impression upon receipt, mainly by spraying.18
The effectiveness of various spray disinfectants with different concentrations and contact time on irreversible hydrocolloid impression materials (alginate) found that not all the ADA-approved concentrations of surface disinfectants work equally well. Diluted sodium hypochlorite (0.5%) was very effective against S. aureus, S. viridans and B. subtilis, while a 5.25% concentration of sodium hypochlorite was the most effective disinfectant overall and required the shortest contact time of 1 min.19
The effectiveness of four different disinfectant solutions (Dimenol, Perform-ID, MD 520, and Haz-tabs) on three commonly used impression materials (alginate, polyether, and polyvinyl siloxane) established that impressions sprayed with Dimenol for a 15 mins contact time and those immersed in 2% solution of Perform-ID for 10 mins were found to be completely free of microorganisms but alginate specimens retained an average of 49 to 74 times more microorganisms than polyether and PVS, respectively. The differences between the 2 elastomeric impression materials, however, were insignificant. Polyether specimens retained only 1.5 times more microorganisms than PVS specimens.20 Spray disinfection is widely used but few studies have determined its effectiveness, which is the degree of benefit under real-world clinical conditions.
This study aimed to determine the effectiveness of 2 spray disinfectants, one alcohol-based and the other alcohol-free but containing glutaraldehyde for decontamination of dental impressions in a hospital setting.
Materials and Methods
The local Research Ethics Committee approved this study (30/09/2017) as exempt since the microbiological investigation was laboratory-based, no new treatment was introduced as normal clinical practice was conducted and there was no random allocation to intervention groups meaning this was service evaluation.21 None of the impressions and microbial counts had any patient identifier as this was not relevant. All patients consented to have impressions taken as part of their treatment. The effectiveness of spray disinfectants on three dental impression materials: alginate (Tropicalgin, Zhermack), polyether (Impregum Penta, 3M ESPE) and poly-vinyl siloxane (Express XT, 3M ESPE) was assessed. Two spray disinfectants, the alcohol-based Bossklein (Silsden, W Yorks, BD20 0EF, UK) and glutaraldehyde based but alcohol-free MD520 (Dürr Dental, 74321 Bietigheim-Bissingen, Germany) were assessed for antimicrobial effectiveness. Maxillary and mandibular full arch impressions were swabbed from the same gingival area after rinsing under running tap water for 10 seconds but before spraying with the disinfectant (pre-disinfection) and a second swab was taken 10 mins after spraying (post-disinfection). The impressions were taken on the prosthodontic and orthodontic clinics and sprayed by 1 dentist or by one of four dental nurse assistants who had no prior knowledge which impression was to be swabbed. Impressions were selected arbitrarily over a time framed period of 2 months and thus form a convenience sample. The alcohol-based disinfectant (Bossklein) is contained in a hand held spray bottle and in order to have a meaningful comparison, the Dürr Hygojet® spray system was not used as this closed box system has pneumatically controlled air and water pressure for spraying MD520. Therefore, the glutaraldehyde-based disinfectant was decanted from its container into a similar hand held spray bottle as the alcohol-based disinfectant. This helped standardize the method of delivery. Clinic staff had no prior knowledge when swabs were to be taken and therefore the study was under real-world conditions. Once the impressions were taken, they were left to dry for a minimum of 10 mins, prior to being swabbed for the second time, washed again under running cold tap water and sealed in plastic bags as per normal practice. Storage was at room temperature. The swabs were run across the palatal or lingual aspects of teeth in the impression from left to right whilst rolling the swab. Amies transport medium swabs were used and returned to the microbiology laboratory in the sterile tubes provided. Two swabs were thus taken for each impression, one immediately after rinsing under running tap water and a second after spraying the disinfectant. All swabs were plated onto sheep blood agar (HiMedia Laboratories Pvt Ltd., Mumbai, 400086, India) within 2 hrs at Medlab Analytica, Dubai. Plates were incubated for 3 days at 37°C then at room temperature for 3 days. After incubation, all plates were examined for growth and Colony Forming Units were counted using the grid contact plate and expressed as CFU/cm2. The counts were described as “no growth” when there was <25 CFU/cm2 after the incubation period and considered as “growth” when ≥25 CFU/cm2 were present. This cut-off was chosen as experimental studies have shown poor accuracy in plate counts below 25.22
All data were entered into SPSS v20. The number of contaminated impressions before and after disinfection for each impression material was compared using the chi square test with the level of significance set at p≤0.05.
Results
A total of 87 impressions were analysed; 41 alginate, 31 poly-vinyl siloxane (PVS) and 15 polyether. Results are presented for pre- and post-disinfection for type of impression and type of disinfectant. Table 1 shows the presence or absence of bacterial growth according to impression material before disinfection. The number of contaminated polyether impressions pre-disinfection were significantly lower than the other two impression materials (x2 = 7.75, p<0.05).
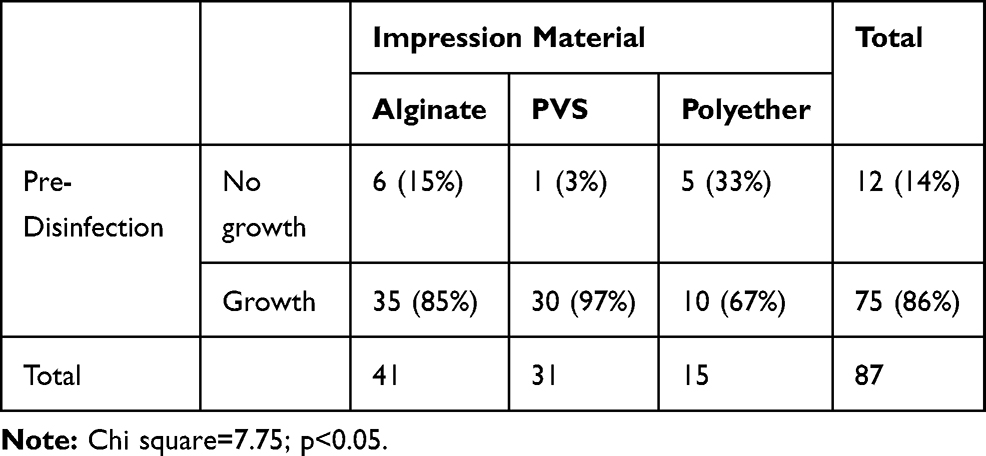 |
Table 1 The Number of Contaminated Impressions Pre-Disinfection According to the Type of Impression Material |
After disinfection, there were a total of 13 contaminated impressions, with an equal number of 6 contaminated alginate and polyvinyl siloxane impressions, but this was not statistically significant (Table 2).
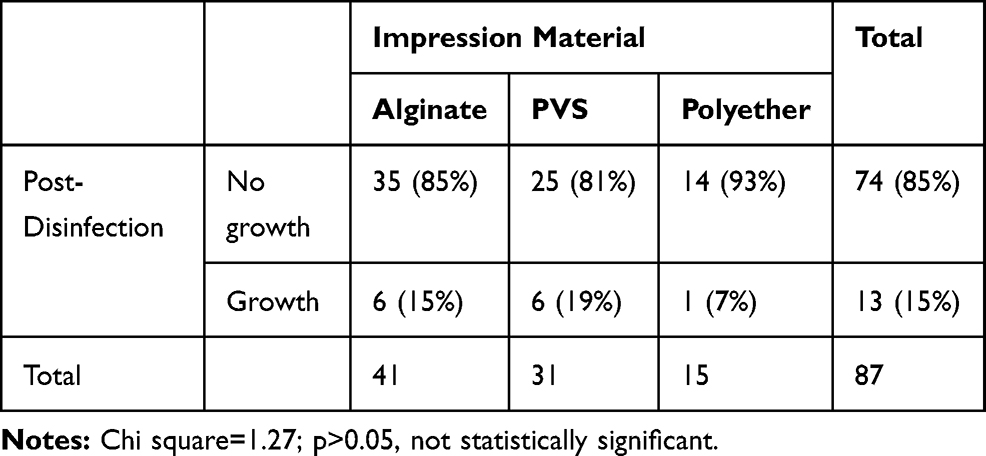 |
Table 2 The Number of Contaminated Impressions Post-Disinfection According to the Type of Impression Material |
Tables 3 and 4 show the bacterial growth pre- and post-disinfection according to disinfectant type. The difference in bacterial growth between the two disinfectants was not statistically significant. Both spray disinfectants reduced the number of contaminated impressions but an important finding is that 20% of impressions disinfected with the alcohol-based spray were still contaminated after disinfection.
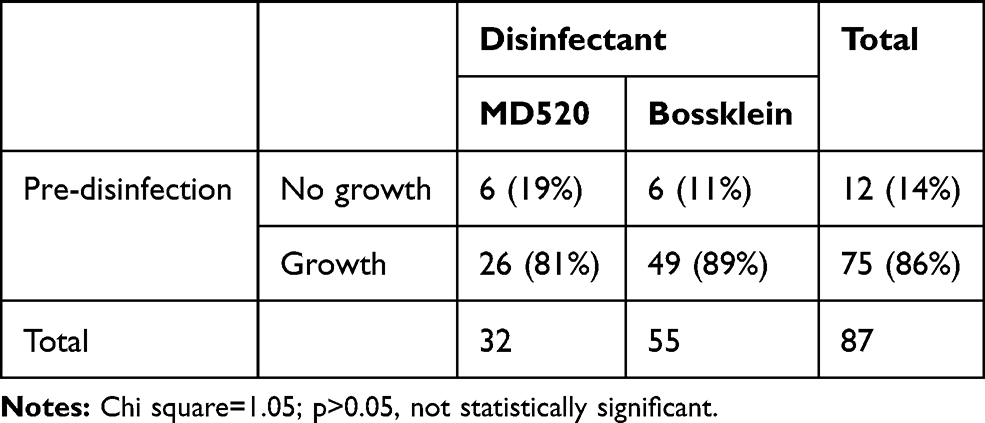 |
Table 3 Pre-Disinfection Growth According to Disinfectant |
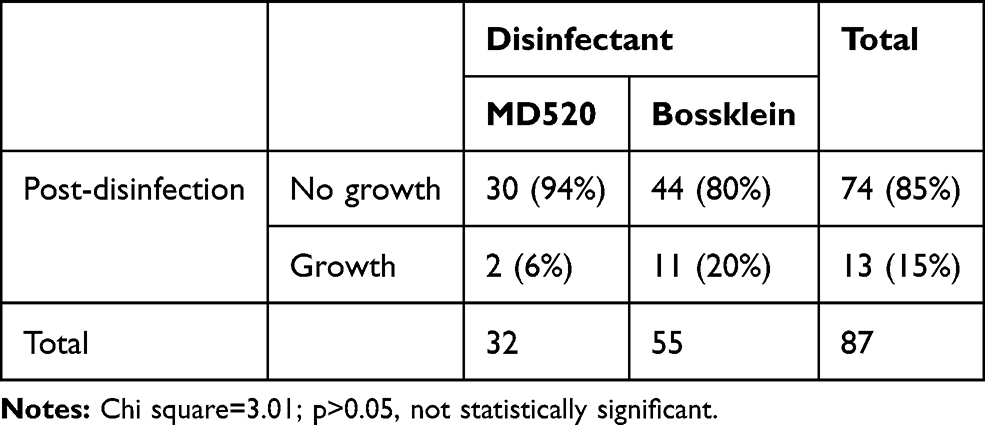 |
Table 4 Post-Disinfection Growth According to Disinfectant |
Table 5 shows the post-disinfection bacterial growth according to impression material and disinfectant solution. There was no growth after disinfection with the glutaraldehyde spray on both PVS and polyether impressions. Two alginate impressions were still contaminated after disinfection with aldehyde spray. Disinfection with the alcohol-based spray, however, resulted in 6 impressions having growth on PVS and 4 on alginate with only 1 polyether impression being contaminated. The occurrence of post-disinfection growth using the alcohol-based disinfectant on PVS was significantly greater than expected (x2= 5.37, p<0.05).
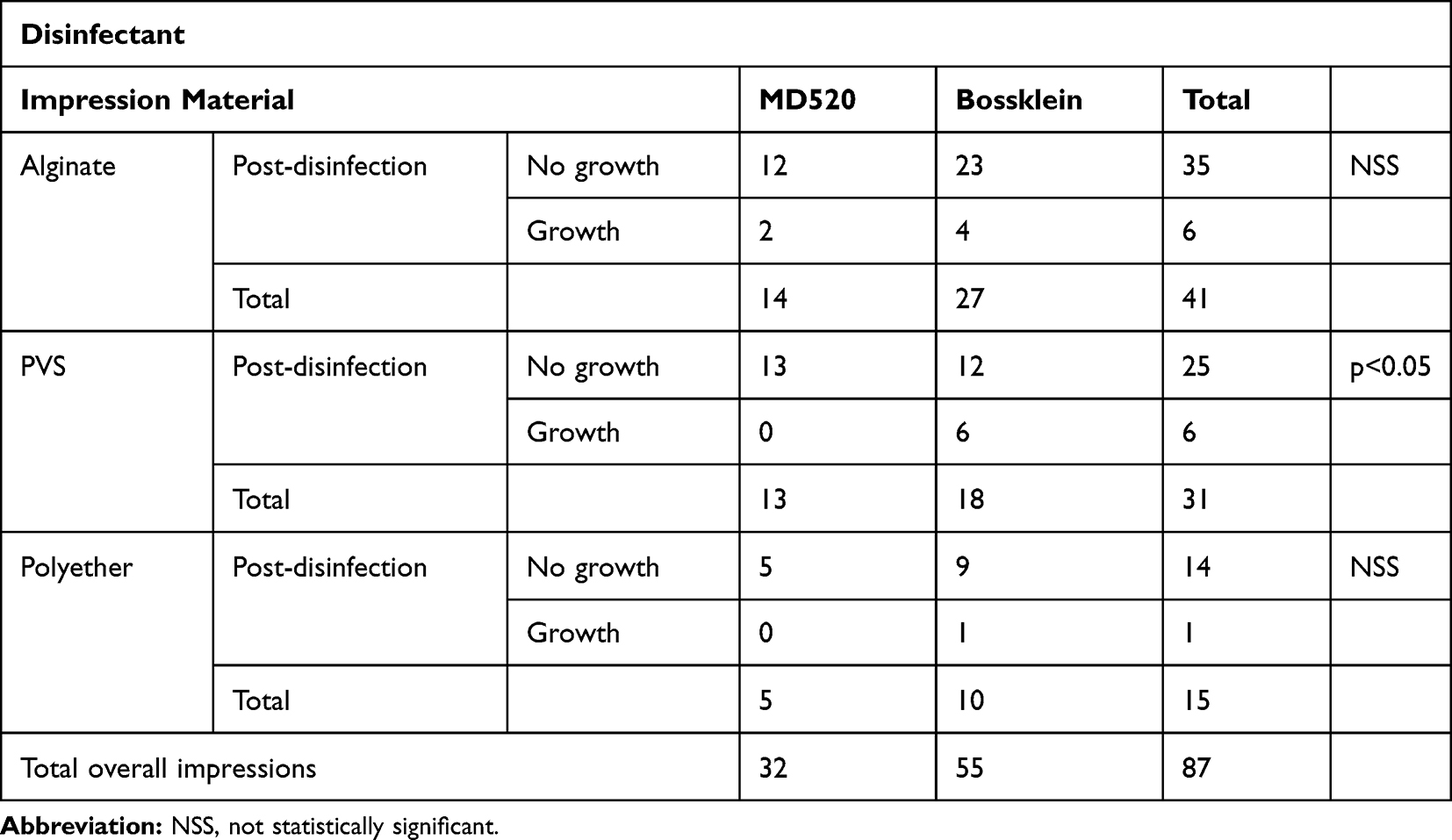 |
Table 5 Post-Disinfection Growth According to Impression Material and Disinfectant |
Discussion
It has been shown that just rinsing impressions under running tap water is insufficient to remove microbes but it may spread them over the surface of the impression material. Disinfection is therefore required.23 Spray disinfectants have been introduced which can provide good disinfection and avoid the problems associated with immersion techniques such as adverse effects on dimensional stability.19
MD 520 solution is based on a range of antimicrobially active constituents including glutaraldehyde, quaternary ammonium cations and special surfactants. Glutaraldehyde is toxic in high concentration but 100 g of MD 520 has a low concentration of 0.5 g glutaraldehyde and is safe. The other active antibacterial agent is 0.25 g alkyl benzyl dimethyl ammonium chloride. It effectively disinfected all but 2 alginate impressions in 10 mins. This finding is in agreement with Egusa et al who recommended it for clinical and laboratory use.20,23
Bossklein impression disinfectant spray is composed of ethanol and didecyldimethyl ammonium chloride. No studies were found in the literature evaluating its effectiveness in disinfecting dental impressions. Similar alcohol-based solutions such as Dimenol and Perform-ID were found to be comparable to solutions of chlorine or glutaraldehyde using either a spray or immersion technique.20 A spray disinfectant of 0.5% sodium hypochlorite was slightly more effective then 2% glutaraldehyde on alginate impressions.24 Demajo et al reported, however, that glutaraldehyde-based disinfectant (MD520) was more effective than an alcohol-based disinfectant (Minuten), particularly on alginate impression material, which corroborates the results presented here (Table 5).25 They mentioned that the action of alcohol also depends on surface friction; thus, mechanical friction needs to be applied during disinfection and therefore it was not recommended as an impression disinfectant.25 Similarly, isopropyl alcohol with povidone-iodine was found to be the least effective in decontaminating dental impressions.26
The results of the current investigation confirmed that polyether impression materials harbour fewer organisms before disinfection. Microbial growth varies according to impression material as alginate was previously reported to have 2–5 fold higher microbial counts compared to elastomeric impression materials because of its hydrophilic nature.27,28 Consequently, alginate powders and admix aqueous solutions containing 0.2% chlorhexidine digluconate have been developed which have shown superior antimicrobial activity against a range of micro-organisms in vitro compared to alginates without the agent.28 In the current study, a major finding was that 20% of impressions disinfected by the alcohol-based spray were still contaminated after disinfection compared to 6% with the glutaraldehyde-based spray, which although not statistically significant is a clinically significant result. Failure to adequately decontaminate impressions may be due to incorrect clinical procedure or inferior disinfecting properties. The Bossklein spray bottle had somewhat confusing information as the text in French stated that ‘Impressions are disinfected in 5 mins’ whilst the English text on the front of the spray bottle stated “Leave the impression to dry naturally”. A UK dental-hospital-based survey concluded all impressions should be immersed in 1% sodium hypochlorite for a minimum of 10 mins.29 Alcohol-based spray disinfection of dental impressions may not be as effective as aldehyde-based disinfectants and immersion methods are the gold standard. As a result of this study, staff training will ensure that thorough wetting/soaking of all impression surfaces is carried out.
Conclusion
Within the limitations of this study both aldehyde and alcohol spray disinfectants were able to disinfect the three types of impression material but the alcohol-based disinfectant was less effective with post-disinfection contamination on all three impression materials. Effective spray disinfection relies on correct operator technique such as thoroughness of wetting/soaking. A low number of spray bottle trigger activations may be related to cost saving, which is not an issue with immersion disinfectants.
Ethics Approval
This study was exempt from ethics approval as no patient intervention or randomisation was undertaken, normal clinical practice was employed and no patient identifiers were included as pooled data were analysed. All patients consented to treatment which included impression taking.
Data Sharing Statement
The data set is available on request and with the agreement of MBRU.
Author Contributions
All authors made substantial contributions to conception and design, data acquisition, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The post graduate student was given an internal MBRU grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Salvia ACRD, Dos Santos M, Rosa FCS, et al. Disinfection protocols to prevent cross-contamination between dental offices and prosthetic laboratories. J Infect Public Health. 2013;6:377–382. doi:10.1016/j.jiph.2013.04.011
2. Sofou A, Larsen T, Fiehn NE, Owall B. Contamination level of alginate impressions arriving at a dental laboratory. Clin Oral Invest. 2002;6:161–165. doi:10.1007/s00784-002-0173-4
3. Miller C, Palenik C. Infection Control and Management of Hazardous Materials for the Dental Team.
4. Mushtaq MA, Khan MWU. An overview of dental impression disinfection techniques – a literature review. J Pak Dent Assoc. 2018;27:207–212. doi:10.25301/JPDA.274.207
5. Spaulding E. The role of chemical disinfection in the prevention of nosocomial infections.
6. British Dental Association. Health Technical Memorandum 01-05: Decontamination in Primary Care Dental Practices. London: Department of Health; 2013.
7. Merchant VA. Infection control and prosthodontics. J Calif Dent Assoc. 1989;17:49–53.
8. ADA. Infection control recommendations for the dental office and the dental laboratory. ADA council on scientific affairs and ADA council on dental practice. J Am Dent Assoc. 1996;127:671–680.
9. Almortadi N, Chadwick RG. Disinfection of dental impressions – compliance to accepted standards. Br Dent J. 2010;209:607–611. doi:10.1038/sj.bdj.2010.1134
10. Lepe X, Johnson GH, Berg JC. Surface characteristics of polyether and addition silicone impression materials after long-term disinfection. J Prosthet Dent. 1995;74(2):181–186. doi:10.1016/S0022-3913(05)80184-2
11. Lepe X, Johnson G. Accuracy of polyether and addition silicone after long-term immersion disinfection. J Prosthet Dent. 1997;78:245–249. doi:10.1016/S0022-3913(97)70021-0
12. Johnson G, Chellis K, Gordon GE, Lepe X. Dimensional stability and detail reproduction of irreversible hydrocolloid and elastomeric impressions disinfected by immersion. J Prosthet Dent. 1998;79:446–453. doi:10.1016/S0022-3913(98)70160-X
13. Look J, Clay D, Gong K. Preliminary results from disinfection of irreversible hydrocolloid impressions. J Prosthet Dent. 1990;63:701–707. doi:10.1016/0022-3913(90)90329-B
14. Van Noort R. Impression materials. In: Introduction to Dental Materials.
15. Drennon D, Johnson G, Powell G. The accuracy and efficacy of disinfection by spray atomization on elastomeric impressions. J Prosthet Dent. 1989;62:468–475. doi:10.1016/0022-3913(89)90183-2
16. Centers for Disease Control and Prevention. Recommendations from the Guidelines for Infection Control in Dental Health-Care Settings. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2003.
17. Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services;2016.
18. Al Mortadi N, Al-Khatib A, Alzoubi KH, Khabour OF. Disinfection of dental impressions: knowledge and practice among dental technicians. Clin Cosmet Investig Dent. 2019;11:103–109. doi:10.2147/CCIDE.S205144
19. Doddamani S, Gangadhar S, Patil R. Efficacy of various spray disinfectants on irreversible hydrocolloid impression materials: an in vitro study. Indian J Dent Res. 2011;22:764–769. doi:10.4103/0970-9290.94662
20. Al-Jabrah O, Al-Shumailan Y, Al-Rashdan M. Antimicrobial effect of 4 disinfectants on alginate, polyether, and polyvinyl siloxane impression materials. Int J Prosthodont. 2007;20:299–307.
21. Healthcare Quality Improvement Partnership. A guide for clinical audit, research and service review – an educational toolkit designed to help staff differentiate between clinical audit, research and service review activities. Sheffield Teaching Hospitals NHS Foundation Trust; 2011. Available from http://hquip.org.uk.
22. Sutton S. Accuracy of plate counts. J Validation Technology. 2011;17:42–46.
23. Egusa H, Watamoto T, Matsumoto T, et al. Clinical evaluation of the efficacy of removing microorganisms to disinfect patient-derived dental impressions. Int J Prosthodont. 2008;21:531–538.
24. Aeran H, Jurel SK, Dhobhal A. Antimicrobial efficacy of spray disinfectants on dental impressions. Indian J Dent Sci. 2010; 2(6):10–14.
25. Demajo J, Cassar V, Farrugia C. Effectiveness of disinfectants on antimicrobial and physical properties of dental impression materials. Int J Prosthodont. 2016;29:63–67. doi:10.11607/ijp.4358
26. Sukhija U, Rathee M, Kukreja N, Khindria S, Singh V, Palaskar J. Efficacy of various disinfectants on dental impression materials. Internet J Dent Sci. 2010;9:1–6.
27. Samaranayake LP, Hunjan M, Jennings KJ. Carriage of oral flora on irreversible hydrocolloid and elastomeric impression materials. J Prosthet Dent. 1991;65:244–249. doi:10.1016/0022-3913(91)90169-W
28. Casemiro LA, Pires-de-Souza FCP, Panzeri H, Martins CHG, Ito IY. In vitro antimicrobial activity of irreversible hydrocolloid impressions against 12 oral microorganisms. Braz Oral Res. 2007;21:323–329. doi:10.1590/S1806-83242007000400008
29. Blair FM, Wassell RW. A survey of the methods of disinfection of dental impressions used in dental hospitals in the United Kingdom. Br Dent J. 1996;180:369–375. doi:10.1038/sj.bdj.4809092
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.