")
Back to Journals » Journal of Pain Research » Volume 15
Effectiveness and Safety of Acupuncture-Related Therapies for Chronic Musculoskeletal Pain: A Protocol for Systematic Review and Network Meta-Analysis
Authors Zhou Z , Xu G , Huang L, Shu Y, Tian H , Huang F , Liu Y , Liang F , Sun M
Received 27 August 2022
Accepted for publication 9 December 2022
Published 16 December 2022 Volume 2022:15 Pages 3959—3969
DOI https://doi.org/10.2147/JPR.S387756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Zhuo Zhou,1 Guixing Xu,1 Liuyang Huang,1 Yunjie Shu,1 Hao Tian,1 Fengyuan Huang,1 Yilin Liu,1 Fanrong Liang,2 Mingsheng Sun1
1Acupuncture and Tuina School/The 3rd Teaching Hospital, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Acupuncture and Tuina School/The 3rd Teaching Hospital, Chengdu University of Traditional Chinese Medicine/Clinical Research Center for Acupuncture and Moxibustion in Sichuan Province, Chengdu, People’s Republic of China
Correspondence: Fanrong Liang, Acupuncture and Tuina School/The 3rd Teaching Hospital, Chengdu University of Traditional Chinese Medicine/Clinical Research Center for Acupuncture and Moxibustion in Sichuan Province, Chengdu, People’s Republic of China, Tel +86 136 0805 8216, Fax +86-28-87683962, Email [email protected]
Introduction: Chronic pain is one of the major health problems worldwide in recent years, and acupuncture-related therapies have been reported to have definite analgesic effects. However, it is still unclear which treatment is the most effective. Our systematic review and network meta-analysis protocol aims to summarize the evidence and determine the most effective method to treat the chronic musculoskeletal pain.
Methods and Analysis: Our literature search will be performed in five electronic databases—the Cochrane Library, EMBASE, and PubMed, AMED, CINAHL, until May 20, 2022. All randomized controlled trials of acupuncture-related therapies for chronic musculoskeletal pain will be included. The primary outcomes will be common pain-related scales, and the secondary outcomes will include quality of life and incidence of adverse events. Excel 2019 will be used for data extraction, RoB2 will be used for bias risk assessment. R 3.6.2 and WinBUGS V.1.4.3 software will be used for network data synthesis and to produce related plots. During the study, literature selection, data extraction, quality assessment and bias risk assessment will be independently completed by two reviewers, and differences will be judged by the third reviewer. Finally, the risk of bias and sources of heterogeneity in the study will be analyzed and explained in order to obtain reliable results.
Results: Our study will evaluate the effectiveness and safety of acupuncture-related therapies for the treatment of chronic musculoskeletal pain, and we will rank all methods to recommend the best appropriate treatment option.
Conclusion: This study will provide a good foundation for complementary and alternative medicine to treat chronic musculoskeletal pain. It will be also helpful to promote the clinical practice by providing evidence-based medical evidence.
Keywords: systematic review, network meta-analysis, acupuncture-related therapies, chronic musculoskeletal pain
Introduction
Chronic pain is pain that persists or recurs in one or more anatomical areas for more than 3 months.1 The global rate of chronic pain patients is up to 30%.2 Approximately 25.3 million adults have chronic pain on a daily life in the United States,3 and the proportion of chronic pain patients is also over 30% in China.4 Although chronic pain-related diseases not immediately endanger lives of patients, the long-term impact on them makes it become the most important cause of mental health problems and disability.5,6 Among them, chronic musculoskeletal pain (CMP) is the leading cause of disability worldwide,7 with the consultation rate ranking second in chronic pain.8 The total annual cost to pain management, including patients, caregivers and healthcare systems, is estimated to be as high as 3.0% of GDP, and even higher than heart disease and cancer.9 More importantly, the social burden of chronic pain will increase significantly due to the aging of the population in the future.10
Although there are many causes of chronic musculoskeletal pain, the pathogeneses are generally related to inflammatory response, fibrotic scar formation, massive release of neurotransmitters, neuroimmune abnormalities, peripheral and central sensitization.11 The main purpose of treatment is to improve pain symptoms and the quality of life of patients. At present, the treatments of CMP are mainly divided into drugs, interventional therapies and other physical therapies.12 Drugs commonly used in clinical practice, such as opioids and non-steroidal anti-inflammatory drugs (NSAIDS), can temporarily relieve pain, but long-term use will produce side-effects such as gastrointestinal symptoms, liver and kidney toxicity, and even lead to addiction and drug abuse.13,14 Surgical treatments such as nerve blocks can also have serious sequelae.15 With the in-depth research, physical therapy represented by acupuncture has been widely used in recent years.
Acupuncture, as a safe and effective treatment with a long history, is widely popular in improving chronic pain.16–18 Several previous systematic reviews and meta-analysis have demonstrated that acupuncture and acupuncture-related therapies have beneficial effects on CMP related diseases such as back pain, shoulder pain and neck pain.19–21 The researchers conducted a network meta-analysis (NMA) and found that acupuncture was more effective than other physical therapies on relieving pain.22,23 Liu et al found that fire needle, warm acupuncture and electroacupuncture (EA) were more effective in improving the Western Ontario and McMaster Universities osteoarthritis index (WOMAC),24 while Wang et al believed that acupuncture plus moxibustion is the most effective way to reduce low back pain.25 SW Li et al previously proved that warm acupuncture and EA were effective treatment methods for knee osteoarthritis,26 and Wei et al thought that acupuncture plus acupoint application had the best effect in improving the Visual Analogue Scale (VAS) and alleviating pain.27 However, most of the current studies are limit to traditional meta-analysis, and there is still a lack of efficacy comparison between different treatments. At the same time, previous studies only focus on single disease type, such as neck pain, back pain, low back pain or knee osteoarthritis. There are shortcomings such as small number of studies, insufficient sample size and low statistical efficiency in the process of research, which lead to uncertainty in the results of studies and fail to provide a good guidance for clinical practice and scientific research.
Based on the above background, it is urgent to conduct a study on different acupuncture-related therapies of chronic musculoskeletal pain that have a common pain mechanism.28 In this study, we will focus on high quality research (Jadad ≥4) in the field of CMP. Then, we will use the method of Bayesian network analysis to systematically compare and rank different therapies. It will be a good way to improve statistical efficiency and increase the credibility of the findings, thus providing the latest evidence for clinicians and patients with chronic musculoskeletal pain.
Methods
Study Registration
This network meta-analysis will be conducted according to the guidelines stated in the Preferred Reporting Program for Systematic Evaluation and Meta-Analysis (PRISMA 2020) statement.29,30 It is registered on the PROSPERO website (https://www.crd.york.ac.uk/prospero/) for PROSPERO registration number CRD42022330971.
Data Sources and Search Strategy
An electronic search will be performed on acupuncture-related therapies for chronic pain from the establishment of the database to May 20, 2022 in the following online databases: The Cochrane Library, The Excerpta Medica Database (EMBASE), and PubMed, The Allied and Complementary Medicine Database (AMED), Cumulative Index to Nursing and Allied Health Literature (CINAHL). We only included the English literature in the above database. Specific retrieval strategy is shown in Table 1.
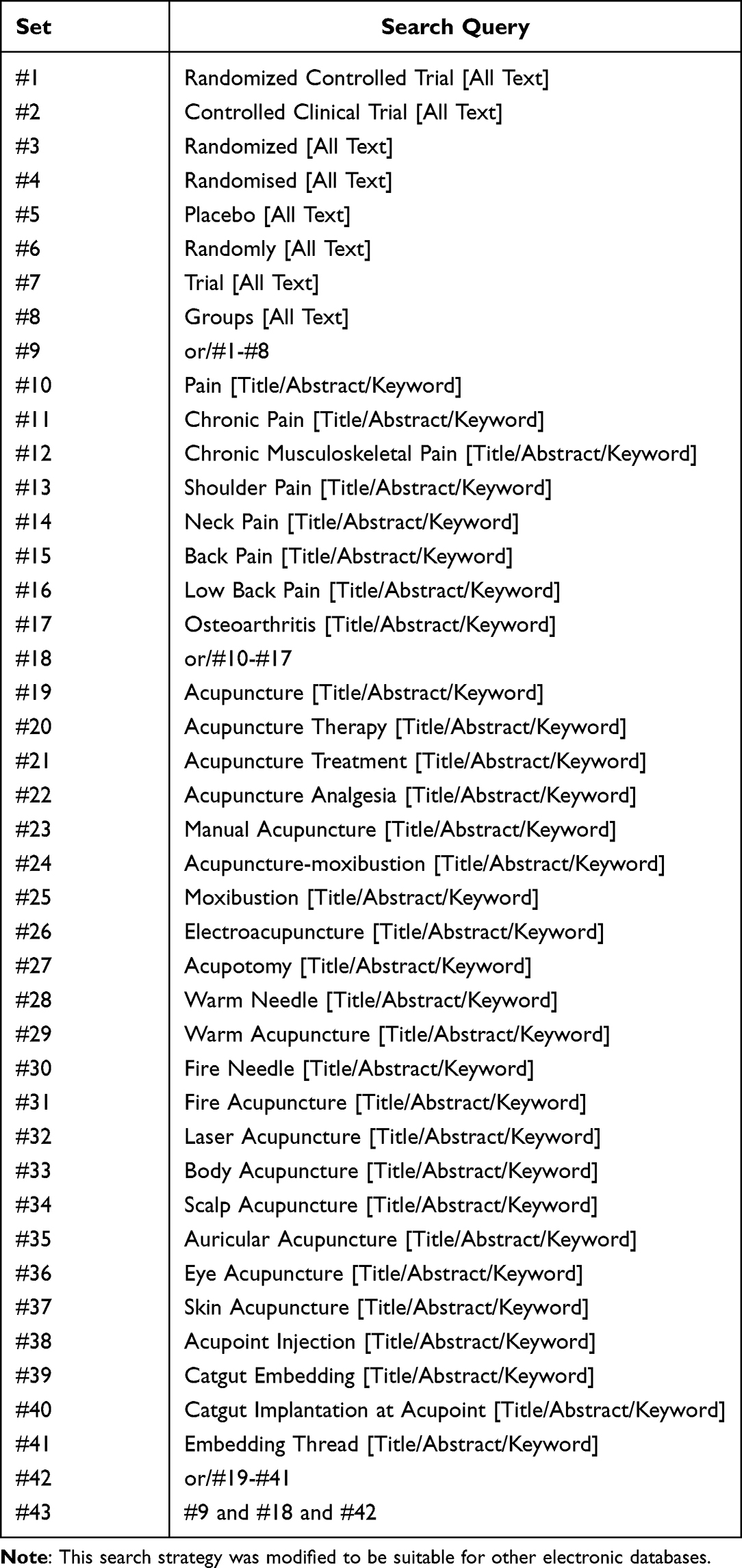 |
Table 1 Search Strategy for Cochrane Library Database |
Inclusion and Exclusion Criteria
Types of Studies
Only randomized control trials (RCTs) of acupuncture-related therapies for chronic primary musculoskeletal pain will be included.
Participants
All patients with chronic musculoskeletal pain will be included, including a definitive diagnosis of nonspecific neck pain, shoulder pain, low back pain, back pain, limb pain, chest pain and osteoarthritis. The diagnosis of the above diseases can be carried out according to the relevant guidelines of Chinese medicine or Western medicine. Patients are 18 years of age or older, regardless of gender, race or nationality, and there are no restrictions on the severity.
We will rule out diseases according to the International Classification of Diseases (ICD-11):1(1) chronic widespread pain; (2) complex regional pain syndromes; (3) chronic primary and secondary headache or orofacial pain; (4) chronic primary and secondary visceral pain; (5) chronic cancer-related pain; (6) chronic postsurgical or post-traumatic pain; (7) chronic neuropathic pain; (8) chronic secondary musculoskeletal pain.
Types of Interventions
We will include control groups if they were treated with manual acupuncture, moxibustion, electroacupuncture, acupotomy, warm acupuncture, fire acupuncture, laser acupuncture, body acupuncture, scalp acupuncture, auricular acupuncture, eye acupuncture, skin acupuncture, acupoint injection, catgut embedding. Acupressure, cupping therapy will be excluded. The intervention in this group could be a single intervention or combined with traditional drugs (including opioid painkillers or NSAIDS).
Types of Comparison
The control group will be treated with any inactive interventions (sham acupuncture, waiting list, placebo and no intervention), opioid painkillers, NSAIDS.
Outcomes
For the outcome measures, effect sizes will be extracted at the first time point after the end of the interventions and at the follow-up time point. The primary outcomes will be common continuous variables pain-related scales, including the following: (1) WOMAC;31 (2) VAS or Facial-VAS,32 (3) The Numeric Pain Rating Scale (NPRS) or the Numeric Rating Scale (NRS),33 (4) The Brief Pain Inventory (BPI).33 Finally, we will use the VAS with a total score of 10 to convert the different scales into uniform units according to the International unit system to obtain robust results.
The secondary outcomes will be included: Quality of Life Survey Summary Form (QoL) SF-12 or SF −36,34 Side effects or adverse events (AE). Again, we were going to use the same units for conversion.
Selection of Studies
Two researchers (ZZ and XGX) will independently select studies based on inclusion and exclusion criteria using bibliographic software EndNote X9 (https://www.endnote.com/). First, duplicate studies will be deleted. Then, title and abstract will be read to exclude studies that do not meet the criteria. Carefully read the full text of all remaining articles to determine the final inclusion of the article. If there is incomplete basic information or data to contact the author for access. Any disagreement arising during the assessment will be adjudicated by a third investigator (LFR) to achieve consensus. Finally, we will provide a list of excluded studies and an argument for exclusions. The selection procedure is shown in the PRISMA flowchart as presented in Figure 1.
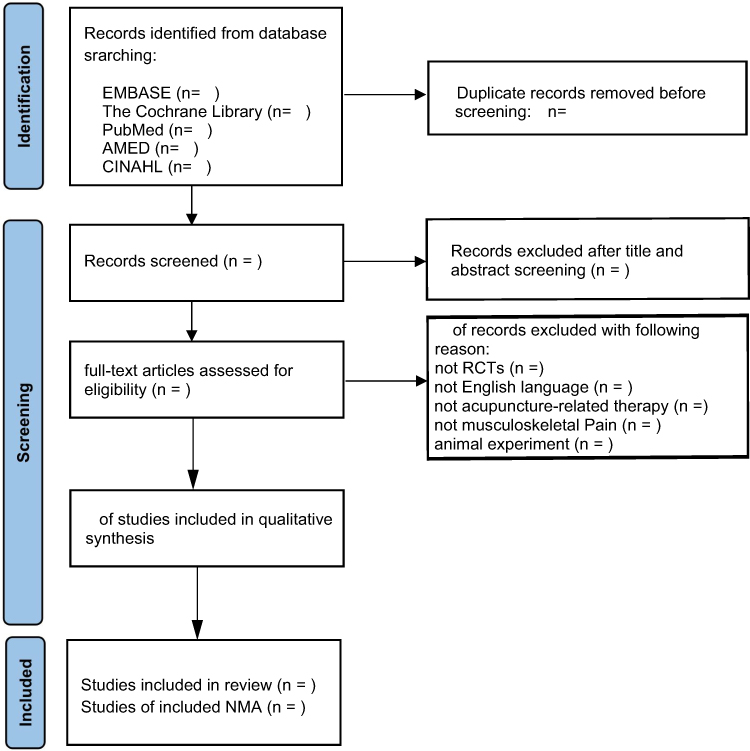 |
Figure 1 Flowchart of study selection. |
Data Extraction and Management
Two researchers (HLY and SYJ) will use Excel 2019 software independently extracted data from five major aspects: basic study information (Title, author information, publication), the participants information (Gender, age, sample size, the types of chronic pain, pain grading), intervention in detail (Intervention method, follow-up duration, frequency, time), methods, information (Study design, random sequence generation, allocation hiding, blinding, and other issues related to bias) and related outcome indicators (primary outcome, secondary outcome, adverse events) as presented in Table 2. A third researcher (LFR) will check and verify the entered data to ensure consistency and validity.
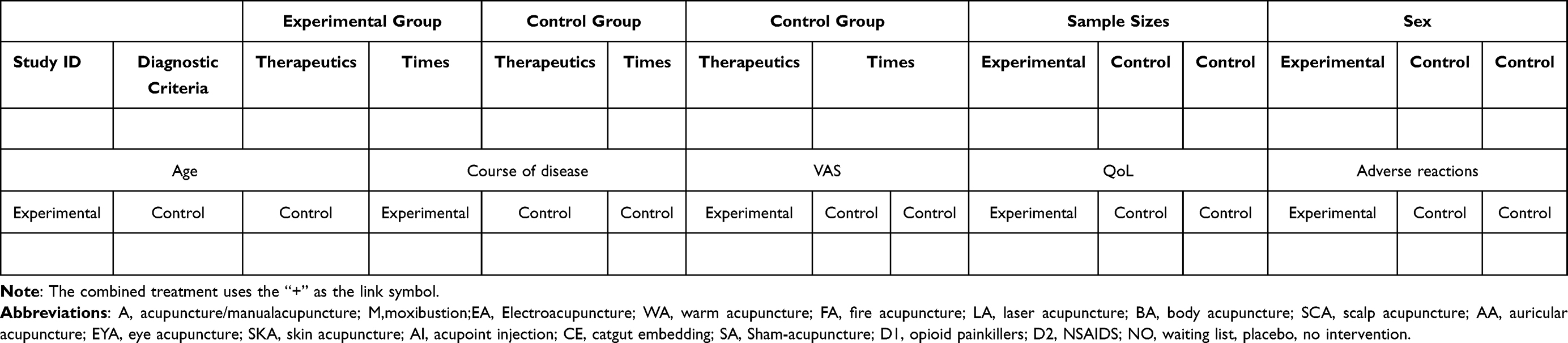 |
Table 2 The Main Characteristics of Each Identified Study |
Risk of Bias Assessment
Two reviewers (TH and HFY) will use the Version 2 of the Cochrane tool for assessing risk of bias (RoB2) in randomised trials to assess the quality of the included studies.35–37 The evaluation will be included the following aspects: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in measurement of the outcome; (5) bias in selection of the reported result. The risk of bias in each area falls into three grades: “low risk of bias”, “some concerns” and “high risk of bias”. We will evaluate the magnitude and direction of bias from the following six aspects: (1) favours experimental; (2) favours comparator; (3) towards null; (4) away from null; (5) unpredictable; (6) not apply.36 Finally, RoB2 software provided by the website of risk of bias (https://www.riskofbias. Info/) will be used to complete the drawing of the risk of bias map.
Dealing with Missing Data
In the process of data collection and entry, once the original data is found missing or in doubt, we will obtain the missing information from the author through the contact information in the article. If there is no response, we will impute the missing data with the replacement value. To ensure the reliability of the findings, sensitivity analyses will be conducted to assess the potential impact of missing data on the review results, which will be explained in the discussion section of the NMA results.
Statistical Analysis
Standard Pairwise Meta-Analysis
After a rigorous screening process, we will conduct a comprehensive and systematic summary of the characteristics of RCTs that met the inclusion criteria. The Odds Ratio (OR) value with 95% CI will be used to analyze the dichotomous data and the mean difference (MD) with 95% CI will be used to analyze the continuous data. The Mantel-Haenszel χ2 test and Higgins I2 test will be used to assess heterogeneity and check whether the included articles could be combined. If I2≤ 50%, the fixed-effects model (FEM) will be used. Otherwise, the random-effects model (REM) will be used.
NMA and Network Geometry
In this study, R 3.6.2 software and WinBUGS V.1.4.3 software will be used to draw the network plot in order to quickly understand the comparative relationship between different interventions. The nodes in the figure represent different interventions, and the area of the nodes represent the number of intervention studies evaluated. The lines between the nodes indicate that there is a direct correlation between the two interventions, and no connection means no direct comparison. The larger the node is, the more times there are in the corresponding direct comparison; the thicker the line is, the more direct comparisons there are. All of the interventions included in the plot are described in detail. At the same time, the possible bias will be explained to describe the influence of bias on the treatments involved.
The Markov chain Monte Carlo method (MCMC) will be used to establish Bayesian network analysis. The initial set will be 4 chains for simulation analysis, and the number of iterations is 50,000. The 20,000 will be used for annealing to eliminate the influence of the initial value, and the last 30,000 will be used for sampling calculation, so as to draw the iteration history plot to judge whether the convergence degree of the model is satisfactory. The iterative convergence will be evaluated by Brooks-Gelman-Rubin diagnosis method. When the Potential Scale Reduction Factor (PSRF) is closer to 1, the convergence degree is better, and the reliability of consistency model analysis results is higher. Otherwise, the reliability is low. It indicates that the current number of simulations is insufficient to achieve good convergence, and the number of simulations needs to be increased.
Finally, the ranking probabilities and rankogram will be drawn to evaluate the efficacy differences between acupuncture-related therapies in treating chronic musculoskeletal pain, so as to quickly predict the optimal or worst interventions. At the same time, we will make the cumulative ranking plot and calculate the Surface Under the Cumulative Ranking (SUCRA) of all intervention measures according to the cumulative data. To rank the various interventions for all outcomes, the higher the SUCRA score, the better the analgesic effect. SUCRA equals 1 indicates that the intervention is considered to be the best, while 0 indicates that it is the worst.
Assessment of Inconsistency
We will use node-splitting method to explore the inconsistency.38 The ultimate goal of NMA is to produce consistent results which means that the results of indirect and direct comparisons are similar. Each node of the NMA will be analyzed to compare the statistical differences between direct and indirect evidence.39 If there is no difference, the results will be consistent (P > 0.05), and a consistency model could be used. If there is difference, there is inconsistency, then we need to use the inconsistency model for fitting.40 When there is inconsistency, we will analyze them based on the actual situation. Firstly, it can be determined by the contribution degree of direct comparison and indirect comparison. If the contribution degree of indirect comparison is larger, the result will be more reliable, and vice versa. Of course, we can also see whether direct comparison is highly High heterogeneity. When the heterogeneity of direct comparison is too large, the conclusion of indirect comparison is more reliable. However, if substantial inconsistencies do exist, we may consider only using more reliable direct comparison results to make decisions, rather than using network meta-analysis results during the research process. If there are any differences in the process, we will ask a third investigator (LFR) to evaluate.
Subgroup and Sensitivity Analyses
In pairwise meta-analysis, if there is considerable heterogeneity in the trial, we will conduct a subgroup analysis to explore possible sources of heterogeneity.41 Subgroup analysis was performed based on the following aspects: (1) age; (2) sex; (3) disease type; (4) location of disease area; (5) pain degree (defined by VAS, (0 ~ 3: mild pain; 4–6: moderate pain; 7–10: severe pain).
The sensitivity analysis will be performed to explore the stability of network meta-analysis. Sample size and pain level are likely to be the main reasons for the consistency and will be analyzed concretely. The study with sample size of less than 30 or risk of bias assessment is very low will be excluded. Meanwhile, the degree of pain will also be considered as a factor in the sensitivity analysis and will be excluded according to the pain score. For example, studies with VAS>4 or VAS ≤4 will be excluded.
Grading the Quality of Evidence
The quality of the evidence will be evaluated by two reviewers (LYL and SMS) through the GRADE system (http://www.gradeworkinggroup.org/).42 The following five aspects will be considered: (1) The methodological quality of the included studies (risk of bias);43 (2) The extrapolation of the study population, interventions and outcome indicators (indirectness);44 (3) The degree of agreement between the results of different studies (inconsistency);45 (4) The accuracy of the combined results of different studies (imprecision);46 (5) The extent to which research is included to meet the criteria (publication bias).47 Due to the particularity of NMA, we will strictly follow the GRADE guidelines to evaluate its evidence quality with four steps:48–50 (1) the direct and indirect treatment estimates for each comparison of the evidence network will be presented; (2) the quality of each direct and indirect effect estimate will be rated respectively. (3) the NMA estimate for each comparison of the evidence network will be presented. (4) the quality of each NMA effect estimate will be rated. Eventually, the quality of research evidence will be classified as “high”, “medium”, “low” or “very low”.51
Ethics and Dissemination
The data used in this study are all public data of clinical studies that have passed ethical review and do not involve patients’ personal data, so there is no need for ethical review and privacy issues.
Discussion
Chronic musculoskeletal pain (especially low back and neck pain) has been the leading causes of disability internationally when measuring years lived with disability,52 and other chronic pain conditions also occupy the important position in the top 10 causes of disability.53 It as a persistent pathological symptom, not only seriously affects the daily work and quality of life,54 but also induces psychological problems including anxiety and depression in the long run.2,55 More importantly, it makes patients lose confidence in treatment. We found that different acupuncture interventions can improve this pathological state through different analgesic mechanisms.17 Studies have shown that acupuncture can inhibit the spinal cord dorsal horn of microglia and astrocytes activity to relieve chronic pain, and electroacupuncture (EA) blocks pain by activating a variety of bioactive chemicals through peripheral, spinal, and supraspinal mechanisms.56 Liu et al found that moxibustion could increase pain threshold by increasing the concentrations of dynorphin (Dyn) and endomorphin (EM) in spinal cord of rats.57
Network meta-analysis allows the comparison of multiple interventions from different studies.58 To the best of our knowledge, this study is the first systematic review and NMA of different acupuncture-related therapies to improve CMP symptoms using Bayesian network meta-analysis method. To retrospect previously published systematic reviews and meta-analysis of acupuncture related to the improvement of CMP, most of them focused only on one of the categories of neck pain, back pain, or limb pain. The meta-analysis involving CMP is only a traditional direct comparison.59–64 These studies have included acupuncture, laser acupuncture, and dry needles as interventions, but they have not reached a consistent conclusion, so it is impossible to know which treatment is more effective. Our research will systematically synthesize the evidence on the efficacy and safety of acupuncture-related therapy for CMP. To a large extent, our study will help clinical evidence-based treatment decisions and fill the evidence gap in the management of this disease that afflicts patients.
Our study will be conducted strictly accordance with the PRISMA 2020 guidelines. We will conduct a comprehensive search of the common disease types in chronic musculoskeletal pain. So, there will be a lot of clinical studies involved, and the sample size will be significantly larger than previous studies. We will further evaluate the literature, only studies with Jadad ≥ 4 will be included in the end. Of course, doing so will also help us to reach the most reliable and instructive research conclusions. Our study will make a detailed summary and analysis of the factors that affect the quality, such as heterogeneity and inconsistency of the included literature in the process of the study. And ranking the effectiveness of interventions to make the best choice. We will also summarize and evaluate the adverse effects in the study to verify the safety of acupuncture-related therapies. In conclusion, our results can not only provide patients with cost-effective treatment options, but also provide clinicians with treatment ideas.
Our study may have the following limitations: First of all, CMP is a very broad concept, and we only include some common bone and muscle pain diseases, but do not completely include all diseases of this type. There may be some limitations, but at the same time, by selecting these representative diseases, we can improve our statistical effectiveness. Second, only 5 English databases were retrieved in this study, which may lead to bias in the selection of studies, thus ignoring the potential risks of some studies. Third, we only included studies with Jadad ≥ 4, which may also lead to selection bias. But undoubtedly, it can also ensure the high quality of our research and increase the credibility of the results. Finally, the conversion of continuous scores into the same dimension VAS scores in our data analysis may lead to statistical inaccuracies, but it is inevitable in the statistical process.
Ethics and Dissemination
The data used in this study are all public data from clinical studies that have passed ethical review and do not involve patients’ personal data, so there is no need for ethical review and privacy issues.
Author Contributions
ZZ conceived the programme and drafted the manuscript. GXX registered the project at PROSPERO and developed the search strategies. Data were extracted by LYH and YJS. HT and FYH were responsible for assessing the risk of bias. YLL and MSS were responsible for assessing the quality of evidence. All differences in the study were adjudicated by the FRL. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Innovation Team and Talents Cultivation Program of National Administration of Traditional Chinese Medicine. (No: ZYYCXTD-D-202003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain. 2019;160(1):28–37. doi:10.1097/j.pain.0000000000001390
2. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
3. Chen L, Michalsen A. Management of chronic pain using complementary and integrative medicine. BMJ. 2017;357:j1284. doi:10.1136/bmj.j1284
4. Chen B, Li L, Donovan C, et al. Prevalence and characteristics of chronic body pain in China: a national study. Springerplus. 2016;5(1):938. doi:10.1186/s40064-016-2581-y
5. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
6. Hooten WM, Pain C. Mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. 2016;91(7):955–970. doi:10.1016/j.mayocp.2016.04.029
7. Briggs AM, Woolf AD, Dreinhofer K, et al. Reducing the global burden of musculoskeletal conditions. Bull World Health Organ. 2018;96(5):366–368. doi:10.2471/BLT.17.204891
8. Bond M. A decade of improvement in pain education and clinical practice in developing countries: IASP initiatives. Br J Pain. 2012;6(2):81–84. doi:10.1177/2049463712444062
9. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–147. doi:10.1016/j.mayocp.2014.09.010
10. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a national institutes of health pathways to prevention workshop. Ann Intern Med. 2015;162(4):276–286. doi:10.7326/M14-2559
11. Ying ZH, Yu JJ, Li HM, Ma RR, Wu TJ. Research overview and drug treatment progress of chronic musculoskeletal pain. Zhejiang Med. 2020;42(09):883–886.
12. Association CAW. Expert consensus on diagnosis and treatment of chronic musculoskeletal pain. Orthopaedics. 2021;12(05):389–395.
13. Da Costa BR, Pereira TV, Saadat P, et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and Hip osteoarthritis: network meta-analysis. BMJ. 2021;375:n2321. doi:10.1136/bmj.n2321
14. Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320(23):2448–2460. doi:10.1001/jama.2018.18472
15. Joshi G, Gandhi K, Shah N, Gadsden J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016;35:524–529. doi:10.1016/j.jclinane.2016.08.041
16. Zhuang Y, Xing JJ, Li J, Zeng BY, Liang FR. History of acupuncture research. Int Rev Neurobiol. 2013;111:1–23.
17. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
18. Liu HR, Qi L, Wu LY, et al. Effects of moxibustion on dynorphin and endomorphin in rats with chronic visceral hyperalgesia. World J Gastroenterol. 2010;16(32):4079–4083. doi:10.3748/wjg.v16.i32.4079
19. Yao Y, Zhou L, Chen FQ, et al. The effect and safety of thunder-fire moxibustion for low back pain: a meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:6114417. doi:10.1155/2022/6114417
20. Yuan T, Xiong J, Wang X, et al. The effectiveness and safety of moxibustion for treating knee osteoarthritis: a PRISMA compliant systematic review and meta-analysis of randomized controlled trials. Pain Res Manag. 2019;2019:2653792. doi:10.1155/2019/2653792
21. Hu HT, Gao H, Ma RJ, Zhao XF, Tian HF, Li L. Is dry needling effective for low back pain?: a systematic review and PRISMA-compliant meta-analysis. Medicine. 2018;97(26):e11225. doi:10.1097/MD.0000000000011225
22. Corbett MS, Rice SJ, Madurasinghe V, et al. Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta-analysis. Osteoarthritis Cartilage. 2013;21(9):1290–1298. doi:10.1016/j.joca.2013.05.007
23. Baroncini A, Maffulli N, Eschweiler J, Molsberger F, Klimuch A, Migliorini F. Acupuncture in chronic aspecific low back pain: a Bayesian network meta-analysis. J Orthop Surg Res. 2022;17(1):319. doi:10.1186/s13018-022-03212-3
24. Liu W, Fan Y, Wu Y, et al. Efficacy of acupuncture-related therapy in the treatment of knee osteoarthritis: a network meta-analysis of randomized controlled trials. J Pain Res. 2021;14:2209–2228. doi:10.2147/JPR.S315956
25. Wang L, Yin Z, Zhang Y, et al. Optimal acupuncture methods for nonspecific low back pain: a systematic review and bayesian network meta-analysis of randomized controlled trials. J Pain Res. 2021;14:1097–1112. doi:10.2147/JPR.S310385
26. Li S, Xie P, Liang Z, et al. Efficacy comparison of five different acupuncture methods on pain, stiffness, and function in osteoarthritis of the knee: a network meta-analysis. Evid Based Complement Alternat Med. 2018;2018:1638904. doi:10.1155/2018/1638904
27. Wei W, He Y, Liao X. Reticular meta-analysis of different acupuncture and moxibustion therapy for cervical spondylosis. World J Acupunct Moxibustion. 2022;38(05):35–41.
28. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Hauser W. Chronic primary musculoskeletal pain: a new concept of nonstructural regional pain. Pain Rep. 2022;7(5):e1024. doi:10.1097/PR9.0000000000001024
29. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
30. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160
31. Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (Tas). Arthritis Care Res. 2011;63(Suppl 11):S208–228.
32. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798–804. doi:10.1111/j.1365-2702.2005.01121.x
33. Wang L, Zhao Q, Chen J, et al. Expert consensus on the application of pain evaluation questionnaires in China (2020). Chin J Painol. 2020;16(03):177–187.
34. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Med. 2016;4:2050312116671725. doi:10.1177/2050312116671725
35. Jinchi L, Chang L, Chengge H. Risk bias assessment tool RoB2 (revised version 2019) for randomized controlled trial: an interpretation. Chin J Evid Based Med. 2021;21(06):737–744.
36. Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
37. Minozzi S, Cinquini M, Gianola S, Gonzalez-Lorenzo M, Banzi R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J Clin Epidemiol. 2020;126:37–44. doi:10.1016/j.jclinepi.2020.06.015
38. Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med. 2010;29(7–8):932–944. doi:10.1002/sim.3767
39. Veroniki AA, Vasiliadis HS, Higgins JP, Salanti G. Evaluation of inconsistency in networks of interventions. Int J Epidemiol. 2013;42(1):332–345. doi:10.1093/ije/dys222
40. Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making. 2013;33(5):641–656. doi:10.1177/0272989X12455847
41. Dias S, Sutton AJ, Welton NJ, Ades AE. Evidence synthesis for decision making 3: heterogeneity--subgroups, meta-regression, bias, and bias-adjustment. Med Decis Making. 2013;33(5):618–640. doi:10.1177/0272989X13485157
42. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
43. Guyatt GH, Oxman AD, Vist G, et al. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407–415. doi:10.1016/j.jclinepi.2010.07.017
44. Rasch A, Perleth M, Langer G, et al. GRADE guidelines: 8. Rating the quality of evidence - indirectness. Z Evid Fortbild Qual Gesundhwes. 2012;106(10):745–753. German. doi:10.1016/j.zefq.2012.10.019
45. Perleth M, Langer G, Meerpohl JJ, Gartlehner G, Kaminski-Hartenthaler A, Schunemann HJ. GRADE guidelines: 7. Rating the quality of evidence - inconsistency. Z Evid Fortbild Qual Gesundhwes. 2012;106(10):733–744. German. doi:10.1016/j.zefq.2012.10.018
46. Kulig M, Perleth M, Langer G, et al. GRADE guidelines: 6. Rating the quality of evidence: imprecision. Z Evid Fortbild Qual Gesundhwes. 2012;106(9):677–688. German. doi:10.1016/j.zefq.2012.10.016
47. Nolting A, Perleth M, Langer G, et al. GRADE guidelines: 5. Rating the quality of evidence: publication bias. Z Evid Fortbild Qual Gesundhwes. 2012;106(9):670–676. German. doi:10.1016/j.zefq.2012.10.015
48. Puhan MA, Schunemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi:10.1136/bmj.g5630
49. Wang Q, Wang JC, Pan B, et al. Advance in the GRADE approach to rate the quality of evidence from a network metaanalysis. Chin J Evid Based Med. 2020;20(08):979–985.
50. Nan Y, Shujun X, Qi Z, et al. An introduction of principles and methods of applying GRADE to network meta-analysis. Chin J Evid Based Med. 2016;16(05):598–603.
51. Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi:10.1016/j.jclinepi.2010.07.015
52. Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1211–1259.
53. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e283. doi:10.1016/j.bja.2019.03.023
54. Pereira MG, Carvalho C, Costa ECV, Leite A, Almeida V. Quality of life in chronic pain patients: illness- and wellness-focused coping as moderators. Psych J. 2021;10(2):283–294. doi:10.1002/pchj.410
55. Means-Christensen AJ, Roy-Byrne PP, Sherbourne CD, Craske MG, Stein MB. Relationships among pain, anxiety, and depression in primary care. Depress Anxiety. 2008;25(7):593–600. doi:10.1002/da.20342
56. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
57. Hongmei D, Ying L, Ling L. Correlation between self-efficacy and self-transcendence among patients with chronic pain. J Nurs Sci. 2020;35(21):32–35.
58. Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Intern Emerg Med. 2017;12(1):103–111. doi:10.1007/s11739-016-1583-7
59. Yuan QL, Wang P, Liu L, et al. Acupuncture for musculoskeletal pain: a meta-analysis and meta-regression of sham-controlled randomized clinical trials. Sci Rep. 2016;6:30675. doi:10.1038/srep30675
60. Lenoir D, De Pauw R, Van Oosterwijck S, Cagnie B, Meeus M. Acupuncture versus sham acupuncture: a meta-analysis on evidence for longer-term effects of acupuncture in musculoskeletal disorders. Clin J Pain. 2020;36(7):533–549. doi:10.1097/AJP.0000000000000812
61. Ha G, Tian Z, Chen J, et al. Coordinate-based (ALE) meta-analysis of acupuncture for musculoskeletal pain. Front Neurosci. 2022;16:906875. doi:10.3389/fnins.2022.906875
62. Law D, McDonough S, Bleakley C, Baxter GD, Tumilty S. Laser acupuncture for treating musculoskeletal pain: a systematic review with meta-analysis. J Acupunct Meridian Stud. 2015;8(1):2–16. doi:10.1016/j.jams.2014.06.015
63. Hung YC, Lin PY, Chiu HE, Huang PY, Hu WL. The Effectiveness of laser acupuncture for treatment of musculoskeletal pain: a meta-analysis of randomized controlled studies. J Pain Res. 2021;14:1707–1719. doi:10.2147/JPR.S308876
64. He C, Ma H. Effectiveness of trigger point dry needling for plantar heel pain: a meta-analysis of seven randomized controlled trials. J Pain Res. 2017;10:1933–1942. doi:10.2147/JPR.S141607
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.