")
Back to Journals » Infection and Drug Resistance » Volume 14
Effective Treatment of Small Uncomplicated Skin Abscesses with Fire Needle: A Case Series
Authors Zhang HH , Zhang CM , Xu QQ , Zhang CH
Received 30 June 2021
Accepted for publication 21 September 2021
Published 5 October 2021 Volume 2021:14 Pages 4085—4090
DOI https://doi.org/10.2147/IDR.S327089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Huan-Huan Zhang, Chun-Min Zhang, Qing-Qing Xu, Chun-Hong Zhang
Department of Dermato-Venereology, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China
Correspondence: Chun-Hong Zhang
Department of Dermato-Venereology, The Second Hospital, Cheeloo College of Medicine, Shandong University, 247 Beiyuan Dajie Street, Jinan, 25000, People’s Republic of China
Fax +86-531-88962544
Email [email protected]
Background: Uncomplicated skin abscesses are collections of pus within the skin structure and are usually caused by bacterial infections. Clinically, they are quite common and inevitably affect people of any age. The current management strategies comprise prompt initiation of antibiotics and incision and drainage. However, pain and the long healing process of skin lesions can cause distress to a lot of patients. Fire needling is a characteristic treatment in traditional Chinese medicine (TCM) and has proven effective in treating skin abscesses. Moreover, fire needle therapy has a more desirable cosmetic outcome in contrast to surgical debridement. The purpose of the study is to demonstrate the rapid, effective, minimally invasive, and better cosmetic outcomes of fire needles in the treatment of uncomplicated skin abscesses.
Methods: A total of 10 patients, aged between 1 and 45 years, with skin abscesses, were recruited. All patients who fulfilled the inclusion criteria with lesions less than 4 cm in diameter were topically treated with mupirocin ointment twice a day after fire needle therapy. If the lesion was still purulent after 2 days, it was treated again with fire needle therapy. The efficacy was assessed by a 4-grade scale at 2 days, 1 week, 2 weeks, 4 weeks and 12 weeks post-fire needling.
Results: Lesions with a diameter of less than 2 cm achieved significant remission (SR) or partial remission (PR), after 2 days post-treatment and reached complete remission (CR) or significant remission (SR) after 1 week following treatment. Meanwhile, lesions with a diameter of 2– 4 cm achieved PR after 2 days and were assessed as CR or SR 1 week after post-fire needle therapy. None of the patients had a recurrence within 12 weeks after treatment.
Conclusion: Fire needle therapy is a promising treatment method for uncomplicated skin abscesses smaller than 4 cm, which warrants further in-depth and more large-scale studies.
Keywords: fire needle, uncomplicated skin abscess, traditional Chinese medicine
Introduction
Skin infections are relatively common conditions in inpatient and outpatient settings.1 Furuncles and carbuncles form part of skin abscesses and are particularly frequent clinically. Many of these conditions share similar management strategies, including prompt initiation of antibiotics and incision and drainage when indicated. Wound care and follow-up care are critical parts of managing skin infections to ensure appropriate resolution and prevent further disease progression.2 However, incision and drainage inevitably lead to a larger wound, which is then allowed to heal by a secondary intention and hence involves a longer duration of wound healing.3
Fire needle therapy uses a stainless-steel needle with a diameter of 0.30 mm. The wound is much smaller, and the pain is more bearable compared to current surgical treatment. Besides, local pus and blood discharge are also promoted through the small opening. In addition, these small wounds can promote the permeability of local drugs and improve the efficacy, avoiding the large surgical incisions,4–6 which may require secondary wound healing.
This paper reports on a series of 10 cases of uncomplicated skin abscess treated with fire needle therapy, which brought about a quick clearance of redness and swelling as well as excellent cosmetic outcomes. The study was approved by the Ethics Committee of the Second Hospital of Shandong University (Ethics No. KYLL-2019(KJ)P-0185).
Methods
Inclusion Criteria
We included patients diagnosed with uncomplicated skin abscesses with a diameter of less than 4 cm and who refused incision and drainage or had contraindications to incision and drainage.
Before treatment, we explained to each patient the operation process using fire needle therapy and the safety and precautions after the treatment. We then gave each patient or their legal guardian 30 minutes to decide and obtain verbal consent from all patients or their legal guardian, and sign informed consent in the treatment room before treatment.
Treatment Protocol
We obtained all the patients’ or their guardians’ consents for the publication. After disinfecting the skin lesion with 75% alcohol, the lesion was treated with fire needle therapy. We chose disposable sterile stainless-steel acupuncture needles (0.30 × 25 mm, Wujiang Yunlong Medical Instrument Co Ltd). We chose the appropriate number of needles utilized during the treatment according to the patient’s tolerance. The lower part of the needle was heated using a spirit lamp until the needle was red-hot. The heated needle was then used to puncture the skin abscess lesion (approximately the depth of the skin abscess sac wall) at a 90 degrees angle for about 0.5 s before swiftly removing it. The needle spacing on the lesion was kept at around 0.5 cm apart (Figure 1C). We asked the patients to keep the lesions away from water and skin care products for 24 h.
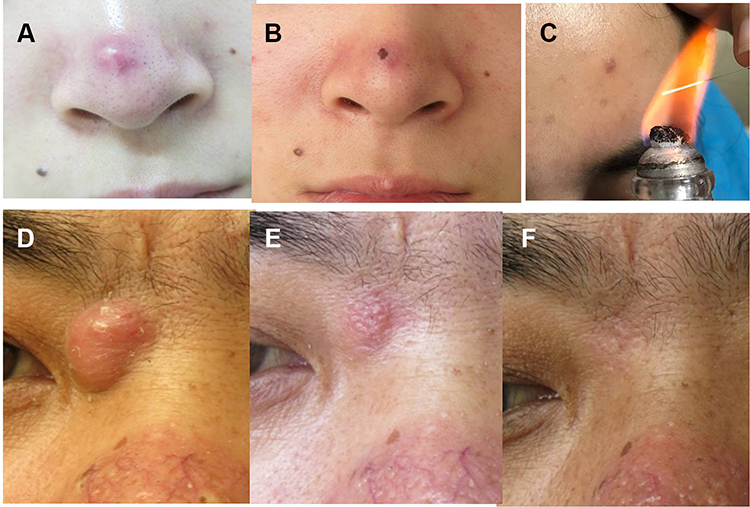 |
Figure 1 Patient 1: A furuncle on the nasal tip. (A) Lesion before fire needle therapy. (B) Lesion 2 days after fire needle therapy. (C) Fire needle therapy. Patient 4: A skin abscess on the right medial canthus. (D) Lesion before fire needle therapy. (E) Lesion 10 days after fire needle therapy. (F) Lesion after one year of fire needle therapy; no recurrence within one year. |
After piercing the skin with the fire needle, the blood and/or pus were gently squeezed out and cleaned with cotton swabs. Finally, we applied a 0.5 mm thick mupirocin ointment on the lesion with a sterile cotton swab. After treatment, the patients were asked to apply a similarly thick layer of mupirocin ointment twice a day on the lesion.
2 days following the initial treatment, we assessed the patient’s condition. If fire needling was effective and the disease did not progress, but there was still pus, the patient could be treated with fire needles again. If there was progress and/or fire needle therapy did not work, we further assessed the condition of these patients with a B-scan ultrasonography and gave them oral or intravenous antibiotics. Patients with suppuration were referred for surgery.
Apart from the pain attributed to needle insertion, we did not identify any other side effects.
Patients’ baseline data were recorded during an outpatient visit. Efficacy was assessed using a 4-grade scale: 1) complete remission (CR): complete disappearance of lesions and symptoms; or ≥90% reduction of erythema, swelling and symptoms; 2) significant remission (SR): 60–90% reduction of erythema and swelling, significant improvement of symptoms; 3) partial remission (PR): 30–60% reduction of erythema and swelling, some improvement of symptoms; 4) no remission (NR): <30% reduction of erythema and swelling, little improvement of symptoms. Follow-ups were performed at 2 days, 1 week, 2 weeks, 4 weeks and 12 weeks after the first treatment of fire needle therapy. Follow-up was terminated when recurrence was observed.
Results
Our study included 10 patients, including 5 women and 5 men, aged 1 to 45 years old. The course of the disease ranged from 3 days to 30 days (Table 1). Patients 3, 4 and 7 did not receive any treatment before the initial visit. The effect of external antibiotic ointments on the other patients before their first visit was not satisfactory.
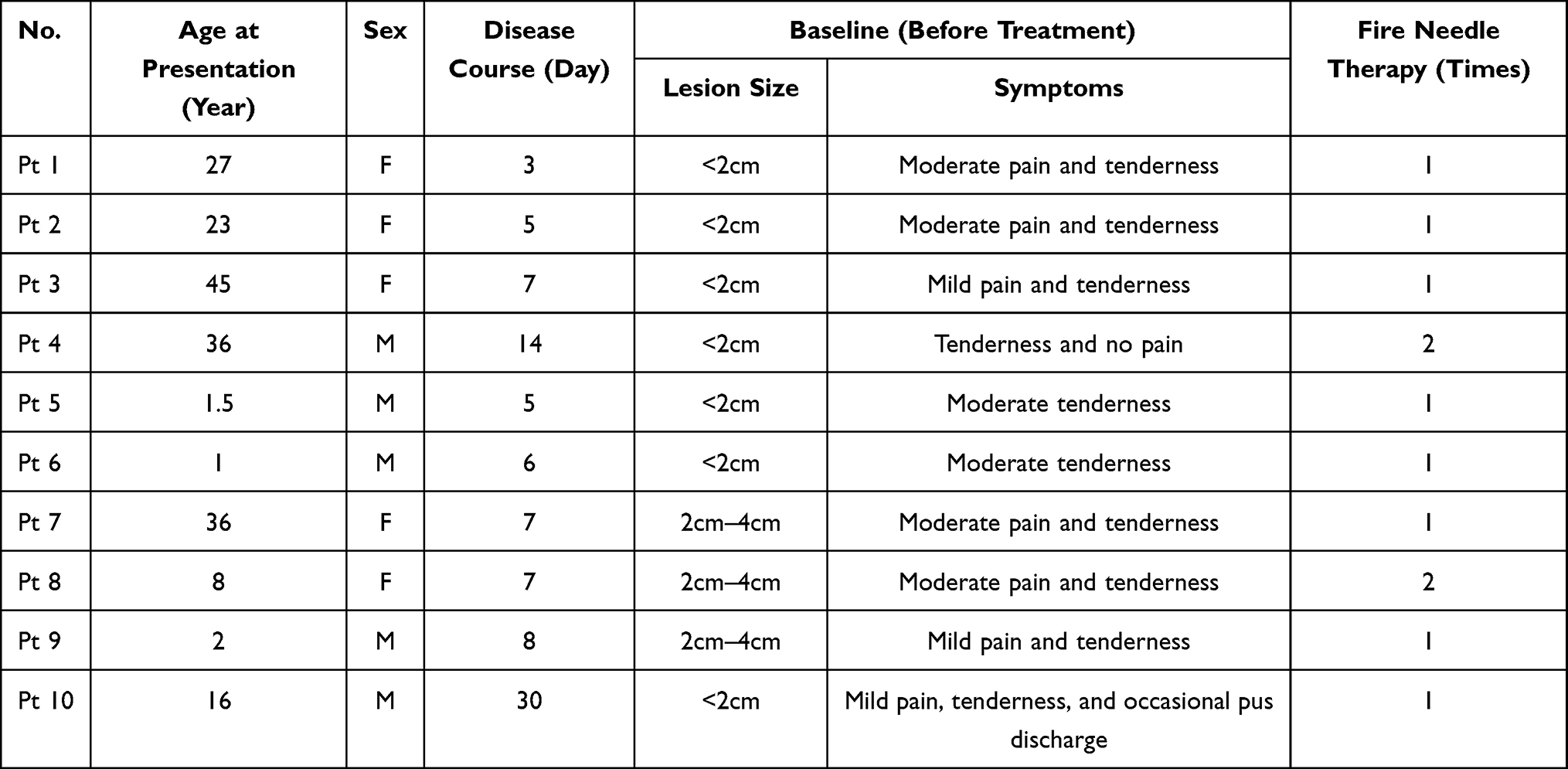 |
Table 1 Baseline Data of the Study |
Patients 1 and 2 achieved PR 2 days after one fire needle therapy and achieved SR 1 week later due to their smaller skin lesion and early onset. Patients 4 and 8 received fire needle therapy twice because of more pus, achieving SR and CR at 1 and 2 weeks, respectively, after treatment. Except for patient 4, who achieved SR 1 week after treatment due to a longer medical history, other patients with abscesses measuring less than 4 cm in diameter all achieved CR 1 week after treatment (Tables 2 and 3). Representative images are shown in Figure 1A, B, D–F. All patients had no recurrence within the 12 weeks after treatment. There was no reported recurrence in patient 4 after a 1-year follow-up post-fire needling.
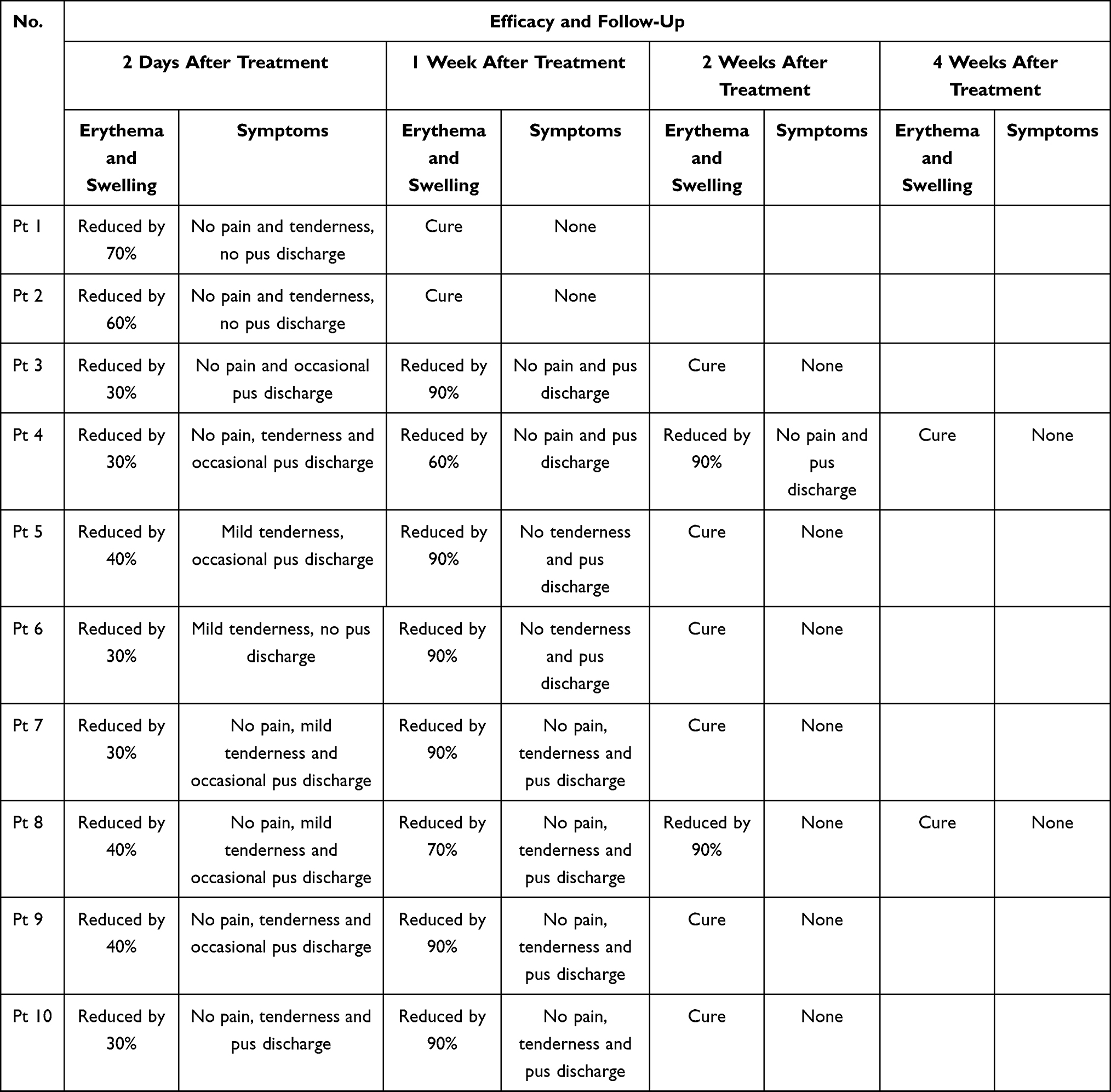 |
Table 2 Effectiveness of the Study |
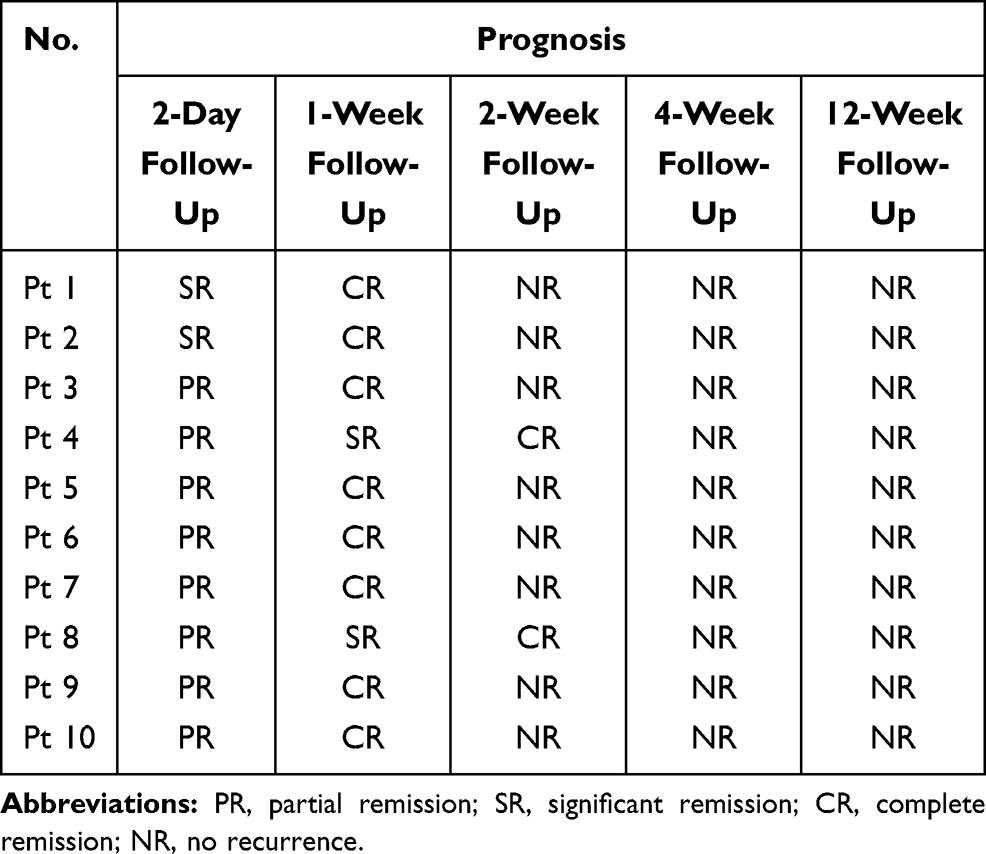 |
Table 3 Prognosis of Patients in This Study |
All treatments were well tolerated, with patients complaining of moderate pain at most that quickly subsided after a fire needle intervention.
Discussion
Abscesses are collections of pus within the dermis and deeper skin tissues. They are often caused by a progression of skin infections.2 Infections can progress rapidly, and early recognition and proper medical and surgical management are the cornerstones of successful therapy.7 Skin abscesses manifest as painful, tender, fluctuant, and erythematous nodules, frequently surmounted by a pustule and surrounded by a rim of erythematous swelling.1,2 Spontaneous drainage of purulent material may occur, and regional adenopathy may be observed.2 Based on our literature review, incision and drainage are the primary and definitive treatments of abscesses.2,8–11 Small abscesses are often self-limiting and need little to no treatment.12 Antibiotics are not recommended as an adjuvant to incision and drainage, except in cases of systemic manifestations or impaired host defenses.13 Therefore, the only way to treat an abscess is to open the pocket and drain the pus.14 Opinions on the surgical treatment are divided between saucerization, and simple incision and drainage, especially for large abscesses.15 As an alternative to incision and drainage, fire needle therapy works by puncturing the abscess to drain the pus through a tiny vulnus.
Fire needle therapy was first recorded in The Yellow Emperor’s Canon of Medicine, one of the earliest medical books in China. In the 1980s–1990s, the theoretical system of fire needle therapy developed rapidly and was more systematic.16 It is one of the three main types of acupuncture in traditional Chinese medicine and has the dual functions of heat power and acupuncture.17 In recent years, fire needle therapy has reportedly been used to treat bacterial infectious dermatosis.16,18,19 The needles used in those studies were larger than 0.6 mm in diameter and can easily cause pain and leave scars, limiting the application of fire needle therapy. Therefore, we chose stainless-steel acupuncture needles with a diameter of 0.30 mm to improve the patient’s tolerance of pain, and in all cases, we only used one needle during treatment. Based on our literature review, fire needle therapy can quickly eliminate or improve local tissue edema and adhesion to repair the damaged tissue. An animal study revealed that fire needle therapy had good therapeutic results on chronic soft tissue injury.20
The 10 cases reported above were challenging as their lesions were located in important areas that needed high aesthetic or had functional requirements. Fire needle therapy not only possesses an excellent clinical effect but can also achieve a favorable cosmetic outcome. All patients in this study could live and work as usual after the fire needle therapy. This alternative therapy promotes the discharge of pus through minor wounds and can also facilitate the absorption of topical drugs. More importantly, it is less painful than surgical incision and drainage and leaves less obvious scars.
In all cases, patients reported a notable and rapid decrease in pain after the fire needle therapy. And the wounds healed completely in about several days to three weeks, with no significant cosmetic concerns.
Aprahamian et al21 described that micro-incisions and loop drainage is a safe and effective treatment modality for subcutaneous abscesses in children. Another study described how most abscesses could be drained with a single small incision, which was safe, efficacious and led to better cosmetic results.11 Ngui et al3 reported three facial carbuncle cases with minimal necrotic tissue debridement, pus drainage and copious irrigation with gentamicin solution. The wounds healed in about two to four weeks, with no major cosmetic concerns. We believe that their method bears similarities to fire needle therapy, which also shows effectiveness in the early stage of abscess without suppuration. Patients 1 and 2 were treated in the early stage, and the time to reach SR and CR was significantly shortened. We only used the fire needle method alone for uncomplicated skin abscesses of less than 4 cm in diameter. Because fire needle therapy has the characteristics of minimal trauma, good efficacy, technically less demanding, requires less medical equipments, low cost, and results in no significant scarring, we advocate the use of fire needle therapy in the treatment of uncomplicated skin abscesses. It is especially good for abscesses in areas that require high cosmetic or functional requirements, such as the face, neck and breast. Furthermore, it might be suitable for patients who cannot tolerate or refuse surgical debridements, such as children and the elderly. Fire needle therapy can quickly relieve swelling and pain, control the development of skin abscesses, thereby reducing the use of intravenous or oral antibiotics and incidence of bacterial resistance. In conclusion, fire needle therapy is a simple and safe treatment, which may be an effective alternative strategy for dealing with uncomplicated skin abscesses.
Abscesses are a common form of skin and soft-tissue infections and are increasing in incidence. It is not difficult to diagnose by careful history and clinical examination. Although the standard approach of incision and drainage remains a mainstay of abscess management, the use of fire needle therapy may be considered in appropriate cases and may even provide a better alternative.
Conclusion
The present study was designed to determine the effect of fire needles on uncomplicated skin abscesses. The findings indicate that fire needle therapy showed a quick reduction in pain, promoted rapid recovery of the infection, provided significant benefits in terms of cosmetic outcome, reduced the systemic use of antibiotics and lowered patients’ medical costs. In general, fire needle therapy is a likely alternative, conservative and promising treatment method for small uncomplicated skin abscesses.
Acknowledgments
All the authors thank the operators of all cases, Ying-Cai, Changyu-Han, Mengdi-Sun, Lu-Cui. We also thank all patients and their guardians for their consent to the publication.
Funding
This work was supported by the National Natural Science Foundation of China (81973856), the Natural Science Foundation of Shandong Province (ZR2017MH126).
Disclosure
All authors declare that there are no conflicts of interest.
References
1. Stulberg DL, Penrod MA, Blatny RA. Common bacterial skin infections. Am Fam Physician. 2002;66:119–124. doi:10.1080/00325481.1993.11701692.
2. Ibrahim F, Khan T, Pujalte GGA. Bacterial skin infections. Prim Care. 2015;42:485–499. doi:10.1016/j.pop.2015.08.001.
3. Ngui LX, Wong LS, Shashi G, Abu Bakar MN. Facial carbuncle - a new method of conservative surgical management plus irrigation with antibiotic-containing solution. J Laryngol Otol. 2017;131:830–833. doi:10.1017/S0022215117000834.
4. Zhang Zhao-hui M, Xuya JL, Qiang X. The application of annular drainage with electric pyropuncture needle for treatment of patients with diabetic foot. Chin J TCM W M Crit Care. 2012;19:220–222.
5. Guo H, Liu G. Clinical observation of electric fire needle drainage combined with local closure in the treatment of head abscess perforating perifolliculitis. Tianjin J Tradit Chin Med. 2016;33:541–544.
6. Shen H, Gu J, Feng Q, et al. Clinical observation on abscess of breast carbuncle in purulent stage treated by burning hole with fire needle and adding medicine line drainage. JETCM. 2014;23:2127–2128.
7. Brook I. Microbiology and management of soft tissue and muscle infections. Int J Surg. 2008;6(4):328–338. doi:10.1016/j.ijsu.2007.07.001
8. Talan DA. Adjunctive antibiotics for drained skin abscesses improve clinical cure rate. Evid Based Med. 2017;22:214. doi:10.1136/ebmed-2017-110815
9. Vermandere M, Aertgeerts B, Agoritsas T, et al. Antibiotics after incision and drainage for uncomplicated skin abscesses: a clinical practice guideline. BMJ. 2018;360:1–8. doi:10.1136/bmj.k243
10. Aung KK. Guideline: TMP–SMX is recommended after uncomplicated skin abscess incision and drainage. Ann Intern Med. 2018;168:JC50. doi:10.7326/ACPJC-2018-168-10-050
11. Singer AJ, Talan DA. Management of Skin abscesses in the era of methicillin-resistant Staphylococcus aureus. N Engl J Med. 2014;370:1039–1047. doi:10.1056/nejmra1212788
12. Galli L, Venturini E, Bassi A, et al. Common community-acquired bacterial skin and soft-tissue infections in children: an intersociety consensus on impetigo, abscess, and cellulitis treatment. Clin Ther. 2019;41:532–551.e17. doi:10.1016/j.clinthera.2019.01.010
13. Stevens DL, Bisno AL, Chambers HF, et al. Executive summary: practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147–159. doi:10.1093/cid/ciu296
14. Baiu I, Melendez E. Skin abscess. JAMA. 2018;319(13):1405. doi:10.1001/jama.2018.1355
15. Guan Hee T, Jan Jin B. The surgical treatment of carbuncles: a tale of two techniques. Iran Red Crescent Med J. 2013;15(4):367–370. doi:10.5812/ircmj.2992
16. Changjin Huang CC, Huang Y. The origin and development of fire needle therapy. Chin Acupunct Moxibustion. 2013;33:455–458. doi:10.13703/j.0255-2930.2013.05.022
17. Huang M, Tang L, Li X, et al. Clinical observation on therapeutic effect of filiform fire needle for vitiligo: a Retrospective Study. Dermatol Ther. 2020;33(6). doi:10.1111/dth.14415
18. Pan Zhang HZ, Wang Z, Chao G, Huang P. Mechanism of fire needle therapy and its research progress in treatment of erysipelas ZHANG. Jilin J Tradit Chin Med. 2015;35:418–420. doi:10.1017/CBO9781107415324.004
19. Min Jiang WW, Jiang K, Zeng X. Observations on the efficacy of fire needling plus medication in treating cystic acne. Shanghai J Acu Mox. 2015;34:1082–1084. doi:10.3969/j.issn.1005-0957.2010.11.700
20. Jun W, Rongrong S, Rongshi S. Experimental study on treatment of chronic soft tissue injuries with fire-needle therapy. Chin Acupunct Moxibustion. 2002;31–33. doi:10.3969/j.issn.1008-8849.2003.21.007
21. Aprahamian CJ, Nashad HH, DiSomma NM, et al. Treatment of subcutaneous abscesses in children with incision and loop drainage: a simplified method of care. J Pediatr Surg. 2017;52(9):1438–1441. doi:10.1016/j.jpedsurg.2016.12.018
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.