")
Back to Journals » OncoTargets and Therapy » Volume 12
Effect of XPC polymorphisms on the response to platinum-based chemotherapy: a meta-analysis
Authors Xie C, Zhao J, Hua W, Tan P , Chen Y, Rui J, Sun X , Fan J, Wei X, Xu X, Yang X
Received 23 January 2019
Accepted for publication 28 March 2019
Published 16 May 2019 Volume 2019:12 Pages 3839—3848
DOI https://doi.org/10.2147/OTT.S202617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Chenyao Xie,1,* Jing Zhao,1,* Wenxi Hua,2,* Pei Tan,1,* Yudi Chen,1,* Jingwen Rui,2 Xiaohan Sun,1 Jiaying Fan,1 Xiangyu Wei,1 Xiaojing Xu,1 Xiaoqin Yang1
1School of Biology and Basic Medical Sciences, Soochow University, Suzhou 215123, People’s Republic of China; 2Medical College, Soochow University, Suzhou 215123, People’s Republic of China
*These authors contributed equally to this work
Objective: As an important DNA repair gene, the xeroderma pigmentosum complementation group C (XPC) gene and its functional genetic variants’ relationship with chemotherapy response has been extensively studied. To quantitatively elucidate the genetic impact of the XPC rs2228000 and rs2228001 polymorphisms on the response to platinum-based chemotherapy, the present meta-analysis was conducted.
Materials and methods: A systematic literature search was performed in seven cyber databases until February 20, 2019, for all relevant studies that assessed the relationship between XPC polymorphisms and the response to platinum-based chemotherapy. Odds ratios (ORs) with a 95% confidence interval (95% CI) were measured to assess the strength of the association. R programs were developed to perform the statistical analyses, including calculations of pooled estimates, publication bias and sensitivity analyses, and heterogeneity interpretations.
Results: A total of 1,615 patients from 10 studies for the rs2228001 polymorphism were winnowed for further statistical analysis. For the rs2228000 polymorphism, 858 samples from six datasets were included. However, this meta-analysis indicated no significant effect of these two XPC polymorphisms on the response to platinum-based chemotherapy. When stratified according to sample size, country or cancer type, no statistical significance for association was identified in all subgroups. Further sensitivity analysis and publication bias assessment ensured the reliability of the meta-analysis.
Conclusions: The pooled estimates suggest that neither the rs2228000 polymorphism nor the rs2228001 polymorphism contributes to the genetic predisposition for an altered response to platinum-based chemotherapy. Considering the limitations of our present meta-analysis, more studies with large-scale cohorts and rigorous methods are needed to validate our results.
Keywords: XPC, polymorphism, meta-analysis, platinum-based chemotherapy
Introduction
As a mainstay of chemotherapy, platinum-based regimens are still widely employed for the treatment of a wide spectrum of advanced-stage cancers. Unfortunately, in clinical practice, a significant proportion of patients exhibit intrinsic or acquired resistance to platinum-based therapies. Genome structural variations, such as single nucleotide polymorphisms (SNPs), are genetic factors that may influence chemotherapy response.1 Therefore, extensive studies have been conducted on the genetic loci associated with sensitivity to platinum-based regimens.
As an important DNA damage recognition protein, xeroderma pigmentosum complementation group C (XPC) plays a key role in nucleotide excision repair. In vitro experiments suggest that XPC overexpression could lead to enhanced sensitivity to cisplatin treatment,2 and its defect could result in reduced p53 responses to cisplatin treatment.3 Two common polymorphic loci of the XPC gene, rs2228000 (G>A, Ala499Val) and rs2228001 (G>T, Lys939Gln), have been investigated for the effectiveness of carcinogenesis.4–6 Scattered evidence has demonstrated that the G allele homozygotes of these two polymorphisms could lead to significantly increased XPC mRNA expression in the Asian population.4,7 Given the obvious importance of the XPC gene, it is reasonable to hypothesize that the XPC rs2228000 and rs2228001 polymorphisms can affect responses to platinum-based therapy.
Several previous association studies tried to quantitatively assess the relationship between the XPC polymorphism and the response to platinum-based chemotherapy. However, their results were incongruous, and those scattered datasets were also plagued by small sample sizes and consequently led to very restricted statistical power. The aim of this meta-analysis was to comprehensively evaluate the diagnostic value of the XPC genotypes of the rs2228000 and rs2228001 polymorphisms as a biomarker for chemotherapy response in cancer patients subjected to platinum-based treatments.
Materials and methods
Literature search
For this study, a comprehensive literature screening was conducted to identify relevant datasets published in the China Knowledge Resource Integrated Database (
Study selection
For a dataset to be included in this meta-analysis, full-text content should be accessible, and the corresponding relevant study had to meet the following predefined inclusion criteria: (1) study for the XPC polymorphism (rs2228000 or rs2228001); (2) study for the response to platinum-based cancer chemotherapy; and (3) enough genotype data to construct at least one genetic comparison model. Studies were taken out from further processing when failing any of the prespecified exclusion criteria: (1) nonplatinum-based chemotherapy; (2) no data for chemotherapy response; (3) no data for the XPC polymorphisms; (4) duplicated data; (5) noncancer study; or (6) no chemotherapy response evaluation criteria or details in responder definition.
Data extraction and processing
The name of the author and the publication year were extracted from individual studies to mark the corresponding dataset used in further meta-analyses. Information regarding the features of the study design and patient characteristics were included. We recorded cancer type, chemotherapy regimens, geographical region, and criteria in the assessment of treatment outcomes. Furthermore, the numbers of patients with good and poor response for different polymorphism genotypes were extracted to construct 2×2 contingency tables for statistical analysis. The methodological quality assessment for the eligible studies was conducted according to the 9-point Newcastle–Ottawa Scale (NOS,
Statistical analysis
Statistical meta-analyses were conducted with our in-house R pipeline (R version: 3.5.1,
All steps involved in this study strictly complied with the principles of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) from the beginning until the end.14 At least three investigators participated in every step of this meta-analysis. All inconsistencies were resolved by discussion among all investigators.
Results
Literature search and data extraction
After removing duplicates, our initial literature screening yielded 282 manuscripts and theses. Among them, 76 were in English and 206 were in Chinese. The number of relevant studies was narrowed down through the implementation of the predefined inclusion and exclusion criteria. A total of ten articles with relevant datasets were identified.15–24 Of the ten included datasets, there were four studies for lung cancer,15,16,19,23 three for ovarian cancer,20,22,24 one for cervical cancer,21 one for gastric cancer,18 and one for bone malignant tumor.17 For the XPC rs2228000 polymorphism, six studies with 409 good responders and 449 poor responders to chemotherapy were included.15,16,19,20,22,23 For the XPC rs2228001 polymorphism, the corresponding numbers collected from 10 datasets were 892 and 723, respectively.15–24 The workflow of the literature selection process is demonstrated in Figure 1. The characteristics of the involved studies are summarized in Table 1. All included studies for both polymorphisms were considered good or moderate quality according to the NOS scores. Specifically, one cervical cancer study for the rs2228001 polymorphism only presented the genotype data for the major allele homozygote (AA) and the minor allele carriers (Aa+aa), which could only be integrated in the dominant model.21 Two case–control studies were not integrated into our meta-analysis for the rs2228001 polymorphism. One osteosarcoma study was excluded because of the discrepancy between the number of poor responders and the sum of homozygote wild-type, heterozygote mutant, and homozygote mutant of these samples.25 One study for cisplatin-based chemotherapy on esophageal squamous cell carcinoma was not included due to the lack of details of the definitions of good and poor responders.26
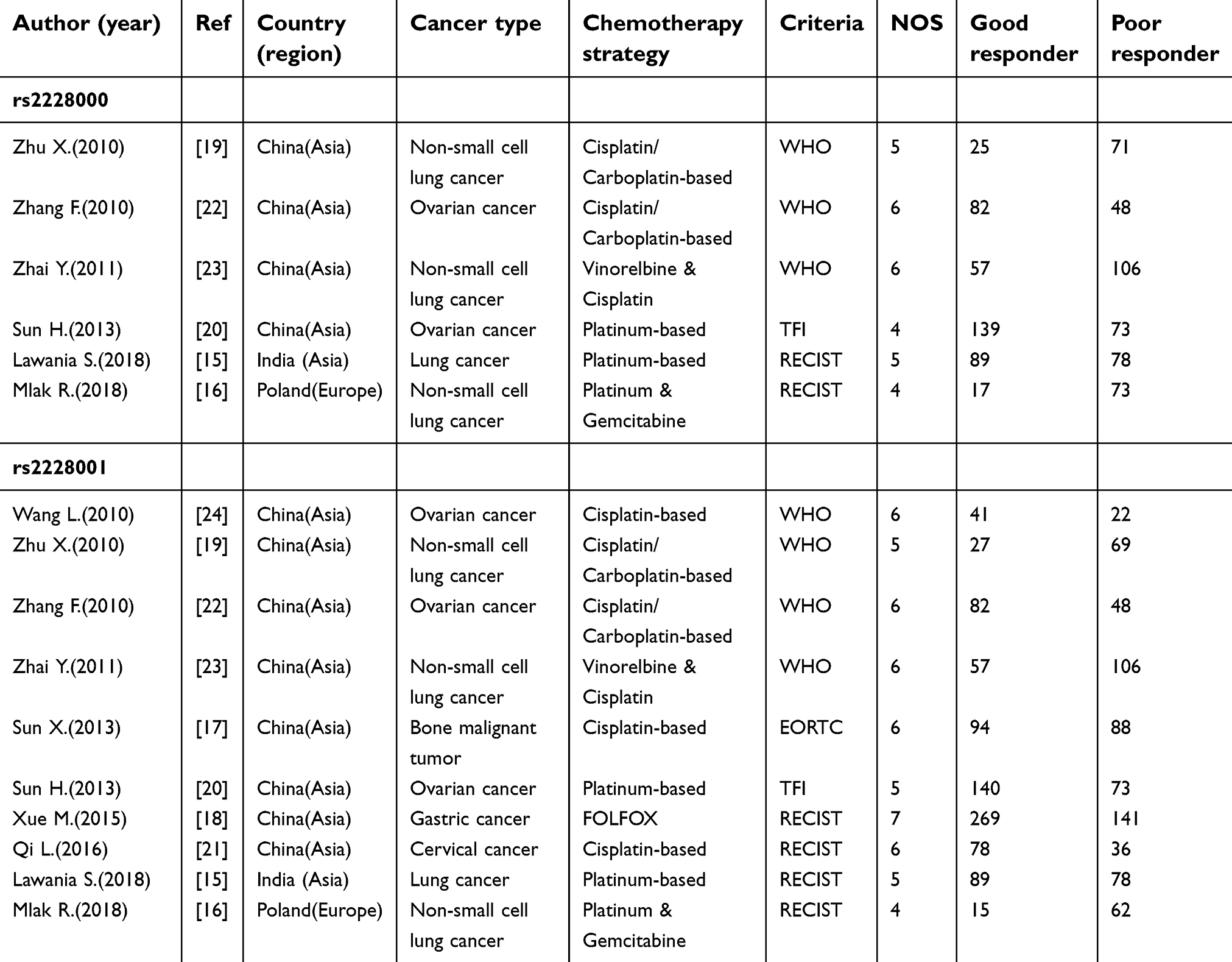 | Table 1 Principal characteristics of studies included in this meta-analysis |
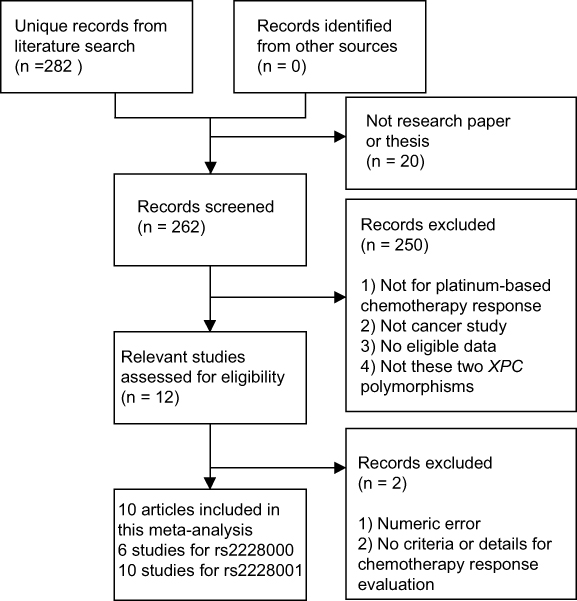 | Figure 1 Flowchart showing the detailed processes of literature screening and study selection. |
Meta-analysis and subgroup analysis
In the overall population, there was no statistical significance for the association between the XPC rs2228000 polymorphism and the response to platinum-based chemotherapy (homozygote model: OR=1.46, 95% CI 0.84–2.54; heterozygote model: OR=1.23, 95% CI 0.90–1.67; dominant model: OR=1.27, 95% CI 0.95–1.70, Figure 2; recessive model: OR=1.35, 95% CI 0.80–2.29). Stratified analysis by sample size did not reveal a material difference between the large sample size subgroup and the small sample size subgroup. Studies were also classified according to geographical region. The pooled estimates suggested that this polymorphism could not influence the platinum-based chemotherapy response in the Chinese population and in populations from other countries. No statistical significance for pooled estimates could be observed in all subgroups divided according to chemotherapy response evaluation criteria. Stratification by cancer type also showed no substantial differences for the subgroups of lung cancer and other cancers (Table 2).
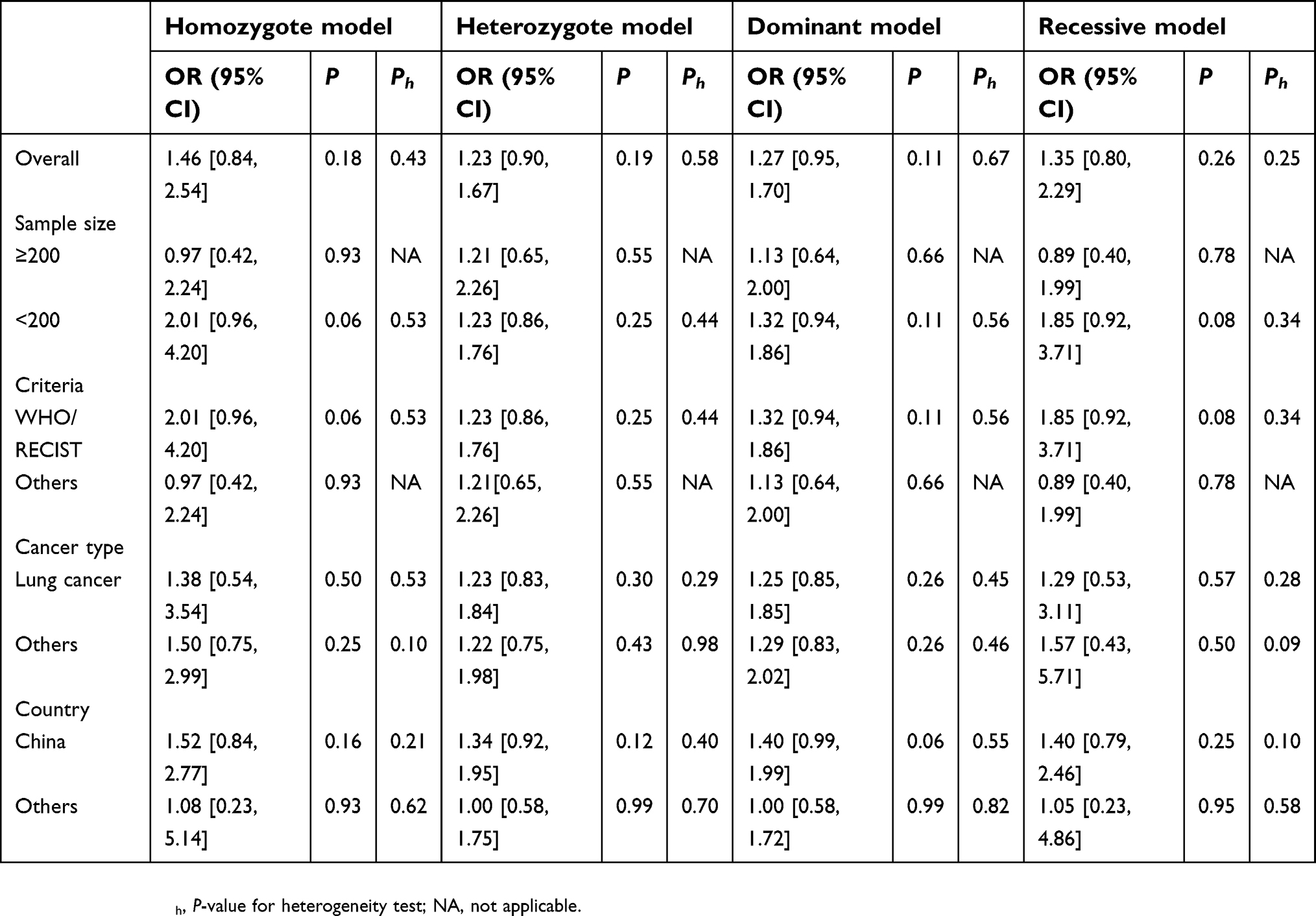 | Table 2 Association between the XPC rs2228000 polymorphism and the response to platinum-based chemotherapy |
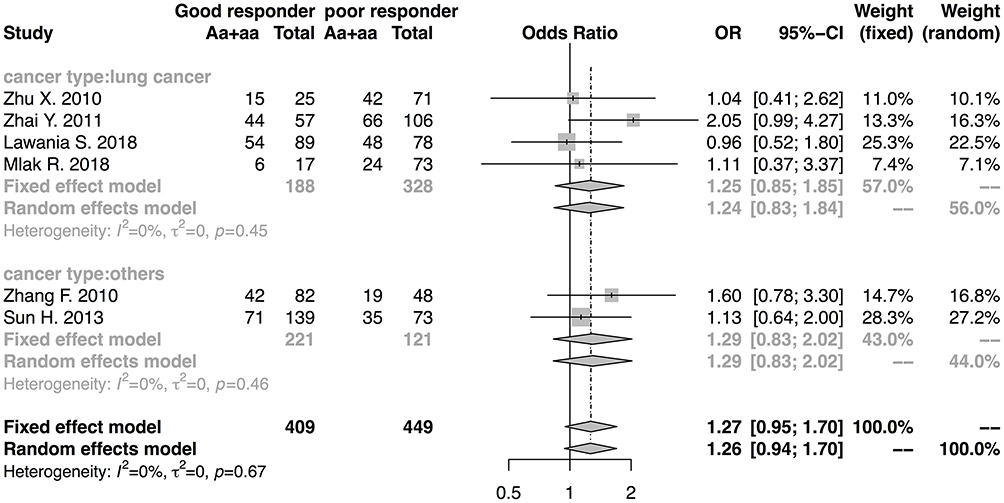 | Figure 2 Forest plot showing the association between the XPC rs2228000 polymorphism and the response to platinum-based chemotherapy. The odds ratio (OR) and corresponding 95% confidence interval (95% CI) were calculated under the dominant model. Involved studies were stratified according to cancer type. Each study was labeled with the name of the author and the year of publication. The area of the gray box represents the weight of the sample size assigned under the fixed effect model. The lateral points of the gray diamond icon represent the upper and lower bounds of a 95% CI, while the vertical points indicate the point estimate. The solid vertical line represents the null effect (OR=1). A represents the major allele, and a represents the minor allele. |
As for the XPC rs2228001 polymorphism, the quantitative synthesis of the included studies revealed no statistical significance for its association with response to platinum-based chemotherapy (homozygote model: OR=0.84, 95% CI 0.53–1.32; heterozygote model: OR=0.83, 95% CI 0.54–1.27; dominant model: OR=0.87, 95% CI 0.60–1.27, Figure 3; recessive model: OR=0.99, 95% CI 0.75–1.32). When subdivided by sample size, neither the subgroup with ≥200 samples nor the subgroup with <200 samples showed a statistically significant change. Regarding the geographical region of the involved studies, the pooled estimates indicated no conflict between patients from China and from other nations. Stratified analysis according to chemotherapy response evaluation criteria indicated that the null hypothesis could not be rejected in any subgroups. When restricting the analysis to lung cancer or other cancers, no significance was evident in either subgroup under all genetic models (Table 3).
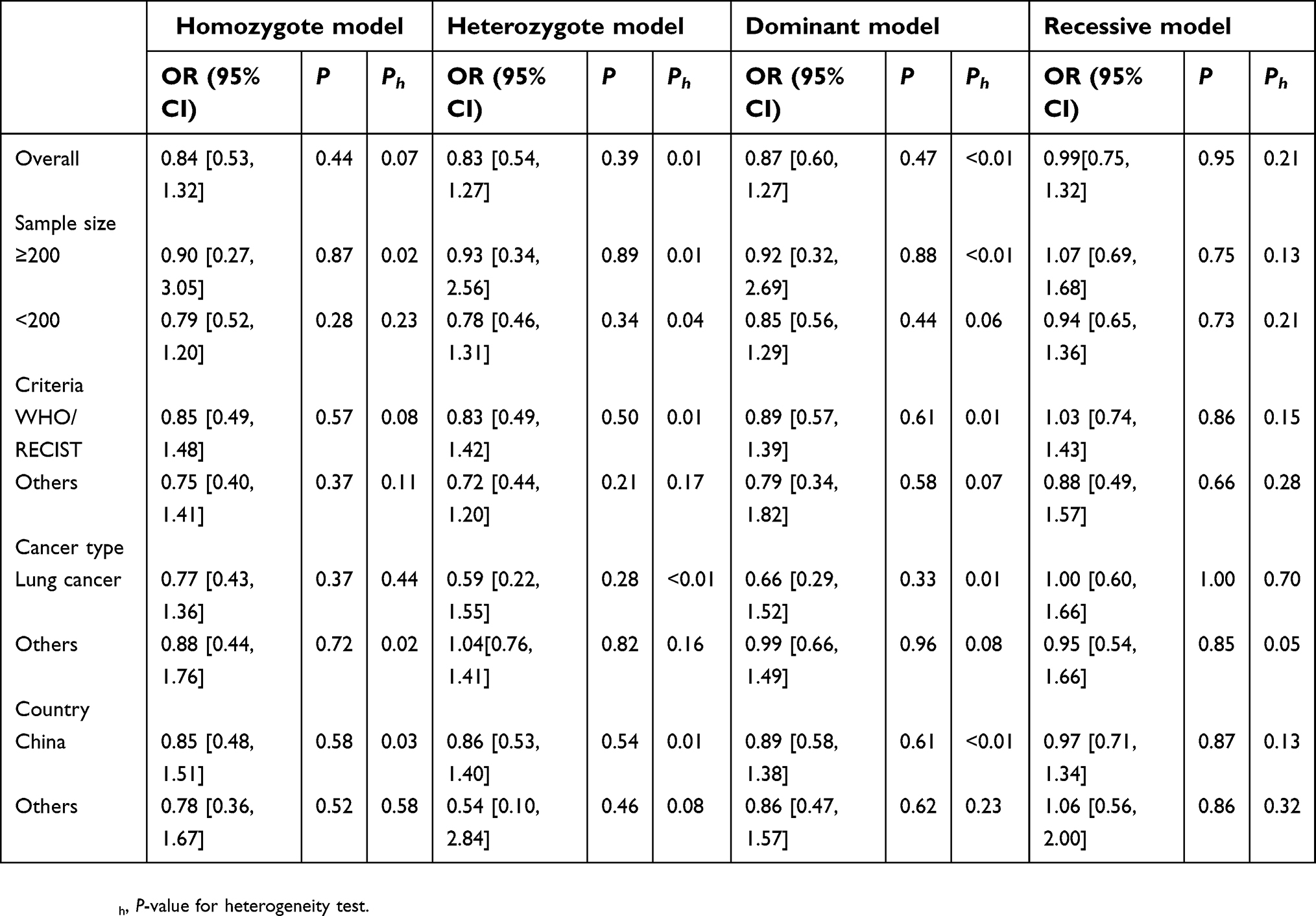 | Table 3 Association between the XPC rs2228001 polymorphism and the response to platinum-based chemotherapy |
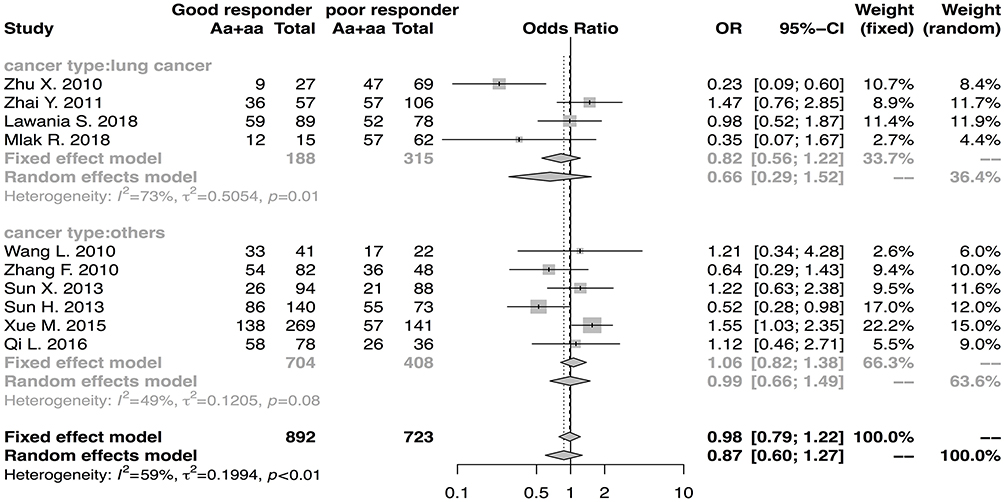 | Figure 3 Forest plot showing the association between the XPC rs2228001 polymorphism and the response to platinum-based chemotherapy. The odds ratio (OR) and corresponding 95% confidence interval (95% CI) were calculated under the dominant model. Involved studies were stratified according to cancer type. Each study was labeled with the name of the author and the year of publication. The area of the gray box represents the weight of the sample size assigned under the fixed effect model. The lateral points of the gray diamond icon represent the upper and lower bounds of a 95% CI, while the vertical points indicate the point estimate. The solid vertical line represents the null effect (OR=1). A represents the major allele, and a represents the minor allele. |
Publication bias and sensitivity analysis
Publication bias was interpreted by visual inspection of the degree of asymmetry in the Begg’s funnel plots. For both polymorphisms studied in this meta-analysis (Figures 4 and 5), no evidence of obvious asymmetry could be drawn from the funnel plots, which indicated only a tiny likelihood of publication bias. By omitting individual datasets, their influence on the pooled estimates was evaluated. The results suggested no material change of statistical significance (data not shown).
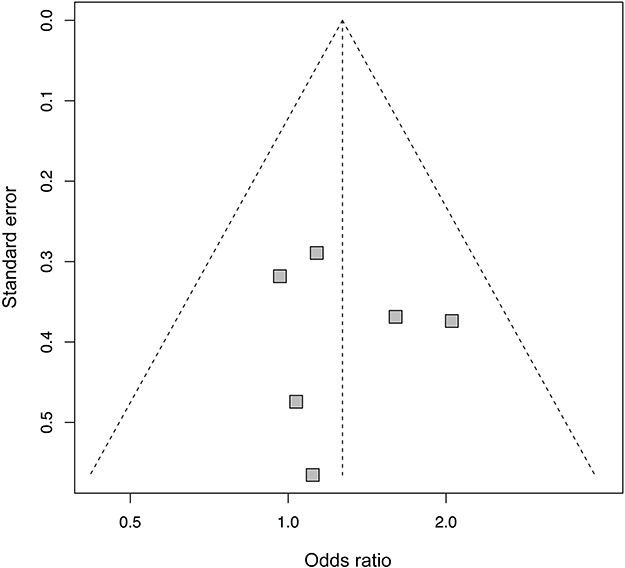 | Figure 4 Funnel plot of the meta-analysis for the XPC rs2228000 polymorphism under the dominant model. Each gray square represents an included dataset. The vertical dashed line indicates the pooled odds ratio. The funnel defined by the two crossed dashed lines represents the pseudo 95% confidence interval. |
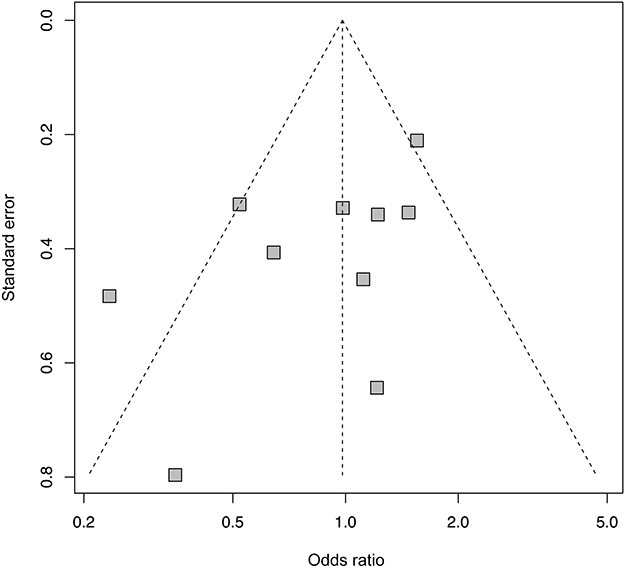 | Figure 5 Funnel plot of the meta-analysis for the XPC rs2228001 polymorphism under the dominant model. Each gray square represents an included dataset. The vertical dashed line indicates the pooled odds ratio. The funnel defined by the two crossed dashed lines represents the pseudo 95% confidence interval. |
Heterogeneity analysis
For the XPC rs2228001 polymorphism, significant between-study heterogeneity was detected in the homozygote, heterozygote, and dominant models. Galbraith plot analysis (data not shown) identified two outliers in the homozygote model,18,22 two in the heterozygote model,18,19 and three in the dominant model18-20 as the potential sources of heterogeneity. The removal of these outliers significantly reduced the between-study heterogeneity (homozygote model: heterogeneity test P-value=0.38; heterozygote model: heterogeneity test P-value=0.26; dominant model: heterogeneity test P-value=0.59) but did not materially influence the significance of the pooled estimates (homozygote model: OR=0.81, 95% CI 0.54–1.22, P-value=0.31; heterozygote model: OR=0.90, 95% CI 0.66–1.23, P-value=0.50; dominant model: OR=1.04, 95% CI 0.77–1.41, P-value =0.78).
Discussion
Based on the published datasets, we intended to quantitatively elucidate the possible genetic impact of the XPC rs2228000 and rs2228001 polymorphisms on the response to platinum-based chemotherapy. The lack of a significant effect on the response to chemotherapy might reflect the unlikelihood of these two XPC polymorphisms as causative factors for altered sensitivity to platinum-based regimens, masking the potential involvement of other genetic or clinical factors. However, these conclusions did not differ from the findings in the stratified analysis according to cancer type, sample size, and country. Other confounding factors not discussed in this study, such as cancer stage, patient age, and accumulative effect of genetic variances, should be included in further research when data are available.
In this meta-analysis, we only selected studies with explicit criteria for chemotherapy response evaluation and details of the definition process. This selection was done to avoid the impact on the accuracy of pooled estimates led by inconsistency, which could result from the simultaneous inclusion of heterogeneous case and control groups. The details for using the same response evaluation criteria could be quite different between studies. For example, several studies using the RECIST criteria defined complete response (CR), partial response (PR), and stable disease (SD) as good responders,27,28 while some studies grouped CR and PR as good responders15,21 We did not include the data set for esophageal squamous cell carcinoma26 in our meta-analysis for rs2228001 due to its lack of details in responder definition. However, we still calculated the pooled estimates after adding this dataset. No material change for statistical significance could be observed (homozygote model: OR=0.75, 95% CI 0.48–1.18; heterozygote model: OR=0.87, 95% CI 0.60–1.25; dominant model: OR=0.87, 95% CI 0.63–1.21; recessive model: OR=0.86, 95% CI 0.59–1.27), which indicated the stability of our results.
For the XPC rs2228001 polymorphism, significant between-study heterogeneity was detected in the homozygote, heterozygote and dominant models. However, the removal of the identified outliers18-20,22 in the Galbraith plots not only led to significant relief of heterogeneity but also indicated the stability of the pooled estimates. However, the hidden confounding factors introduced by these outliers could not be explored in the present study due to the lack of detailed clinical information for the samples involved in the included studies. For this reason, further large-scale multicenter-clinical studies with elaborate, relevant data should be performed to address the impact of these factors. For the two polymorphisms, sensitivity analysis further strengthened stability, and the inference of publication bias also revealed unbiasedness. Because of the advantages listed earlier, we are greatly confident in the robustness of the results.
The accuracy of genotyping experiments and chemotherapy response measurements in the genetic association studies involved in this meta-analysis could vary according to the personal experience of the genotype researchers and clinical investigators. Furthermore, the differences inherent in both the variance of chemotherapy regimens and the different chemotherapy response evaluation criteria should not be ignored. These subjective factors were out of the scope of this study but are important areas that need to be taken into account in prospective settings for future research.
Although this meta-analysis strictly followed the principles suggested by the PRISMA guidelines for meta-analysis,14 a number of inherent limitations should be noted when interpreting the results. First, the number of involved studies was relatively small, and the sample size was comparatively limited, especially for the XPC rs2228000 polymorphism, calling for updated analyses when more datasets are available. Moreover, the influence of other XPC polymorphisms in the response to platinum-based chemotherapy was not evaluated in this meta-analysis because of limited sample sizes. Furthermore, several cancer types receiving platinum-based chemotherapy were not covered in this meta-analysis also due to the lack of data. Last but not least, most of the involved studies originated from Asia, especially China, which significantly impacted ethnic variety and could subsequently lead to sampling bias. However, the superiority of this meta-analysis should be worth noting. Compared with every single study included, the conclusions drawn from this meta-analysis showed higher authenticity based on a substantially enlarged sample size and consequently increased statistical power and a greatly minified risk of random errors. On the other hand, the results of the NOS quality assessment, sensitivity evaluation, and publication bias analysis further ensured robustness.
Conclusions
In conclusion, our pooled estimates of meta-analysis based on a systematic literature review revealed no statistically significant association between the XPC rs2228000 and rs2228001 polymorphisms and the response to platinum-based chemotherapy. However, further statistical investigation will be merited with the synthesis of more multicentric datasets with a large sample size to elucidate the impact of the XPC polymorphisms on the response to platinum-based chemotherapy.
Acknowledgments
This study was funded by the research start-up fund of Soochow University (Q413400116), the natural Science Foundation of Jiangsu Province (No. BK20170334), the Priority Academic Program Development of Jiangsu Higher Education Institutions, and the National Undergraduate Training Program for Innovation and Entrepreneurship (201810285050Z).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Rosell R, Wei J. Single nucleotide polymorphisms (SNPs) in non-small cell lung cancer (NSCLC) patients. Oncologist. 2012;17(12):1484–1485. doi:10.1634/theoncologist.2012-0205
2. Chen Z, Yang J, Wang G, Song B, Li J, Xu Z. Attenuated expression of xeroderma pigmentosum group C is associated with critical events in human bladder cancer carcinogenesis and progression. Cancer Res. 2007;67(10):4578–4585. doi:10.1158/0008-5472.CAN-06-0877
3. Wang G, Chuang L, Zhang X, et al. The initiative role of XPC protein in cisplatin DNA damaging treatment‐mediated cell cycle regulation. Nucleic Acids Res. 2004;32(7):2231–2240. doi:10.1093/nar/gkh541
4. He J, Shi TY, Zhu ML, Wang MY, Li QX, Wei QY. Associations of Lys939Gln and Ala499Val polymorphisms of the XPC gene with cancer susceptibility: a meta-analysis. Int J Cancer. 2013;133(8):1765–1775. doi:10.1002/ijc.28089
5. Jiang X, Zhou LT, Zhang SC, Chen K. XPC polymorphism increases risk of digestive system cancers: current evidence from a meta-analysis. Chin J Cancer Res. 2012;24(3):181–189. doi:10.1007/s11670-012-0181-0
6. Francisco G, Menezes PR, Eluf-Neto J, Chammas R. XPC polymorphisms play a role in tissue-specific carcinogenesis: a meta-analysis. Eur J human genet. 2008;16(6):724–734. doi:10.1038/ejhg.2008.6
7. Zhu M-L, Hua R-X, Zheng L. Associations between polymorphisms of the XPC gene and lung cancer susceptibility: a meta-analysis. Tumor Biol. 2014;35(4):2931–2939. doi:10.1007/s13277-013-1377-8
8. Schwarzer G. Meta: an R package for meta-analysis. R News. 2007;7(3):40–45.
9. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–748.
10. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188.
11. Galbraith R. A note on graphical presentation of estimated odds ratios from several clinical trials. Stat Med. 1988;7(8):889–894.
12. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634.
13. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;1088–1101. doi:10.2307/2533446
14. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339.
15. Lawania S, Singh N, Behera D, Sharma S. XPC polymorphism and risk for lung cancer in north indian patients treated with platinum based chemotherapy and its association with clinical outcomes. Pathol Oncol Res. 2018;24(2):353–366. doi:10.1007/s12253-017-0252-0
16. Mlak R, Krawczyk P, Homa-Mlak I, et al. Predictive value of single nucleotide polymorphisms of ERCC1, XPA, XPC, XPD and XPG genes, involved in NER mechanism in patients with advanced NSCLC treated with cisplatin and gemcitabine. Pathol Oncol Res. 2018. doi:10.1007/s12253-018-0459-8
17. Sun X-H, Hou W-G, Zhao H-X, Zhao Y-L, Ma C, Liu Y. Single Nucleotide Polymorphisms in the NER Pathway and Clinical Outcome of Patients with Bone Malignant Tumor. Asian Pac J Cancer Prev. 2013;14(3):2049–2052.
18. Xue M-H, Li G-Y, Wu X-J, Zhang C-X, Zhang C-F, Zhu K-X. Genetic variability of genes in NER pathway influences the treatment outcome of gastric cancer. Int J Clin Exp Pathol. 2015;8(5):5563–5569.
19. Zhu XL, Sun XC, Chen BA, et al. XPC Lys939Gln polymorphism is associated with the decreased response to platinum based chemotherapy in advanced non-small-cell lung cancer. Chin Med J. 2010;123(23):3427–3432.
20. Sun H. Association of Single Nucleotide Polymorphism in DNA Repair Gene with the Clinical Outcome to Platinum-Based Chemotherapy in Epithelial Ovarian Cancer. Shijiazhuang, Hebei, China: Hebei Medical University; 2013.
21. Qi L, Lv J, Zhu X, et al. Association between ERCC1, XPD, XPC polymorphisms and chemosensitivity of platinum-based neoadjuvant chemotherapy in patients with locally advanced cervical cancer. J Wenzhou Med Univ. 2016;46(10):724–729.
22. Zhang F. Association of the DNA Repair Gene XPC Polymorphisms with Susceptibility to Platinum-Based Chemotherapy in Epithelial Ovarian Cancer. Shijiazhuang, Hebei, China: Hebei Medical University; 2010.
23. Zhai Y, Xu Q, Hong C, Zhang Y, Yuan Y. The correlation of the sensitivity to NP chemotherapy in non-small lung cancer to DNA repair gene XPC polymorphism. Med J Liaoning. 2011;25(4):177–183.
24. Wang L. Correlation of Genotype in Nucleotide Excision Repair System to Sensitivity of Epithelial Ovarian Carcinoma Patients to Platinum-Based Chemotherapy. Wenzhou, Zhejiang, China: Wenzhou Medical University; 2010.
25. Zhao Y-L, Yang L-B, Geng X-L, et al. The association of XPG and MMS19L polymorphisms response to chemotherapy in osteosarcoma. Pak j med sci. 2013;29(5):1225–1229.
26. Yang PW, Hsieh CY, Kuo FT, et al. The survival impact of XPA and XPC genetic polymorphisms on patients with esophageal squamous cell carcinoma. Ann Surg Oncol. 2013;20(2):562–571. doi:10.1245/s10434-012-2622-x
27. Shindo Y, Hazama S, Maeda Y, et al. Adoptive immunotherapy with MUC1-mRNA transfected dendritic cells and cytotoxic lymphocytes plus gemcitabine for unresectable pancreatic cancer. J Transl Med. 2014;12(1):175. doi:10.1186/1479-5876-12-175
28. Zhou J, Deng W, Gao J, Yuan J, Li Y, Shen L. Association between ABCB1 G2677T/A polymorphisms and chemosensitivity of paclitaxel in advanced gastric cancer. Chin J Gastrointestinal Surg. 2015;18(2):123–126.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.