")
Back to Journals » Clinical Ophthalmology » Volume 11
Effect of topical 3% diquafosol sodium on eyes with dry eye disease and meibomian gland dysfunction
Received 3 August 2017
Accepted for publication 28 August 2017
Published 14 September 2017 Volume 2017:11 Pages 1677—1682
DOI https://doi.org/10.2147/OPTH.S148167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shiro Amano, Kenji Inoue
Inouye Eye Hospital, Chiyoda-ku, Tokyo, Japan
Purpose: To prospectively evaluate the effect of topical diquafosol sodium on eyes with dry eye disease (DED) and meibomian gland dysfunction (MGD).
Patients and methods: The subjects were consecutive patients diagnosed with both DED and MGD at Inouye Eye Hospital between March and September of 2016. The subjects were administered topical 3% diquafosol sodium ophthalmic solution six times a day for 3 months. At each study visit, subjects underwent slit-lamp examination and completed MGD symptoms and dry eye-related quality of life score (DEQS) questionnaires. Meibum quality (meibum score) and meibomian gland loss (meiboscore) were evaluated. Tear lipid layer thickness was measured in both eyes with an ocular surface interferometer immediately after clinic arrival and 20 minutes after instillation of one drop of topical diquafosol.
Results: Thirteen patients (3 men, 10 women) with a mean age of 69.5±8.3 years completed the 3-month study. The number of telangiectasia and plugged meibomian gland orifices significantly decreased from baseline after 1 month of diquafosol use. The meibum score and the meiboscore significantly decreased from baseline at 3 months. Also, the lipid layer thickness was greater after diquafosol administration than before administration at baseline and 1, 2, and 3 months by 12.2, 11.5, 9.5, and 17.0 nm, respectively, but this difference was only significant at 3 months (p=0.039). The DEQS ocular symptom (p=0.065) and MGD questionnaire (p=0.081) scores tended to be lower than baseline at 3 months.
Conclusion: Diquafosol sodium ophthalmic solution improves DED- and MGD-related signs in eyes with MGD.
Keywords: diquafosol, meibomian gland dysfunction, dry eye
Introduction
Diquafosol is a P2Y2 receptor agonist that activates P2Y2 receptors. When used on the ocular surface, rehydration occurs through increased fluid secretion from conjunctival epithelial cells (via accessory lacrimal fluid pump activation) and increased mucin secretion from conjunctival goblet cells.1–5 As a result, topical diquafosol solutions have been used to treat dry eye disease.6,7 Expression of the P2Y2 receptor occurs in ocular surface tissue, including the corneal epithelium, conjunctival epithelium, lacrimal gland ductal epithelium, meibomian gland sebaceous cells, and meibomian gland ductal cells.8,9 Therefore, diquafosol is expected to have at least some effect on the meibomian glands. We previously demonstrated the beneficial effects of topical diquafosol sodium on the ocular surface in subjects with meibomian gland dysfunction (MGD), including decreases in ocular symptoms, lid margin abnormalities, and meibum grade and increases in tear film break-up time (BUT) and meibomian gland area.10 However, the duration of diquafosol use widely varied (4–16 months), likely reducing the reliability of our findings. This study was performed to resolve this issue and to prospectively evaluate the effect of topical diquafosol sodium use on the signs and symptoms of dry eye disease in eyes with MGD.
Patients and methods
This study was reveiwed and approved by the institutional review board of Inouye Eye Hospital (Tokyo, Japan). It is registered with the University Hospital Medical Information Network in Japan (number UMIN000018510). The entire study conduct adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all study participants before any study examinations were performed.
Study subjects
Consecutive adult patients diagnosed with both dry eye disease and MGD at Inouye Eye Hospital between March and September 2016 were considered for enrollment. Subjects were excluded from participation if any of the following was found: active ocular infection, ocular inflammation, or history of ocular surgery within 3 months of enrollment.
Diagnosis of MGD
An MGD diagnosis was made using the diagnostic criteria proposed by the MGD Working Group in Japan.11 Briefly, an MGD diagnosis was given when lid margin abnormalities and meibomian gland occlusion signs were both present. Lid margin abnormalities were considered to be present when at least two of the following were present in at least one eye: ≥2 telangiectasias, lid margin irregularity (notching), and mucocutaneous junction shifts. Meibomian gland occlusion was considered to be present when at least one eye had meibum secretions that were reduced when moderate pressure was applied with the thumb to the middle-third region of the upper eyelid and ≥2 gland orifices appeared to be plugged.
Diagnosis of dry eye disease
Dry eye disease was diagnosed using standard diagnostic criteria used in Japan.12 Briefly, a patient was given a definitive dry eye disease diagnosis when dry eye symptoms, a tear film abnormality (BUT ≤5 seconds or a Schirmer I test value of ≤5 mm), and keratoconjunctival epithelial disorders (fluorescein staining score ≥3 [maximum score =9]) were present. When two of the three criteria were met, the patient was given a diagnosis of probable dry eye disease.
Treatment with diquafosol sodium ophthalmic solution
All patients underwent topical administration of 3% diquafosol sodium ophthalmic solution (Diquas® ophthalmic solution 3%; Santen Pharmaceutical Co., Ltd., Osaka, Japan). Subjects were instructed to use one drop of topical diquafosol six times day for 3 months.
Study examinations
Examinations were performed before and 1, 2, and 3 months after initiating diquafosol treatment in the order listed. Subjects were asked not to use eye drops for at least 2 hours before study visits to minimize the influence of eye drops on the tear lipid layer thickness (LLT). Immediately after the subjects arrived at our clinic, LLT was measured using the LipiView ocular surface interferometer (TearScience, Morrisville, NC, USA).13,14 One drop of diquafosol was then instilled in both eyes and LLT was measured again 20 minutes later.
Subjects completed a symptoms questionnaire (MGD questionnaire), which included rating the presence of 11 ocular symptoms using the following scoring system: 0= never, 1= rarely, 2= sometimes, 3= often, and 4= all of the time. The rated symptoms included discomfort, pressure sensation, fatigue, discharge, stickiness, itching, heavy sensation, dryness, foreign body sensation, burning sensation, and redness. All 11 symptom scores were totaled to calculate the MGD symptom score. Subjects also completed a questionnaire to determine the dry eye-related quality of life score (DEQS).15 Medication use compliance was evaluated as 100%, 75%–99%, 25%–74%, or <25%.
A slit-lamp examination was performed to thoroughly examine the upper and lower eyelids for lid margin abnormalities (eg, irregular lid margin, telangiectasia, plugged meibomian gland orifices, and mucocutaneous junction shift). Telangiectasias needed to occupy at least one half of the lid margin width to be considered present. Mucocutaneous junction shifts were evaluated based on the location of the Marx line after fluorescein instillation.16,17 When all or part of the Marx line touched the meibomian gland orifices in the upper or lower eyelid, a mucocutaneous junction shift was considered to be present.
The ocular surface was evaluated by measuring the tear BUT and corneal and conjunctival fluorescein staining. Tear BUT was measured using a slit-lamp after of fluorescein instillation into the conjunctival sac. The time from normal blinking to the first appearance of a break in the tear film was measured three times using a stopwatch. The mean of the three measurements was calculated and recorded as the tear BUT. To obtain the fluorescein staining score, the ocular surface was divided into the nasal conjunctival, corneal, and temporal conjunctival sections. Each section was graded on a severity scale of 0–3 (0= no staining, 3= severe staining). Section gradings were summed to obtain the overall epithelial damage score (maximum of 9).18,19
Meibomian gland secretions and orifice plugging were then examined. Moderate pressure was applied to the middle-third region of the upper eyelid using the thumb. Meibum appearance and the ease at which it was expressed were considered when grading meibum (meibum score) using the following semi-quantitative grading system: grade 0= clear meibum that is easily expressed, grade 1= cloudy meibum that could be expressed with mild pressure, grade 2= cloudy meibum that could only be expressed after more than moderate pressure was applied, and grade 3= no meibum expression, even with hard pressure.20 Meibomian gland loss was evaluated using the following meiboscore definitions: 0= no loss, 1= lost gland area accounts for less than one-third of the total meibomian gland area, 2= lost area was between one-third and two-thirds of the total meibomian gland area, and 3= lost area over two-thirds or more of the total meibomian gland area.21 Meibomian gland area was measured using a mobile pen-shaped infrared meibography device (Meibom Pen; JFC Sales Plan Co. Ltd., Tokyo, Japan).22 A standard Schirmer I test was performed 5 minutes after administering topical anaesthesia (0.4% oxybuprocaine hydrochloride; Santen Pharmaceutical Co. Ltd.).
Statistical analyses
Data from the right eye of all subjects were used in analyses because the right eye qualified for the study in all cases. Baseline and posttreatment values of continuous variables were compared using a mixed-effects model with eyes (right) or subjects as a random effect. A generalized estimating equation model or McNemar test was used for binominal variables. Changes from baseline in LLT values in each pre- and post-diquafosol application and differences between pre- and post-diquafosol dosing at each visit were evaluated using a mixed-effects model with eyes (right) as a random effect.
Results
Study subjects
Thirteen subjects were ultimately included in the study analyses. Fourteen subjects were enrolled in this study. However, one subject reported pain immediately after the first instillation of 3% diquafosol sodium ophthalmic solution. Therefore, this subject stopped using the medication and withdrew from the study. Fortunately, the pain quickly resolved and this subject experienced no further adverse events.
The 13 subjects (3 men, 10 women) included in the analyses had a mean age of 69.5±8.3 years (range: 54–83 years). One subject missed the 1-month follow-up visit, and 1 subject refused to undergo further Schirmer tests after the 1-month visit. Hence, the number of subjects was 13 at baseline, 2 and 3 months, and 12 at 1 month. For Schirmer tests, the number of subjects used in the analyses was 13 at pretreatment, 12 at 2 and 3 months, and 11 at 1 month. All subjects had satisfactory medication compliance at each study visit, reporting a topical diquafosol eye drop use of at least 75%. None of the 13 subjects used any ophthalmic solutions other than 3% diquafosol sodium ophthalmic solution during the study. None of the subjects performed self-care of MGD, such as lid hygiene and warm compression, during the study.
Effect of diquafosol on the ocular surface
Table 1 shows the changes over time in ocular surface parameters. The number of telangiectasia and plugged meibomian gland orifices in each eye was significantly lower at 1, 2, and 3 months than at baseline. Also, the meibum score and the total meiboscore were significantly lower at 3 months than at baseline. The Schirmer test results were significantly higher at 3 months than at baseline. Tear BUT also significantly increased and fluorescein staining score significantly decreased 1 month after initiating diquafosol use.
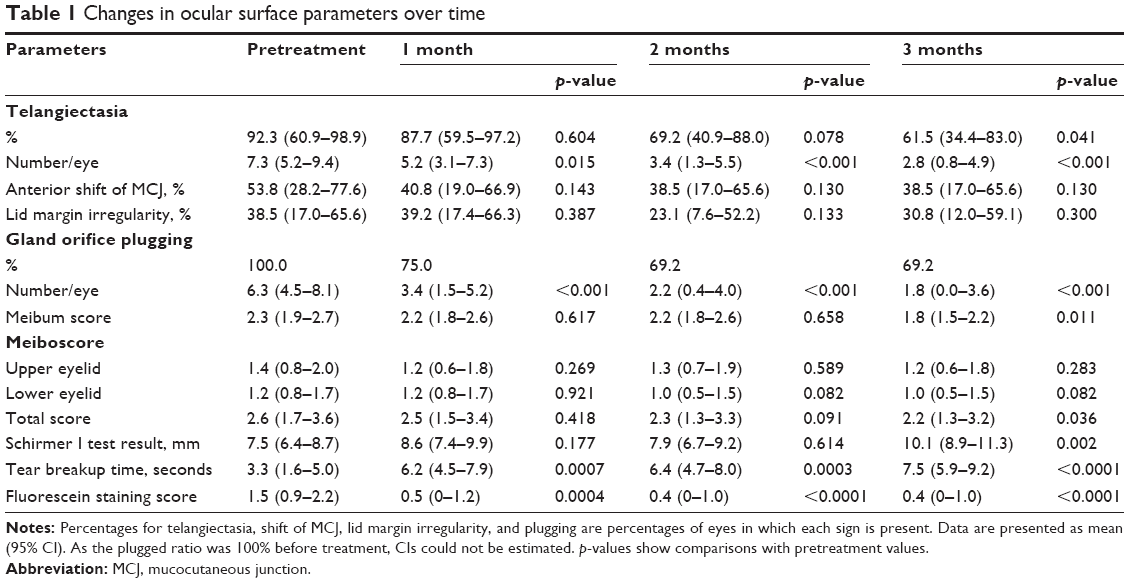 | Table 1 Changes in ocular surface parameters over time |
Table 2 summarizes the LLT measurements. Briefly, LLT measured immediately after clinic arrival was not significantly different from baseline at 1, 2, or 3 months. This was also true of LLT measured 20 minutes after diquafosol administration. At each time point, the second LLT measurement was higher than the first LLT measurement, but this difference (17 nm) was only significant at 3 months (p=0.039).
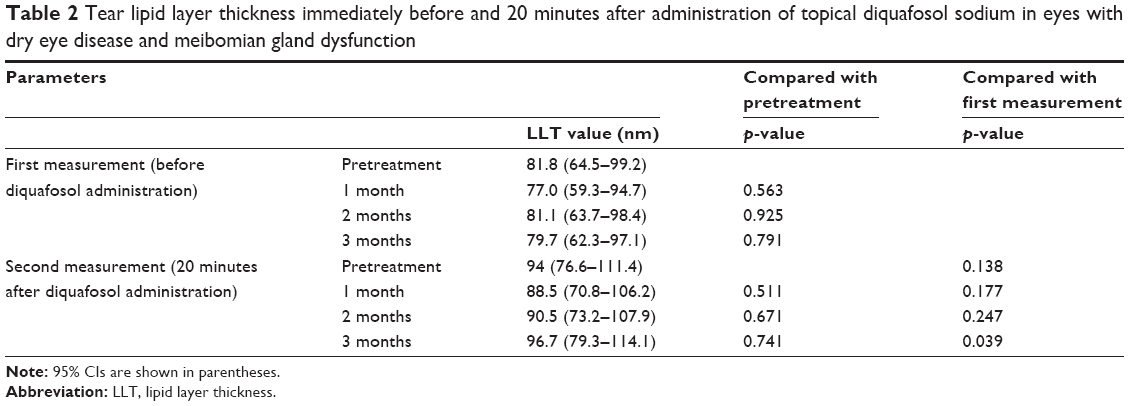 | Table 2 Tear lipid layer thickness immediately before and 20 minutes after administration of topical diquafosol sodium in eyes with dry eye disease and meibomian gland dysfunction |
Effect of diquafosol on subject symptoms
Subject symptoms associated with dry eye disease and MGD were evaluated at each study visit (Table 3). The DEQS ocular symptom (p=0.065) and MGD (p=0.081) scores were both marginally, but not significantly, lower at 3 months than at baseline.
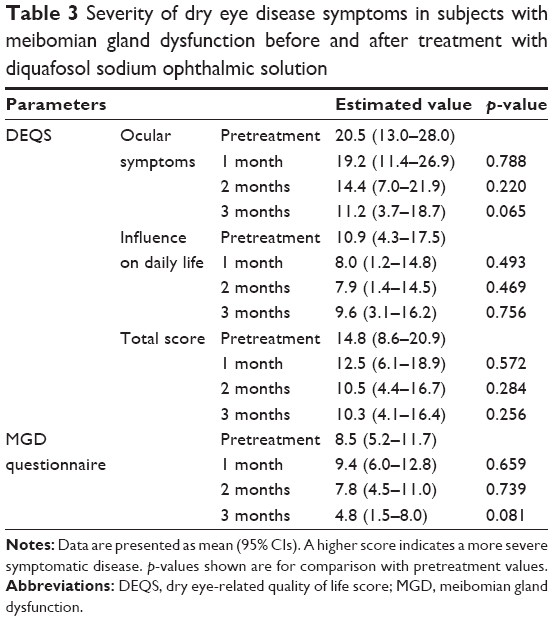 | Table 3 Severity of dry eye disease symptoms in subjects with meibomian gland dysfunction before and after treatment with diquafosol sodium ophthalmic solution |
Discussion
This study examined the effect of 3% diquafosol sodium ophthalmic solution on the signs and symptoms of dry eye disease in eyes with MGD. The number of telangiectasia and plugged meibomian gland orifices in each eye significantly decreased after 1 month of diquafosol use. Also, the meibum score and the meiboscore were significantly lower than baseline at 3 months. The MGD questionnaire score was also lower than baseline at 3 months, but this change was only marginally significant. These results suggest that topical diquafosol sodium improves pathologic ocular surface changes and symptoms associated with MGD. As gene expression of the P2Y2 receptor has been observed in meibomian gland sebaceous and ductal cells,8,9 it is likely that these improvements were directly related to the effect of diquafosol on meibomian glands. However, it has not been confirmed that topically applied diquafosol penetrates into the meibomian glands, and this should be examined in future studies.
Schirmer I test scores significantly increased after 3 months of topical diquafosol use. Also, at 1 month, tear BUT had significantly increased over baseline and the fluorescein staining score had significantly decreased from baseline. Furthermore, the DEQS ocular symptoms score consistently decreased in each subject, but, when averaged, this change was only marginally significant. These improvements in dry eye-related signs and symptoms agree with the findings of previous studies that reported a high efficacy of topical diquafosol sodium when used to treat dry eye disease.6,7 It is thought that diquafosol stimulates water secretion from the conjunctival epithelial cells and mucin secretion from the conjunctival goblet cells via P2Y2 receptor activation. As some symptoms included in the MGD questionnaire are related to dry eye disease, improvements in MGD questionnaire score may be attributed to improvements in meibomian gland function and enhancement of aqueous tear and mucin secretion from conjunctival cells.
We measured LLT when subjects arrived at our clinic and 20 minutes after instillation of topical diquafosol. A previous study23 showed that LLT was significantly increased 15 minutes after the instillation of 3% diquafosol in healthy human eyes and the increase was maintained for 60 minutes. Hence, we thought 20 minutes is enough to observe the effect of diquafosol on LLT. The second LLT measurement was ~10 nm higher than the first at baseline and 1 and 2 months and 17 nm higher at 3 months (p=0.039). This suggests that a single instillation of diquafosol increases lipid secretion from the meibomian glands, and that using topical diquafosol for 3 months enhances lipid secretion from the meibomian glands in subjects with MGD. These results are consistent with the simultaneous decrease in the number of plugged meibomian gland orifices, which was significantly lower at 1 month than at baseline. These findings, together with the fact that LLT is significantly associated with MGD severity and meibomian gland dropout grade,13,14 suggest that topical diquafosol use over 3 months somewhat restores meibomian gland lipid secretion in patients with MGD.
A recent study by Kam et al reported that uridine-5′-triphosphate (UTP), a P2Y2 receptor agonist, had no effect on immortalized human meibomian gland epithelial cells.24 The authors also concluded that if diquafosol does influence human meibomian glands, it may be that ductal, not acinar, epithelial cells are affected. In contrast, Wen et al found that P2Y2 receptor agonists enhance lipid production in primary cultured rabbit meibocytes.25 These discrepant results may have resulted from differences in species and/or culture conditions. Also, UTP easily degrades in aqueous solutions, making it necessary to use UTP immediately after it is dissolved in water.5,26 In contrast, diquafosol is stable when dissolved in water.5,26 As Kam et al did not mention whether or not UTP solutions were immediately used,24 we do know for certain whether or not their results are applicable to the actions of diquafosol on meibomian gland acinar cells. Either way, our results suggest that topical diquafosol is beneficial to meibomian glands. Further studies are needed to elucidate which meibomian gland cell types (acinar and/or ductal) are affected by diquafosol.
One of our subjects withdrew from the study because of ocular pain that began immediately after the first instillation of diquafosol sodium. Ocular pain and discomfort were previously observed in a Japanese Phase II clinical trial,7 where one subject (1.0%) reported eye pain and seven subjects (7.3%) reported ocular irritation after using 1% diquafosol. Furthermore, 4 subjects (4.2%) reported eye pain and 12 subjects (12.5%) reported ocular irritation after using 3% diquafosol. However, no serious treatment-related adverse events occurred in any subject. In agreement with this, no adverse events occurred in any of our study subjects during the 3-month follow-up period, including the subject who experienced ocular pain. Therefore, our study further supports the safety of using diquafosol sodium ophthalmic solution to treat MGD.
Our study was limited in that it was an uncontrolled study (no placebo group), had a relatively small number of subjects, and had a short follow-up period. Future randomized, placebo-controlled studies with a larger number of participants and a longer follow-up period are needed to confirm the efficacy of topical diquafosol sodium for treating the signs and symptoms in patients with MGD. Another limitation was that the slit-lamp diagnostic criteria, including meibum evaluations, were subjective. These parameters require standardized grading methods or objective measures to allow more accurate comparisons within and between studies.16
In conclusion, diquafosol sodium ophthalmic solution improves MGD and dry eye-related signs and symptoms in subjects with MGD. Also, the use of topical diquafosol sodium for at least 3 months likely increases lipid secretions from the meibomian glands in patients with MGD.
Acknowledgments
We would like to acknowledge Dr Toshihito Furukawa (Biostatistical Research Co., Ltd., Tokyo, Japan) for completing the statistical analyses and Editage (www.editage.jp) for English language editing services. This study was partly supported by a grant from Santen Pharmaceutical Co. Ltd. (Osaka, Japan).
Disclosure
Dr Amano reports a grant and personal fees from Santen Pharmaceutical. Dr Inoue reports personal fees from Santen Pharmaceutical. The authors report no other conflicts of interest in this work.
References
Vallejo CG, Lobaton CD, Quintanilla M, Sillero A, Sillero MA. Dinucleosidasetetraphosphatase in rat liver and Artemia salina. Biochim Biophys Acta. 1976;438(1):304–309. | ||
Hosoya KI, Ueda H, Kim KJ, Lee VH. Nucleotide stimulation of Cl(−) secretion in the pigmented rabbit conjunctiva. J Pharmacol Exp Ther. 1999;291(1):53–59. | ||
Jumblatt JE, Jumblatt MM. Regulation of ocular mucin secretion by P2Y2 nucleotide receptors in rabbit and human conjunctiva. Exp Eye Res. 1998;67(3):341–346. | ||
Murakami T, Fujihara T, Horibe Y, Nakamura M. Diquafosol elicits increases in net Cl− transport through P2Y2 receptor stimulation in rabbit conjunctiva. Ophthalmic Res. 2004;36(2):89–93. | ||
Nichols KK, Yerxa B, Kellerman DJ. Diquafosol tetrasodium: a novel dry eye therapy. Expert Opin Investig Drugs. 2004;13(1):47–54. | ||
Tauber J, Davitt WF, Bokosky JE, et al. Double-masked, placebo-controlled safety and efficacy trial of diquafosol (INS365) ophthalmic solution for the treatment of dry eye. Cornea. 2004;23(8):784–792. | ||
Matsumoto Y, Ohashi Y, Watanabe H, Tsubota K, et al; Diquafosol Ophthalmic Solution Phase 2 Study Group. Diquafosol ophthalmic solution phase 2 study group. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial. Ophthalmology. 2012;119(10):1954–1960. | ||
Cowlen MS, Zhang VZ, Warnock L, Moyer CF, Peterson WM, Yerxa BR. Localization of ocular P2Y2 receptor gene expression by in situ hybridization. Exp Eye Res. 2003;77(1):77–84. | ||
Tanioka H, Kuriki Y, Sakamoto A, Katsuta O, Kawazu K, Nakamura M. Expression of the P2Y2 receptor on the rat ocular surface during a 1-year rearing period. Jpn J Ophthalmol. 2014;58(6):515–521. | ||
Arita R, Suehiro J, Haraguchi T, et al. Topical diquafosol for patients with obstructive meibomian gland dysfunction. Br J Ophthalmol. 2013;97(6):725–729. | ||
Amano S, Inoue K. Clinic-based study on meibomian gland dysfunction in Japan. Invest Ophthalmol Vis Sci. 2017;58(2):1283–1287. | ||
Shimazaki J, Tsubota K, Kinoshita S, et al. [Definition and diagnosis of dry eye 2006]. Atarasii Ganka. 2007;24(2):181–184. Japanese. | ||
Finis D, Pischel N, Schrader S, Geerling G. Evaluation of lipid layer thickness measurement of the tear film as a diagnostic tool for Meibomian gland dysfunction. Cornea. 2013;32(12):1549–1553. | ||
Ji YW, Lee J, Lee H, Seo KY, Kim EK, Kim TI. Automated measurement of tear film dynamics and lipid layer thickness for assessment of non-Sjögren dry eye syndrome with meibomian gland dysfunction. Cornea. 2017;36(2):176–182. | ||
Sakane Y, Yamaguchi M, Yokoi N, et al. Development and validation of the dry eye-related quality-of-life score questionnaire. JAMA Ophthalmol. 2013;131(10):1331–1318. | ||
Arita R, Minoura I, Morishige N, et al. Development of definitive and reliable grading scales for meibomian gland dysfunction. Am J Ophthalmol. 2016;169:125–137. | ||
Yamaguchi M, Kutsuna M, Uno T, Zheng X, Kodama T, Ohashi Y. Marx line: fluorescein staining line on the inner lid as indicator of meibomian gland function. Am J Ophthalmol. 2006;141(4):669–675. | ||
Yokoi N, Uchino M, Uchino Y, et al. Importance of tear film instability in dry eye disease in office workers using visual display terminals: the Osaka study. Am J Ophthalmol. 2015;159(4):748–754. | ||
van Bijsterveld OP. Diagnostic tests in the Sicca syndrome. Arch Ophthalmol. 1969;82(1):10–14. | ||
Shimazaki J, Goto E, Ono M, Shimmura S, Tsubota K. Meibomian gland dysfunction in patients with Sjogren syndrome. Ophthalmology. 1998;105(8):1485–1488. | ||
Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. | ||
Shirakawa R, Arita R, Amano S. Meibomian gland morphology in Japanese infants, children, and adults observed using a mobile pen-shaped infrared meibography device. Am J Ophthalmol. 2013;155(6):1099–1103. | ||
Fukuoka S, Arita R. Increase in tear film lipid layer thickness after instillation of 3% diquafosol ophthalmic solution in healthy human eyes. Ocul Surf. 2017;S1542–0124(16):30288–30289. | ||
Kam WR, Liu Y, Ding J, Sullivan DA. Do cyclosporine A, an IL-1 receptor antagonist, uridine triphosphate, rebamipide, and/or bimatoprost regulate human meibomian gland epithelial cells? Invest Ophthalmol Vis Sci. 2016;57(10):4287–4494. | ||
Wen Q, Li Y, Kuang K, Yerxa B, Fischbarg J. Effects of P2Y2 agonists on lipid secretion by cultured rabbit meibocytes. Invest Ophthalmol Vis Sci. 2002;43(13):3146. | ||
Yerxa BR, Sabater JR, Davis CW, et al. Pharmacology of INS37217 [P1-(uridine 5′)-P4-(2′-deoxycytidine 5′)tetraphosphate, tetrasodium salt], a next-generation P2Y2 receptor agonist for the treatment of cystic fibrosis. J Pharmacol Exp Ther. 2002;302(3):871–880. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.