")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Effect of Thoracic Kyphosis and Lumbar Lordosis on the Distribution of Ground Reaction Forces on the Feet
Authors Żurawski A, Śliwiński Z, Suliga E, Śliwiński G, Wypych Ż , Kiebzak W
Received 4 January 2022
Accepted for publication 27 April 2022
Published 16 May 2022 Volume 2022:14 Pages 187—197
DOI https://doi.org/10.2147/ORR.S344972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Arkadiusz Żurawski,1 Zbigniew Śliwiński,1 Edyta Suliga,1 Grzegorz Śliwiński,2 Żaneta Wypych,1 Wojciech Kiebzak1
1Collegium Medicum, Jan Kochanowski University, Kielce, Poland; 2Engineering, Technical University, Dresden, Germany
Correspondence: Żaneta Wypych, Tel +48 728373970, Email [email protected]
Introduction: In clinical practice, foot load receptors are very important in shaping the correct vertical posture and optimal equilibrium reactions. They are so important that stimulating them gives measurable effects in improving both balance and posture. Plantar pressure distribution is an important parameter that provides information on changes in a person’s posture, also during gait.
Aim: The aim of the work is to assess the effect of thoracic kyphosis and lumbar lordosis on the distribution of ground reaction forces on the feet.
Materials and Methods: A total of 211 subjects aged 8– 12 were examined. Body posture and distribution of ground reaction forces on the feet were assessed using the following parameters: thoracic kyphosis angle, lumbar lordosis angle, maximum pressure (static), average pressure (static), foot surface, distribution of foot pressure, maximum pressure (dynamic), time load (dynamic). DIERS formetric and DIERS pedoscan methods were used to measure the parameters.
Results: The level of the kyphosis angle correlated positively with the percentage distribution of forefoot load in static conditions. The level of lordosis angle correlated positively with the foot surface and forefoot load. Positive correlation of the lordosis angle is also related to its connection with the difference in leg load during gait. A broader cause and effect view of body posture defects and the distribution of ground reaction forces on the feet can affect a more complete assessment of the correlation between these variables, contributing to more effective treatment of any disorders of the described phenomena.
Conclusion: The size of thoracic kyphosis and lumbar lordosis affects the distribution of ground reaction forces on the feet. The effect of lumbar lordosis has a linear value in relation to percentage distribution of forefoot and heel loads.
Keywords: posture, spine, pressure feet, foot load, postural disorders
Introduction
Posture is a standard, individual arrangement of respective body parts in space and against each other in a dynamic and static state, it corresponds with biomechanical principles of the functioning of a human body and is determined by physiological curves which depend on muscle strength and mass of various body parts.1 The right proportions of thoracic kyphosis angle and lumbar lordosis, which determine keeping the correct size of the remaining angular parameters of the spine, are the main components of correct posture.2 Correct body posture allows you to keep your eyes directed horizontally – in accordance with otoscopy, which implies that the human body adapts to the surrounding conditions so as to maintain eyesight in a horizontal plane and limit the movement of the center of gravity to the support plane.3,4 In the postural development are two critical periods: the start of schooling of a child (aged 6–7 years) and the second occurs during puberty. What is more at ages 4–6 years the postural stability is connected with somatosensory and visual input and plantar surfaces.5
Shifts of the body figure from the axis cause an asymmetrical load on the limbs, which affects the occurrence of disproportion of postural muscle tension, and thus the shift of the center of gravity.6 Furthermore, the same impact is connected with obesity or overweight.7 It is assumed that the load on both limbs should be 50% for the left and right sides, while the load distribution for each foot should be as follows: heels 60%, mid-foot 8%, forefoot 28%, toes 4%.8 A change in these proportions may indicate the presence of dysfunction in the feet.
Static and dynamic foot shape disorders are one of the most commonly diagnosed defects in pediatric practice. Foot deformity is one of the most common disorders observed in clinical practice (approximately 70–80% of the population has this type of disorder).4,8 Diagnosis of foot dysfunction must go beyond clinical and visual observation. There are numerous methods for assessing foot shape, eg radiology, contour graphics, anthropometry, strength platforms, and pedobarographs. Most techniques are labor-intensive, time-consuming and insufficient to gather reliable data.9 The pedobarographic method, which was used for the purpose of this study, shows changes in the distribution of plantar pressure, along with an increase and decrease of pressure in some areas of the foot. Plantar pressure distribution is an important parameter that provides information about changes in human posture, also during gait.9
In clinical practice, the importance of foot load receptors in shaping the correct vertical body posture and optimal equilibrium reactions is very important. It is so important that their stimulation gives measurable effects in improving both balance and figure.10
It is also interesting that the body posture is inextricably related to ergonomics of the gait, and its symmetry is necessary for the proper movement of the center of gravity while moving.11 Shifts in the center of gravity are registered by pressure receptors on the feet, and setting reactions aimed at maintaining balance occur by reflex.12 Winter argues that despite the involvement of many muscle groups of the limbs and torso, the process of maintaining balance during locomotion occurs without the involvement of the vestibular system.11
Aim
The aim of the work is to assess the effect of thoracic kyphosis and lumbar lordosis on the distribution of ground reaction forces on the feet.
Materials and Methods
Subjects of the Study
The study included 211 people in the 8–12 age range. In this group, 53% were girls (N = 112) and 46.92% were boys (N = 99) (Table 1).
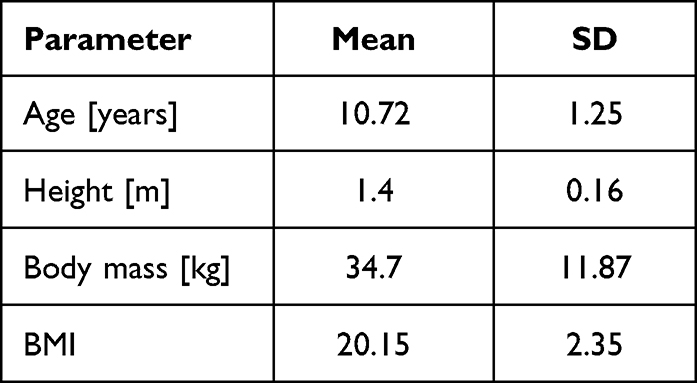 |
Table 1 Morphological Parameters of Studied Children |
The presented study protocol was approved by the Bioethics Committee of the Faculty of Medicine and Health Sciences of the Jan Kochanowski University in Kielce – approval No. 1/2016, issued on 15/01/2016.
All participants gave their written consent to participate in the study. The research was conducted in accordance with WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects.
Inclusion Criteria
- Age 8–12
- Good general health (≤2 according to WHO/ECOG – Eastern Cooperative Oncology Group – it describes a patient’s level of functioning in daily and physical activity or their ability to care for themselves).
- Declared legal guardian’s consent for participation in the study.
Exclusion Criteria
- Occurrence of concomitant disorders which may affect body axis disturbance eg Scheuermann's disease, genetic diseases such as Beckwith-Wiedemann Syndrome or metabolic diseases
= deformities in the lower extremities
- BMI below 10 and above 90 percentile.
Participation in the study was voluntary, combined with ensuring anonymity in accordance with Ustawa o ochronie danych osobowych z dnia 29.08.1997 r. (Dz. U. Nr 133 poz. 883. RP) [the Personal Data Protection Act of 29.08.1997 (Journal of Laws of the Republic of Poland No. 133, item 883)].
Study Method
Body posture was assessed in static conditions in a habitual standing position. The subjects were positioned with their back to the camera with eyes facing straight ahead. At the same time, along with the assessment of body posture, the ground reaction forces on the feet were measured in a static position. The distribution of ground reaction forces on the feet during gait was also assessed.
- Body posture was assessed with the DIERS Formetric 4D system. The DIERS formetric is a light-optical scanning method based on Video-Raster-Stereography (VRS). Accordingly, the system consists of a light projector which projects a line grid on the back of the patient which is recorded by an imaging unit. A computer software analyzes the line curvature and generates from it – by means of the method of the Photogrammetrie – a three-dimensional model of the surface (Figure 1).
- The measurement of the ground reaction forces on the feet in a static position was made with the DIERS Pedoscan correlated with the DIERS Formetric system. Diers Pedoscan is allowed to evaluate the foot pressure distribution while standing (Figure 2).
- The measurement of the ground reaction forces on the feet in dynamic conditions was made with the DIERS Pedogait, which allows the foot pressure reaction forces while walking (Figure 3).
 |
Figure 1 Diers formetric 4D system (consent from Diers International GMBH). |
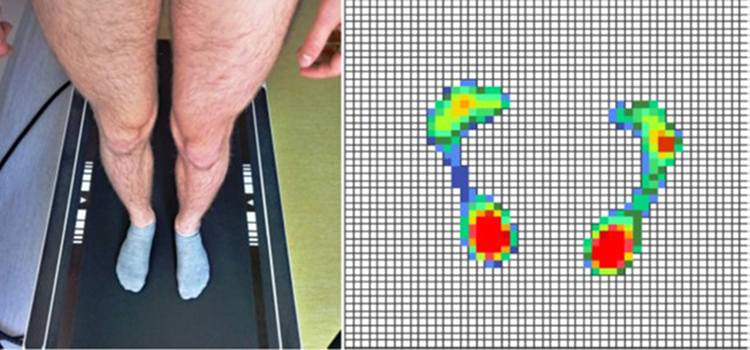 |
Figure 2 Disposure the feet in static position – Diers pedoscan. |
 |
Figure 3 Treadmill for examining – Diers pedogait. |
The following parameters were assessed:
- Thoracic kyphosis angle – parameter measured in degrees [°] is the angle measured between C7 Th12.
- Lumbar lordosis angle – parameter measured in degrees [°] is the angle measured between Th12 and L4.
- Maximum pressure (static) - a parameter calculated in N/cm2 illustrating the force of the ground pressure on the feet in the spot where it is the biggest in a standing position. The parameter was calculated for the left and right foot separately.
- Average pressure (static) - a parameter calculated in N/cm2, illustrating the average strength of the ground’s impact on the entire foot surface in a standing position. The parameter was calculated for the left and right foot separately.
- Foot surface - a parameter calculated in cm2 denoting the size of the area on which the foot is in contact with the ground in a standing position.
- Foot pressure distribution - a parameter calculated in percentage [%], illustrating the ratio of forefoot and heel load. It was calculated for each foot separately, as well as for both feet together in a standing position.
- Maximum pressure (dynamic) - a parameter calculated in Newtons [N], which is the force of the ground reaction on the feet when it is the biggest in the whole gait cycle. The parameter was calculated for the left and right foot separately.
- Load time (dynamic) – Parameter calculated in seconds [sec], denoting the average time in which a given foot was in contact with the ground during the gait cycle. The average is calculated from all gait cycles the patient has covered over a 16-metre distance. The parameter was calculated for the left and right foot separately; the difference between the left and right foot was also calculated.
Statistical Analysis
Statistical analyses were performed with the IBM SPSS Statistics 23. Basic descriptive statistics analysis was performed.
To assess the normality of the distribution of variables, the nonparametric Kolmogorov–Smirnov (K-S) test was used.
To determine the relationship between the studied variables, Spearman’s ρrank correlation analysis was used.
The level of significance was p <0.05.
Results
Basic descriptive statistics of tested quantitative variables were calculated (Table 2). The results of the measurements of individual respondents are contained in the directories in Supplementary Tables 1 and 2.
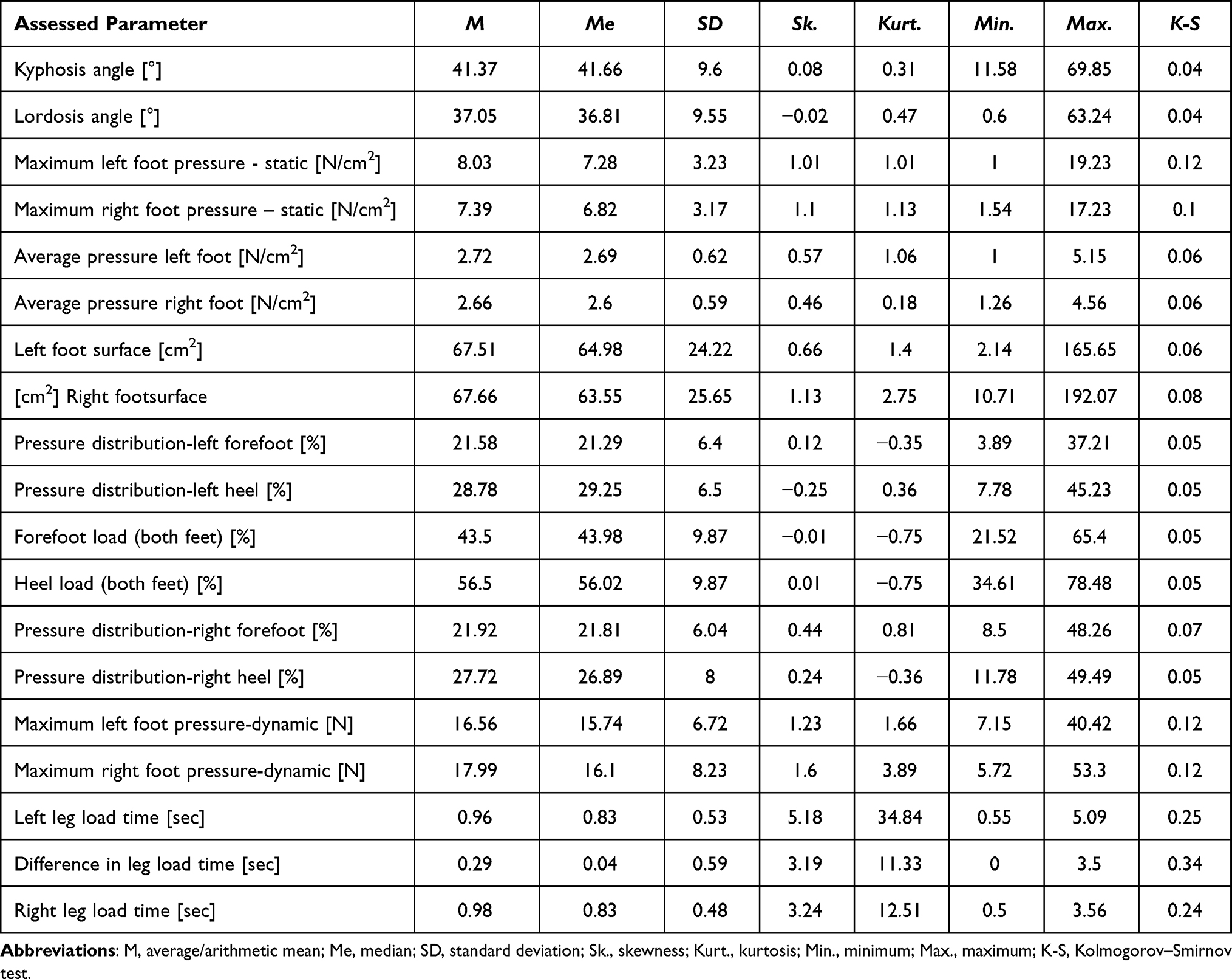 |
Table 2 Basic Descriptive Statistics of Studied Variables |
Correlations between the kyphosis angle and the distribution of ground reaction forces on the feet were calculated in static and dynamic conditions. A series of Spearman’sρ rank correlation analyses were performed (Table 3).
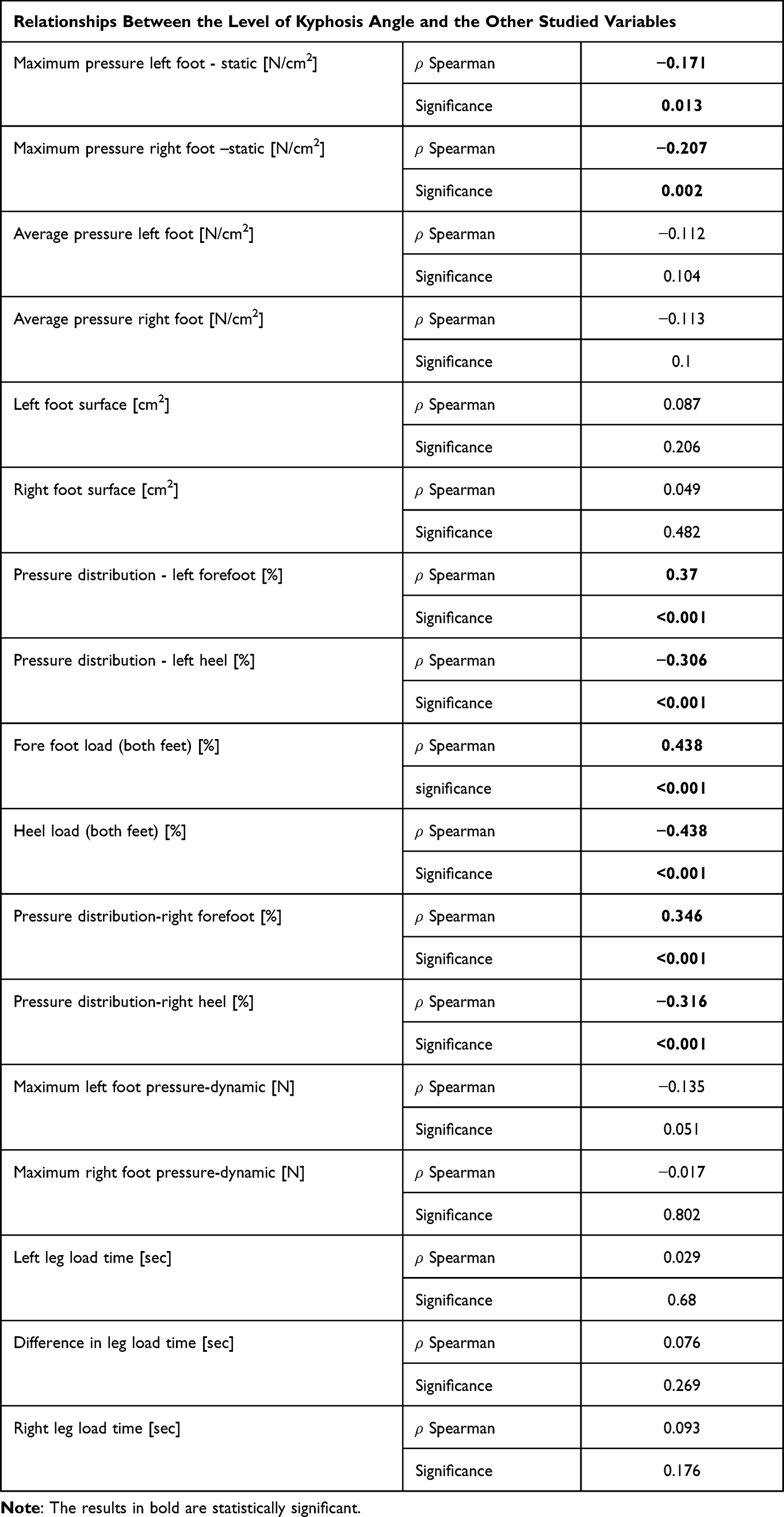 |
Table 3 Relationships Between the Level of Kyphosis Angle and the Other Studied Variables |
The degree of kyphosis angle correlated positively with the percentage distribution of left and right forefoot pressure (0.37 left foot, 0.346 right foot) under static conditions, and forefeet loads put together (0.438) under static conditions. Connections of the kyphosis angle with the maximum left (−0.17) and right (−0.207) foot pressure, heel load (−0.306 left foot, −0.316 right foot, both feet together −0.438) were negative. Correlations between the lordosis angle and the distribution of ground reaction forces on the feet under static and dynamic conditions were calculated. A series of Spearman ρ rank correlation analyses were performed (Table 4).
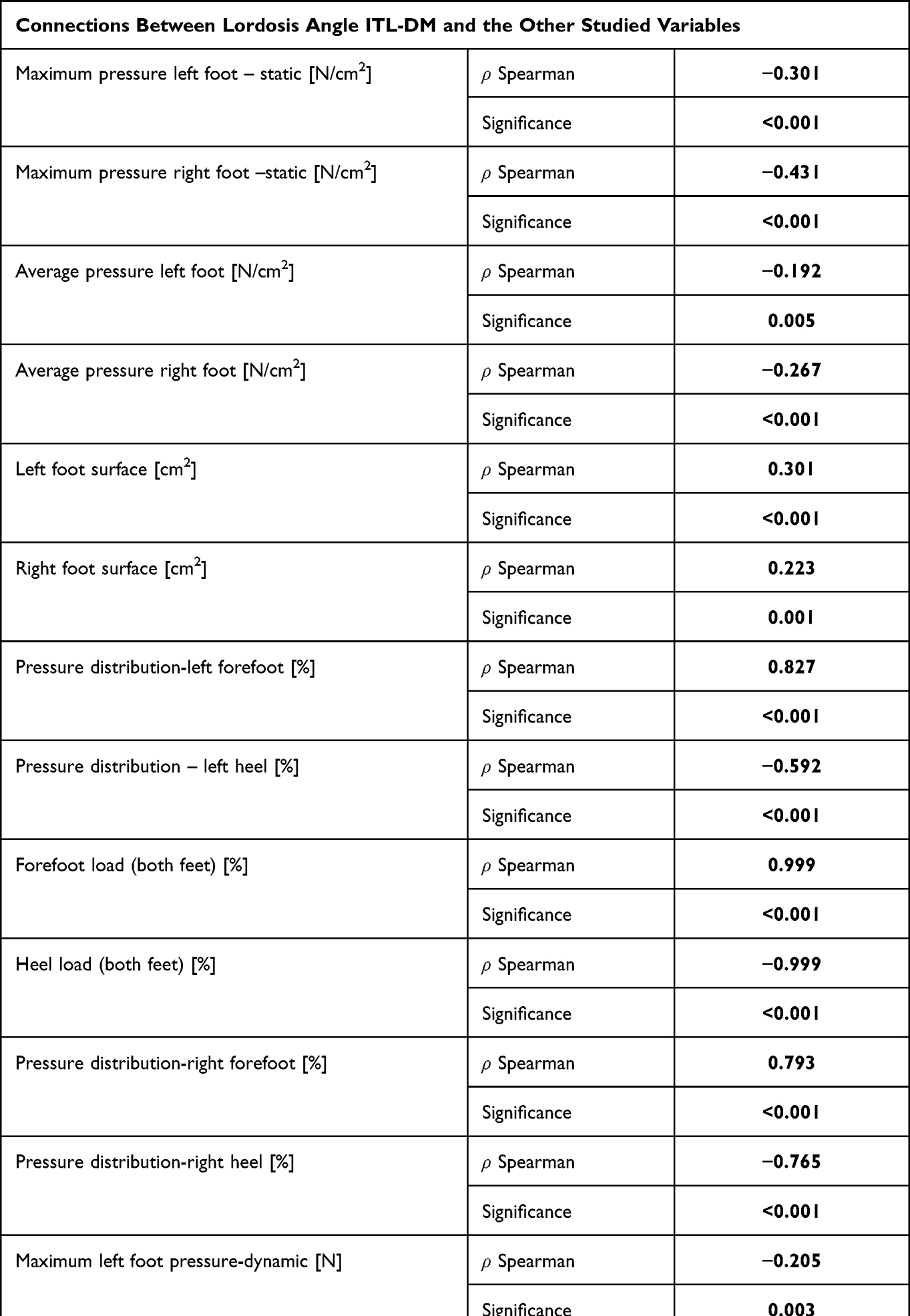 |
Table 4 Relationship Between Lordosis Angle and the Other Studied Variables |
As can be seen in Table 4, numerous statistically significant correlations were noted. The degree of lordosis angle correlated positively with the surface of the left (0.301) and right (0.223) foot, pressure of the left (0.827) and right (0.999) forefoot, as well as with the pressure of both forefeet assessed together (0.999). Positive correlation of the lordosis angle also included its relationship with a difference in leg load during gait (0.136). The degree of lordosis angle correlated negatively with the maximum pressure of the left (−0.301) and right (−0.431) foot in the static test, the average pressure of the left (−0.192) and right (−0.267) foot in the static test, and heel load; left (−0.592) and right (−0.765) and both calculated together (−0.999) in a static test. The most significant correlations are presented in the figures.
The relationship in which the test results are linear is the relationship between lordosis angle and forefoot load presented in Figure 4.
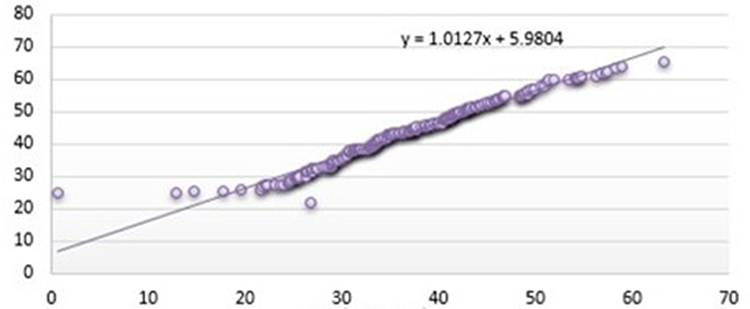 |
Figure 4 Relationship between lordosis angle and forefoot load. x-axis shows lordosis angle and y-axis shows forefoot load. |
Along with the increase in lordosis angle, the heel load decreases, this correlation is also linear (Figure 5).
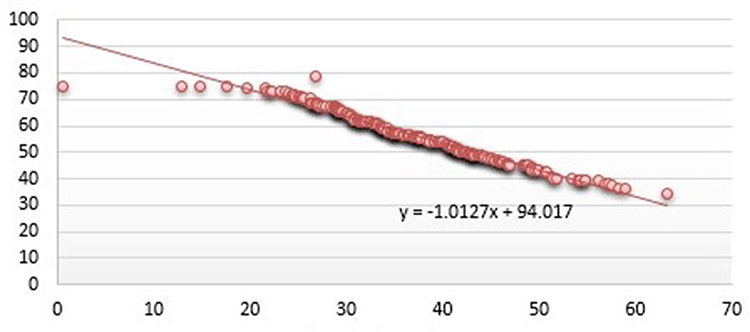 |
Figure 5 Relationship between the lordosis angle and the heel load. x-axis shows lordosis angle and y-axis shows hindfoot load. |
Discussion
An effective and important, in clinical practice, cause and effect approach to health problems leads to the search for functional relationships, often anatomically distant from the original source of the problem. A review of the literature indicates that postural defects related to spine disorders are an inspirational topic in this search. The fact that body posture disorders are one of the factors that can generate various dysfunctions of the human body makes this inspirational aspect.13 Changes in body posture affect the dysfunction of the foot load proportion.6
Winter11 writes that any change in the position of the upper torso results in a shift of the body mass centre which moves to the plantar part of the foot through the hip and ankle joints, causing a change in the load distribution. Carlsöö6 associates this phenomenon with irradiation of the dorsal muscles tension shifting the tension on the calf muscles, causing a change in the proportion of load on individual parts of the feet.
The authors’ own research has shown a significant impact of postural disorders in the sagittal plane on the proportions of foot load. The size of thoracic kyphosis significantly correlated with the forefoot load (0.438 p < 0.001) and heel load (−0.438 p < 0.001) and with maximum left foot pressure (−0.17 p = 0.013) and maximum right foot pressure (−0.207 p = 0.002) in the static test (Table 3). The authors’ own results correspond with the studies of Souza et al14 and Mazzocchi et al,15 who also describe the impact of thoracic kyphosis on the distribution of foot load. The authors14 in their research show an increase in forefoot load along with an increase in thoracic kyphosis angle. Draus et al16 calculated a coefficient describing this phenomenon; according to this author, every 1.8 degree increase in thoracic kyphosis corresponds to a 10% greater load on the forefoot.
The size of lumbar lordosis significantly correlated with forefoot load (0.999 p < 0.001) and heel load (−0.999 p < 0.001), and with maximum left foot pressure (−0.301 p < 0.001) and maximum right foot pressure (−0.431 <0.001) in a static test (Table 4). In the standing position, a relationship between lumbar lordosis size with average left foot pressure (−0.192 p = 0.05) and average right foot pressure (−0.267 p < 0.001) is also shown (Table 4). The size of this curvature of the spine also affected the contact surface of the feet with the ground; for the left foot at 0.301 (p < 0.001) and for the right foot at 0.223 (p = 0.01) (Table 4). Souza et al14 in his study also describes a significant correlation of lumbar lordosis angle, whose increase, in his observations, causes an increase in forefoot load while reducing heel load, which directly corresponds to the results presented in the paper. Mazzocchi et al15 describes the reaction consisting in shifting the load within the feet towards the forefoot along with an increase in pelvic inclination angle, but in this author’s view it is the result of setting reactions resulting primarily from a change in the head position in space and in the angle of thoracic kyphosis. In the case of lumbar lordosis Draus et al16 also calculated a coefficient describing the effect of lordosis on the load of individual parts of the feet; in this author’s view, every 0.8 degree increase in lumbar lordosis corresponds to a 10% greater load on the forefoot. The fact that both an increase in thoracic kyphosis, as well as deepening of lumbar lordosis affect the forward shift of the ground reaction forces can be explained by hypotension coexisting with round-concave back, about which the authors write.14 Passive position with the so-called suspension on the elements of the osteoarticular system, mentioned by Kiebzak2 it may cause a shift of the body’s center of gravity in relation to the support plane around the feet, thus changing the load distribution in individual areas of the feet.
The authors’ own results presented here as well as the observations made by other authors6,11,14–16 clearly confirm the correlation between the size of the kyphosis angle and the lordosis angle and the distribution of ground reaction forces on the feet. However, they do not allow to clearly state which one of these phenomena occurs first and which is secondary. Determining the vector in this cause - effect chain requires further research.
The indicated relations between the shape of the spine and the distribution of load within the feet may contribute to the analysis of the basics of overloading foot diseases. The presented aspect can be considered in diseases such as Morton’s disease, hallux valgus, calcaneal spur or idiopathic Toe Walking. These relationships can be considered by clinicians when searching for the causes of spinal deformities, especially in the sagittal plane. The presented results indicate that in the clinical evaluation of patients with enlarged lumbar lordosis, flat back or round-concave back, it may be important to assess the foot load distribution.
Limitations of the Study
The study did not include the assessment of postural muscles tone, whose activity also affects the distribution of ground reaction forces on the feet. Therefore, further analyses should be considered with the extension of assessment with sEMG of postural muscles.
Clinical Significance
A broader cause and effect view of body posture defects and the distribution of ground reaction forces on the feet can affect a more complete assessment of the correlation between these variables, contributing to more effective treatment of any disorders of the described phenomena.
Conclusions
- The size of thoracic kyphosis and lumbar lordosis affects the distribution of ground reaction forces on the feet.
- The effect of lumbar lordosis is linear in relation with percentage distribution of forefoot and heel loads.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Radzevičienė L, Kazlauskas A. Posture disorders and their causes in rural schools pupils. Soc Welf Interdiscip Approach. 2016;1(6):118–125. doi:10.21277/sw.v1i6.241
2. Kiebzak WP. Positioning of the Sternum and the Sacrum in Relation to Spine Curvatures as a Way of Assessment of Body Posture While Sitting. Kielce: The Jan Kochanowski University Publishing Company; 2018.
3. Lamartina C, Berjano P. Classification of sagittal imbalance based on spinal alignment and compensatory mechanisms. Eur Spine J. 2014;23(6):1177–1189. doi:10.1007/s00586-014-3227-9
4. Pauk J, Daunoraviciene K, Ihnatouski M, Griskevicius J, Raso JV. Analysis of the plantar pressure distribution in children with foot deformities. Acta Bioeng Biomech. 2010;12:29–34. PMID: 20653322.
5. Wojtków M, Szkoda-Poliszuk K, Szotek S. Influence of body posture on foot load distribution in young school-age children. Acta Bioeng Biomech. 2018;2:101–107. doi:10.5277/ABB-01079-2018-01
6. Carlsöö S. The static muscle load in different work positions: an electromyographic study. Ergonomics. 1961;4(3):193–211. doi:10.1080/00140136108930520
7. Cavanagh P, Abdul Razak AH, Zayegh A, Begg RK, Wahab Y. Foot plantar pressure measurement system: a review. Sensors. 2012;12:9884–9912. doi:10.3390/s120709884
8. Paolucci T, Pezzi L, Mannocci A, La Torre G, Bellomo RG, Saggini R. Flat foot and postural harmony in 6-year-old caucasians: what is their relationship. Ann Rehabil Med. 2020;44(4):320–326. doi:10.5535/arm.19091
9. Wafai L, Zayegh A, Woulfe J, Aziz S, Begg R. Identification of foot pathologies based on plantar pressure asymmetry. Sensors. 2015;15(8):20392–20408. doi:10.3390/s150820392
10. Vuillerme N, Chenu O, Demongeot J, Payan Y. Controlling posture using a plantar pressure-based, tongue-placed tactile biofeedback system. Exp Brain Res. 2007;179(3):409–414. doi:10.1007/s00221-006-0800-4
11. Winter DA. Human balance and posture control during standing and walking. Gait Posture. 1995;3(4):193–214. doi:10.1016/0966-6362(96)82849-9
12. Volker D. Interaction between central programs and afferent input in the control of posture and locomotion. J Biomech. 1996;29:841–844. doi:10.1016/0021-9290(95)00175-1
13. Paprocki M, Rychter P, Wilczyński J. Accuracy of the optoelectronic test body posture FormetricDiers Method III 4D in comparison with the result of the x-ray pictures. J Educ Health Sport. 2016;6:385–398. doi:10.5281/zenodo.50535
14. Souza J, Pasinato F, Corrêa E, da Silva A. Global body posture and plantar pressure distribution in individuals with and without temporomandibular disorder: a preliminary study. J Manipulative Physiol Ther. 2014;37:407–414. doi:10.1016/j.jmpt.2014.04.003
15. Mazzocchi M, Dessy LA, Iodice P, et al. A study of postural changes after breast augmentation. Aesth Plast Surg. 2012;36(3):570–577. doi:10.1007/s00266-011-9841-6
16. Draus C, Moravec D, Kopiec A, Knott P. Comparison of barefoot vs. shod gait on spinal dynamics using DIERS formetric 4D and DIERS pedoscan systems. Open j Ther Rehabil. 2015;3(3):70–76. doi:10.4236/ojtr.2015.33010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.