")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Effect of Switching to Brexpiprazole on Plasma Homovanillic Acid Levels and Antipsychotic-Related Side Effects in Patients with Schizophrenia or Schizoaffective Disorder
Authors Ichinose M, Miura I , Horikoshi S, Yamamoto S, Kanno-Nozaki K, Watanabe K, Yabe H
Received 14 February 2021
Accepted for publication 30 March 2021
Published 13 April 2021 Volume 2021:17 Pages 1047—1053
DOI https://doi.org/10.2147/NDT.S306573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Mizue Ichinose,1,2 Itaru Miura,1 Sho Horikoshi,1,3 Shinnosuke Yamamoto,1,4 Keiko Kanno-Nozaki,1 Kenya Watanabe,5 Hirooki Yabe1
1Department of Neuropsychiatry, Fukushima Medical University School of Medicine, Fukushima, Japan; 2Department of Neuropsychiatry, Hoshigaoka Hospital, Koriyama, Japan; 3Department of Psychiatry, Horikoshi Psychosomatic Clinic, Fukushima, Japan; 4Department of Psychiatry, Fukushima Red Cross Hospital, Fukushima, Japan; 5Department of Pharmacy, Fukushima Medical University Hospital, Fukushima, Japan
Correspondence: Itaru Miura
Department of Neuropsychiatry, Fukushima Medical University School of Medicine, Hikarigaoka 1, Fukushima, 960-1295, Japan
Tel +81-24-547-1331
Fax +81-24-548-6735
Email [email protected]
Objective: Although switching antipsychotics is a common strategy in the treatment of schizophrenia, caution is needed because of the risk of worsening of psychosis, particularly when switching to a dopamine D2 partial agonist. Homovanillic acid (HVA), a dopamine metabolite, is thought to be a possible indicator of the response to antipsychotics. We examined the effects of switching to brexpiprazole monotherapy from other antipsychotics on plasma HVA levels and side effects during maintenance treatment of schizophrenia.
Methods: The antipsychotics of 37 Japanese patients with schizophrenia or schizoaffective disorder were switched to brexpiprazole for the improvement of side effects. We evaluated clinical symptoms and extrapyramidal symptoms (EPS) and took fasting blood samples at baseline and endpoint (eight weeks after completing the switch) to measure plasma levels of HVA, prolactin, and metabolic parameters.
Results: Switching to brexpiprazole significantly decreased the Drug-Induced Extrapyramidal Symptoms Scale total score (p=0.008), prolactin levels (p< 0.001), body weight (p=0.046), and body-mass index (p=0.034), and increased HDL cholesterol (p=0.008). On the other hand, switching to brexpiprazole did not change plasma levels of HVA or Positive and Negative Syndrome Scale scores.
Conclusion: Switching to brexpiprazole significantly improved EPS, high prolactin levels, and metabolic side effects without elevating plasma HVA levels. Brexpiprazole may stabilize dopaminergic neural transmission and could be a useful strategy to decrease the burden in patients with schizophrenia during the maintenance phase. Because of the small sample size, further studies with larger sample sizes are needed to confirm and extend our results.
Keywords: brexpiprazole, extrapyramidal symptoms, EPS, homovanillic acid, prolactin, schizophrenia, switching
Introduction
In the treatment of schizophrenia, side effects caused by antipsychotics including extrapyramidal symptoms (EPS), hyperprolactinemia, and metabolic effects impair quality of life and decrease medication adherence, while the differences in efficacy may be small between individual antipsychotics.1–3 Particularly, most second-generation antipsychotics (SGAs) have higher metabolic and cardiovascular effects compared with first-generation antipsychotics (FGAs), which may lead to mortality risk.1,2 Switching antipsychotics is a common strategy to reduce such side effects, although caution is needed because of the risk of worsening of symptoms.
Brexpiprazole (BPZ) is a partial agonist for dopamine D2 and 5-HT1A receptors and an antagonist for 5-HT2A receptors,4 and it has a favorable safety and efficacy profile in the treatment of schizophrenia.1 Although switching to BPZ from other antipsychotics typically decreases various side effects, caution may be needed when switching to antipsychotics that are partial agonists of dopamine D2 receptors (DRD2),5 particularly in patients with dopamine supersensitivity psychosis.6 Plasma levels of homovanillic acid (HVA), a dopamine metabolite, are thought to be a possible indicator of the response to antipsychotics in the treatment of schizophrenia.7–9 Although it is difficult to regard plasma monoamine metabolite levels as direct reflections of central activity, it is estimated that 30–50% of plasma HVA is derived from the brain.10 Few studies report the effects of switching to BPZ from other antipsychotics on dopamine turnover and antipsychotic-related side effects in patients with schizophrenia.
In this study, we examined the effects of switching to BPZ monotherapy from other antipsychotics on plasma levels of HVA, EPS, prolactin levels, and metabolic side effects during maintenance treatment of schizophrenia and schizoaffective disorder.
Patients and Methods
Subjects were Japanese patients diagnosed with schizophrenia or schizoaffective disorder according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. All patients had been treated with antipsychotics before the study. Antipsychotics in all patients were switched to BPZ based on a physician’s decision to improve side effects such as EPS, hyperprolactinemia, or metabolic side effects. The switching methods, duration, and the dose of BPZ were not fixed. Benzodiazepines and anticholinergics were permitted as additional medications to manage insomnia, restlessness, and EPS. The endpoint was defined as eight weeks after completion of the antipsychotic switching. We evaluated symptom severity via the Positive and Negative Syndrome Scale (PANSS), Clinical Global Impression (CGI), and Drug-Induced Extrapyramidal Symptoms Scale (DIEPSS) at baseline and endpoint. In addition, fasting blood samples were taken at baseline and endpoint to measure triglycerides (TG), LDL cholesterol (LDL), HDL cholesterol (HDL), fasting glucose (BS), hemoglobin A1c (HbA1c), prolactin, and HVA, body weight (BW) and body-mass index (BMI) was also measured at those times. Plasma levels of HVA were analyzed by high-performance liquid chromatography with electrochemical detection using methods previously described.11 In brief, 1000 μL of plasma sample was deproteinized and extracted into ethyl acetate saturated with NaCl twice. The organic phases were evaporated to dryness. After dissolving in 500 μL of ultrapure water, 20 μL was injected into the HPLC. All chromatographic separations were performed on octadecyl-functionalized silica gel (3 μm particles, 4.5 mm 150 mm) reversed-phase column. The intra- and inter-assay coefficients of variation for plasma HVA levels in our laboratory were 3.4% and 6.2%, respectively. This study was approved by the ethics committee of Fukushima Medical University, and the patients provided written informed consent after having been informed of the purpose of the study.
This study was conducted in accordance with the Declaration of Helsinki.
We used a t-test to compare PANSS, CGI-S, DIEPSS scores, plasma HVA levels, and other laboratory data at baseline and endpoint. Intent-to-treat analyses were performed using the last observation carried forward method for PANSS, CGI, and DIEPSS scores. The Mann–Whitney U-test was used to compare the baseline data and the changes between the completion group and the dropout group. The chi-square test was used to compare the baseline data.
Results
A total of 37 subjects (23 men and 14 women, schizophrenia: n=34; schizoaffective disorder: n=3) were included in this study. Most were chronic outpatients, and the duration of illness was 27.1±14.8 years. Five of 37 patients (13.5%) received antipsychotic polypharmacy at baseline. The average chlorpromazine-equivalent dose of the previous antipsychotics was 410.2±272.3 mg, and 24.3% of the patients were taking high-dose antipsychotics (chlorpromazine-equivalent doses ≥600 mg) (Table 1). Twenty-seven patients completed the study, and ten patients dropped out because of worsening of schizophrenia (n=5), irritation (n=2), insomnia (n=2), and other reasons (n=1). The switching methods were add-on switching in 24 cases (64.9%) and cross titration switching in 13 cases (35.1%) (Table 1).
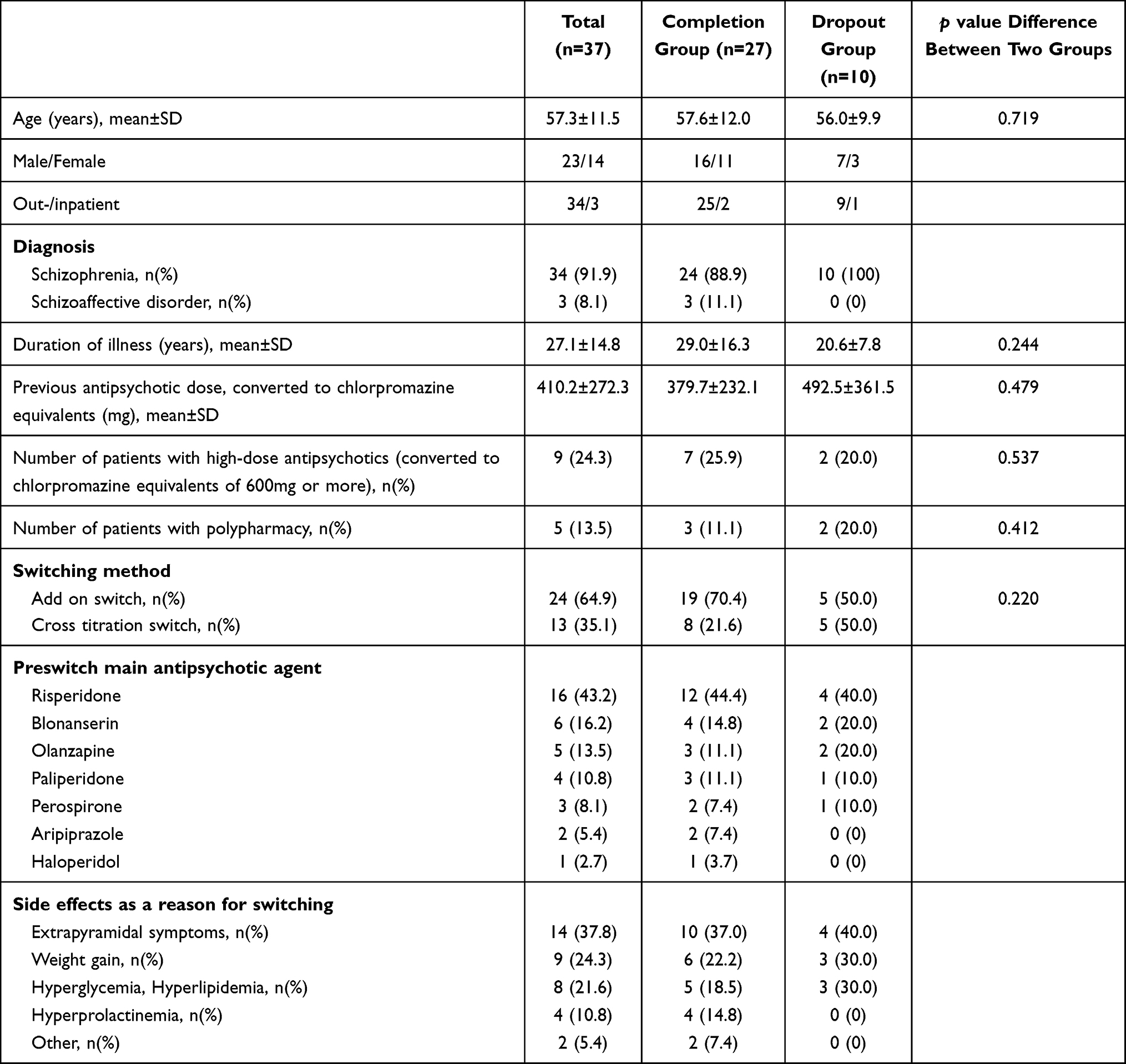 |
Table 1 Baseline Characteristics |
For all subjects, there were no significant changes in the PANSS total score (baseline 61.5±19.5, endpoint 63.5±23.1, p=0.498), CGI-S (Severity) (baseline 3.5±0.9, endpoint 3.5±0.9, p=0.624), and plasma HVA levels (baseline 11.8±7.7 ng/mL, endpoint 13.2±6.0 ng/mL, p=0.296) after the switch (Table 2). DIEPSS total score and prolactin levels showed a significant decrease after the switch (DIEPSS; baseline 3.6±3.7, endpoint 2.5±2.9, p=0.008, prolactin; baseline 28.9±26.9 ng/mL, endpoint 13.0±14.6 ng/mL, p<0.001) (Table 2). Prolactin levels significantly decreased in each gender (male; baseline 20.7±11.6 ng/mL, endpoint 6.6±4.1 ng/mL, p<0.001, female; baseline 40.0±36.9 ng/mL, endpoint 21.8±19.0 ng/mL, p=0.044) (Table 2). Furthermore, BW and BMI showed a significant decrease (BW; baseline 73.6±24.1, endpoint 72.4±23.9, p=0.046, BMI; baseline 28.0±7.1, endpoint 27.5±7.1, p=0.034) and HDL significantly increased (baseline 48.4±11.1 mg/dl, endpoint 52.2±11.6 mg/dl, p=0.008) after the switch (Table 2).
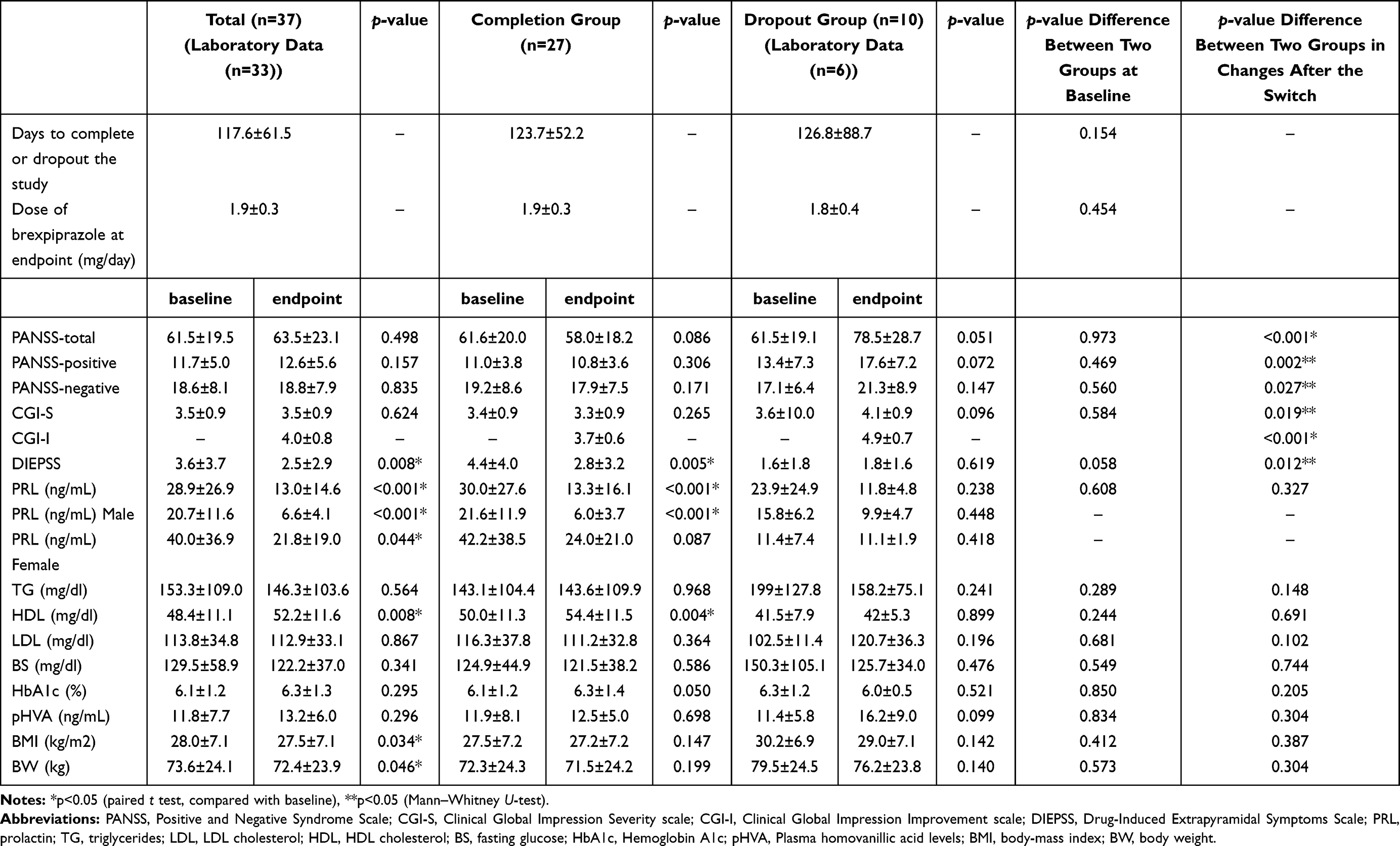 |
Table 2 Clinical Outcomes in Each Group |
Comparing the completion and the dropout groups, although there were no significant differences in the characteristics at baseline, switching method, duration of switching, and the dose of BPZ after the switching between the two groups, the DIEPSS total score of the completion group tended to be higher than that of the dropout group at baseline (p=0.058) (Tables 1 and 2). Furthermore, the changes in PANSS total (p<0.001), positive (p=0.002), and negative (p=0.027) scores, CGI-S (p=0.019), and DIEPSS total score (p=0.012) were significantly different between the two groups after the switching (Table 2). The PANSS total (p=0.051) and positive score (p=0.072), CGI-S (p=0.096), and plasma HVA levels (p=0.099) tended to increase at the endpoint in the dropout group but not in the completion group. In the completion group, the DIEPSS total score (p=0.005) and PRL levels (p<0.001) showed a significant decrease, whereas HDL (p=0.004) showed a significant increase after the switch.
Discussion
To our knowledge, this is the first study to investigate the effects of switching to BPZ from other antipsychotics on plasma levels of HVA, prolactin, EPS, and metabolic side effects simultaneously in patients with schizophrenia or schizoaffective disorder. In this study, for all subjects, the switch to BPZ improved EPS and decreased prolactin levels significantly, whereas it did not change PANSS scores and plasma HVA levels. With regard to EPS and prolactin, the results were consistent with a previous study in Japan, although that study included patients who received >2mg/day of BPZ.12 Moreover, a recent network meta-analysis suggested that BPZ did not show a significant increase of prolactin compared with placebo in patients with acute schizophrenia.1 BPZ has a unique pharmacological profile as a partial agonist for DRD2, which may lead to these results. Most subjects (30 of 37, 81.0%) received serotonin-dopamine antagonists or FGA before the switch, and the partial agonism and relatively higher D2 intrinsic activity of BPZ brought the improvement of EPS and high prolactin levels, which were associated with DRD2 antagonism. Notably, switching to BPZ did not alter plasma levels of HVA, which is a possible indicator of antipsychotic treatment response in the switching strategy in patients with schizophrenia.9 Previous studies have suggested that psychotic symptoms were correlated to plasma HVA levels in the treatment of schizophrenia.9,13–15 Taken together, our results suggest that switching to BPZ may stabilize dopaminergic neural transmission, which leads to an improvement of high prolactin levels and EPS induced by D2 antagonism without elevating of HVA levels.
The discontinuation rate of this study was 27%, which was higher than that of a previous study (17.0%).16 In that study,16 however, the discontinuation rate of the subgroup in which subjects received non-aripiprazole before the switch to BPZ was 25.4%, which was comparable to that in our study. In this study, the changes in PANSS scores, CGI-S, and DIEPSS total score were significantly different between the two groups after the switching (Table 2). Furthermore, PANSS total (p=0.051), positive score (p=0.072), and plasma HVA levels (p=0.099) tended to increase in the dropout group at the endpoint, although a small number of patients restricted the results. At the patient level, plasma levels of HVA in 5 of 6 patients (83.3%) who finished blood tests at both baseline and endpoint in the dropout group increased after incomplete switching to BPZ. These results were comparable with a previous study of our’s,9 which showed that plasma HVA levels of worsened patients increased after switching to aripiprazole or blonanserin from other antipsychotics in patients with schizophrenia. Our results suggest that plasma levels of HVA may be a possible indicator for switching to D2 partial agonists during the maintenance phase of schizophrenia or schizoaffective disorder.
There were several possible reasons for the dropout and completion rates in this study. A recent study suggested that add-on switching to aripiprazole may induce a better outcome for the continuation of aripiprazole than cross switching and direct switching.17 In addition, it has been suggested that the incidences of adverse events and worsening of psychiatric symptoms were lower when switching slowly over time.16,18 In this study, the switching method of 5 (55.6%) of the 9 dropout patients because of worsening psychiatric symptoms was cross switching. The switching method may have effects on the dropout rate, and careful add-on switching may induce a favorable outcome for the continuation of BPZ. In addition, although there was no significant difference in the duration of switching between the groups, the pace of reduction of the previous drug might have been accelerated, which may also lead to the worsening of psychiatric symptoms. Yoshimura et al reported that patients who had previously taken high doses of antipsychotics (CP-equivalent doses of more than 800 mg/day) had a higher discontinuation rate of BPZ.19 Although the CP-equivalent doses of antipsychotics at baseline in the dropout group were relatively low (492.5±361.5 mg/day) and not different from those in the completion group, most subjects in this study were chronic and had received long-term antipsychotic treatment. Caution is needed in switching antipsychotics to a partial agonist, particularly in patients with dopamine supersensitivity psychosis,5,6 and partial agonism of BPZ may be associated with the worsening of psychosis in this study. Moreover, the maximum dose of BPZ in Japan is 2 mg/day, which is lower than that of other countries. A higher dose of BPZ may be needed to prevent the worsening of psychosis in some patients, in particular patients who are chronic and have received long-term antipsychotic treatment before switching. At baseline, the DIEPSS total score of the completion group tended to be higher than that of the dropout group. Although the reason remains unclear, more severe EPS may reflect an overblockade of DRD2, and the subjects in the completion group may tend to accept the switching because of BPZ’s partial agonism and favorable profile for EPS.
Regarding metabolic parameters, there was a significant decrease in BW and BMI, and a significant increase in HDL after switching to BPZ, which is consistent with previous meta-analyses showing that BPZ has a favorable profile for metabolic side effects.1,2 A previous study reported that the average weight gain associated with BPZ was 3.2 kg vs 4.0 kg with aripiprazole, and the rate of weight increase ≥7% was 18.6% for BPZ vs 25.3% for aripiprazole in acute and 52-week studies.20 Weight gain is one of the common side effects of SGAs, which leads to non- or partial adherence, metabolic and cardiovascular risks. Murray et al raised several issues about the long-term prophylactic use of antipsychotics, including effects of antipsychotics on physical health, antipsychotic-induced dopamine receptor supersensitivity, and treatment-resistant schizophrenia.21 Together with previous studies indicating that it seems that dopamine partial agonists do not induce D2 receptor supersensitivity,22,23 our results of significant effects on prolactin, EPS, and metabolic side effects suggest that switching to BPZ is a useful long-term treatment strategy for patients with SGAs-associated side effects in real-world settings.
Our study has several limitations. First, this is a non-randomized open study, and our sample size was very small. Furthermore, previous studies have reported the safety of BPZ with a larger sample size.12,16,20 Second, it is difficult to regard plasma dopamine metabolites as direct reflections of central activity, although not only central nervous system but also peripheral markers may be possible biomarkers for schizophrenia.24 Third, because most patients were outpatients, non- or partial adherence to medication may have affected the results. Nevertheless, this is the first study to investigate the effect of switching to BPZ on plasma HVA levels, which is a possible biomarker in the treatment of schizophrenia. Our results suggest that switching to BPZ improves EPS, high prolactin levels, and metabolic side effects without elevating plasma levels of HVA, and may be a useful long-term treatment strategy for patients with schizophrenia or schizoaffective disorder. Furthermore, plasma levels of HVA may be a possible indicator for switching to a D2 partial agonist from other antipsychotics during the maintenance phase of schizophrenia or schizoaffective disorder.
Conclusion
In summary, we found that switching to BPZ from other antipsychotics significantly improved EPS, high prolactin levels, and metabolic side effects (BW, BMI, and HDL) without elevating plasma HVA levels during the maintenance phase of schizophrenia or schizoaffective disorder. Our results suggest that switching to BPZ may stabilize dopaminergic neural transmission and could be a useful long-term treatment strategy to decrease the burden in patients with schizophrenia or schizoaffective disorder, although careful and flexible switching methods may be needed for successful switching. Furthermore, longitudinal measurement of plasma levels of HVA may be useful for switching strategies in the maintenance treatment of schizophrenia, in particular when switching to DRD2 partial agonists. Caution is warranted in interpreting these results because of the small sample size, and further studies with larger sample sizes are needed to confirm and extend our results.
Disclosure
Dr. Ichinose has received speaker’s honoraria from Otsuka. Dr. Miura has received speaker’s honoraria from Daiichi Sankyo, Dainippon Sumitomo, Janssen, Meiji Seika, Mochida, MSD, Mylan, Otsuka, Pfizer, and Takeda. Dr. Horikoshi has received speaker’s honoraria from Dainippon Sumitomo, Janssen, Meiji Seika Pharma, MSD, Otsuka, and Yoshitomi. Dr. Yabe has received speaker’s honoraria from Dainippon Sumitomo, Nippon Chemiphar, MSD, Otsuka, Meiji Seika Pharma, Eisai, Janssen, Mochida, Mylan EPD, and Yoshitomi. The authors report no other conflicts of interest in this work.
References
1. Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939–951. doi:10.1016/S0140-6736(19)31135-3
2. Pillinger T, McCutcheon RA, Vano L, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(1):64–77. doi:10.1016/S2215-0366(19)30416-X
3. Tandon R, Lenderking WR, Weiss C, et al. The impact on functioning of second-generation antipsychotic medication side effects for patients with schizophrenia: a worldwide, cross-sectional, web-based survey. Ann Gen Psychiatry. 2020;13(19):42. doi:10.1186/s12991-020-00292-5
4. Ward K, Citrome L. Brexpiprazole for the maintenance treatment of adults with schizophrenia: an evidence-based review and place in therapy. Neuropsychiatr Dis Treat. 2019;15(15):247–257. doi:10.2147/NDT.S169369
5. Takeuchi H, Fathi A, Thiyanavadivel S, et al. Can aripiprazole worsen psychosis in schizophrenia? A meta-analysis of double-blind, randomized, controlled trials. J Clin Psychiatry. 2018;79(2):17r11489. doi:10.4088/JCP.17r11489
6. Takase M, Kanahara N, Oda Y, et al. Dopamine supersensitivity psychosis and dopamine partial agonist: a retrospective survey of failure of switching to aripiprazole in schizophrenia. J Psychopharmacol. 2015;29(4):383–389. doi:10.1177/0269881115570083
7. Yoshimura R, Ueda N, Hori H, et al. Different patterns of longitudinal changes in plasma levels of catecholamine metabolites and brain-derived neurotrophic factor after administration of atypical antipsychotics in first episode untreated schizophrenic patients. World J Biol Psychiatry. 2010;11(2 Pt 2):256–261. doi:10.3109/15622970802309617
8. Miura I, Takeuchi S, Katsumi A, et al. Effects of aripiprazole and the Taq1A polymorphism in the dopamine D2 receptor gene on the clinical response and plasma monoamine metabolites level during the acute phase of schizophrenia. J Clin Psychopharmacol. 2012;32(1):106–109. doi:10.1097/JCP.0b013e31823f87ac
9. Miura I, Shiga T, Katsumi A, et al. Switching antipsychotics to aripiprazole or blonanserin and plasma monoamine metabolites levels in patients with schizophrenia. Hum Psychopharmacol. 2014;29(2):199–202. doi:10.1002/hup.2386
10. Maas JW, Hattox SE, Greene NM, Landis DH. Estimates of dopamine and serotonin synthesis by the awake human brain. J Neurochem. 1980;34:1547. doi:10.1111/j.1471-4159.1980.tb11240.x
11. Watanabe K, Miura I, Kanno-Nozaki K, et al. Associations between five-factor model of the Positive and Negative Syndrome Scale and plasma levels of monoamine metabolite in patients with schizophrenia. Psychiatry Res. 2015;230(2):419–423. doi:10.1016/j.psychres.2015.09.030
12. Ishigooka J, Inada K, Niidome K, et al. Safety of switching to brexpiprazole in Japanese patients with schizophrenia: a post-hoc analysis of a long-term open-label study. Hum Psychopharmacol. 2021. doi:10.1002/hup.2777
13. Pickar D, Labarca R, Doran AR, et al. Longitudinal measurement of plasma homovanillic acid levels in schizophrenic patients. Correlation with psychosis and response to neuroleptic treatment. Arch Gen Psychiatry. 1986;43(7):669–676. doi:10.1001/archpsyc.1986.01800070059008
14. Davidson M, Kahn RS, Knott P, et al. Effects of neuroleptic treatment on symptoms of schizophrenia and plasma homovanillic acid concentrations. Arch Gen Psychiatry. 1991;48(10):910–913. doi:10.1001/archpsyc.1991.01810340042005
15. Kelley ME, Yao JK, van Kammen DP. Plasma catecholamine metabolites as markers for psychosis and antipsychotic response in schizophrenia. Neuropsychopharmacology. 1999;20(6):603–611. doi:10.1016/S0893-133X(98)00094-3
16. Ishigooka J, Usami T, Iwashita S, et al. Post-hoc analysis investigating the safety and efficacy of brexpiprazole in Japanese patients with schizophrenia who were switched from other antipsychotics in a long-term study (Secondary Publication). Neuropsychopharmacol Rep. 2020;40(2):122–129. doi:10.1002/npr2.12107
17. Obayashi Y, Mitsui S, Sakamoto S, et al. Switching strategies for antipsychotic monotherapy in schizophrenia: a multi-center cohort study of aripiprazole. Psychopharmacology. 2020;237:167–175. doi:10.1007/s00213-019-05352-7
18. Correll CU, Shi L, Weiss C, et al. Successful switching of patients with acute schizophrenia from another antipsychotic to brexpiprazole: comparison of clinicians’ choice of cross-titration schedules in a post hoc analysis of a randomized, double-blind, maintenance treatment study. CNS Spectr. 2019;24(5):507–517. doi:10.1017/S1092852918001086
19. Yoshimura Y, Shimizu H, Yamashita R, et al. Association between previous high-dose antipsychotic therapy and brexpiprazole discontinuation after the initiation of brexpiprazole in patients with schizophrenia or schizoaffective disorder. Int Clin Psychopharmacol. 2020;35(2):98–104. doi:10.1097/YIC.0000000000000296
20. Weiss C, Weiller E, Baker RA, et al. The effects of brexpiprazole and aripiprazole on body weight as monotherapy in patients with schizophrenia and as adjunctive treatment in patients with major depressive disorder: an analysis of short-term and long-term studies. Int Clin Psychopharmacol. 2018;33(5):255–260. doi:10.1097/YIC.0000000000000226
21. Murray RM, Quattrone D, Natesan S, et al. Should psychiatrists be more cautious about the long-term prophylactic use of antipsychotics? Br J Psychiatry. 2016;209(5):361–365.
22. Tadokoro S, Okamura N, Sekine Y, et al. Chronic treatment with aripiprazole prevents development of dopamine supersensitivity and potentially supersensitivity psychosis. Schizophr Bull. 2012;38:1012–1020. doi:10.1093/schbul/sbr006
23. Amada N, Akazawa H, Ohgi Y, et al. Brexpiprazole has a low risk of dopamine D2 receptor sensitization and inhibits rebound phenomena related to D2 and serotonin 5‐HT2A receptors in rats. Neuropsychopharmacol Rep. 2019;39(4):279–288. doi:10.1002/npr2.12076
24. Cao T, Li NN, Cai HL. Candidate metabolic biomarkers for schizophrenia in CNS and periphery: do any possible associations exist? Schizophr Res. 2020;226:95–110.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.