")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Effect of stent-assisted angioplasty on cognitive status and serum levels of amyloid beta in patients with intracranial and/or extracranial artery stenosis
Authors Zhao L, Zhao Y, Zhang H
Received 28 December 2014
Accepted for publication 29 January 2015
Published 24 February 2015 Volume 2015:11 Pages 471—475
DOI https://doi.org/10.2147/NDT.S79950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Wai Kwong Tang
Liandong Zhao,1 Ying Zhao,1 Haijun Zhang2
1Department of Neurology, The Second People’s Hospital of Huai’an and The Affiliated Huai’an Hospital of Xuzhou Medical College, Huai’an, Jiangsu, 2Department of Oncology, Zhongda Hospital, Medical School, Southeast University, Nanjing, People’s Republic of China
Aim: The study reported here aimed to examine how stent-assisted angioplasty affects cognitive status and serum levels of amyloid betas (Aβs) 1-40 and 1-42 in patients with cerebral arterial stenosis.
Methods: Patients with cerebral arterial stenosis were given stent-assisted angioplasty plus conventional treatment (stent-assisted angioplasty group) or conventional treatment alone (control group). Cognitive status and Aβ1-40 and Aβ1-42 serum levels were determined before treatment and at 4 and 8 weeks after treatment.
Results: At 4 weeks after treatment, cognitive status in patients with stent-assisted angioplasty had clearly improved. Aβ1-42 serum levels changed insignificantly in all patients. However, Aβ1-40 serum levels and Aβ1-40/Aβ1-42 ratio decreased further in patients with stent-assisted angioplasty than in patients who received conventional treatment (controls). Eight weeks after treatment, cognitive status in patients who had undergone stent-assisted angioplasty were continuing to improve, Aβ1-42 serum levels had begun to increase dramatically, and Aβ1-40 serum levels and Aβ1-40/Aβ1-42 ratio had declined further.
Conclusion: Stent-assisted angioplasty could improve cognitive status and decrease Aβ1-40 serum levels and Aβ1-40/Aβ1-42 ratio.
Keywords: arterial stenosis, Alzheimer’s disease, Aβ1-40, Aβ1-42, Aβ1-40/Aβ1-42 ratio
Introduction
Intracranial and/or extracranial artery stenoses are characterized by narrowed arteries that supply blood to the brain, which can lead to cerebral hypoperfusion or impaired cognitive function, and promote the development of Alzheimer’s disease (AD). AD is the most common type of dementia and represents a serious threat to both physical and psychological health.1–3
The pathological process of AD can be accelerated by hypoxia.4 The current hypothesis of the pathogenesis of familial AD results mainly from aberrant cleavage of amyloid beta precursor protein (APP), which produces cytotoxic amyloid beta (Aβ) fragments, causes progressive degeneration and dysfunction of neurons, and ultimately leads to the development of AD. The contribution of Aβ deposition in the pathogenesis of AD has been well established and Aβ appears to have a role in ischemic cerebral damage.4 Studies have suggested that plasma or serum concentrations of Aβ1-40 and Aβ1-42, as well as well as the ratio of Aβ1-40 to Aβ1-42, may be used as biomarkers for AD and dementia.5–10 For example, increased plasma Aβ1-40 levels are associated with an increased risk of dementia.6 Elevated serum levels of Aβ in the first-degree relatives of patients with AD appear to be indicative of presymptomatic AD.11
However, the correlation of cerebral ischemia due to intracranial and/or extracranial artery stenosis with serum levels of Aβ remains poorly characterized. In the study reported here, we evaluated the cognitive status and serum levels of Aβ1-40 and Aβ1-42 in patients both treated and not treated with stent-assisted angioplasty for their intracranial and/or extracranial arterial stenosis before treatment and at 4 and 8 weeks after treatment.
Materials and methods
Patients
The patients were recruited from the Second People’s Hospital of Huai’an (the Affiliated Huai’an Hospital of Xuzhou Medical College) from October 1, 2013 to September 30, 2014. Patients with dizziness, transient ischemic attack, and 70% or more internal carotid artery stenosis on one or both sides as determined by digital subtraction angiography were included in the study. Patients were excluded if they had a history of major medical illness, such as heart failure, pulmonary insufficiency, renal insufficiency, hepatic dysfunction, or blood diseases unfit for antiplatelet therapy.
The stent-assisted angioplasty group consisted of 78 patients (45 men and 33 women) aged from 43 to 83 years (mean age of 58.6 years). The non-stent-assisted angioplasty (control) group consisted of 44 patients (26 men and 18 women) aged from 41 to 78 years (mean age of 54.3 years). In the stent-assisted angioplasty group, there were 41 (52.56%) cases of unilateral internal carotid artery stenosis, 22 (28.21%) cases of bilateral internal carotid artery stenosis, ten (12.82%) cases of unilateral internal carotid artery stenosis associated with vertebral artery stenosis, and five (6.41%) cases of unilateral internal carotid artery stenosis associated with middle cerebral artery stenosis. In the control group, there were 19 (43.18%) cases of unilateral internal carotid artery stenosis, eleven (25%) cases of bilateral internal carotid artery stenosis, nine (20.45%) cases of unilateral internal carotid artery stenosis associated with vertebral artery stenosis, and five (11.36%) cases of unilateral internal carotid artery stenosis associated with middle cerebral artery stenosis.
All patients had experienced at least 1 month of nervous-system dysfunctions. No severe cerebrovascular problems, such as stroke, occurred during the study period. Based on computed tomography examinations, the size of cerebral infarction in all patients was less than 100 mL. Clinical symptoms of cerebral ischemia, such as paralysis of limbs and/or disturbance of consciousness, were observed in most of the cases. During the study period, all patients were given 75 mg of clopidogrel and 100 mg of enteric-coated aspirin orally once a day in addition to the use of salvia, puerarin, and an anti-free-radical agent, edaravone.
The study was approved by the Second People’s Hospital of Huai’an Ethics Committee and informed consent was obtained from all of the participants.
Stent-assisted angiography
Written informed consent was obtained from each patient before surgery. Balloon dilation was performed via the femoral artery approach and a Cordis artery stent (SMART stent and PALMAZ stent: Cordis Corporation, Bridgewater Township, NJ, USA) was implanted into the stenotic artery. Postoperative residual stenosis was determined to be less than 10% by digital subtraction angiography. In the control group, vascular reconstruction was not performed.
Collection of blood samples
Ethylenediaminetetraacetic acid (EDTA)-anticoagulated blood samples (5 mL) were collected via the cubital vein from fasted patients before treatment and at 4 and 8 weeks after treatment. The blood samples were centrifuged at 1,000 rpm for 10 minutes and sera were immediately collected and stored at −70°C.
Cognitive-status evaluation
The cognitive status was evaluated with the Mini-Mental State Examination (MMSE) questionnaire before treatment and at 4 and 8 weeks after treatment in all patients.
Measurement of serum levels of amyloid beta
Plasma concentrations of Aβ were determined using solid-phase sandwich enzyme-linked immunosorbent assay (ELISA) kits per the manufacturer’s instructions (Adlitteram Diagnostic Laboratories, San Diego, CA, USA).
Statistical analysis
All data are expressed as mean ± standard deviation (SD). Statistical analyses were performed using SPSS software (v 10.0; IBM Corp, Armonk, NY, USA). The F-test was used for significance testing, and P<0.05 was considered to be statistically significant, power =0.90.
Results
Effect of stent-assisted angioplasty on cognitive status
To investigate the effect of stent-assisted angioplasty on the cognitive status of patients with intracranial and/or extracranial artery stenosis, we first evaluated the cognitive status with the MMSE before any treatment. As shown in Table 1, the MMSE scores of patients with/without stent-assisted angioplasty had no obvious difference before treatment (P>0.05). Four weeks after treatment, the MMSE scores of patients who had undergone stent-assisted angioplasty had improved sharply (P<0.05), while those of patients who had not undergone stent-assisted angioplasty (ie, the controls) had no obvious change (P>0.05). Eight weeks after treatment, the MMSE scores of patients who had undergone stent-assisted angioplasty had improved further (P<0.05), and those of patients who had not undergone stent-assisted angioplasty still had no obvious change (P>0.05).
 | Table 1 Mini-Mental State Examination scores before and after treatment |
Effect of stent-assisted angioplasty on serum levels of amyloid beta
We also investigated the relationship between serum levels of Aβ and the improved blood supply following stent-assisted angioplasty. As shown in Table 2, no significant difference was found in the serum levels of Aβ1-40 and Aβ1-42 between the stent-assisted angioplasty group and the control group before treatment (P>0.05). Four weeks after treatment, the serum levels of Aβ1-40 in both groups had decreased significantly. This decrease was particularly obvious in the stent-assisted angioplasty group (P<0.05). There were no significant changes in the serum Aβ1-42 levels after 4 weeks in either group (P>0.05). Eight weeks after treatment, the serum levels of Aβ1-40 were further reduced in both of groups – 0.87±0.18 ng/L (mean ± SD) in the stent-assisted angioplasty group and 0.96±0.23 ng/L in the control group. The serum levels of Aβ1-42 had increased significantly in the stent-assisted angioplasty group when compared with the levels before treatment (P<0.05), 4 weeks after treatment (P<0.05), and when compared with levels in the control group, for which there were no significant changes throughout the study (P>0.05). Accordingly, compared with no significant changes in the control group, 4 weeks after treatment, the ratio of Aβ1-40/Aβ1-42 in the stent-assisted angioplasty group had decreased (P<0.05), and a further decrease was detected 8 weeks after treatment (P<0.05).
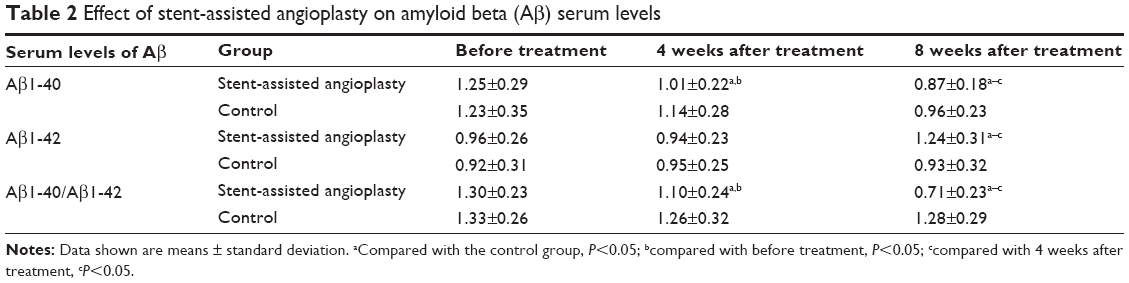 | Table 2 Effect of stent-assisted angioplasty on amyloid beta (Aβ) serum levels |
Discussion
The observation that the incidence of AD is significantly increased after stroke and infarction further implicates brain hypoxia in AD etiology.12,13 Nevertheless, the underlying mechanism remains to be elucidated. It is possible that the decreased cerebral perfusion reduces the nutritional status of cerebral cells, facilitates Aβ production, and inhibits Aβ clearance. Aβ plays a critical role in the pathogenesis of AD. Aβ fragments are hydrophobic peptides consisting of 40–42 residues derived from the sequential cleavage of APP by proteinases and beta (β)- and gamma (γ)-secretases. An imbalance between production and clearance of Aβ fragments may cause abnormal accumulation of these peptides inside the brain and the subsequent development of AD.14,15
Hypoxia due to intracranial and/or extracranial artery stenosis may promote β-site cleavage of APP and cleavage activity of γ-secretase, resulting in increased levels of various Aβ fragments, such as Aβ1-40 and Aβ1-42, in the brain. Hypoxia-induced cellular autophagy has resulted in the accumulation of autophagosomes in the brain of the AD mouse and increased production of Aβ, and inhibition of autophagy has attenuated the production of Aβ in response to hypoxia.16
Tesco et al found that expression of beta-site amyloid beta precursor protein cleaving enzyme (BACE) was upregulated by cerebral ischemia, leading to increased production of Aβ peptides.17 They hypothesized that the increased activities of BACE and γ-secretase are responsible for the increased activity of caspases after cerebral ischemia. They also found that after cerebral ischemia, the level of GGA3, an adaptor protein in the BACE cascade, decreased, while BACE level increased. MicroRNAs targeting GGA3 increase BACE and Aβ levels. Moreover, levels of the GGA3 protein in the brain specimens of AD patients are significantly decreased, whereas BACE levels are significantly increased, which may account for the enhanced BACE and Aβ levels in both cerebral infarction and AD.17 Mäkinen et al demonstrated that transient middle cerebral artery ischemia in rats causes abnormal accumulation of Aβ in the thalamus.18 This abnormality, together with Ca2+ channel disorder, lead to the formation of neuronal degeneration and senile plaques.18 Abdullah et al indicated that the development of AD is positively correlated with high serum levels of Aβ1-40 and a high ratio of Aβ1-40/Aβ1-42 in the peripheral blood.5 Likewise, data from a study by van Oijen et al implicated elevated serum Aβ1-40 levels in the pathogenesis of dementia.9 Aβ1-42 serum levels, however, decrease at the early stage of dementia.9 Finally, Kurapati et al reported that Aβ1-42-induced toxicity in human neuronal cells could be reversed by ashwagandha.19,20
In this study, we noted high serum levels of Aβ1-40 and Aβ1-42 in patients with artery stenosis and confirmed the correlation of Aβ with cerebral ischemia. Various mechanisms are involved in the detrimental effects of Aβ. For example, Aβ could activate astrocytes and microglias and cause inflammatory reactions via stimulating expression and release of tumor necrosis factor-alpha, interleukin (IL)-1, IL-6, and NO. Aβ might also induce nerve-cell apoptosis and disrupt the automatic regulation of vasomotion, collectively aggravating ischemic cerebral damage. Our results show that improved cerebral blood flow with stent-assisted angioplasty resulted in improved cognitive status and decreased Aβ1-40 serum levels, and a lower ratio of Aβ1-40/Aβ1-42, possibly through decreased production or increased clearance of Aβ1-40 in cerebral tissues. In our study cognitive status in patients with stent-assisted angioplasty improved obviously, accompanied by Aβ1-42 increasing. However, the study by Blasko et al suggested that increased serum Aβ1-42 over time was shown to be a significant predictor of mild cognitive impairment or AD. But they also concluded that plasma Aβ1-42 alone was not suitable as a biomarker for AD. Thus, more prospective, clinical trials are needed to prove the difference.21 The authors also concluded that plasma Aβ1-42 alone was not suitable as a biomarker for AD, thus, more prospective, clinical trials are needed. Thus, therapeutic strategies that increase cerebral blood flow may prevent the development and progression of AD and ischemic cerebral injury.
Conclusion
In this study, stent-assisted angioplasty in patients with intracranial and/or extracranial artery stenosis successfully improved cognitive status, and decreased Aβ1-40 serum levels and the Aβ1-40/Aβ1-42 ratio. Therapeutic strategies that increase cerebral blood flow may prevent the development and progression of AD and ischemic cerebral injury.
Acknowledgments
We sincerely thank Simcere Pharmaceutical Group for their fund support. We also thank Xinyong Zhang, Zengjun Wang, Jingming Lu, and Guang Yang for assistance with patient recruitment.
Disclosure
The authors report no conflicts of interest in this work.
References
Nakamura K, Watanabe N, Ohkawa H, et al. Effects on caregiver burden of a donepezil hydrochloride dosage increase to 10 mg/day in patients with Alzheimer’s disease. Patient Prefer Adherence. 2014;15;8:1223–1228. | ||
López-Pousa S, Arranz FJ. Characteristics of patients with Alzheimer’s disease who switch to rivastigmine transdermal patches in routine clinical practice. Patient Prefer Adherence. 2013;7:47–54. | ||
Rentz DM, Locascio JJ, Becker JA, et al. Cognition, reserve, and amyloid deposition in normal aging. Ann Neurol. 2010;67(3):353–364. | ||
Zhang X, Li L, Zhang X, et al. Prenatal hypoxia may aggravate the cognitive impairment and Alzheimer’s disease neuropathology in APPSwe/PS1A246E transgenic mice. Neurobiol Aging. 2013;34(3):663–678. | ||
Abdullah L, Paris D, Luis C, et al. The influence of diagnosis, intra- and inter-person variability on serum and plasma Abeta levels. Neurosci Lett. 2007;428(2–3):53–58. | ||
Frankfort SV, Tulner LR, van Campen JP, Verbeek MM, Jansen RW, Beijnen JH. Amyloid beta protein and tau in cerebrospinal fluid and plasma as biomarkers for dementia: a review of recent literature. Curr Clin Pharmacol. 2008;3(2):123–131. | ||
Graff-Radford NR, Crook JE, Lucas J, et al. Association of low plasma Abeta42/Abeta40 ratios with increased imminent risk for mild cognitive impairment and Alzheimer disease. Arch Neurol. 2007;64(3):354–362. | ||
Mayeux R, Honig LS, Tang MX, et al. Plasma A[beta]40 and A[beta]42 and Alzheimer’s disease: relation to age, mortality, and risk. Neurology. 2003;61(9):1185–1190. | ||
van Oijen M, Hofman A, Soares HD, Koudstaal PJ, Breteler MM. Plasma Abeta(1-40) and Abeta(1-42) and the risk of dementia: a prospective case-cohort study. Lancet Neurol. 2006;5(8):655–660. | ||
Gabelle A, Richard F, Gutierrez LA, et al. Plasma amyloid-β levels and prognosis in incident dementia cases of the 3-City Study. J Alzheimers Dis. 2012;33(2):381–391. | ||
Abdullah L, Luis C, Paris D, et al. High serum Abeta and vascular risk factors in first-degree relatives of Alzheimer’s disease patients. Mol Med. 2009;15(3–4):95–100. | ||
Ihara M, Kalaria RN. Understanding and preventing the development of post-stroke dementia. Expert Rev Neurother. 2014;14(9):1067–1077. | ||
Dregan A, Wolfe CD, Gulliford MC. Does the influence of stroke on dementia vary by different levels of prestroke cognitive functioning?: a cohort study. Stroke. 2013;44(12):3445–3451. | ||
Noor Kamal Al-Qazzaz, Sawal Hamid Ali, Siti Anom Ahmad, et al. Cognitive impairment and memory dysfunction after a stroke diagnosis: a post-stroke memory assessment. Neuropsychiatr Dis Treat. 2014;10:1677–1691. | ||
Fengjin Zhang, Linlan Jiang. Neuroinflammation in Alzheimer’s disease. Neuropsychiatr Dis Treat. 2015;11:243–256. | ||
Jisun Lee, Samantha Giordano, Jianhua Zhang. Autophagy, mitochondria and oxidative stress: cross-talk and redox signaling. Biochem J. 2012;441:523–540. | ||
Tesco G, Koh YH, Kang EL, et al. Depletion of GGA3 stabilizes BACE and enhances beta-secretase activity. Neuron. 2007;54(5):721–737. | ||
Mäkinen S, van Groen T, Clarke J, et al. Coaccumulation of calcium and beta-amyloid in the thalamus after transient middle cerebral artery occlusion in rats. J Cereb Blood Flow Metab. 2008;28(2):263–268. | ||
Kurapati KR, Samikkannu T, Atluri VS, Kaftanovskaya E, Yndart A, Nair MP. β-Amyloid1-42, HIV-1Ba-L (clade B) infection and drugs of abuse induced degeneration in human neuronal cells and protective effects of ashwagandha (Withania somnifera) and its constituent Withanolide A. PLoS One. 2014;9(11):e112818. | ||
Kurapati KR, Atluri VS, Samikkannu T, Nair MP. Ashwagandha (Withania somnifera) reverses β-amyloid1-42 induced toxicity in human neuronal cells: implications in HIV-associated neurocognitive disorders (HAND). PLoS One. 2013;8(10):e77624. | ||
Blasko I, Jellinger K, Kemmler G, et al. Conversion from cognitive health to mild cognitive impairment and Alzheimer’s disease: prediction by plasma amyloid beta 42, medial temporal lobe atrophy and homocysteine. Neurobiol Aging. 2008;29(1):1–11. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.